
Abstract
Artificial intelligence (AI) tools, particularly large language models, are increasingly accessible to medical learners. Early attitudes toward AI may shape how students incorporate these tools into learning and professional development. This study captured first- and second year medical students’ AI familiarity, prior use, and perceptions during orientation week, providing a snapshot of incoming student attitudes. A cross-sectional survey was administered to first- and second year medical students (N = 157) at a single U.S. medical school in August 2024. Data on demographics, AI familiarity, prior use, and perceptions were collected using multiple-choice and five-point Likert scale items. Descriptive statistics, Chi-squared analyses, and Fisher’s exact tests were used to compare responses between cohorts. Of 108 responses, most students reported slight (42.6%) or moderate (37%) AI familiarity. ChatGPT was the most recognized (95.4%) and used (84.3%) tool. First year students were significantly more likely than second year students to have used AI previously, to have used AI during medical school applications, and to plan AI use in medical school (all p < 0.001). Students expressed optimism about AI integration but raised concerns about accuracy (76.9%), clinical thinking (67.6%), and ethics (63%). Over 60% rated ethical AI training as very or extremely important, and 57.4% were uncomfortable with AI-mediated assessment. Pre-clinical students anticipate a growing role for AI in medical education and favor structured, workshop-based ethical training. These findings can inform timely curricular planning as AI technologies continue to evolve.
Introduction
In recent years, artificial intelligence (AI) tools have become increasingly accessible for public use. AI platforms, particularly large language models (LLMs), are now integrated into numerous applications, including Google’s Gemini, Microsoft’s Copilot, and the widely recognized ChatGPT.1–3 Attracting millions of users each month, these technologies have become deeply embedded in modern life, transforming how individuals interact with information and perform tasks. 4
For medical students, AI offers significant advantages, including enhancing evidence-based decision-making, generating differential diagnoses, preparing for Objective Structured Clinical Examinations (OSCEs) and medical knowledge exams, creating presentations, conducting literature reviews, and improving academic writing skills.5–7 Universities are exploring AI-supported approaches to assessments, feedback, intelligent tutoring, personalized learning, and learning analytics. 8 However, challenges remain, including security and privacy concerns, algorithmic bias, unreliable feedback, academic integrity issues, and insufficient institutional guidance. 8 The growing integration of AI in undergraduate medical education (UME) has prompted the development of several frameworks aimed at guiding curricular implementation, though a gap persists between proposed frameworks and actionable integration strategies.9–14
Since 2022, there has been a significant increase in research exploring LLM applications and implications in medical education and healthcare.15–18 Notably, one study demonstrated that ChatGPT could pass the United States Medical Licensing (USMLE) Steps 1 and 2 Examinations, the national board examinations for second- and third-year medical students. This highlights its potential as a valuable study aid for understanding complex concepts and developing critical thinking skills. 19 Despite these capabilities, the widespread availability of such tools necessitates cautious and guided use to address concerns related to ethics, academic integrity, data privacy, and the accuracy of AI-generated content. 20
Several studies have explored how medical students perceive the use of AI tools, finding that students are generally optimistic about AI’s future in healthcare while expressing a desire for training on appropriate use.21,22 While current research has studied the perceptions of pre-clinical students, those who are in their first and second years of medical training and are in the early stages of shaping their professional identity as future physicians, most studies do not specify the timing of data collection within the academic year, making it difficult to contextualize how prior curricular exposure may shape student attitudes. Our study addresses this gap by surveying students during orientation week, a time when incoming first-year students (MS1s) have had no exposure to the medical curriculum, and second year students (MS2s) have completed only 1 year of preclinical training. This timing is significant because it captures baseline attitudes before the academic year’s curricular content, peer influences, and institutional norms have had an opportunity to shape perceptions, providing a clearer window into the preconceptions students bring to medical school.
Additionally, this study investigates whether students used AI tools during the medical school application process, an area that has received limited attention in the literature. As AI tools become more capable and accessible, their use in crafting personal statements, preparing for interviews, and completing secondary applications raises important questions about authenticity, equity, and admissions integrity. Understanding the prevalence and nature of such use is essential for informing admissions policies and applicant guidance.
To provide conceptual context, we reference professional identity formation (PIF), the process by which learners develop the values, norms, and roles associated with being a physician. 23 While PIF serves as a useful lens for interpreting how early attitudes toward AI may relate to students’ evolving sense of professional identity, we note that this framework was not used to drive surgery design or statistical analysis. Rather, it is used to offer a descriptive context for understanding why early-training attitudes matter: the perception students hold at the outset of medical school may influence how they later integrate AI into clinical reasoning and professional practice.
Importantly, this study provides a snapshot of student perspectives at a single point in time, recognizing that attitudes toward AI are evolving as new technologies emerge and as students progress through training. The primary aim of this study was to describe first- and second-year medical students’ familiarity with, prior use of, and perceptions of AI early in training, and to compare findings between the two cohorts (MS1 vs MS2). Furthermore, we investigate whether students used AI for assistance throughout their medical school application process, an area that has not been extensively studied in previous research. The cohort comparison was included because MS1 and MS2 students differ in their exposure to medical education and institutional norms; however, given the cross-sectional design, observed differences should be interpreted as between-group associations rather than evidence of developmental change. A longitudinal follow-up would be needed to make causal or developmental claims. Understanding these perspectives can inform institutional policies on AI use and help educators address the evolving needs of students in an era of rapidly advancing AI technology.
Key Messages
Medical students are increasingly exposed to artificial intelligence (AI) tools and generally report positive attitudes toward their use in education, though concerns about accuracy, ethics, and effects on clinical reasoning persist.
By surveying students during orientation week, this study captures a baseline snapshot of AI perceptions before substantial curricular exposure, revealing high awareness but limited prior undergraduate use, notable AI use during the medical school application process, and greater prior exposure among first-year compared to second-year students.
These findings support early, structured integration of AI education emphasizing ethical use and critical appraisal, and highlight the need for institutional policies addressing AI use in both medical curricular and admission processes.
Methods
Ethical considerations
This study was reviewed and approved by the Institutional Review Board (IRB) at Florida Atlantic University. All procedures involving human participants were performed in accordance with the ethical standards of the institutional research committee and with the Declaration of Helsinki and its amendments. Freely given informed consent to participate in the study was obtained from all individual participants prior to survey completion. Participation was voluntary, and responses were collected anonymously.
Medical school background
The medical school at which the survey was conducted is a community-based medical school in the Southern region of the United States with an approximate class size of 75 students. The school has a traditional, 2-year pre-clinical curriculum, followed by 1 year of required clinical rotations and 1 year of clinical electives. This provides a typical U.S. medical education context for interpreting student perceptions of AI during early training.
Study development
The survey instrument was developed based on a comprehensive literature review on AI in healthcare and medical education.21,22 Content validity was assessed through review by two physician medical educators with expertise in medical education, who evaluated items for relevance, clarity, and alignment with the study objectives. The instrument underwent pilot testing with five medical students from other medical schools from other institutions to assess length and clarity; minor adjustments were made based on their feedback, and their responses were excluded from the final analysis.
The survey was constructed using Qualtrics (Qualtrics International Inc), and administered in English. The final version comprised 35 questions, divided into five sections: demographics, AI familiarity and background, AI use in undergraduate education, AI use during the medical school application cycle, and AI use as a medical student. Demographic questions were multiple-choice and other questions were mostly based on a five-point response scale. The final section included a Likert scale for students to rank their agreement with statements related to AI use in medical school (1 = strongly disagree, 2 = somewhat disagree, 3 = neither agree nor disagree, 4 = somewhat agree, and 5 = strongly agree). All responses were voluntary, no incentives were offered, and the survey was kept open for a duration of 2-weeks in August 2024. The survey instrument is available in Supplemental Digital Appendix 1. Limitations of the survey instrument can be found in the limitations section in the discussion section of this article.
Data analysis
Descriptive statistics were used to summarize and tabulate the frequency of responses across survey items. Subgroup analyses were conducted to explore associations between demographic factors and survey variables. For categorical data, chi-square tests were used to assess associations between variables, such as AI familiarity, past AI use, and perceptions of AI in medical education. When expected cell counts were small, Fisher’s exact tests were used. A p value of <0.05 was considered statistically significant for all tests. Data was analyzed using SPSS version 29.
Because this study was conducted at a single medical school, it is best understood as a case study capturing student perspectives within one institutional context. While this limits generalizability, it allows for detailed examination of AI familiarity, use, and perceptions among early-training medical students at a defined time point.
Results
Demographics
Of the 157 first- and second year medical students (n = 80 and n = 77, respectively), 108 students completed the survey, for a response rate of 69%. The sample was predominantly female (54.6%), aged 23–27 (69.4%), and English-speaking (100%). Most students had undergraduate GPAs between 3.6 and 4.0 (90.7%), and the majority majored in biology or other sciences. The demographic characteristics of the participants are presented in Table 1.
Participant demographic information.
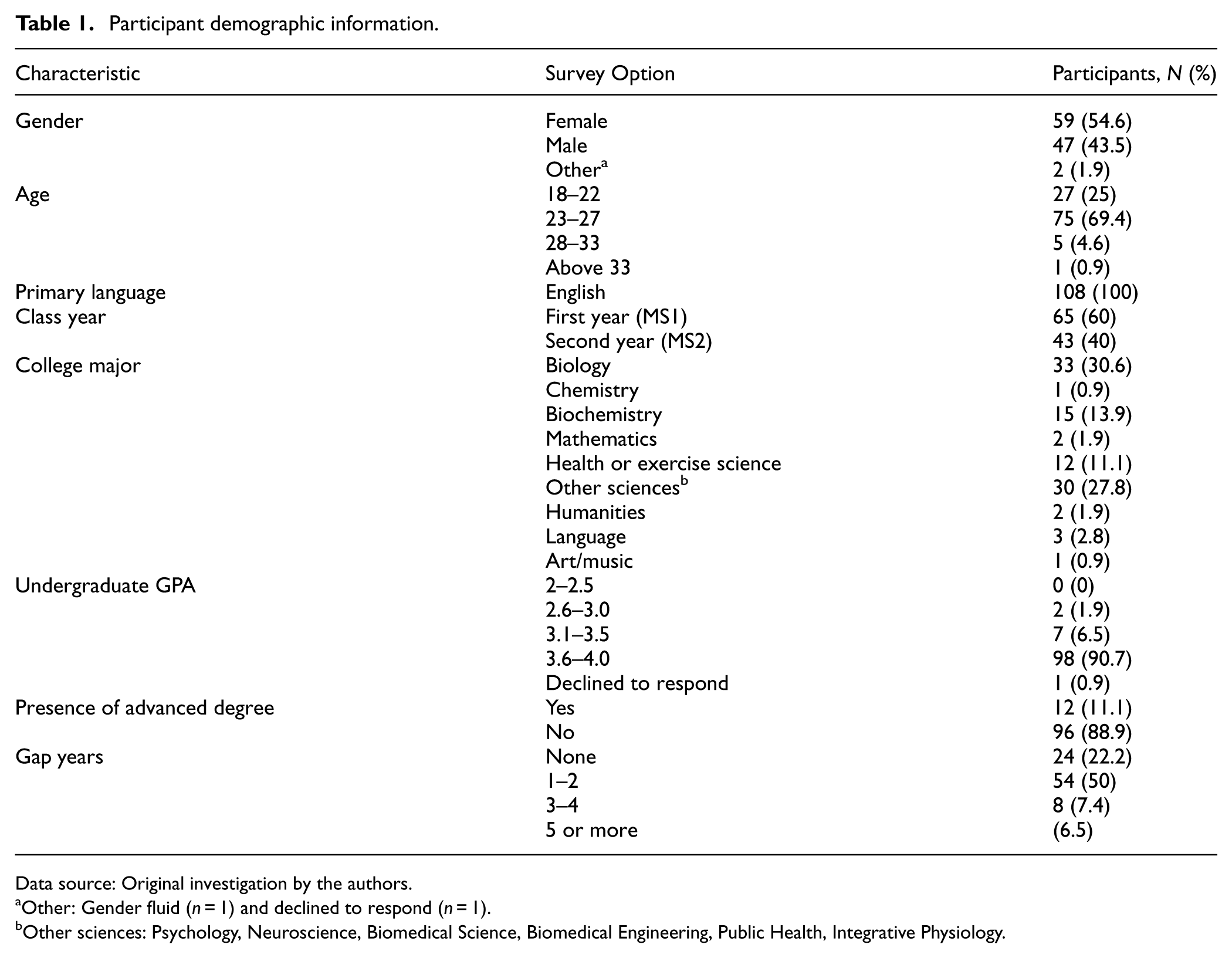
Data source: Original investigation by the authors.
Other: Gender fluid (n = 1) and declined to respond (n = 1).
Other sciences: Psychology, Neuroscience, Biomedical Science, Biomedical Engineering, Public Health, Integrative Physiology.
Familiarity with AI
Most participants reported being slightly (42.6%) or moderately (37%) familiar with AI. ChatGPT was the most recognized and widely used tool (95.4% awareness; 84.3%, prior use). When asked to identify a single preferred AI tool, 80% of students selected ChatGPT. Most students (69.4%) reported that they would not pay for AI tools. Detailed breakdowns of familiarity and tool use are shown in Table 2.
Participant familiarity with AI.
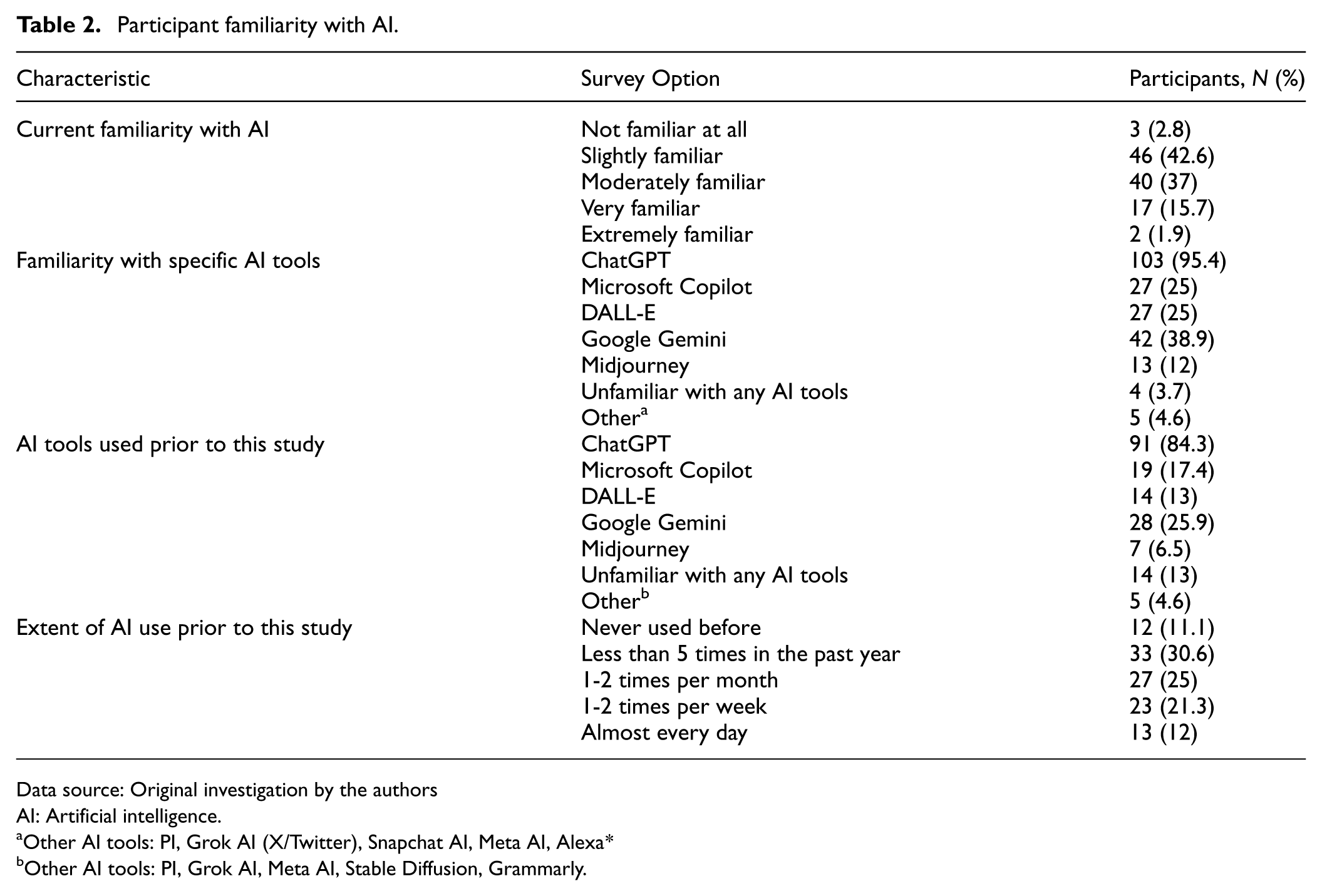
Data source: Original investigation by the authors
AI: Artificial intelligence.
Other AI tools: PI, Grok AI (X/Twitter), Snapchat AI, Meta AI, Alexa*
Other AI tools: PI, Grok AI, Meta AI, Stable Diffusion, Grammarly.
AI use it in undergraduate college
The majority of students (74%) had not used AI during their undergraduate education. Among those who had, the most common uses were for proofreading assignments (19.4%), using AI as a study guide (17.6%), and career guidance, such as resume and interview preparation) (13%).
AI use in medical school applications
Similarly, most students (74.1%) did not use AI for assistance with medical school applications. Among those who did (25.9%), the most common uses were practicing interview questions (20.4%), editing and refining drafts (15.7%), and brainstorming ideas (12%). These findings are detailed in Table 3.
Participant AI use in undergraduate college and medical school applications.
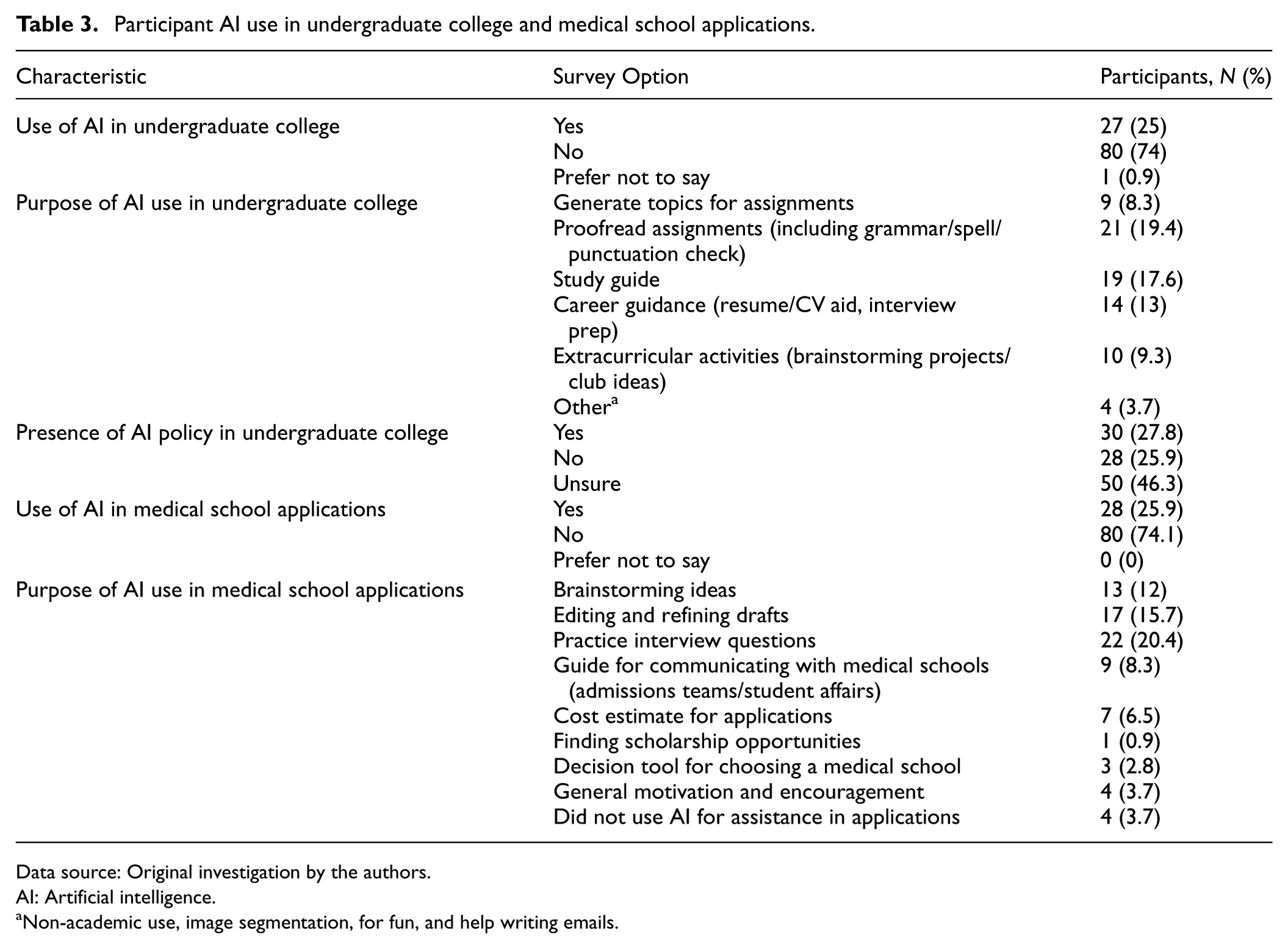
Data source: Original investigation by the authors.
AI: Artificial intelligence.
Non-academic use, image segmentation, for fun, and help writing emails.
AI use in medical school
Students generally viewed AI in medical school positively (45.4%) or neutrally (37%). Nearly half (41.7%) planned to use AI during medical school, most commonly for exam preparation (34.3%), academic writing support (32.4%), and assistance with research projects (29.6%). Approximately half of students (50.9%) believed AI should be integrated into the medical school curriculum, while 35.2% were unsure and 13.9% opposed integration.
Concerns about AI in medical education were concentrated on accuracy and reliability of information (76.9%), potential decreases in clinical thinking skills (67.6%), and ethical issues (63%). Over 60% of students rated ethical AI training as “very” or “extremely” important, and students were more likely to favor optional workshops or seminars (39.8%) over formal coursework (25.9%). Perceptions of AI use in grading and assessments were less favorable, with over 57%% expressing discomfort. Details are presented in Table 4.
Participant AI use in medical school.
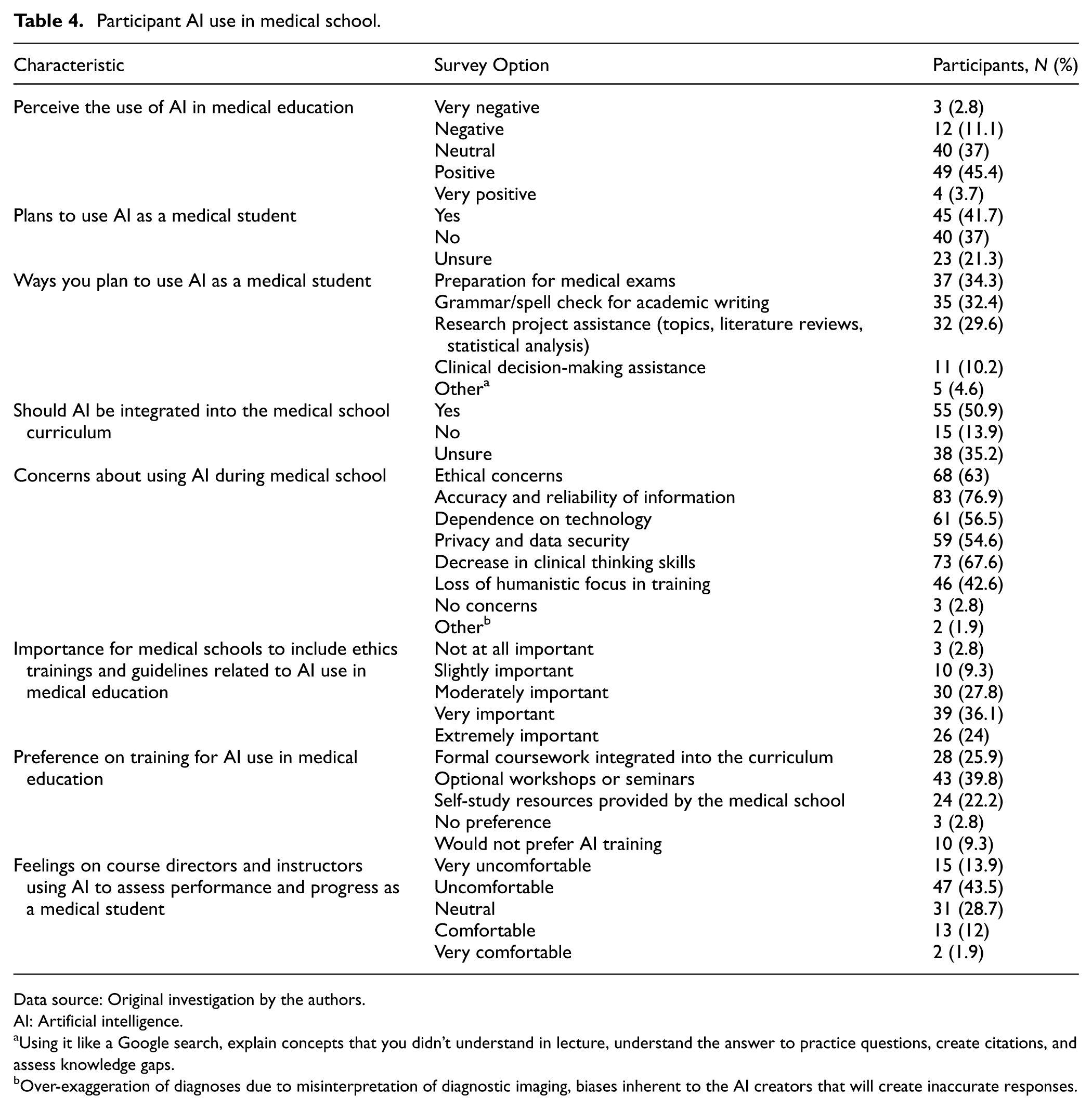
Data source: Original investigation by the authors.
AI: Artificial intelligence.
Using it like a Google search, explain concepts that you didn’t understand in lecture, understand the answer to practice questions, create citations, and assess knowledge gaps.
Over-exaggeration of diagnoses due to misinterpretation of diagnostic imaging, biases inherent to the AI creators that will create inaccurate responses.
Comparisons between first- and second year students
First year students reported more frequent prior AI use, greater use of AI during medical school applications, and stronger intentions to use AI during medical training (all p < 0.001). There were no significant differences between cohorts in overall AI familiarity (p = 0.40), willingness to pay for AI tools (p = 0.40), or perceptions of AI in medical education (p = 0.46). No significant associations were observed by gender or age group.
Perceptions of AI
Students expressed enthusiasm for AI as a support tool but remained cautious about its limitations. Nearly 70% strongly agreed that AI-generated answers must be verified. Many agreed that AI could assist with organization and efficacy, while responses were more neutral regarding its impact on exam performance. A visual summary of responses is shown in Figure 1.
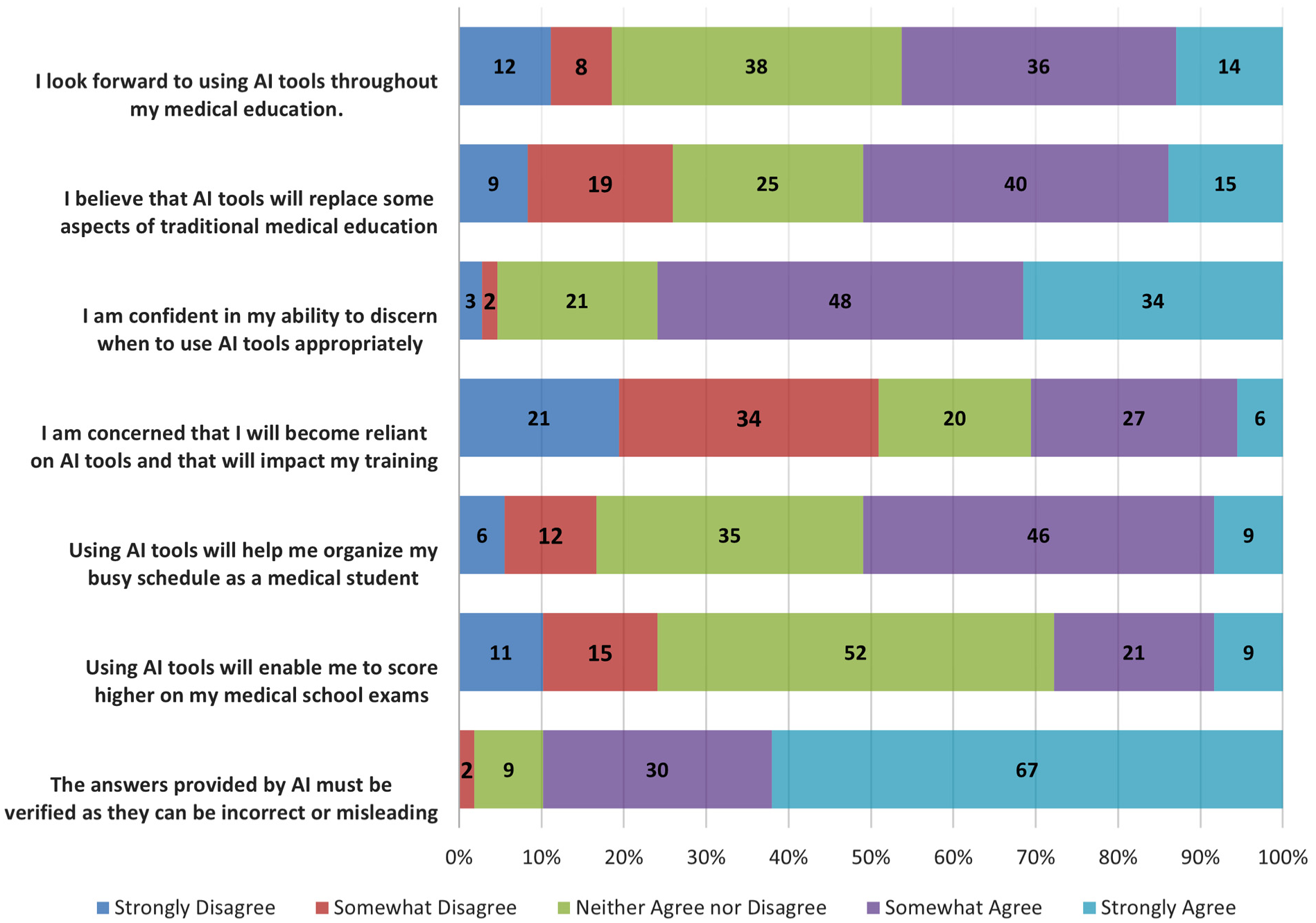
Perceptions of AI among first- and second-year medical students, highlighting attitudes toward AI use in medical education, potential benefits, risks of over-reliance, and the importance of verifying AI-provided information.
Discussion
This study surveyed pre-clinical medical students at the onset of the academic year to capture their familiarity with, prior use of, and perceptions of AI at an early and defined point in training. By collecting data during orientation week, the study provides a baseline snapshot of student attitudes before curricular content, institutional norms, and peer influences have had substantial opportunity to shape perceptions. These findings contribute to the growing global literature on AI perceptions among medical students and healthcare professionals,24,25 adding a perspective from students at the threshold of their medical careers at a U.S. medical school.
These findings represent a snapshot in time, as both AI technologies and medical education practices are evolving rapidly. Students’ perspectives are therefore likely to shift as new tools emerge and training progresses, underscoring the importance of continued research to track how attitudes and experiences change alongside technological advancement.
AI use in undergraduate education and medical school applications
While prior studies focus on medical students’ views and clinical usage of AI,26,27 this survey also examined AI use during undergraduate education and the medical school application process. The finding that 74% of students had not used AI during undergraduate education likely reflects the recency of widespread LLM availability; this proportion may decrease substantially in future cohorts as AI tools become standard in higher education.
The use of AI in medical school applications, which was reported by approximately 26% of students, represents a potentially novel contribution of this study. Students who used AI during the application process most commonly did so to practice interview questions, edit and refine drafts, and brainstorm ideas. As AI tools become increasingly capable of generating polished written content, their use in crafting personal statements and secondary applications raises important questions about authenticity, equity, and admissions integrity. Students with greater access to or familiarity with AI tools may gain an advantage in the application process, potentially widening existing disparities. These findings underscore the need for admissions committees to establish clear guidelines, which have been established in recent years, regarding the acceptable use of AI in application materials, ensuring transparency while maintaining ethical standards. 28
Cohort differences
First-year students reported more frequent prior AI use, greater use of AI during medical school applications, and stronger intentions to use AI during medical training compared to second-year students. These differences likely reflect the rapid increase in AI accessibility between the two cohorts’ application cycles (2022 vs 2023), rather than a developmental effect of medical education. Importantly, the cross-sectional design cannot disentangle cohort effects from temporal trends in AI adoption, and these between-group differences should not be interpreted as evidence that medical school exposure changes AI attitudes. A longitudinal follow-up of the same cohort would be necessary to make developmental claims. Nevertheless, the pattern suggests that successive incoming classes may arrive with progressively greater AI experience, which has practical implications for how medical schools orient and guide new students regarding AI use.
There were no significant differences between cohorts in overall AI familiarity, willingness to pay for AI tools, or perceptions of AI in medical education, suggesting that certain baseline attitudes may be relatively stable across early-training cohorts regardless of prior AI exposure.
AI integration and curriculum expectations
Approximately half of students (50.9%) believed AI should be integrated into the medical school curriculum, while 35.2% were unsure. Several factors may account for this discrepancy. The survey was administered during orientation week, before students had experienced the demands of the medical curriculum and before they may have recognized the potential utility of AI as a learning tool. Additionally, the question wording, institutional context, and the relatively homogeneous single-site sample may have influenced responses. The 69% response rate also introduces the possibility that non-respondents held different views, which could have shifted the overall proportion in either direction.
Despite this, students expressed clear interest in AI training, with over 60% rating ethical AI training as “very” or “extremely” important and a preference for optional workshops or seminars over formal coursework. Concerns about AI were concentrated on accuracy and reliability (76.9%), potential decreases in clinical thinking skills (67.6%), and ethical issues (63%). These concerns are consistent with the broader literature, which has consistently identified accuracy, over-reliance, and ethics as primary student concerns.9,29
Students’ discomfort with AI-mediated grading and assessment (57.4% uncomfortable or very uncomfortable) is also noteworthy. This finding may reflect an understanding of current AI limitations in evaluating nuanced clinical reasoning and humanistic competencies, and suggests that any institutional adoption of AI in assessment should be accompanied by transparency about how such tools are used and validated.
Frameworks for AI integration
Several frameworks have been proposed for integrating AI into medical education curricula, though a gap persists between proposed frameworks and actionable implementation strategies.9,30 Recent scoping reviews have mapped AI competencies across domains, including AI ethics, critical appraisal of AI outputs, clinical applications, and foundational AI literacy. 31 Curricular models such as the DATA-MD curriculum have demonstrated that structured AI training can improve trainees’ knowledge and attitudes. 32 The Macy Foundation Innovation Report has further synthesized the landscape of AI in medical education across admissions, teaching, assessment, and research domains.33,34
Based on the findings of this study, an implementable approach for institutions with similar profiles could include: (1) orientation-week modules introducing AI literacy and institutional AI policies, (2) optional workshops on ethical AI use and critical appraisal of AI-generated content integrated throughout the preclinical years, and (3) periodic reassessment of student attitudes and AI use patterns to inform iterative curricular adjustments. This approach aligns with students’ expressed preference for workshop-based training and addresses the identified concerns about accuracy, ethics, and over-reliance.
Professional identity formation
From the perspective of PIF, the orientation-week timing captures students at a point when they are beginning to internalize professional norms such as accountability for accuracy, ethical conduct, and transparency. 23 Students’ strong emphasis on verifying AI-generated content (nearly 70% strongly agreed) and their discomfort with AI-mediated assessment may reflect early boundary-setting around trust and responsibility in an AI-augmented learning environment. However, this interpretation is offered as a descriptive observation rather than an empirically tested relationship, as the study was not designed to measure PIF constructs directly. Future research incorporating validated PIF instruments could more rigorously examine how AI attitudes relate to professional identity development.
Limitations
This study has several limitations that should be considered when interpreting the findings.
First, the study was conducted at a single community-based medical school in the Southern United States with a relatively homogenous sample (100% English-speaking, 90.7% with undergraduate GPAs of 3.6–4.0). This limits the generalizability of findings to institutions with different educational contexts, curricular structures, student demographics, or geographic settings. Students at institutions with existing AI curricular, greater technological infrastructure, or more diverse student bodies may hold substantially different attitudes.35,36
Second, the cross-sectional design captures associations at a single time point and cannot establish causal or developmental relationships. Observed differences between MS1 and MS2 students may reflect temporal trends in AI adoption rather than effects of medical education exposure. A longitudinal design following the same cohort over time would be needed to assess how attitudes evolve during training.
Third, the 69% response rate, while within the range reported for medical education surveys, introduces the possibility of nonresponse bias. Students who chose not to participate may have differed systematically from respondents in their AI familiarity, attitudes, or usage patterns. For example, students less interested in AI may have been less motivated to complete the survey, potentially inflating positive attitudes in the sample.
Fourth, the survey instrument was developed de novo based on a literature review and underwent content validation through expert review and pilot testing. However, formal psychometric testing was not conducted: no internal consistency analysis (e.g. Cronbach’s alpha), exploratory factor analysis, or test-retest reliability assessment was performed. Items were not adapted from previously validated instruments, which may limit comparability with other studies and introduce uncertainty about the measurement properties of the Likert scales used. These limitations should be considered when interpreting the strength of associations reported.
Fifth, the survey did not include Claude (Anthropic) among the listed AI tools, despite its growing usage nationally. This omission may have underestimated students’ familiarity with and use of non-ChatGPT LLMs.
Finally, given the rapid pace of AI development, these findings represent a snapshot that may not reflect current or future student attitudes. Expanding this work to a longitudinal design, such as by resurveying the same students at later time points, and also to multiple institutions, would substantially strengthen the evidence base. Such studies could also incorporate validated instruments for measuring PIF and AI literacy to enable more rigorous analysis.
Conclusion
This study captured the perspectives of first- and second-year medical students on AI at the onset of the academic year, providing a baseline snapshot of attitudes before substantial curricular exposure. First-year students reported greater prior AI use and stronger intentions to use AI during medical training compared to second-year students, likely reflecting the rapid increase in AI accessibility. Students expressed interest in AI integration and training, particularly through optional workshops focused on ethical use, while also raising concerns about accuracy, over-reliance, and the use of AI in assessment. These findings suggest that medical schools should consider establishing clear AI usage policies, providing structured training opportunities that address both the capabilities and limitations of AI tools, and periodically reassessing student needs as AI technologies continue to evolve.
Footnotes
Ethical considerations
This study was approved by the Institutional Review Board at Florida Atlantic University.
Consent to participate
Informed consent to participate was obtained electronically from all participants prior to enrollment in the study.
Consent for publication
Informed consent to publish was obtained from all participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data can be made available upon reasonable request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.