
Abstract
This meta-analysis systematically evaluates the clinical efficacy and safety of microcatheter-assisted trabeculotomy in glaucoma treatment. We searched databases including PubMed, Embase, Web of Science, Wiley Library, China National Knowledge Infrastructure, Wanfang, and VIP. Four randomized controlled trials and 3 case–control studies, totaling 460 patients, were included. Data were analyzed using Stata/MP18 (StataCorp LLC, College Station, TX, USA) to calculate risk ratio, standardized mean difference (SMD), and 95% confidence interval (CI). It showed a significant short-term (3–6 months) reduction in intraocular pressure (IOP) with microcatheter-assisted trabeculotomy compared to control procedures (SMD = −0.39, 95% CI: −0.72 to −0.05, p = 0.01). Subgroup analysis suggested a significant short-term benefit in adults (SMD = −0.71, 95% CI: −1.37 to −0.05, p = 0.04), but not in pediatric patients. For long-term IOP (>1 year), the overall reduction was statistically significant (SMD = −0.46, 95% CI: −0.89 to −0.04, p = 0.03), with a significant benefit observed in adults (SMD = −1.03, 95% CI: −1.41 to −0.64, p < 0.01) but not in pediatric patients. No significant differences were found in postoperative success rates, number of antiglaucoma medications, or the incidence of ciliary detachment. Current evidence suggests that microcatheter-assisted trabeculotomy provides significant IOP-lowering effects in both the short and long-term overall, with a significant benefit in adults, whereas the benefit in children remains unclear. Its effects on surgical success rates and medication burden remain inconclusive. These findings support its potential as an effective surgical option, but highlight the need for further high-quality, long-term studies.
Introduction
Glaucoma, characterized by progressive optic nerve damage and associated visual field defects, is a chronic and multifactorial disease.1,2 Pathophysiologically, glaucoma involves elevated intraocular pressure (IOP), imbalanced optic nerve blood flow dynamics, decreased neuroprotective factors, and abnormalities in several biochemical and molecular signaling pathways.3,4 IOP is widely recognized as the most significant modifiable risk factor. 5 Despite this, there is a subset of patients who experience optic nerve damage even within normal IOP ranges, a condition commonly known as normal-tension glaucoma, suggesting that the etiology of glaucoma is not solely limited to IOP factors.6,7 According to the World Health Organization, glaucoma is the second leading cause of blindness worldwide after cataract. By 2040, an estimated 110 million people worldwide will be affected by this disease, resulting in a significant burden on patients’ lives and increasing healthcare costs.8,9 Glaucoma treatment has always been a challenging issue, particularly in terms of IOP control and management of complications. In addition, glaucoma involves multiple aspects such as oxidative stress, inflammatory responses, and cellular apoptosis, adding to the complexity of treatment.10,11
Pharmacological treatment is usually considered the first line of treatment for glaucoma. However, due to issues such as medication adherence, local or systemic side effects, and diminishing efficacy over time, surgical intervention is often required.12,13 Microcatheter-assisted trabeculotomy, as a novel surgical technique, involves the implantation of a microcatheter to create a stable and permanent aqueous outflow pathway, effectively lowering IOP.14–16 Compared to traditional trabeculotomy, microcatheter-assisted trabeculotomy offers advantages such as shorter operative time, minimal trauma, faster recovery, and fewer complications.17,18 These benefits are due to the design and material properties of the microcatheter, which reduce resistance to aqueous outflow while minimizing the risk of infection and scarring.19,20
Although numerous studies have investigated microcatheter-assisted trabeculotomy in recent years, no consensus has been reached on its clinical efficacy and safety.14,15,17,18,20–22 This is mainly due to small sample sizes, variations in study design, and inconsistent outcome measures. Therefore, a comprehensive and rigorous meta-analysis is crucial, as it can integrate existing scattered evidence, address issues of inadequate sample size and study heterogeneity through statistical methods, and provide more reliable and precise evidence for clinical decision-making. Therefore, the aim of this study is to systematically evaluate the efficacy and safety of microcatheter-assisted trabeculotomy in the treatment of glaucoma using a meta-analysis approach to provide clinicians with scientific, objective and comprehensive treatment references.
Materials and methods
Literature sources
The data for this meta-analysis came mainly from several medical and biomedical databases, including PubMed, Embase, Wiley Library, Web of Science, China National Knowledge Infrastructure (CNKI), Wanfang, and VIP databases. To ensure comprehensive literature coverage, we also searched web-based sources and tracked references from included studies, with the search limited to English and Chinese publications from inception to January 2025.
Search strategy
This meta-analysis was conducted in accordance with the PRISMA guidelines. The search strategy was developed using keywords and subject headings related to “microcatheter,”“trabeculotomy,” and “glaucoma.” The complete search strategies for all databases (PubMed, Embase, Web of Science, Wiley Library, CNKI, Wanfang, and VIP) are provided in Supplemental Material to ensure transparency and reproducibility.
Inclusion and exclusion criteria
Inclusion criteria
Literature inclusion followed the PICOS principles: (1) Population (P): Patients diagnosed with glaucoma, including both initial diagnoses and recurrent cases. (2) Intervention (I): Microcatheter-assisted trabeculotomy. (3) Comparison (C): Placebo or conventional treatment. (4) Outcomes (O): ① Short-term IOP; ② long-term IOP; ③ postoperative success rate; ④ glaucoma medication use; ⑤ ciliary detachment. (5) Study design (S): Randomized controlled trials and case-control studies.
Exclusion criteria
(1) Non-original studies, such as reviews, conference abstracts, etc.; (2) duplicate studies; (3) incomplete or unclear data; (4) single-arm study
Screening and data extraction
Two independent reviewers (Zhang and Chen) simultaneously performed manual screening according to established inclusion and exclusion criteria. Initially, they conducted a preliminary review of titles and abstracts of all potentially relevant literature retrieved through the initial search. Articles clearly unrelated to the research topic or not meeting the inclusion criteria were excluded. Subsequently, the remaining articles underwent full-text review to further determine their eligibility for inclusion. Any discrepancies between the reviewers regarding the inclusion or exclusion of articles were resolved through arbitration by a third reviewer. After finalizing the literature selection, the same two independent reviewers manually extracted data, including baseline data (such as author, publication year, study type, sample size) and outcome measures.
Assessment of literature quality
To ensure accuracy and consistency, different tools were employed to assess the quality of the included randomized controlled trials (RCTs) and case-control studies. The Cochrane Collaboration’s Risk of Bias (ROB2) tool was used for RCTs. The ROB2 tool assesses five specific domains: the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. 23 The judgment categories (low risk, some concerns, high risk) for each domain and the overall assessment are defined by the ROB2 tool’s official criteria. 23 Studies were rated as high quality if all domains were judged as low risk, moderate quality if one or more domains raised some concerns, and low quality if one or more domains were judged as high risk. For case-control studies, quality was assessed using the Newcastle-Ottawa Scale (NOS). The NOS awards a maximum of 9 points across three domains: selection (4 points), comparability (2 points), and exposure (3 points). Based on established methodological convention, studies with scores of 7–9, 4–6, and 0–3 points were classified as high, moderate, and low quality, respectively. 24 To ensure objectivity, the quality assessment was performed independently by two reviewers. Any discrepancies were resolved through discussion or, if necessary, by consultation with a third senior reviewer.
Statistical methods
Stata/MP18 (StataCorp LLC, College Station, TX, USA) was used for all data analyses. Relative risk (RR) and its 95% confidence interval (CI) were calculated for dichotomous variables, and standardized mean difference (SMD) and its 95% CI for continuous variables. Heterogeneity among the included studies will be assessed using the I2 statistic and the Cochran’s Q-test. Following widely accepted guidelines in meta-analysis methodology, an I2 value greater than 50% (representing moderate to high heterogeneity) or a Cochran’s Q-test p-value less than 0.10 will be considered indicative of significant statistical heterogeneity. 25 In such cases, a random-effects model (DerSimonian and Laird method 26 ) will be applied to provide a more conservative estimate; otherwise, a fixed-effects model (Mantel-Haenszel method 27 ) will be used. To explore potential sources of heterogeneity, a subgroup analysis will be performed based on age categories. Publication bias analysis was performed only for outcomes that included at least five studies. Funnel plots and Egger’s and Begg’s tests 28 were used to assess publication bias. Asymmetry of the funnel plots or a statistically significant result (p < 0.05) in either Egger’s or Begg’s test was considered indicative of publication bias. A two-sided p-value of <0.05 was considered statistically significant for all primary outcome analyses. For outcomes with significant heterogeneity, a leave-one-out sensitivity analysis was performed by sequentially excluding each individual study and comparing the pooled estimates with the overall pooled result.
Results
Literature search results
After completion of the literature search, a total of 414 relevant articles on the use of microcatheter-assisted trabeculotomy in the treatment of glaucoma were retrieved. Among these, 279 were in Chinese and 135 were in English. Among them, 308 articles were excluded after initial screening due to their irrelevance to the research topic or duplicate publication. The remaining 106 articles were read in full and assessed in detail, resulting in the exclusion of 7 articles for reasons including lack of control group, missing key data, review articles and case reports. Finally, seven studies14,15,17,18,20–22 were included in the meta-analysis, as shown in Figure 1.
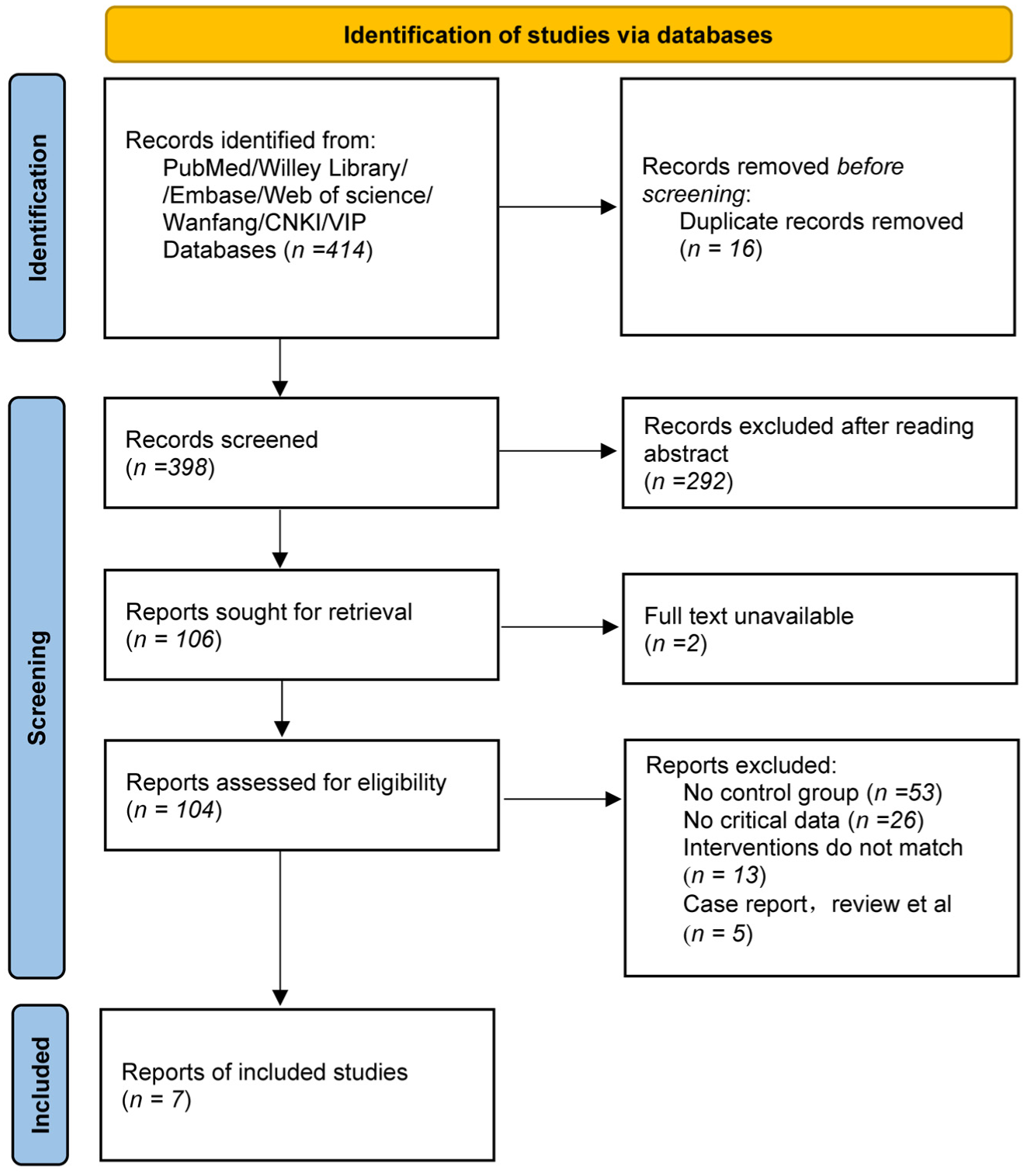
Flow diagram of the study identification, screening, and inclusion process for the systematic review and meta-analysis, according to PRISMA guidelines.
Characteristics and quality of included studies
This meta-analysis included a total of 4 RCTs and 3 case-control studies, involving a total of 460 patients, as shown in Table 1. The quality assessment showed that the majority of the included RCTs were of moderate to high quality (Table 2). In the case-control studies, the included research had NOS scores ranging from 5 to 6 points. Three studies were of moderate quality (Table 3). Overall, the incorporated studies demonstrated relatively sound methodology, with good reliability and representativeness.
General information of included literature.
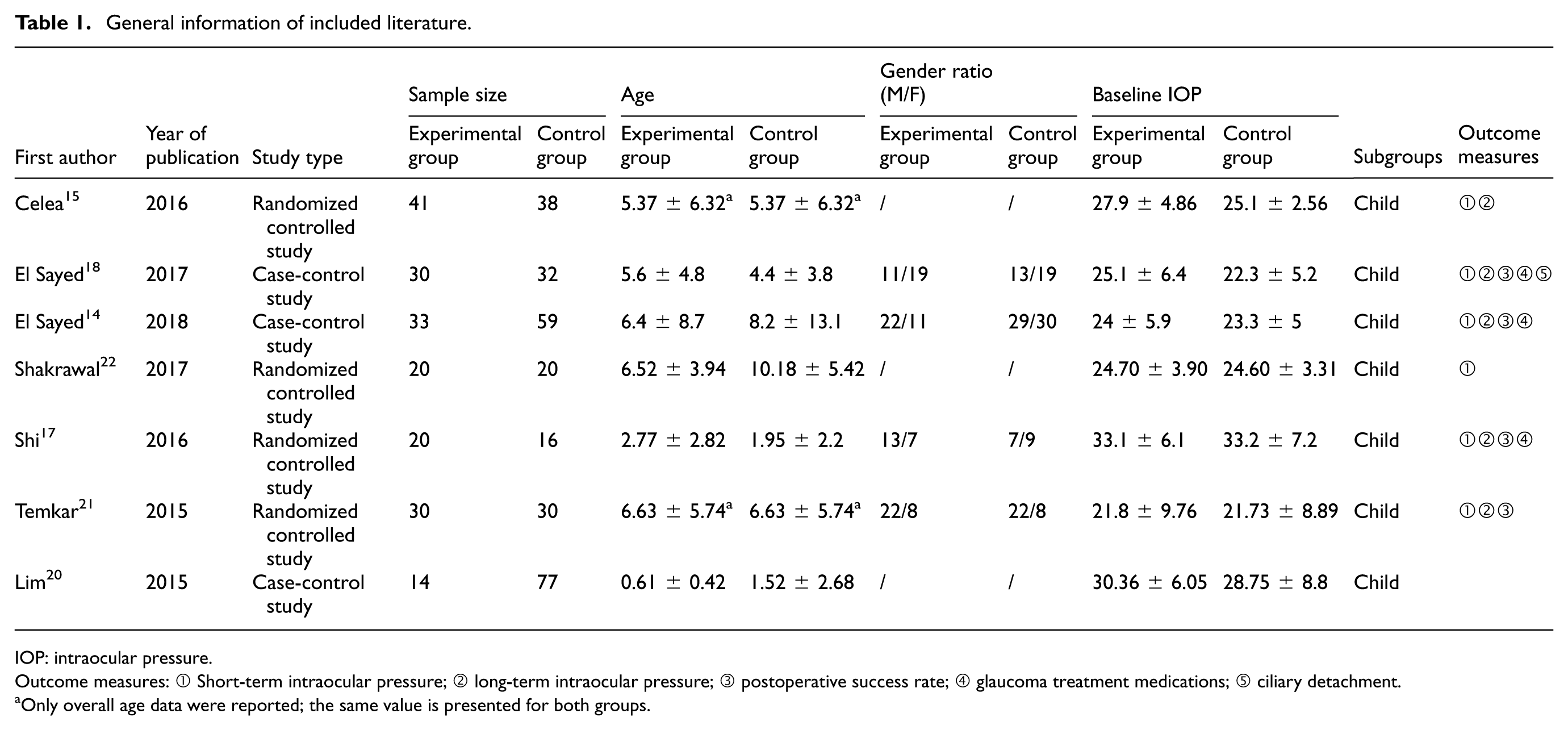
IOP: intraocular pressure.
Outcome measures: ① Short-term intraocular pressure; ② long-term intraocular pressure; ③ postoperative success rate; ④ glaucoma treatment medications; ⑤ ciliary detachment.
Only overall age data were reported; the same value is presented for both groups.
Quality assessment of RCTs: ROB2 tool.
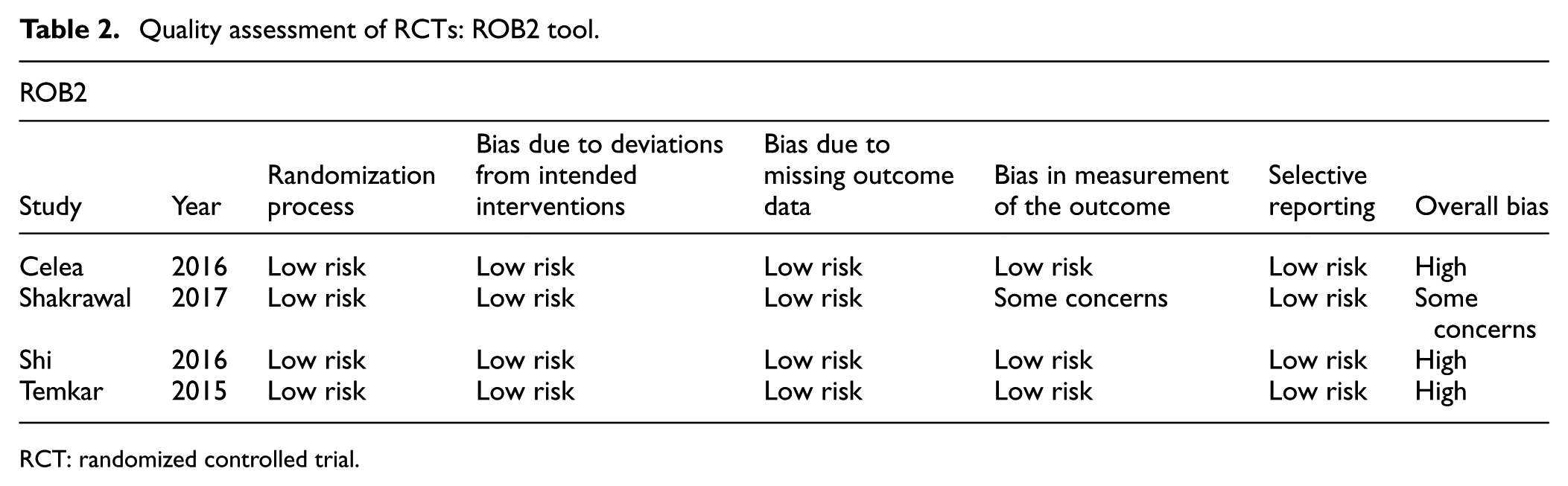
RCT: randomized controlled trial.
Quality assessment of case-control studies: NOS.
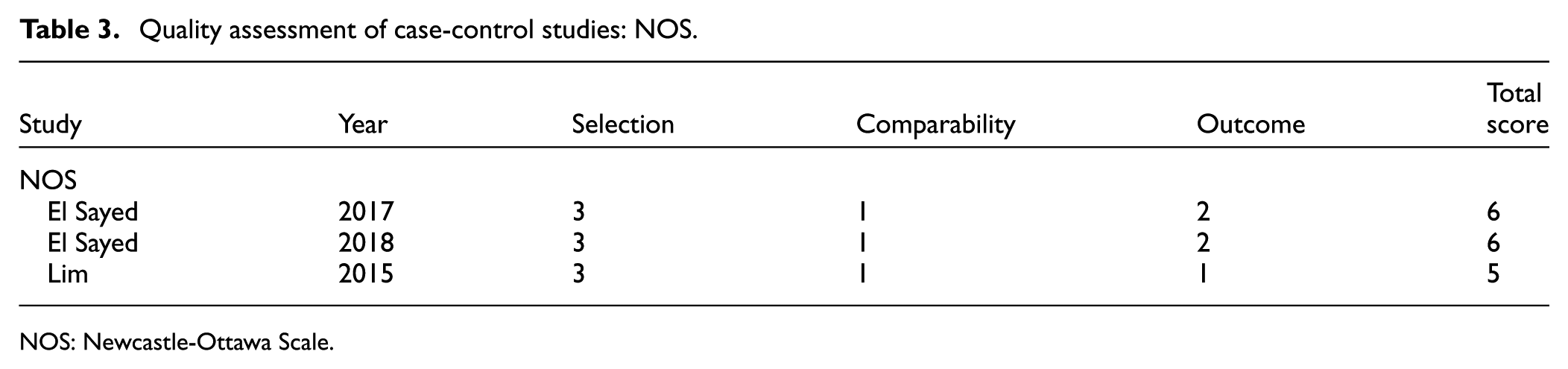
NOS: Newcastle-Ottawa Scale.
Meta-analysis results
Short-term IOP (3–6 months)
To evaluate the effect of microcatheter-assisted trabeculotomy on short-term IOP, we performed a meta-analysis of all included studies, including adult and pediatric subgroups. The meta-analysis results showed that a total of seven studies were included in the analysis, with I2 = 65.94% >50%, and a random-effects model was adopted. The results indicated that at 3–6 months postoperatively, the SMD of IOP in the microcatheter-assisted trabeculotomy group was 0.39 lower (SMD = −0.39) than that of the control group (95% CI: −0.72, −0.05, p = 0.01). Subgroup analysis revealed that the adult subgroup included one study, showing a significant short-term IOP reduction in the adult subgroup (SMD = −0.71, 95% CI: −1.37, −0.05, p = 0.04). The pediatric subgroup included six studies with I2 = 69.22% >50%, and the result was not significant. The between-group difference had a p-value of 0.35, suggesting no significant difference in the short-term effect of microcatheter-assisted trabeculotomy on IOP between adults and children, as shown in Figure 2.
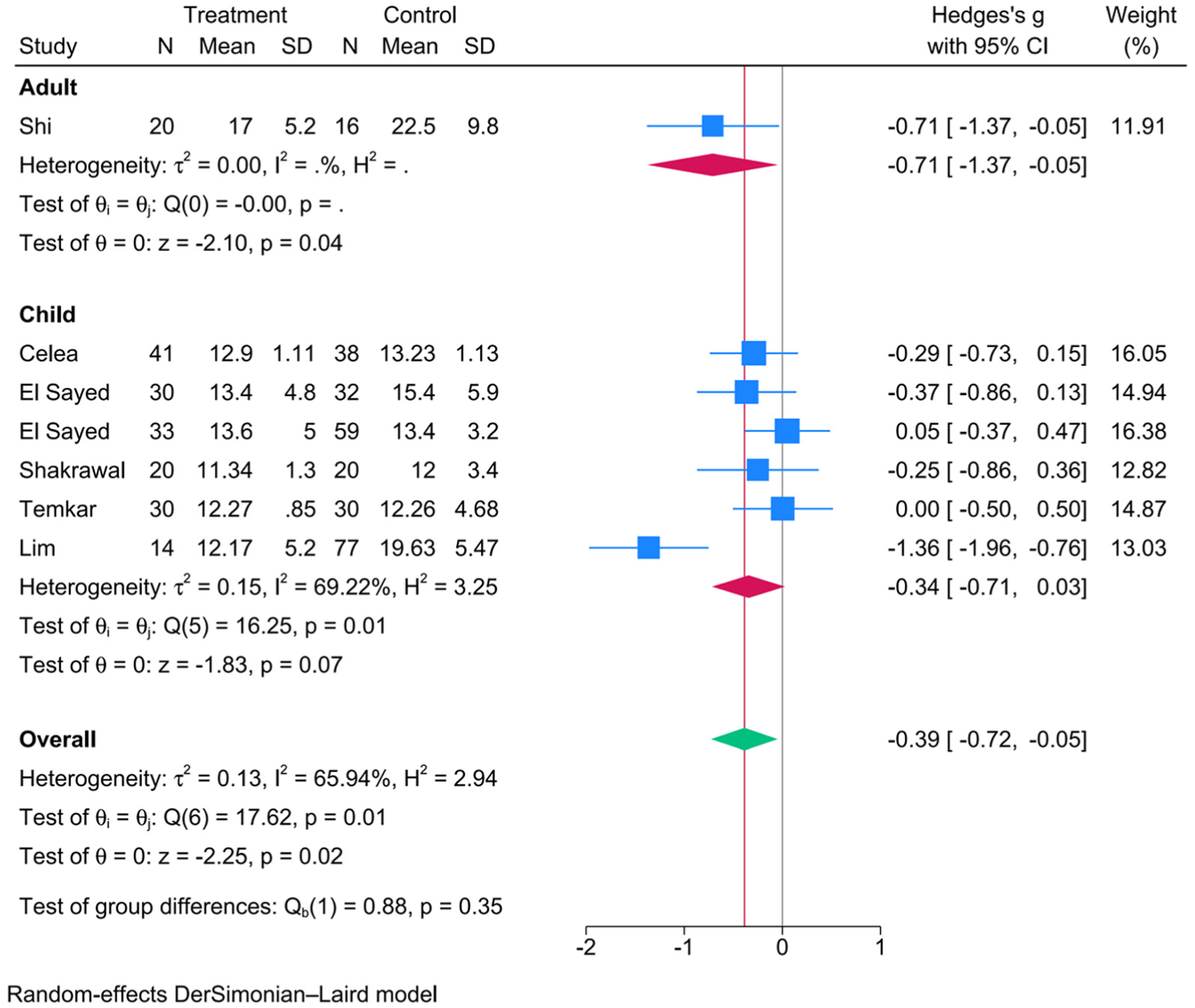
Forest plot comparing short-term IOP at 3–6 months postoperatively between microcatheter-assisted trabeculotomy and control surgery. The SMD was pooled using a random-effects model. Subgroup analyses for adult and pediatric patients are presented.
Long-term IOP (>1 year)
To assess the effect of microcatheter-assisted trabeculotomy on long-term IOP, we performed a meta-analysis including both adult and pediatric subgroups from all eligible studies. The meta-analysis results demonstrated that a total of five studies were included for analysis, with I2 = 72.12% > 50%, leading to the application of a random-effects model. The results showed that the SMD in IOP was 0.46 lower in the microcatheter-assisted trabeculotomy group compared to the control group (95% CI: −0.89 to −0.04, p = 0.03), indicating a statistically significant difference. Subgroup analysis showed a significant reduction in long-term IOP in the adult subgroup (two studies; SMD = −1.03, 95% CI: −1.41 to −0.64, p < 0.01), with I2 = 0.00%; the pediatric subgroup (three studies) showed no significant reduction (SMD = −0.15, 95% CI: −0.42 to 0.12, p = 0.26), also with I2 = 0.00%. After subgrouping, heterogeneity was eliminated, and the between-group difference was statistically significant (p < 0.01), suggesting that age was the major source of heterogeneity for long-term IOP outcomes. Further meta-regression analysis showed a z-value of 3.64 (p = 0.0003), indicating that age group was a significant source of heterogeneity for long-term IOP outcomes (Figure 3).
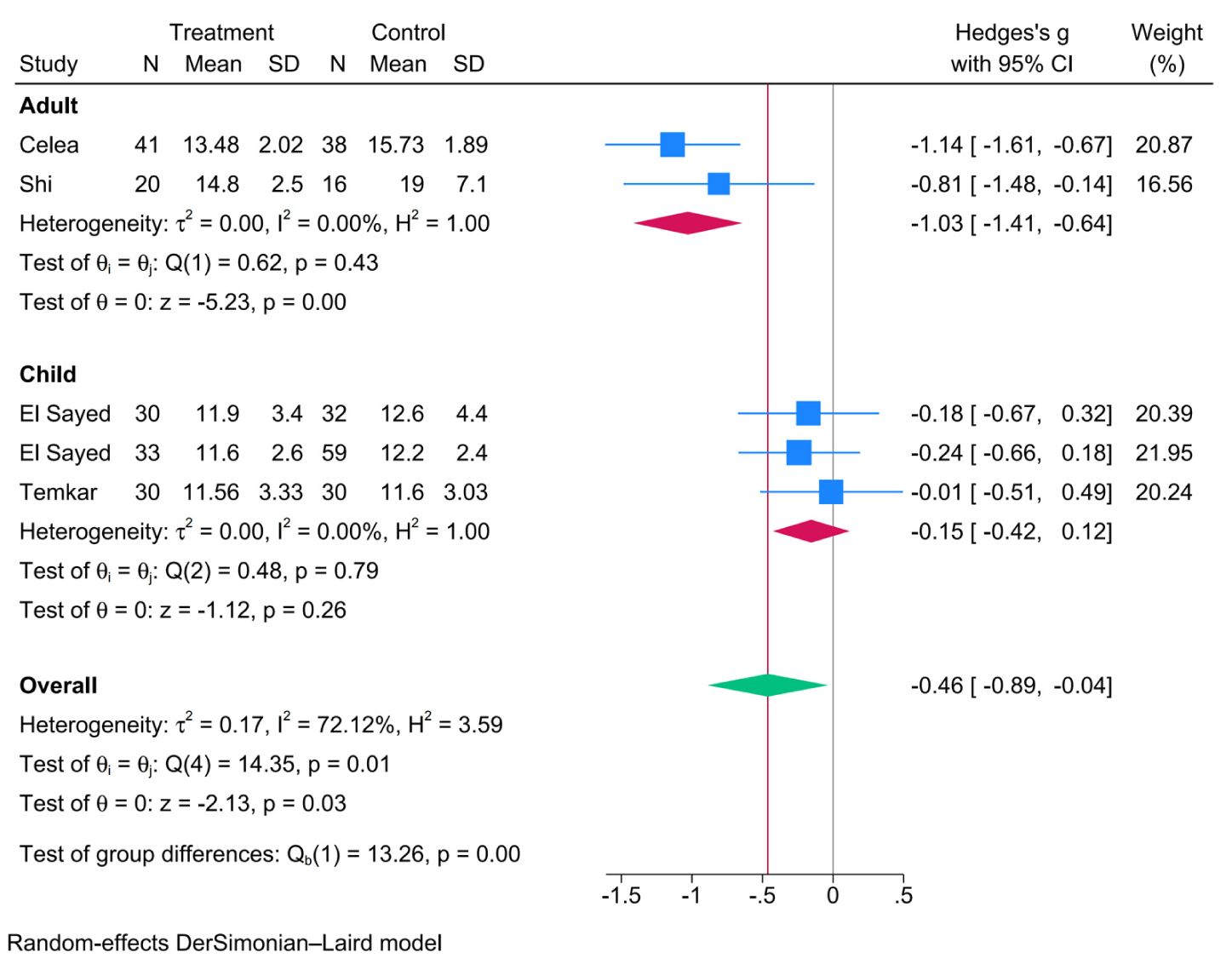
Forest plot comparing long-term IOP at over 1 year postoperatively between microcatheter-assisted trabeculotomy and control surgery. The SMD was pooled using a random-effects model. Subgroup analyses for adult and pediatric patients are presented.
Postoperative success rate
To evaluate the impact of microcatheter-assisted trabeculotomy on postoperative success rates, a meta-analysis was conducted on the four included studies. Heterogeneity analysis showed that under a fixed-effects model, I2 = 50.84%, indicating substantial heterogeneity; therefore, a fixed-effects model was not applicable. Moreover, the pooled estimate crossed the line of no effect, suggesting a non-significant result. Consequently, a random-effects model was used to obtain a more robust estimate, under which I2 = 38.42%—although below 50%, this model better reflects clinical applicability. The results showed a logRR of 0.09 [95% CI: −0.09, 0.28], which was not statistically significant. In the adult subgroup, three studies were included in the analysis, yielding a logRR of 0.36 [95% CI: −0.04, 0.77], which was also not statistically significant. The pediatric subgroup comprised three studies, with a logRR of 0.03 [95% CI: −0.13, 0.18]. Intergroup comparison revealed no significant difference in postoperative success rates between the two treatment groups (p = 0.13), as shown in Figure 4.
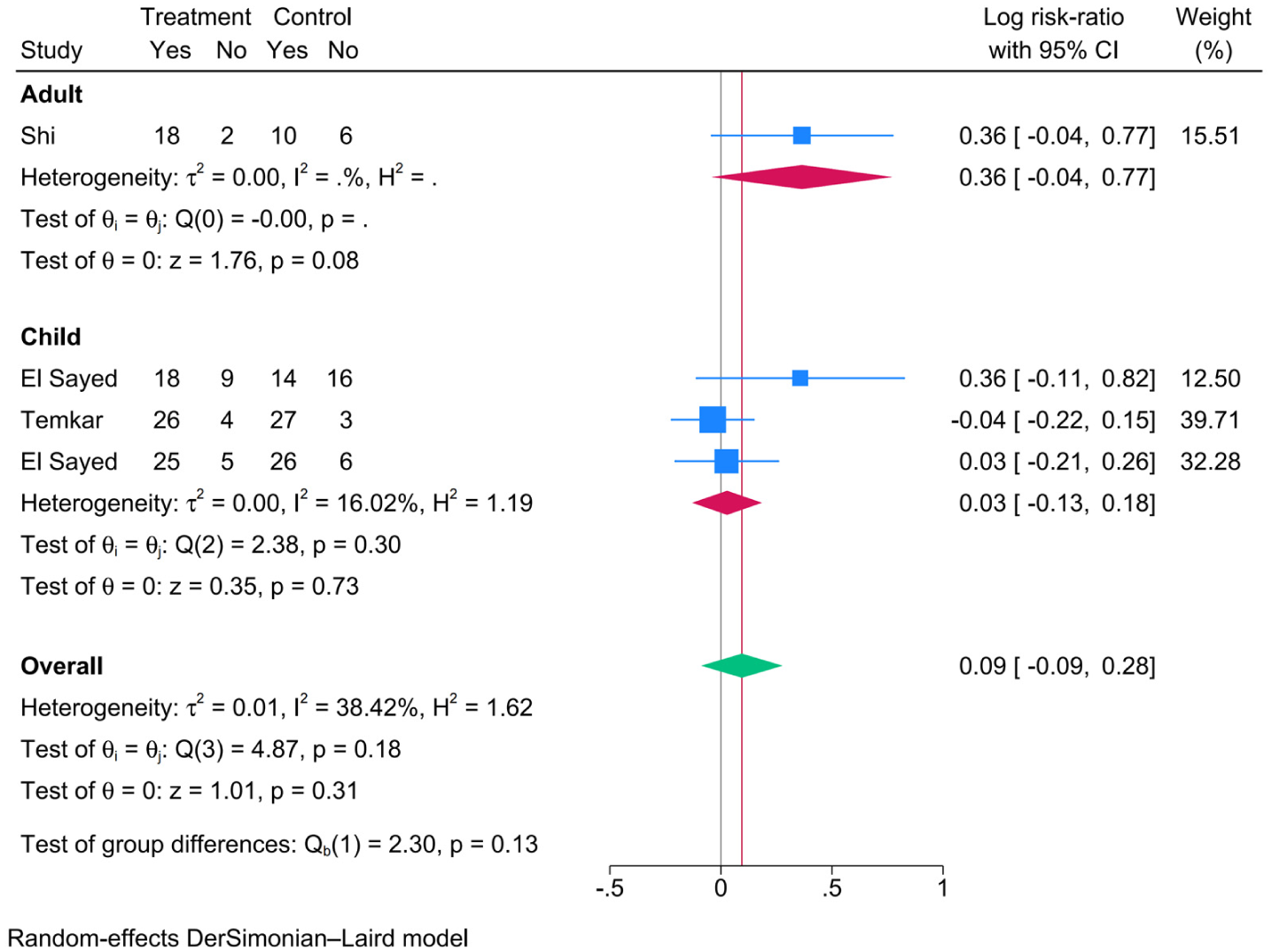
Forest plot comparing the postoperative success rate between microcatheter-assisted trabeculotomy and control surgery. The logRR was pooled using a fixed-effects model. Subgroup analyses for adult and pediatric patients are presented.
Number of postoperative antiglaucoma medications
To evaluate the impact of microcatheter-assisted trabeculotomy on the number of postoperative glaucoma medications, a meta-analysis was conducted on five included studies. With I2 = 52.93% > 50%, a random-effects model was employed. The results showed: SMD = −0.14, 95% CI: −0.57, 0.28, indicating a non-significant outcome. In the adult subgroup, a total of three studies were included in the analysis, yielding SMD = −0.60, 95% CI: −1.20, 0.00, which was not statistically significant. In the pediatric subgroup, two studies were analyzed, with SMD = 0.04, 95% CI: −0.28, 0.36, also showing no significant difference. Intergroup comparison revealed no difference in the number of postoperative antiglaucoma medications between the two subgroups (p = 0.06), as shown in Figure 5.
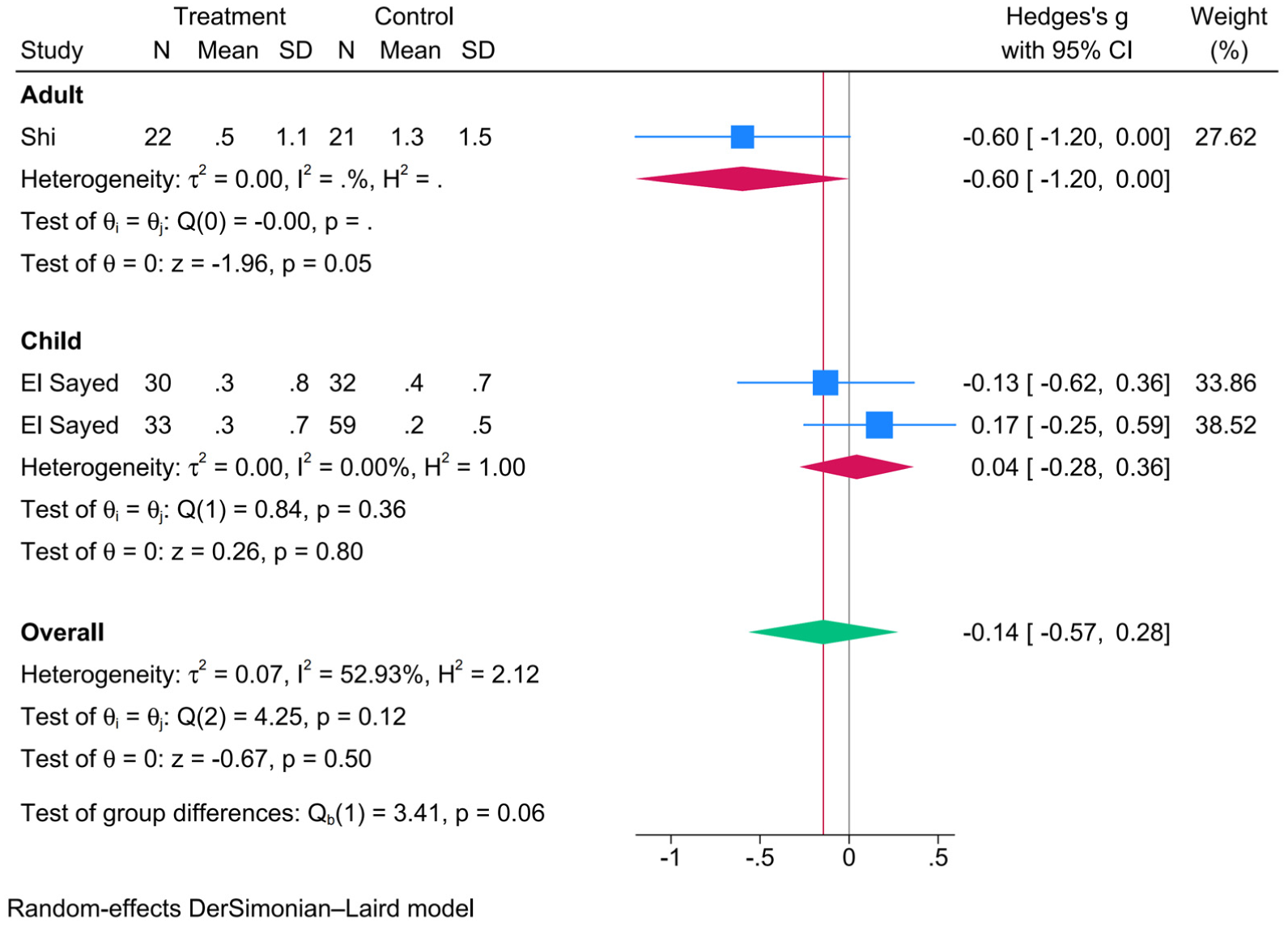
Forest plot comparing the number of postoperative antiglaucoma medications between microcatheter-assisted trabeculotomy and control surgery. The SMD was pooled using a fixed-effects model. Subgroup analyses for adult and pediatric patients are presented.
Ciliary detachment
To evaluate the impact of microcatheter-assisted trabeculotomy on postoperative ciliary detachment, a meta-analysis of one included study was performed. The results revealed no significant difference in the occurrence of postoperative ciliary detachment between the microcatheter-assisted trabeculotomy group and the control group (logRR = 0.00 [−1.89, 1.89]), as shown in Figure 6.
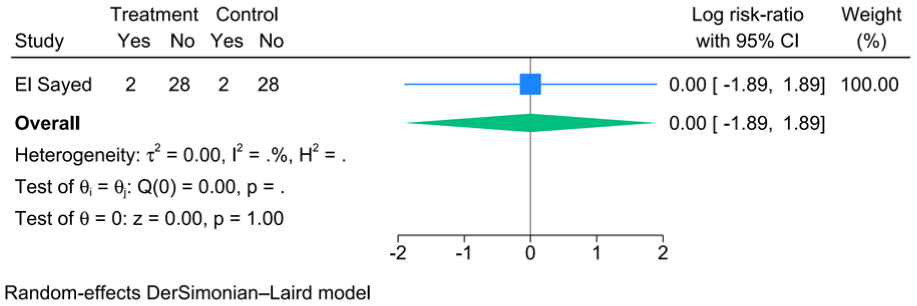
Forest plot comparing the incidence of postoperative ciliary detachment between microcatheter-assisted trabeculotomy and control surgery. The logRR was pooled using a fixed-effects model.
Publication bias and sensitivity analysis
For outcome measures with more than five included studies, publication bias was assessed. The results showed that the funnel plots were generally symmetrical without significant gaps, as shown in Figure 7. Additionally, Egger’s test was performed, and the p-values for all outcome measures were greater than 0.05 (Table 4), further confirming the absence of publication bias in the included literature.
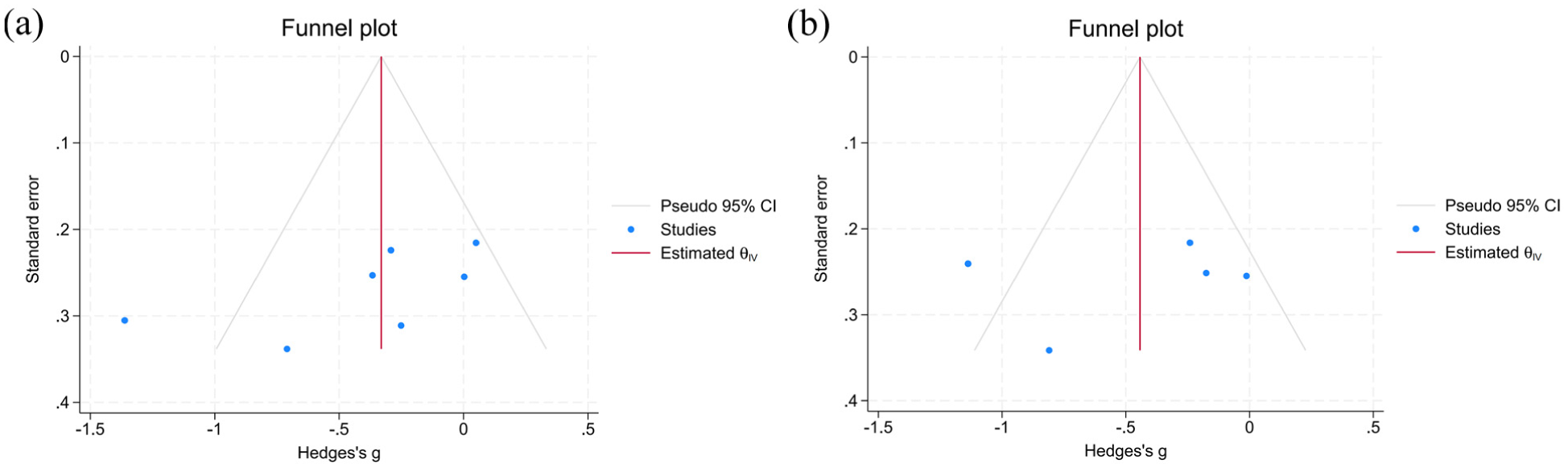
Funnel plots assessing potential publication bias. (a) Short-term IOP at 3–6 months; (b) long-term IOP at over 1 year.
Results of Egger’s test.

Sensitivity analysis
To test the robustness of our meta-analysis results, we performed a sensitivity analysis on outcomes with significant heterogeneity and statistically significant results by sequentially excluding each study and re-conducting the meta-analysis. The results showed that excluding certain studies altered the significance of the pooled estimates, indicating limited robustness of our analysis, as shown in Figure 8.
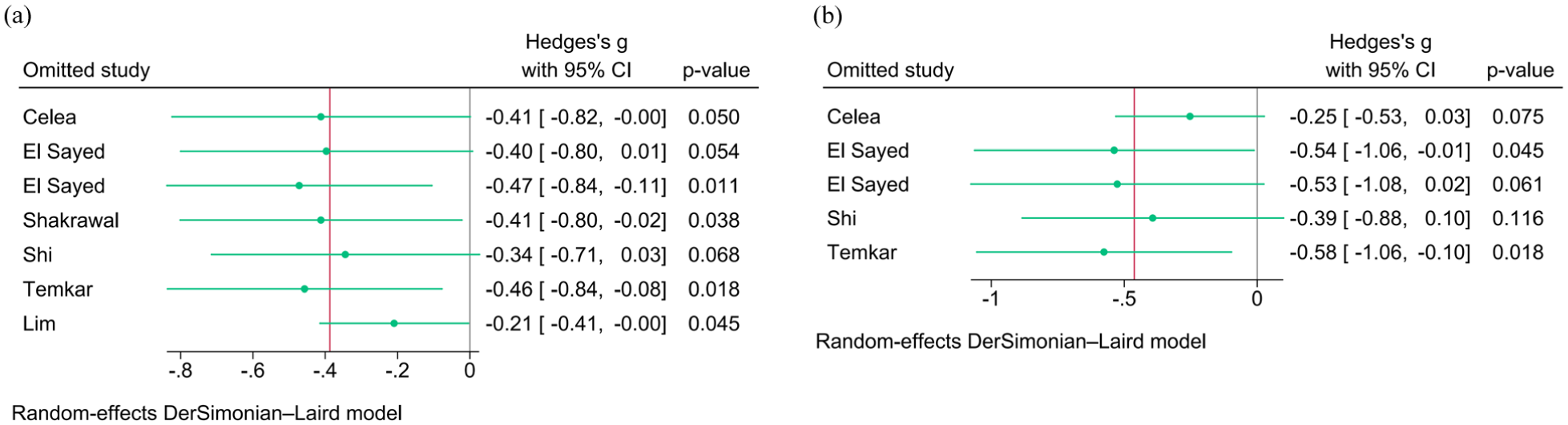
Sensitivity analyses performed by sequentially excluding each individual study to assess the robustness of the pooled estimates. (a) Short-term IOP at 3–6 months; (b) long-term IOP at over 1 year.
Discussion
This meta-analysis included 4 RCTs and 3 case–control studies with a total of 460 patients. We systematically assessed the efficacy and safety of microcatheter-assisted trabeculotomy for glaucoma treatment. This technique involves the use of a microcatheter to assist with fluid outflow, aiming to improve IOP control and reduce postoperative complications.15,17,18,29,30 The results indicated better short-term (3–6 months) IOP control with microcatheter-assisted trabeculotomy compared to the control group, and also demonstrated better long-term (>1 year) IOP control. In the short term, a significant benefit was observed in adults, whereas the pediatric subgroup did not show a significant benefit. Further subgroup analysis and meta-regression revealed that age was a significant source of heterogeneity, with a significant IOP reduction in adults but not in children, suggesting that the long-term effectiveness of this procedure may vary across age groups and warrants further clinical validation.
In terms of postoperative success rates, no significant differences were found either in the overall combined results or in the adult or pediatric groups when compared to the control group. This may imply that although microcatheter-assisted trabeculotomy demonstrates excellent IOP control, its success rate could be similar to that of other surgical methods. Regarding the number of postoperative medications, microcatheter-assisted trabeculotomy did not show a clear advantage. Moreover, although the difference was not statistically significant, a trend was observed between the adult and pediatric groups—the pediatric group tended to require more medications, 31 while the adult group showed a tendency toward fewer medications, although this difference did not reach statistical significance. This trend warrants further investigation in future studies with larger sample sizes to validate the findings.
With regard to postoperative complications, including ciliary detachment, no significant differences in risk were observed in all included studies compared to the control group. This emphasizes the potential safety of microcatheter-assisted trabeculotomy.
However, this study has several limitations. First, the limited number of included studies may lead to instability in the results, and when fewer than 10 studies are included, the power of Egger’s/Begg’s test to detect publication bias is insufficient. Second, variations in the design of the included studies may affect the accuracy of the pooled analysis. Third, the relatively short follow-up duration in most of the included studies makes it difficult to comprehensively evaluate the long-term efficacy and safety of MIGS. Finally, the results of sensitivity analyses showed that the significance of short-term and long-term IOP outcomes was not sufficiently robust; therefore, more studies are needed to achieve stable and significant findings, and readers should interpret the results with caution.
Overall, microcatheter-assisted trabeculotomy demonstrates potential advantages in both short-term and long-term IOP control, with varying trends observed among patients regarding the reduction in medication use. However, the advantages of this surgery in terms of postoperative success rates and medication reduction remain unclear. Further high quality, large-scale RCTs are necessary for a more accurate assessment of the long-term efficacy and safety of this emerging surgical approach.
Supplemental Material
sj-docx-1-imj-10.1177_10815589261462552 – Supplemental material for Meta-analysis of the clinical efficacy of microcatheter-assisted trabeculotomy in the treatment of glaucoma
Supplemental material, sj-docx-1-imj-10.1177_10815589261462552 for Meta-analysis of the clinical efficacy of microcatheter-assisted trabeculotomy in the treatment of glaucoma by Yuqiu Zhang, Juan Wang and Xingjian Chen in Journal of Investigative Medicine
Footnotes
Author contributions
Conception and design: Yuqiu Zhang.
Administrative support: Juan Wang.
Collection and assembly of data: All authors.
Data analysis and interpretation: Xingjian Chen.
Manuscript writing: All authors.
Final approval of manuscript: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Natural Science Foundation of Gansu Province (Grant No. 26JRRA799).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.