
Abstract
Recently, it has been reported that dual agonists of the glucagon-like peptide-1 (GLP-1) receptor and the glucagon receptor (GCGR) have important functions in regulating glucose metabolism and energy expenditure. However, the usefulness of these dual agonists for the treatment of type 2 diabetes remains unclear. This systematic review and meta-analysis of randomized controlled trials aimed to assess the impact of GLP-1/GCGR dual agonists on glycemic markers. The search process was performed in PubMed, Scopus, ClinicalTrials.gov, and Cochrane Library databases. Randomized controlled trials assessing the impact of GLP-1/GCGR agonists on glycemic parameters were included. The meta-analysis was performed with the random-effects model and the generic inverse variance method, and the leave-one-out method was used for the sensitivity analysis. The meta-analysis of 14 randomized controlled trials demonstrated that GLP-1/GCGR agonists significantly decrease fasting glucose (weighted mean difference (WMD): –0.79 mmol/l, 95% confidence interval (CI): –1.14, –0.45, p < 0.0001, I2 = 92%) and glycated hemoglobin (HbA1c; WMD: –0.50%, 95% CI: –0.67, –0.32, p < 0.0001, I2 = 93%). However, these dual agonists had no significant impact on insulin levels (WMD: –14.78 pmol/l, 95% CI: –35.89, 6.34, p = 0.17, I2 = 87%). The subgroup analysis by treatment duration exhibited that GLP-1/GCGR agonists significantly reduced fasting glucose and HbA1c in randomized controlled trials ≤12 and >12 weeks, as well as insulin levels in those studies >12 weeks of treatment. In conclusion, the results of our meta-analysis indicated that GLP-1/GCGR dual agonists have a positive effect by decreasing fasting glucose and HbA1c concentrations.
Keywords
Introduction
Currently, diabetes represents a major global public health problem owing to its increasing prevalence over time. According to data from the IDF Diabetes Atlas, approximately 589 million adults aged 20–79 years were living with diabetes in 2024, corresponding to a prevalence of 11.1%. By 2050, this number is expected to rise to 853 million, with a prevalence of 13.0%. 1 Additionally, diabetes is considered a major cause of mortality, as 9.3% of deaths worldwide among adults aged 20–79 years in 2024 were attributed to diabetes or its complications, representing 3.4 million adults. Of them, only 2.4 million individuals had been diagnosed with this disease, meaning that one in three adults living with diabetes were undiagnosed. 1 Therefore, over the years, different drugs have been developed to improve glucose control and prevent diabetes related complications.
Recently, it has been reported that dual agonists of the glucagon-like peptide-1 (GLP-1) receptor and the glucagon receptor (GCGR), a family of G-protein-coupled receptors, have important functions in regulating glucose metabolism and energy expenditure. 2 Although activation of GLP-1 receptor and GCGR exerts opposite actions on glucose homeostasis, some clinical trials have observed beneficial effects on weight reduction and glucose control after dual agonism treatment.3,4 GLP-1 receptor activation promotes several physiological mechanisms, including postprandial insulin secretion, regulation of food intake by increasing satiety, and delaying gastric emptying. In addition, GLP-1 confers cardiovascular and liver protection by reducing endothelial dysfunction, inflammation, and regulating lipid metabolism.5,6 On the other hand, activation of the GCGR alone reduces food intake, promotes fatty acid oxidation, and increases energy expenditure. However, an unfavorable effect is its hyperglycemic action through de novo glucose production and glycogen breakdown. 7 For this reason, when combined with a GLP-1R agonist, this negative effect can be mitigated, resulting in improved glucose control. 8
The synergistic effects of GLP-1 and GCGRs convert these dual agonists into a therapeutic option for type 2 diabetes accompanied by weight loss, which could enhance the management of diabetes and obesity that usually occur together. 9 However, given that this class of drugs is rarely used because they are in early stages of development and the clinical trials assessing their long-term effects are ongoing, the usefulness of these dual agonists for the treatment of type 2 diabetes is still unclear. Therefore, this systematic review and meta-analysis of randomized controlled trials aimed to assess the impact of GLP-1/GCGR dual agonists on glycemic markers.
Activation of GLP-1 and glucagon receptors exerts opposite actions on glucose homeostasis. Some studies have observed beneficial effects on weight reduction and glucose control after dual agonism treatment.
GLP-1/glucagon receptor dual agonists significantly reduced fasting glucose and glycated hemoglobin concentrations, but they had no significant effect on insulin levels.
Our results show that the glucagon-like peptide-1 and glucagon receptor dual agonists improve glucose control by reducing fasting glucose and glycated hemoglobin concentrations, which highlights the positive synergistic effect of dual agonists for managing type 2 diabetes in patients with obesity.
Materials and methods
Search strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines 10 and a framework for approaches and methods in evidence synthesis (FRAMES), 11 this study was conducted. The search process was performed in PubMed, Scopus, ClinicalTrials.gov, and Cochrane Library databases with the following terms within titles and abstracts (including MESH terms): (GLP-1 OR glucagon-like peptide-1 receptor agonist OR GLP-1 receptor agonist OR GLP-1RA OR glucagon receptor OR GCGR OR dual agonists OR LY3324954 OR LY3305677 OR G49 OR JNJ-64565111 OR MK-6024 OR HM12525A OR MEDI0382 OR IBI362 OR pemvidutide OR survodutide OR mazdutide OR cotadutide OR efinopegdutide) AND (glucose OR postprandial glucose OR insulin OR insulin resistance OR insulin sensitivity OR “HOMA” OR HbA1c OR hemoglobin A1c OR glycated hemoglobin OR glycosylated hemoglobin) AND (“controlled trial” OR randomized OR “clinical trial” OR trial). To improve the search, the wild-card term “*” was used. The articles were searched from inception to August 2025.
Eligibility criteria
Eligible studies were required to meet the following criteria: (1) Population: obesity, type 2 diabetes, non-alcoholic fatty liver disease; (2) Intervention: pemvidutide, survodutide, mazdutide, cotadutide, or efinopegdutide; (3) Comparator: placebo; (4) Outcomes: glucose, insulin, HOMA, and/or glycated hemoglobin (HbA1c); (5) Study design: randomized controlled trials (parallel or cross-over).
Study selection
Randomized controlled trials (parallel or cross-over design) reporting changes in fasting glucose, postprandial glucose, insulin, or HbA1c concentrations after GLP-1/GCGR agonists therapy, and providing complete data at baseline and at the end of follow-up in the study groups or presenting the net change values were included in the meta-analysis. Additionally, uncontrolled clinical trials, observational studies (cross-sectional, case-control, and cohort designs), and incomplete data on glycemic outcomes were exclusion criteria. Two independent authors performed the screening and selection of studies, and disagreements were discussed and resolved by a third author.
Data extraction
After the review of the selected studies, the following data were obtained: name of the first author; year of publication; study design; number of participants in the treatment and control groups; dose and treatment duration with GLP-1/GCGR agonists; age, gender, and body mass index (BMI) of study participants; fasting glucose, insulin, and HbA1c concentrations.
Quality assessment
The quality of the included studies was assessed with the Cochrane risk-of-bias tool for randomized trials version 2 (RoB 2.0), 12 considering the next items: randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each item was qualified as either low risk, some concerns, or high risk.
Quantitative data synthesis
Meta-analysis was conducted with the Review Manager statistical software version 5.3 (The Nordic Cochrane Center, The Cochrane Collaboration, 2014). Values of glucose, insulin, and HbA1c were collated as mmol/l, pmol/l, and percentage (%), respectively. The effect size was obtained using the following formula: (measurement at the end of the study in the intervention group − measurement at baseline in the intervention group) − (measurement at the end of the study in the control group − measurement at baseline in the control group). When overall heterogeneity among studies was >50%, a random-effects model (using the DerSimonian-Laird method) and the generic inverse variance weighting method were used; while a fixed-effects model was selected for an overall heterogeneity <50%. Standard deviations (SDs) of the mean difference were calculated with the formula: SD = square root ((SD baseline) 2 + (SD final) 2 - (2R × SD baseline × SD final)). When the outcomes were provided as a median and interquartile range, mean and SD values were obtained.13,14 When the standard error of the mean (SEM) was provided, SD was calculated as follows: SD = SEM × sqrt (n). Effect sizes were expressed as weighted mean difference (WMD) and 95% confidence interval (CI). An I2 index >50% and the Cochrane Q statistic test with a p-value <0.05 was considered statistically significant to determine interstudy heterogeneity. Furthermore, the leave-one-out method was employed to determine the impact of each study on the overall effect size. 15 If possible, subgroup analyses by treatment duration (≤12 weeks vs >12 weeks) and sample sizes (n ≤ 100 vs n > 100) were conducted. Finally, when at least 10 studies were available for each outcome, a visual inspection of the funnel plot was applied to assess the potential publication bias.
Meta-regression
A random-effects meta-regression model was carried out to assess the potential confounders, such as age and BMI, on the effect size of glycemic markers.
Results
Study selection process
In summary, 805 studies were found after the search in databases, and 781 were excluded after the review of titles and abstracts. Then, 24 full-text articles were checked, and 10 were removed for not reporting the outcomes (n = 7) and no control group (n = 3). Thus, 14 clinical trials were included in the meta-analysis. The study selection process is shown in Figure 1.
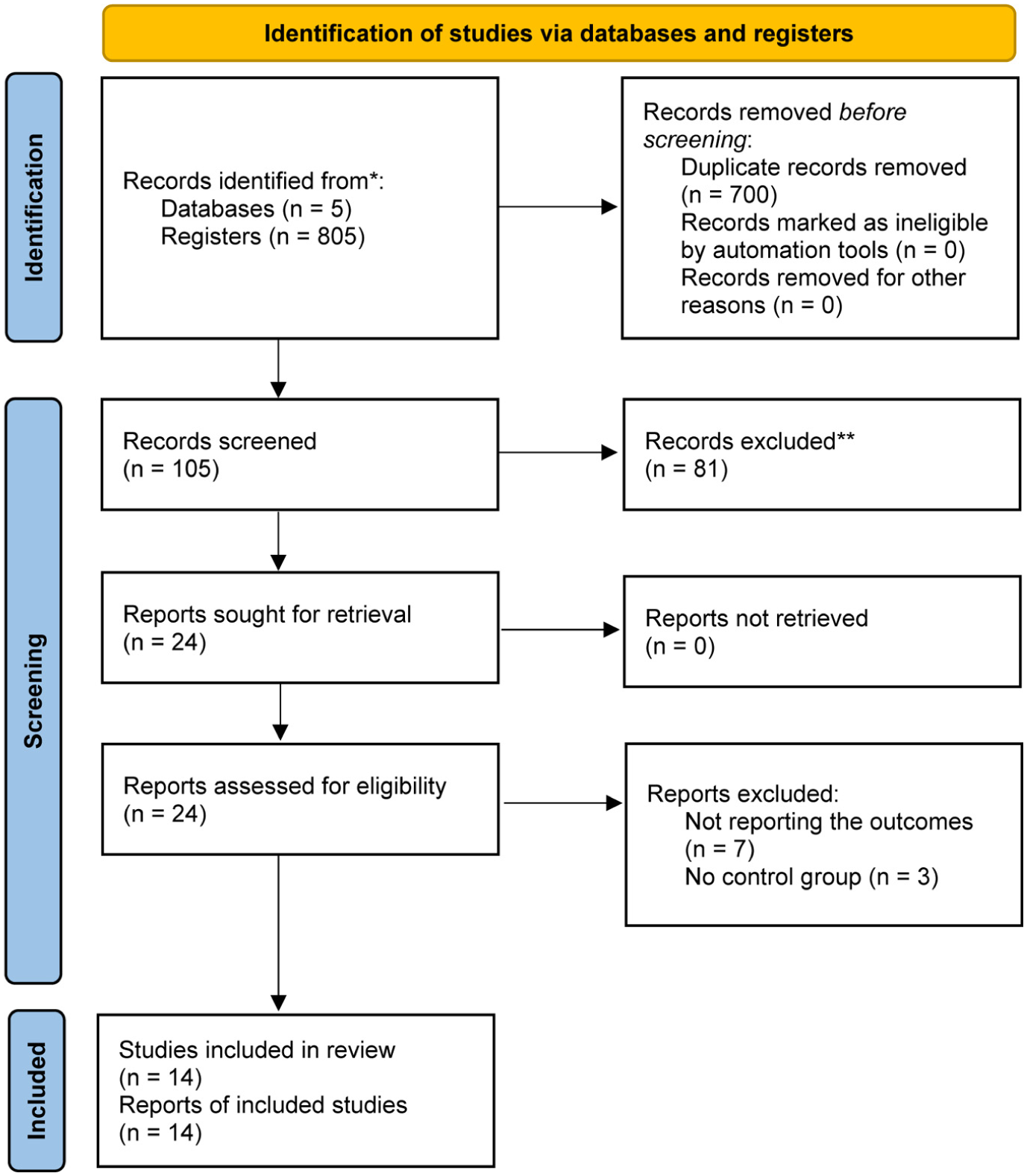
Flow chart of the number of studies selected for meta-analysis.
Characteristics of clinical trials
Table 1 summarizes the characteristics of the included studies. A total of 3466 subjects were included from 14 randomized controlled trials, comprising 2720 and 746 participants in the treatment and control arms, respectively. Selected studies were published between 2014 and 2020.3,4,16–27 The range of intervention periods was from 41 days to 54 weeks. All randomized controlled trials had a parallel design and enrolled patients with overweight, obesity, type 2 diabetes, diabetic kidney disease, or metabolic dysfunction-associated steatotic liver disease.
Demographic characteristics of the included studies.
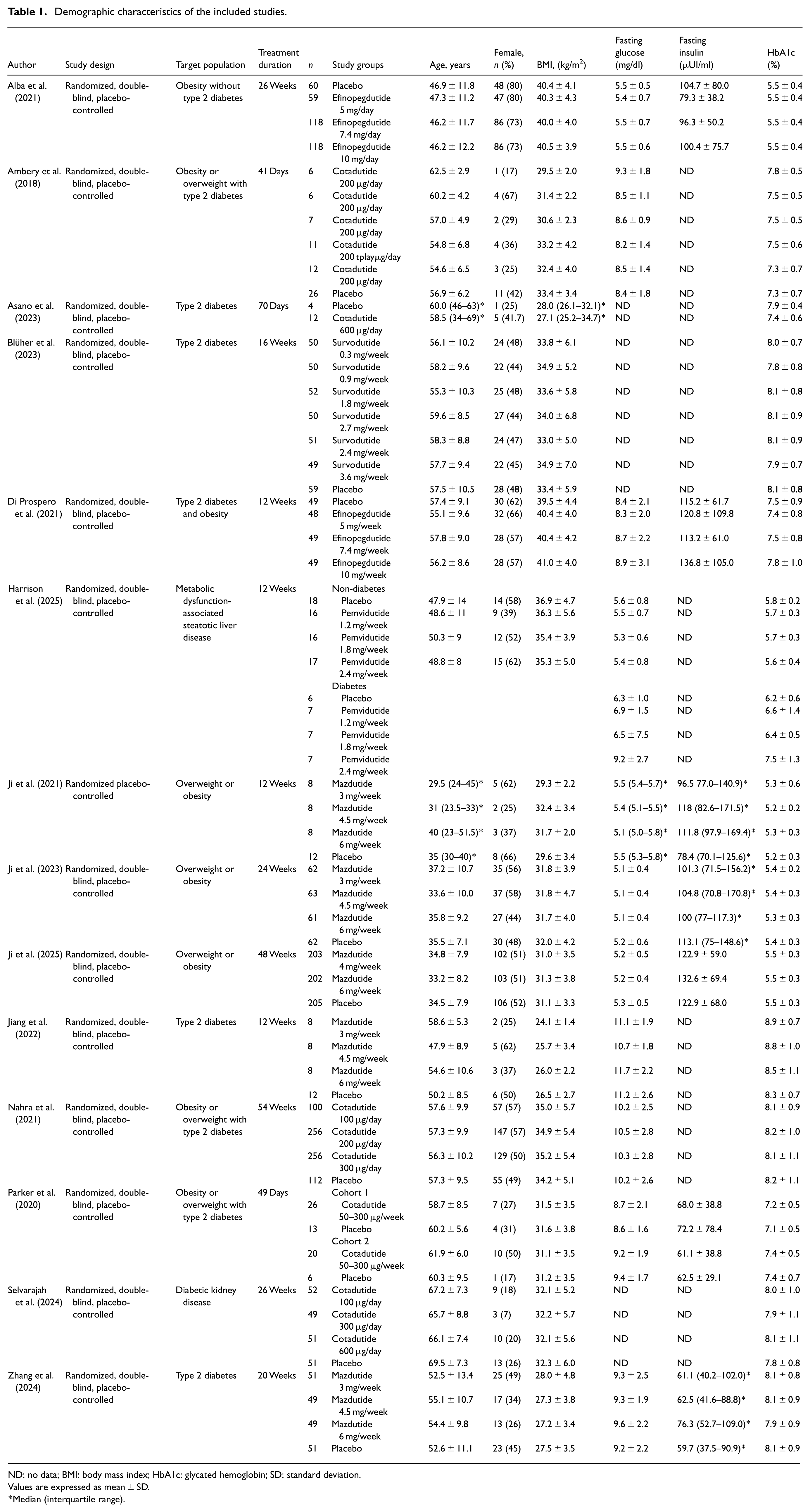
ND: no data; BMI: body mass index; HbA1c: glycated hemoglobin; SD: standard deviation.
Values are expressed as mean±SD.
Median (interquartile range).
Quality of bias assessment of clinical trials
Only one clinical trial showed some concerns for the randomization process. Otherwise, all included studies had a low risk for deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. The overall quality of the selected studies is presented in Figure 2.
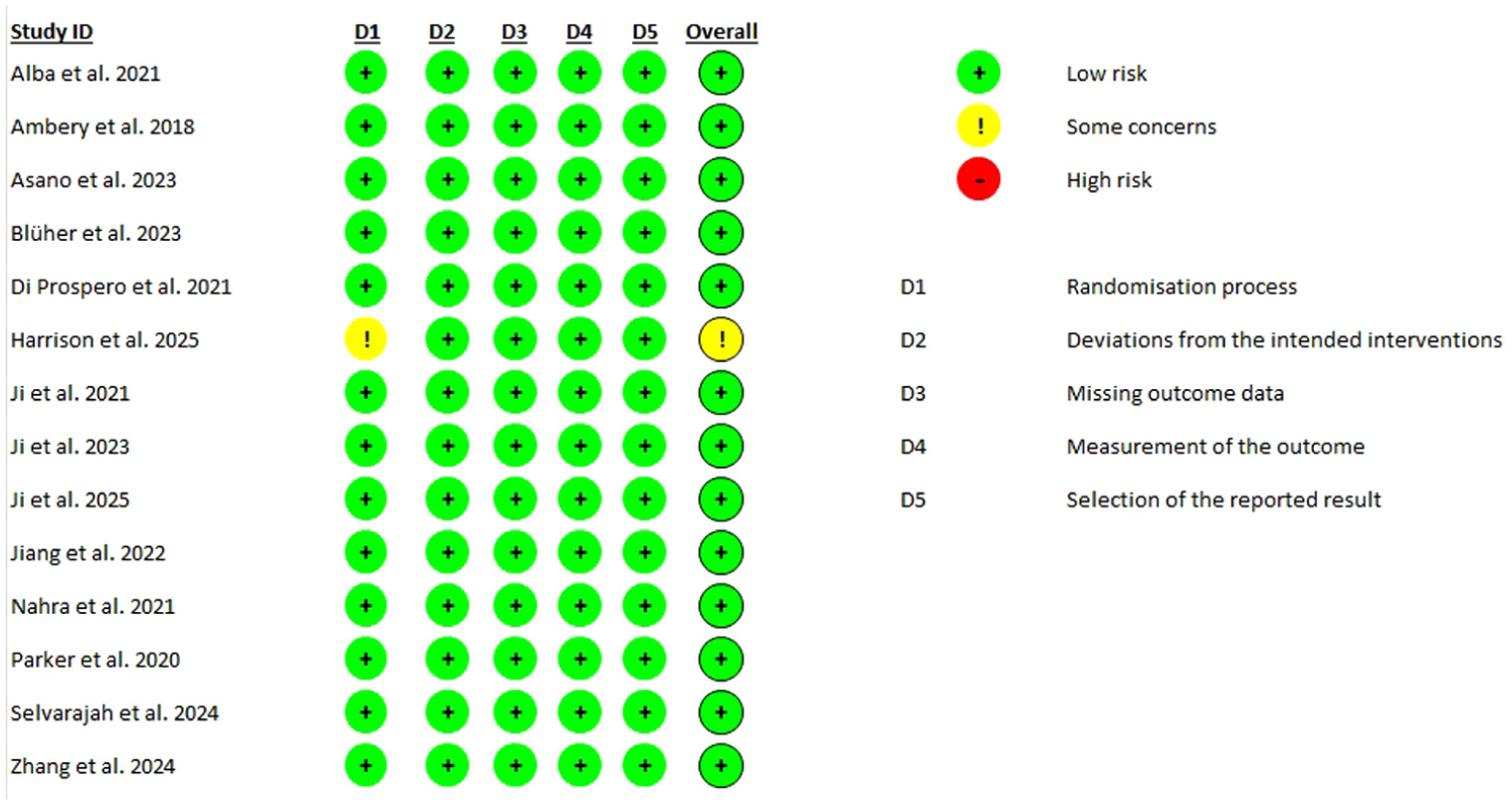
Risk-of-bias assessment of the included studies in the meta-analysis.
Effect of GLP-1/GCGR agonists on glycemic markers
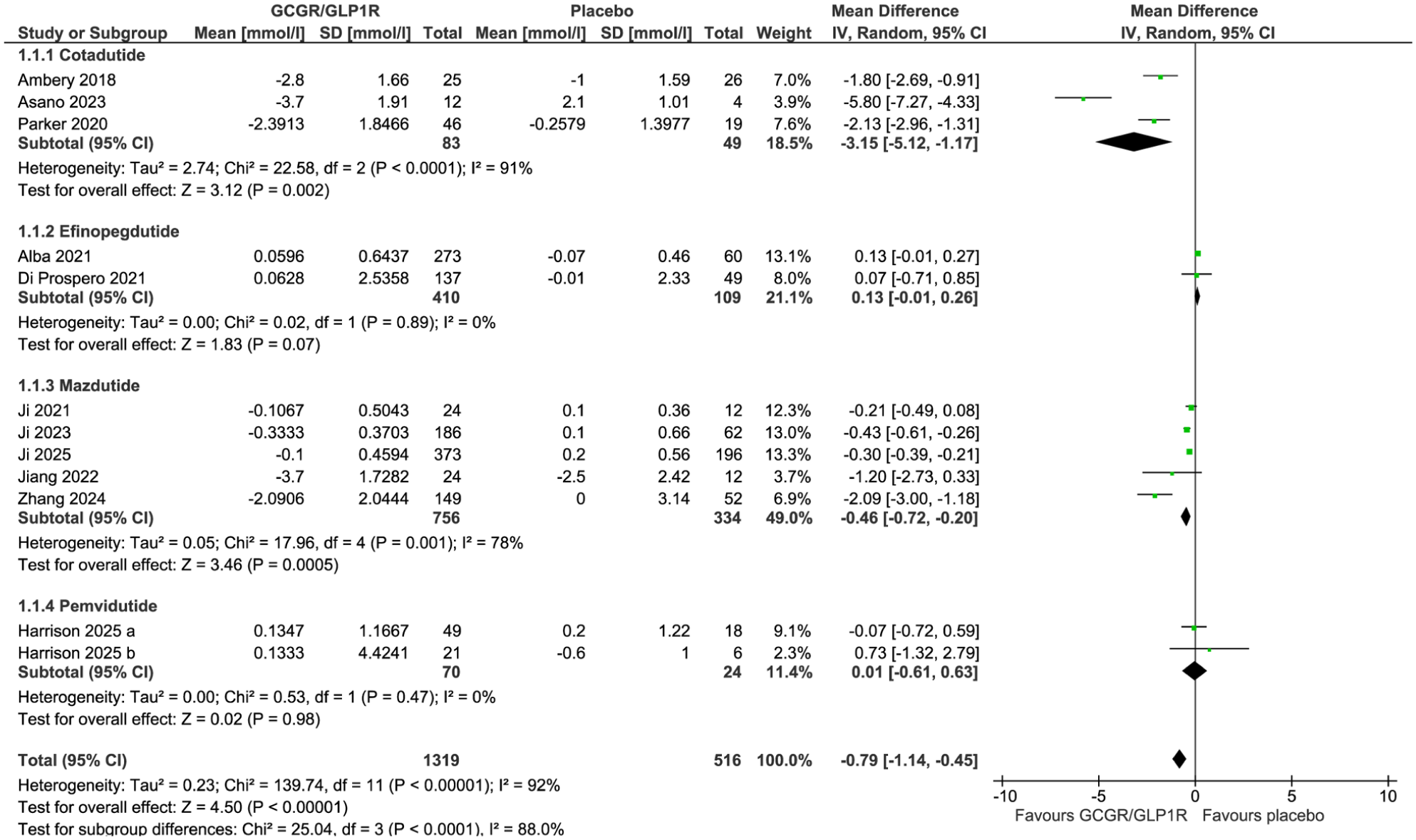
The meta-analysis of 14 randomized controlled trials showed that GLP-1/GCGR agonists significantly decrease fasting glucose (WMD: –0.79 mmol/l, 95% CI: –1.14, –0.45, p < 0.0001, I2 = 92%; Figure 3), and HbA1c (WMD: –0.50%, 95% CI: –0.67, –0.32, p< 0.0001, I2 = 93%; Figure 4). However, these dual agonists had no significant impact on insulin levels (WMD: –14.78 pmol/l, 95% CI: –35.89, 6.34, p = 0.17, I2 = 87%; Figure 5). Consistently, the sensitivity analysis was robust for these parameters (Tables 2–4). Furthermore, sensitivity analyses with alternative correlation coefficients (R = 0.2 and R = 0.8) showed minimal impact on pooled estimates across outcomes. For fasting glucose, medication subanalysis remained essentially unchanged with R = 0.2 and R = 0.8. Duration-based subgroup analyses were likewise stable, with ≤12 weeks remaining significant across all R values, whereas >12 weeks showed no significant effect only at R = 0.2. For HbA1c, the findings in the medication subset were consistent irrespective of R values, while the subgroup analyses by treatment duration demonstrated negligible differences at R = 0.5. For insulin, mazdutide, efinopegdutide, and ≤12 weeks analyses were unchanged and non-significant. However, the estimates in the >12 weeks subgroup were only significant with R = 0.2 (Table 5).
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on fasting glucose.
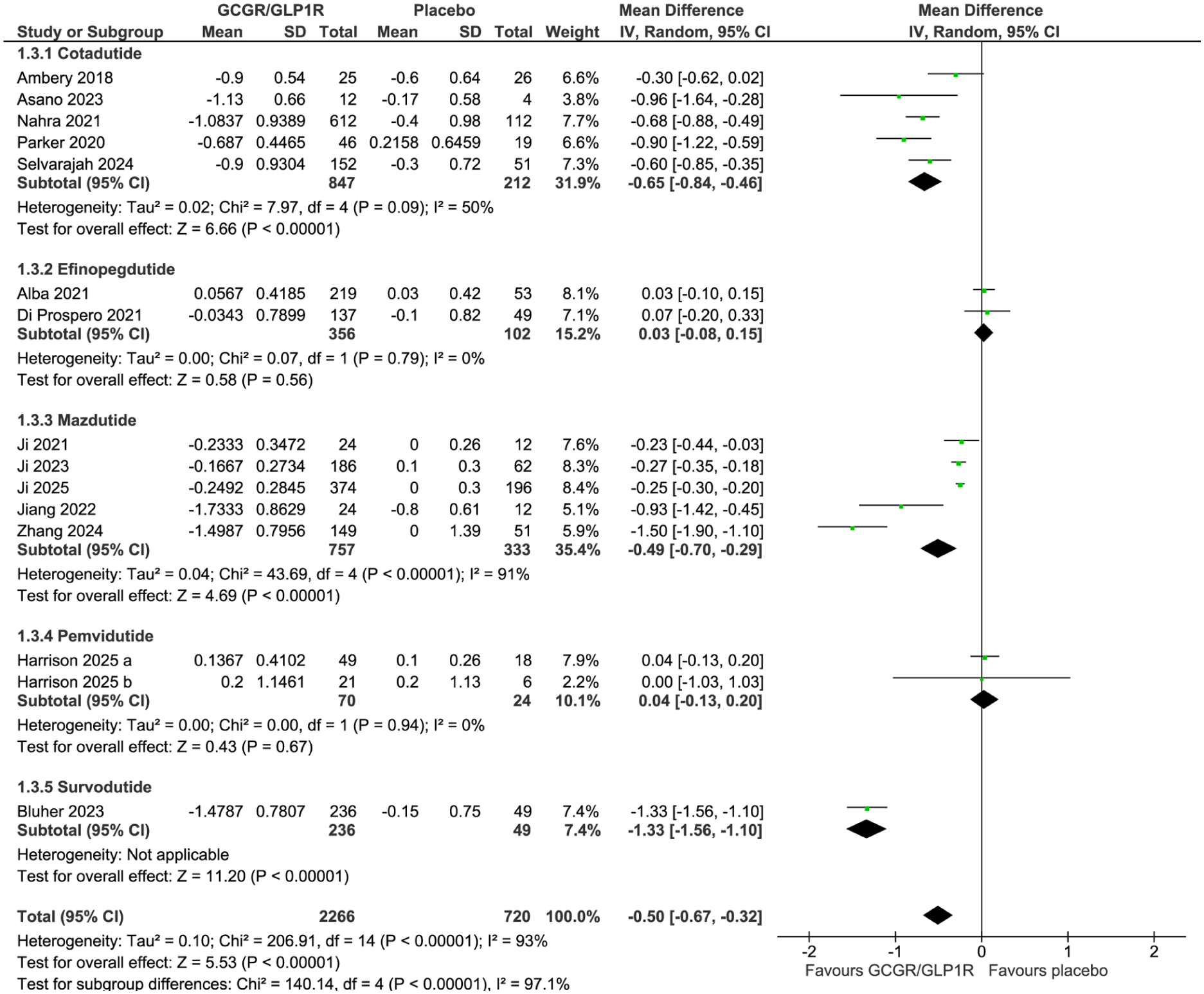
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on HbA1c.
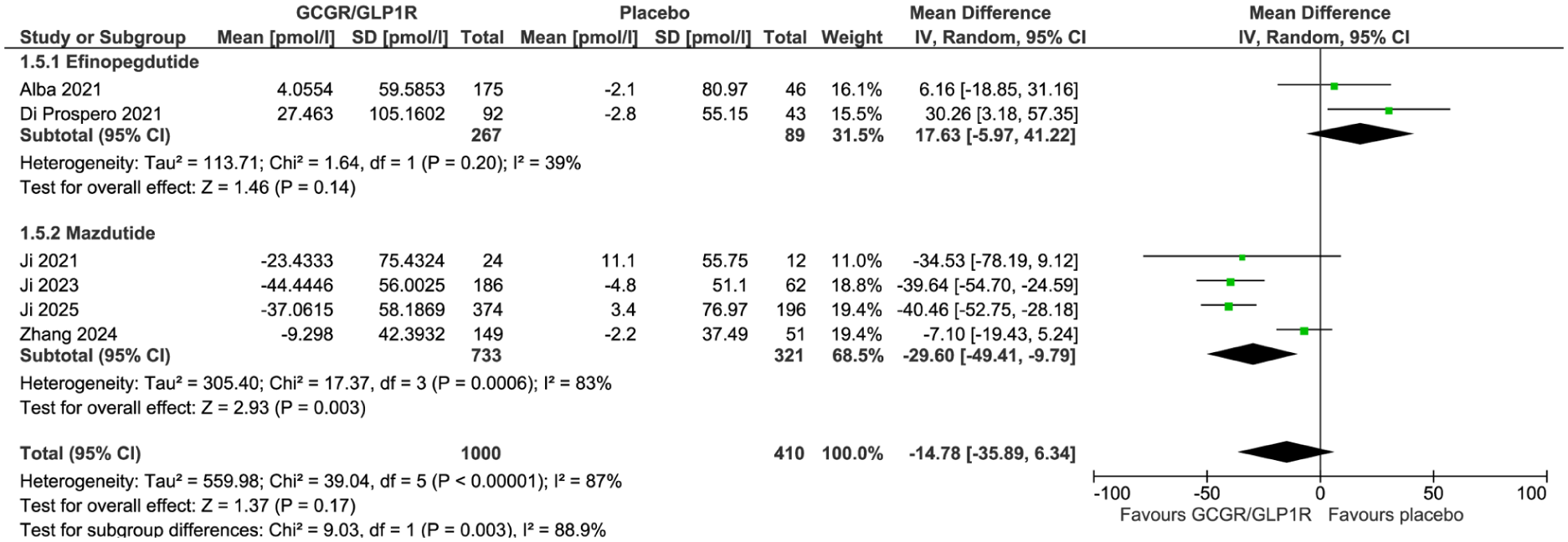
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on insulin levels.
Results of leave-one-out sensitivity analysis for fasting glucose.
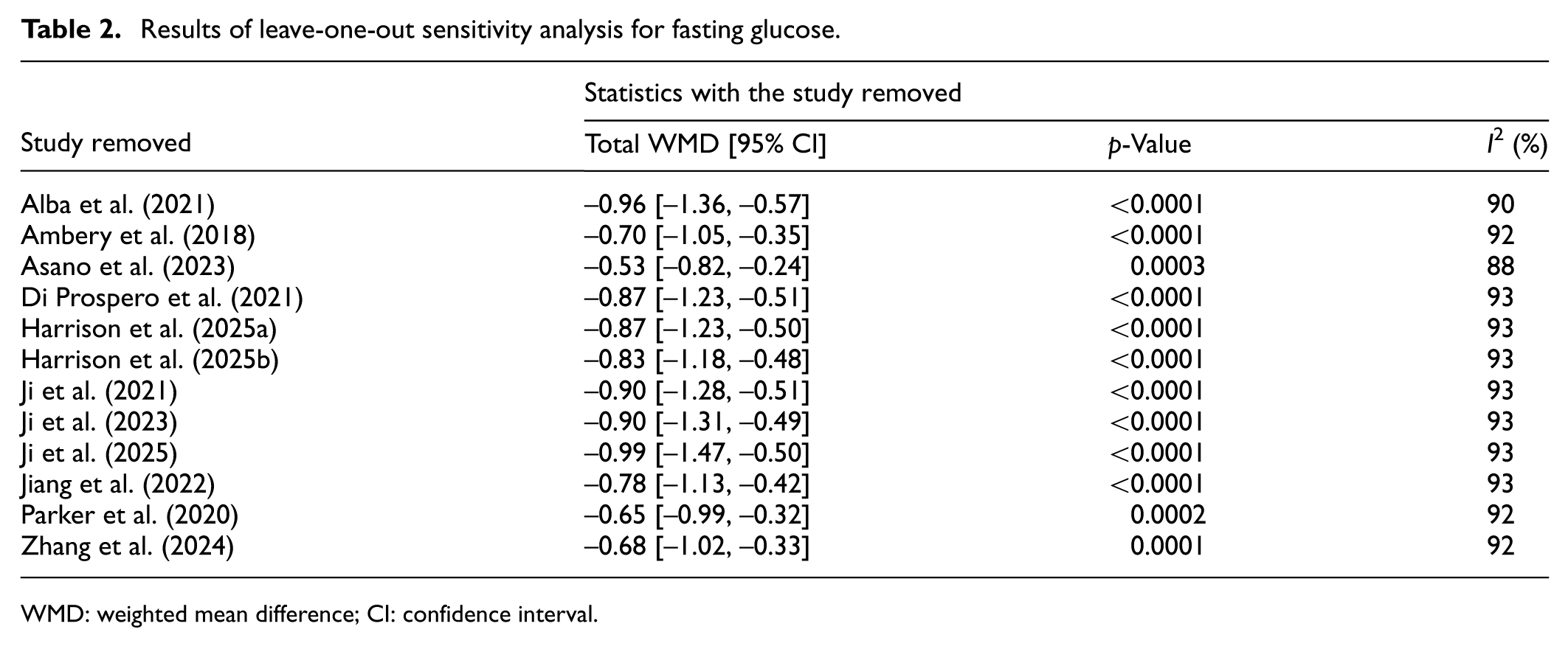
WMD: weighted mean difference; CI: confidence interval.
Results of leave-one-out sensitivity analysis for HbA1c.
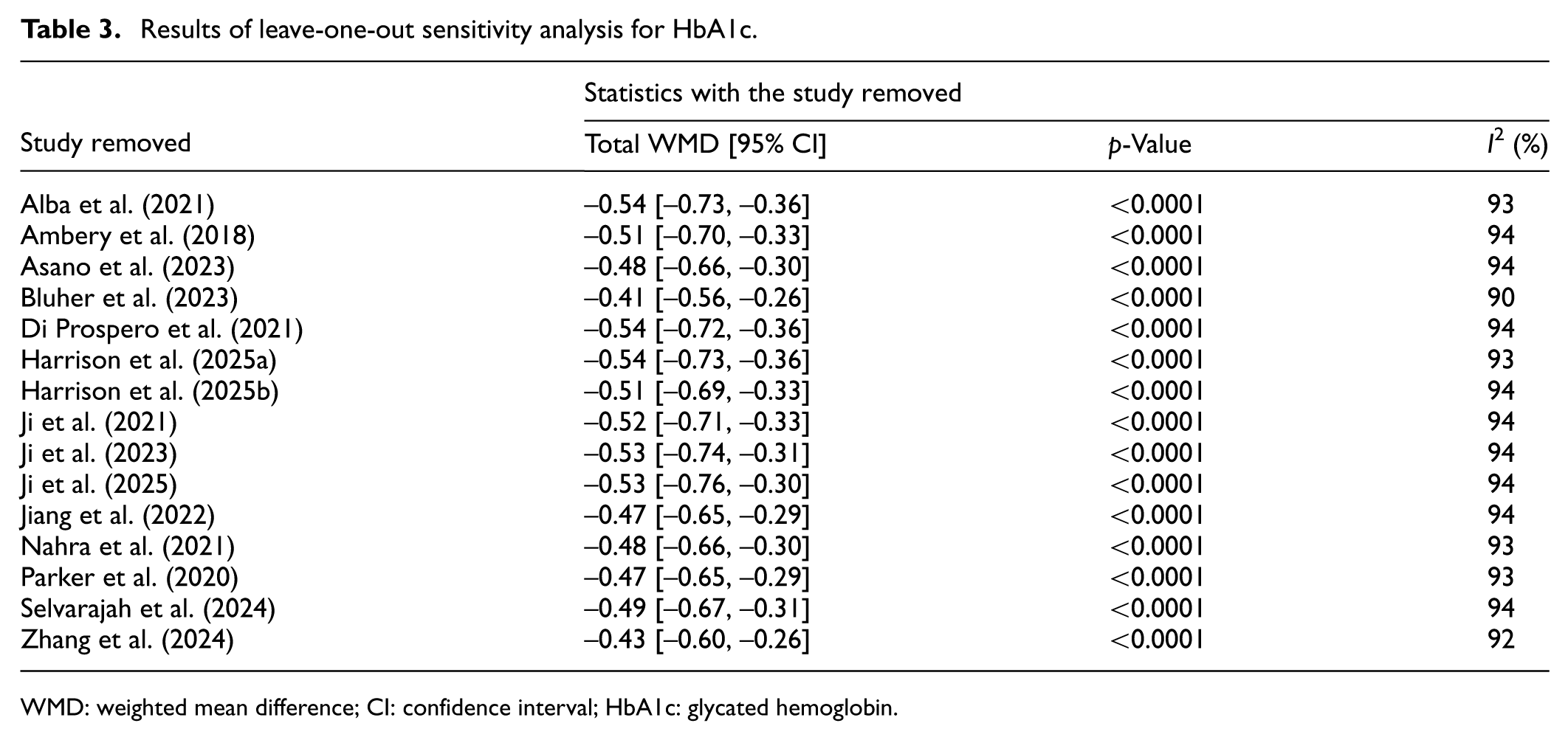
WMD: weighted mean difference; CI: confidence interval; HbA1c: glycated hemoglobin.
Results of leave–one–out sensitivity analysis for insulin.
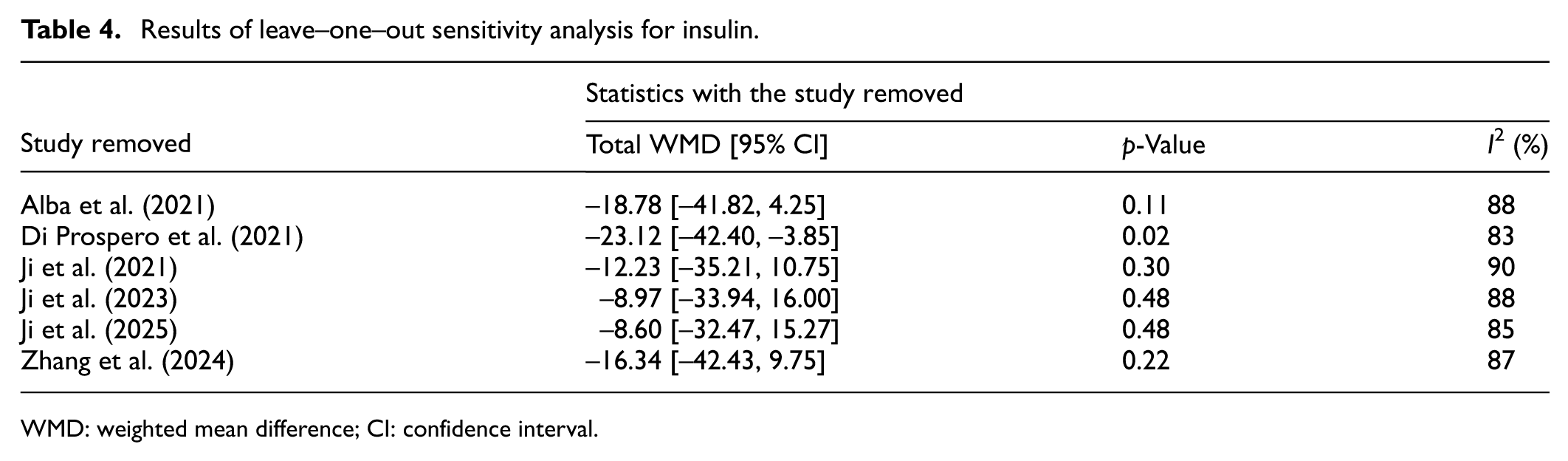
WMD: weighted mean difference; CI: confidence interval.
Robustness of analysis with different correlation coefficients.
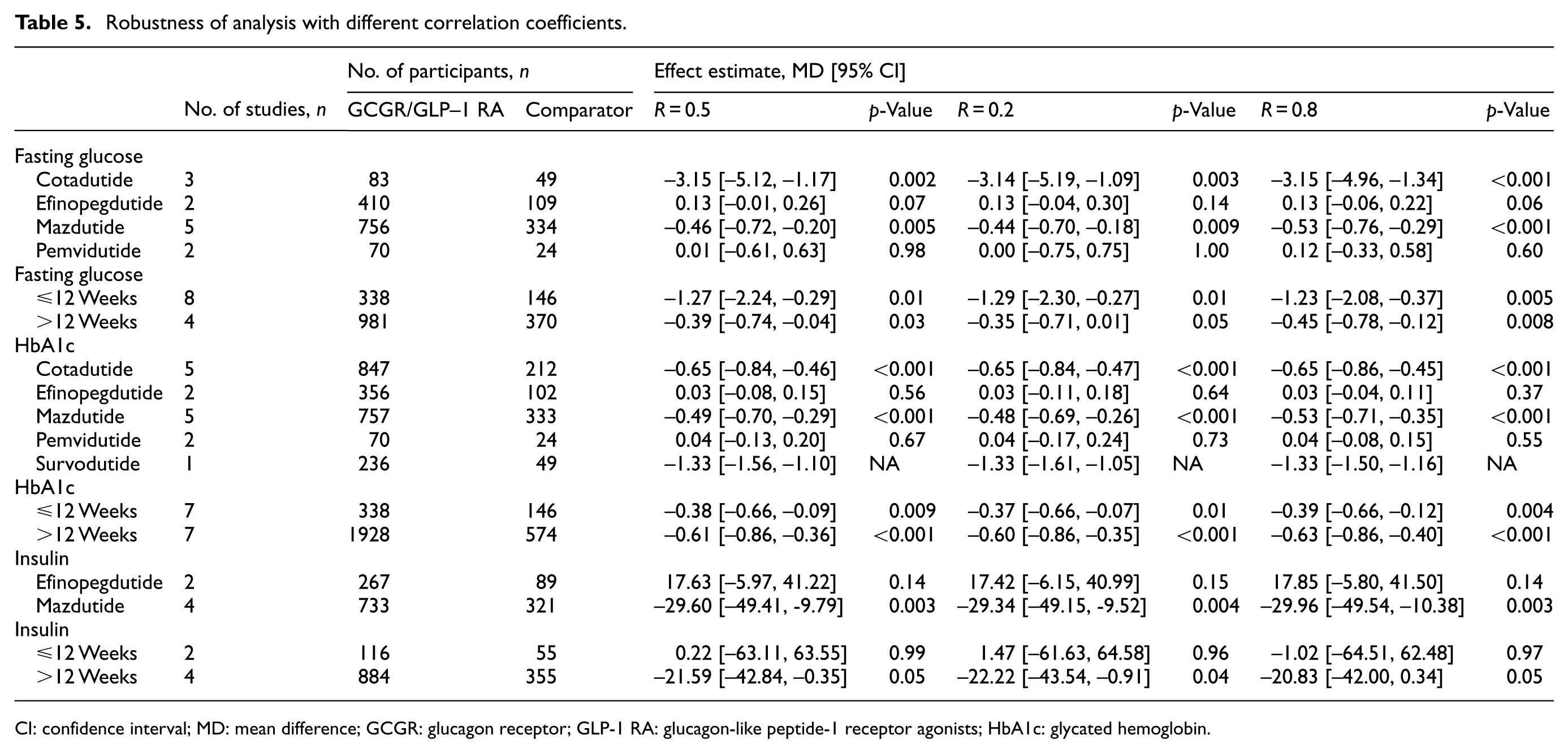
CI: confidence interval; MD: mean difference; GCGR: glucagon receptor; GLP-1 RA: glucagon-like peptide-1 receptor agonists; HbA1c: glycated hemoglobin.
Additionally, the subgroup analysis by treatment duration exhibited that GLP-1/GCGR agonists significantly reduced fasting glucose and HbA1c in randomized controlled trials ≤12 and >12 weeks (Figures 6 and 7). However, insulin levels were only decreased in those studies with >12 weeks of treatment (Figure 8). Otherwise, a subgroup analysis by sample sizes revealed that GLP-1/GCGR agonists significantly decreased fasting glucose and HbA1c in clinical trials with n ≤ 100 and n > 100 (Figures 9 and 10), whereas insulin levels only lowered in those studies with n > 100 (Figure 11).
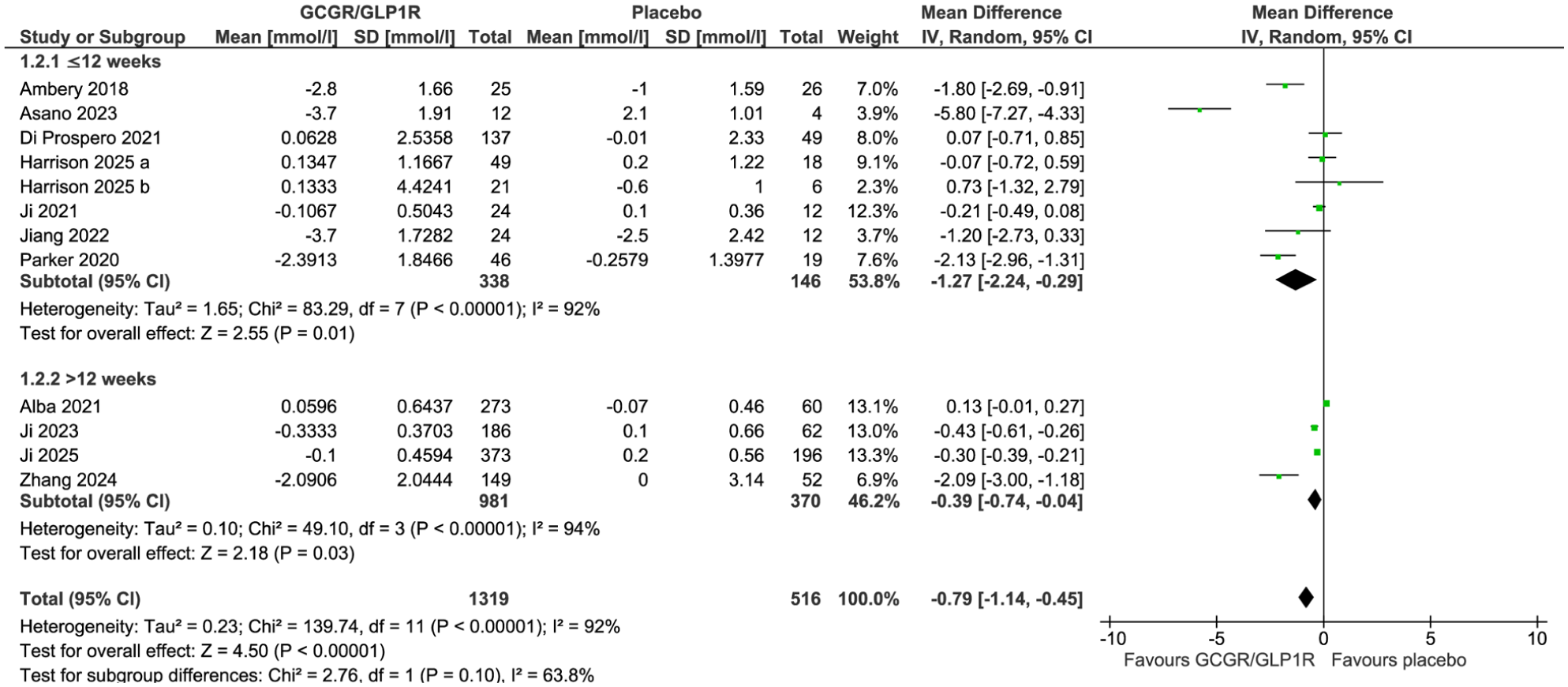
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on fasting glucose in clinical trials with treatment durations of ≤12 and <12 weeks.
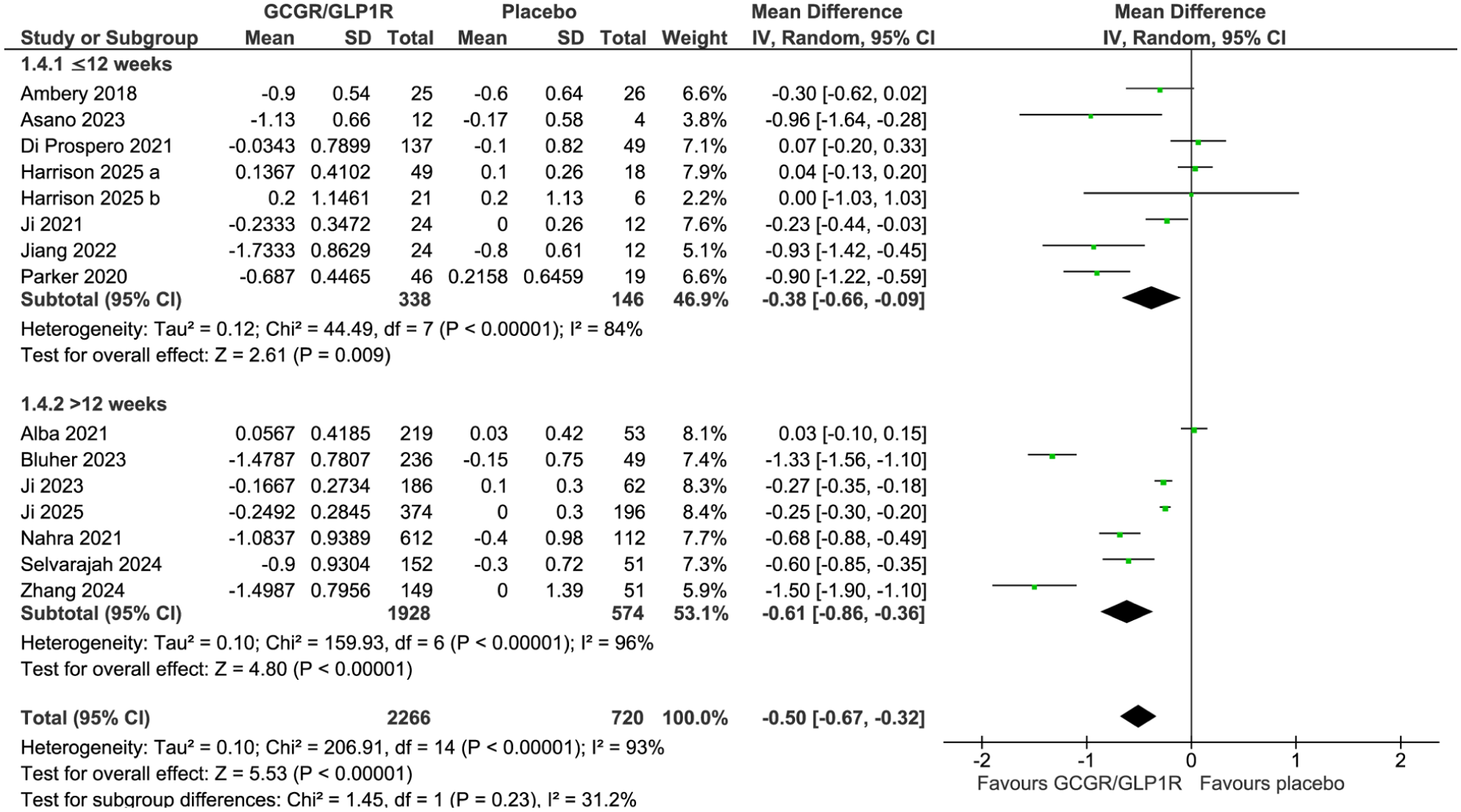
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on HbA1c in clinical trials with treatment durations of ≤12 and <12 weeks.
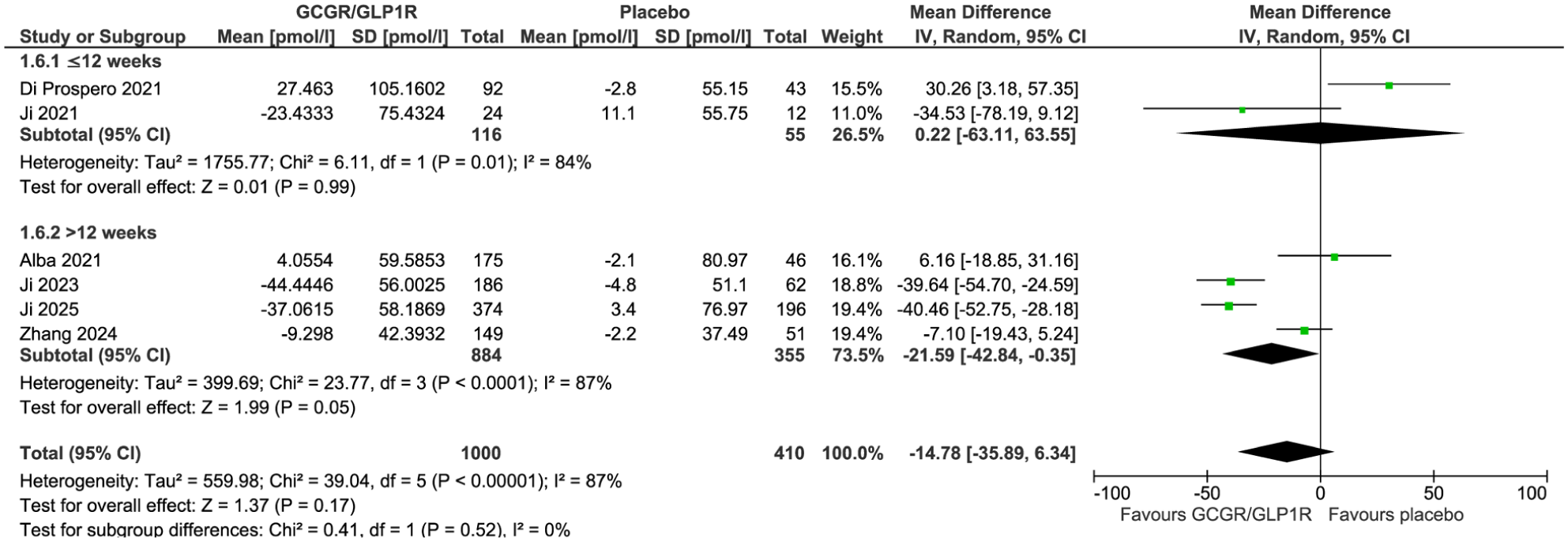
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on insulin levels in clinical trials with treatment durations of ≤12 and <12 weeks.
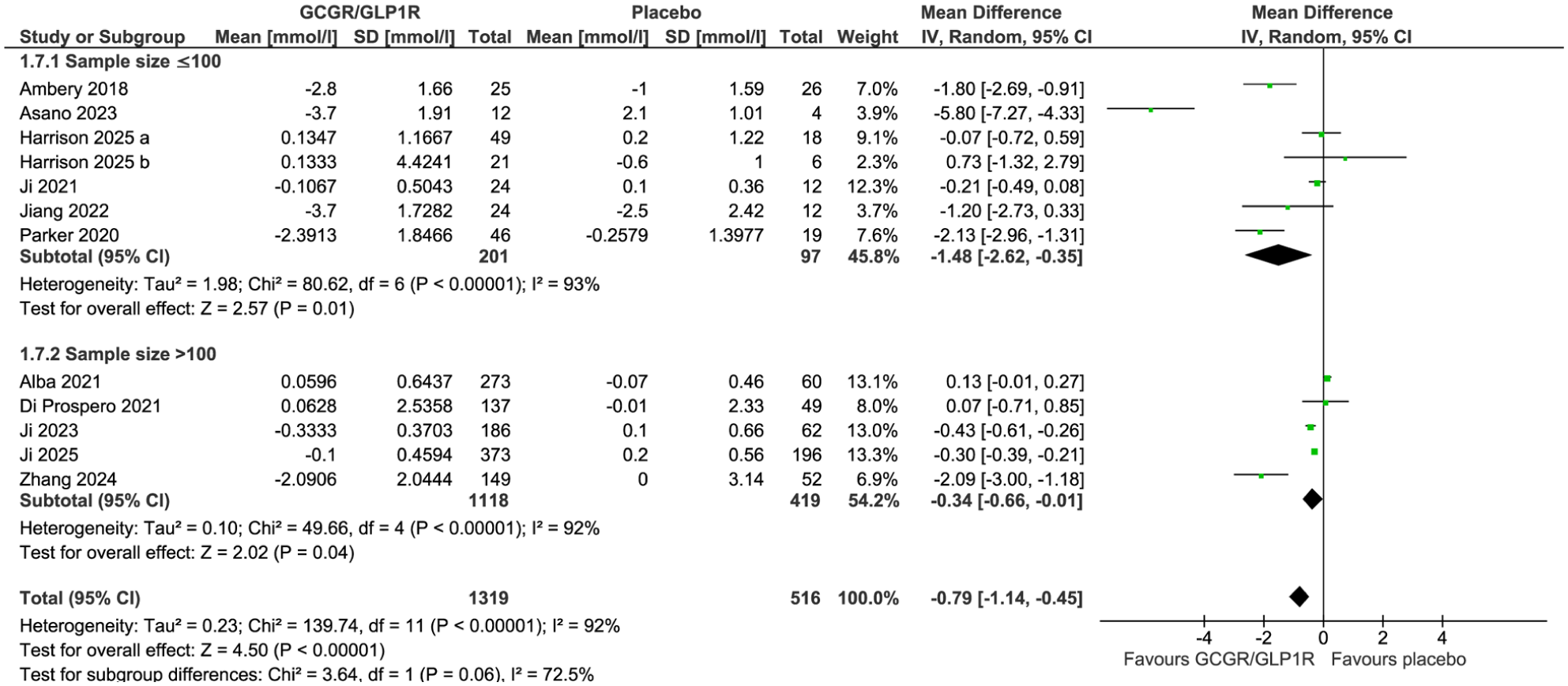
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on fasting glucose in clinical trials with sample sizes of n ≤ 100 and n > 100.
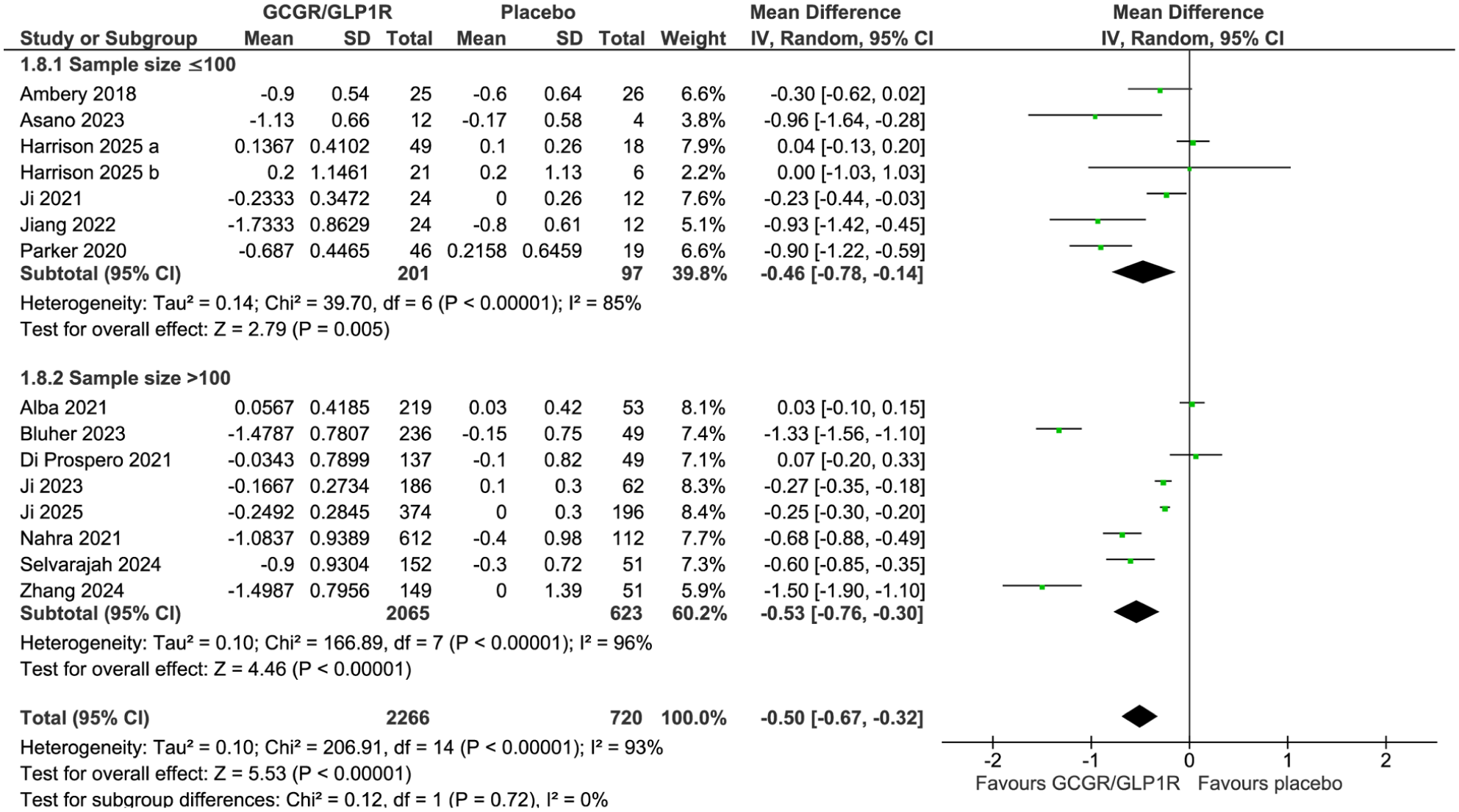
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on HbA1c in clinical trials with sample sizes of n ≤ 100 and n > 100.
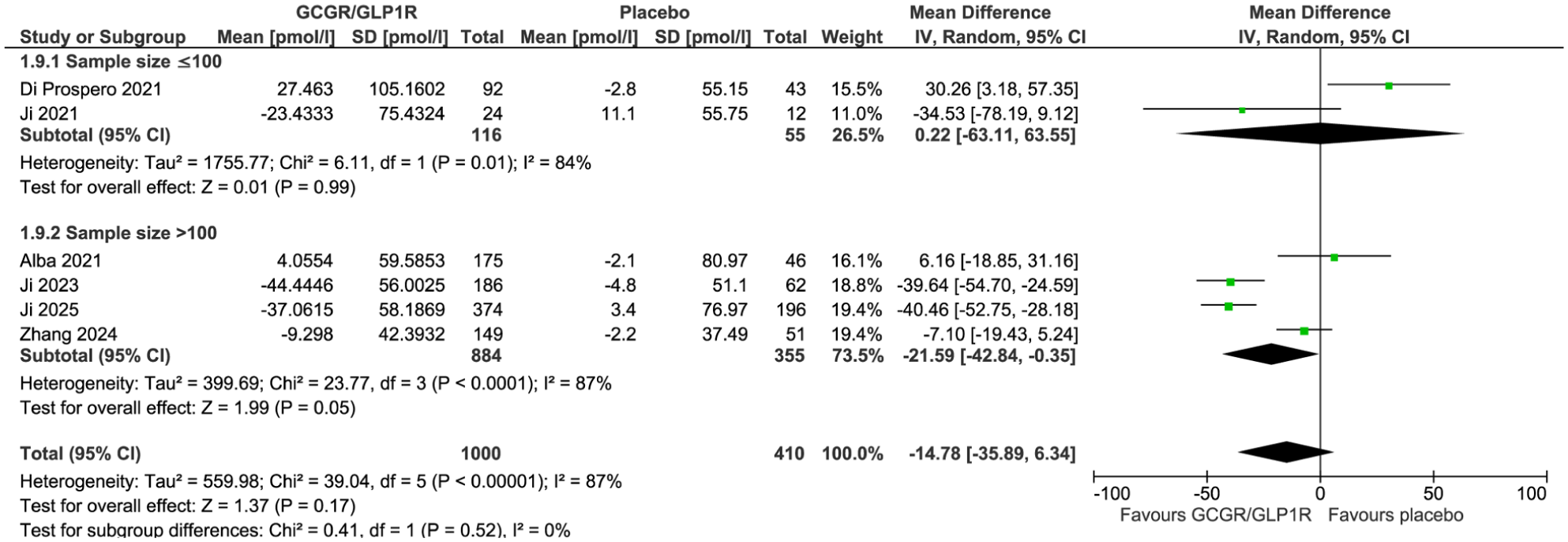
Forest plot displaying weighted mean difference and 95% confidence intervals for the effect of GLP-1/glucagon receptor agonists on insulin levels in clinical trials with sample sizes of n ≤ 100 and n > 100.
Meta-regression
Meta-regression analysis showed that the effect of GLP-1/GCGR agonists on fasting glucose was associated with age (–0.08; 95% CI: –0.11, –0.06; p < 0.001) and BMI (0.09; 95% CI: 0.06, 0.12; p < 0.001). Also, the effect size in HbA1c was associated with age (–0.03; 95% CI: –0.04, –0.01; p < 0.001) and BMI (0.03; 95% CI: 0.01, 0.04; p < 0.001). However, the effect size for insulin is not associated with age (1.19; 95% CI: –1.08, 3.47; p = 0.304) or BMI (–1.90; 95% CI: 4.91, 1.11; p = 0.216; Figures 12 and 13).
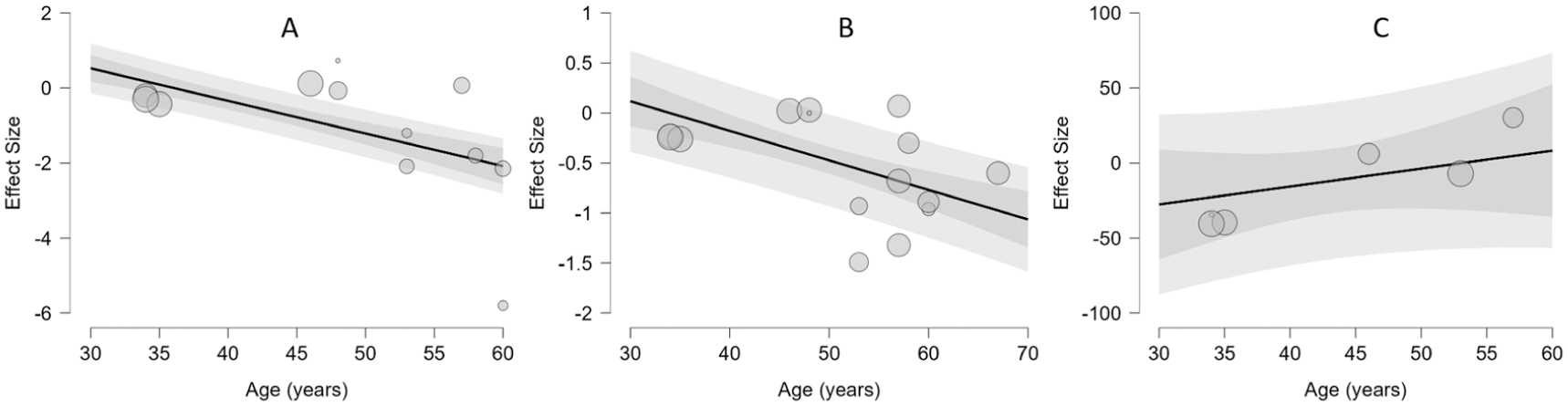
Meta-regression of the association between mean changes in fasting glucose (a), HbA1c (b), and insulin (c) with age.
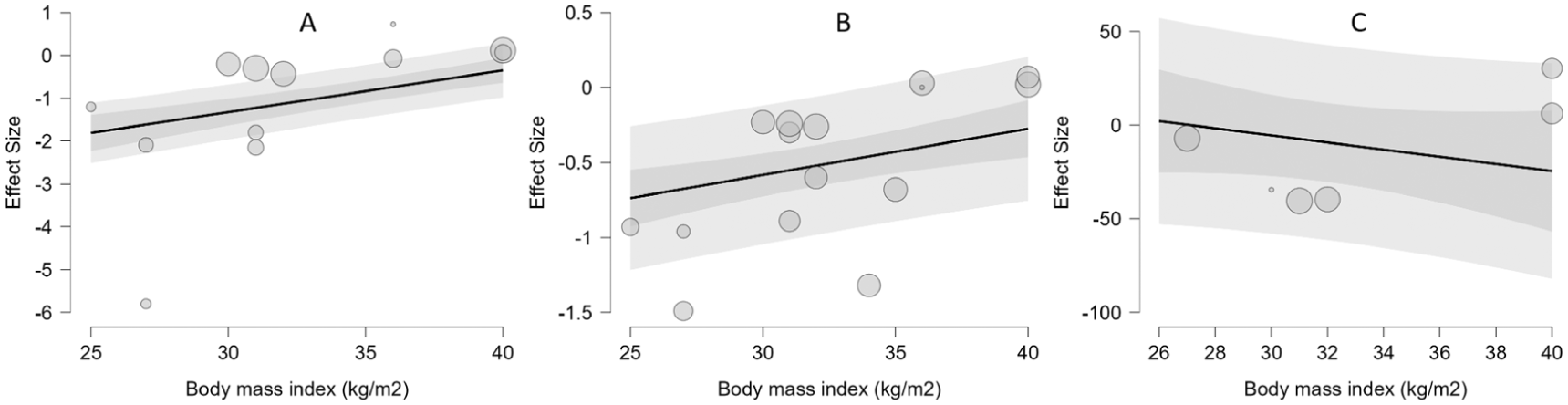
Meta-regression of the association between mean changes in fasting glucose (a), HbA1c (b), and insulin (c) with body mass index.
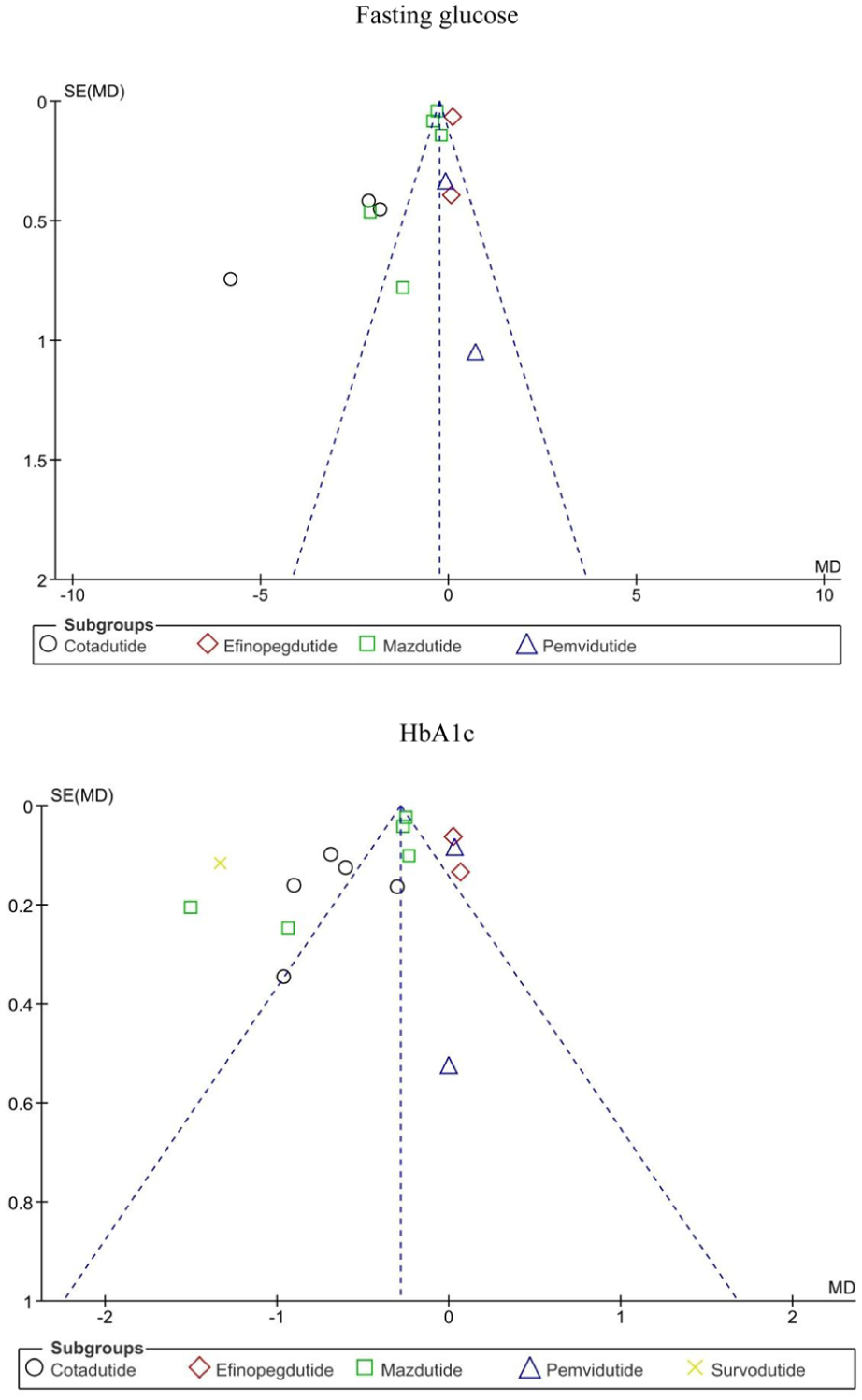
Funnel plots showing publication bias for the effect of GLP-1/glucagon receptor agonists on fasting glucose and HbA1c.
Publication bias
Funnel plots for fasting glucose and HbA1c exhibited an apparent asymmetry following the visual inspection (Figure 14).
Discussion
Dual agonists of the GLP-1/GCGR receptors have emerged as new molecules in GLP-1 pipeline therapeutics. Our findings demonstrated that patients treated with GLP-1/GCGR agonists had a robust effect on glycemic control characterized by decreasing fasting glucose and HbA1c concentrations. However, we did not observe any changes in insulin levels. The beneficial effects on glycemic markers support the consideration of dual agonists as a therapeutic option for type 2 diabetes.
In line with our results, a previous systematic review and meta-analysis reported a significant reduction in both HbA1c and fasting plasma glucose in subjects with type 2 diabetes with or without obesity after treatment with mazdutide and cotadutide. 28 However, it is noted that this meta-analysis only assessed the effect of two GLP-1/GCGR agonists, whilst we additionally evaluated three other drugs: efinopegdutide, pemvidutide, and survodutide. In a network meta-analysis by Liu et al. was observed that mazdutide and survodutide significantly reduced HbA1c, mazdutide decreased fasting plasma glucose, and efinopegdutide did not affect fasting glucose and HbA1c concentrations, 29 findings consistent with our meta-analysis. Another network meta-analysis by Yan et al. revealed that cotadutide, survodutide, and mazdutide reduced HbA1c concentrations, while mazdutide and cotadutide decreased fasting glucose, 30 which is in line with our results. However, it is noteworthy that the former meta-analysis only included 9 studies evaluating the effect of GLP-1/GCGR agonists, including mazdutide, cotadutide, and survodutide, while our study included 14 randomized controlled trials, including cotadutide, efinopegdutide, mazdutide, pemvidutide, and survodutide.
Interestingly, the pooled effect of six studies showed no significant impact on insulin levels after GLP-1/GCGR agonist therapy; however, the subgroup analysis indicated that mazdutide significantly reduces insulin levels. In this regard, it is important to highlight that only two drugs, efinopegdutide and mazdutide, reported outcomes for insulin; therefore, further clinical trials using this class of drugs should be conducted to elucidate the potential effect of GLP-1/GCGR agonists on insulin levels. Additionally, the subanalysis by treatment duration demonstrated that dual agonists decrease insulin levels following more than 12 weeks of treatment, suggesting that the effect on insulin seems to require a longer intervention.
The combination of GLP-1R and GCGR agonism has resulted in a synergistic approach to improve glycemic control by receptor interactions. To date, the innovation of multiagonist novel molecules targeting GLP-1/GCGR receptors (survodutide, pemvidutide, mazdutide, cotadutide, efinopegdutide) or GLP-1/GIP/GCGR receptors (retatrutide, efocipegtrutide) has focused on the development of therapies with added value beyond glycemic control and obesity. 31 The primary mechanisms involve increased insulin secretion and decreased glucagon release in a glucose-dependent manner through the GLP-1 receptor. Simultaneously, GCGR activates energy expenditure and lipid metabolism, which is a positive balance for the hyperglycemic effect of glucagon.32,33 The insulinotropic effect, suppression of glucagon, balanced energy expenditure, weight loss, and improvement in insulin sensitivity, insulin secretion, and lipid profile, represent the main actions of GLP-1/GCGR agonists. 34
As key strengths of our study, we considered a comprehensive and complete search focused on GLP-1R and GCGR dual agonists, a set of results based on the meta-analysis of randomized controlled trials with low risk of bias, and subgroup analyses by specific dual agonist and treatment duration. In counterpart, we identified some limitations that should be mentioned: (1) the meta-analysis showed a high heterogeneity for the outcomes assessed; therefore, our results should be interpreted with caution, (2) insulin levels were only reported in one half of the included studies which in turn prevented a more comprehensive meta-analysis, (3) since few randomized clinical trials were conducted for some dual agonists, such as efinopegdutide and pemvidutide, subgroup analyses were limited, and 4) this study was not registered.
In conclusion, the findings of the present study revealed that treatment with GLP-1/GCGR dual agonists improves fasting plasma glucose and HbA1c concentrations in patients with obesity and type 2 diabetes. However, insulin levels were not modified after the therapy with these dual agonists. Overall, the results highlight the positive synergistic effect of dual agonists for managing type 2 diabetes in patients with obesity. As the development of these drugs is still ongoing, more results from long-term trials are expected to be analyzed.
Footnotes
Author contributions
L.E.S.-M. conceptualized and designed the study, drafted the initial manuscript, and approved the final manuscript as submitted. M.S.-M. carried out the statistical analyses and interpretation of data, critically reviewed the manuscript, and approved the final manuscript as submitted. P.A.-M. drafted the initial manuscript, critically reviewed the manuscript, and approved the final manuscript as submitted. A.S.-G. drafted the initial manuscript, critically reviewed the manuscript, and approved the final manuscript as submitted.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used to support the results of our study are shown within the article.