
Abstract
Breast cancer is the most common nonskin cancer diagnosed among women in the United States and throughout the world, and the leading cause of cancer deaths. Screening recommendations and guidelines vary depending on the organization. Screening modalities include self breast examination, clinical breast examination, mammography, ultrasound, and magnetic resonance imaging. Screening guidelines vary based on individual risk assessment and age.
Breast cancer is the most common nonskin cancer diagnosed among women in the United States and throughout the world, and the leading cause of cancer deaths. The Surveillance, Epidemiology, and End Results (SEER) database estimates that 232,340 women will be diagnosed with and 39,620 women will die of cancer of the breast in 2013. 1 A woman born in the United States today has a 1 in 8 chance of having invasive breast cancer during her lifetime. Worldwide in 2008, there were 1,383,500 estimated new cases of female breast cancer and 458,400 deaths. 2
Of note, the incidence and mortality of breast cancer has been decreasing in the United States from 1999 to 2008. Incidence has been decreasing by 1.2% per year, and mortality has been decreasing by 2% per year. 3 This is thought to be due in part to the increasing use of screening mammography as well as advances in therapy.
Screening Modalities
Screening refers to patients that are asymptomatic only with no palpable changes in the breast or other breast symptoms. The benefit of screening is finding the tumor at an earlier stage or before it has become invasive. Breast cancer mortality odds are largely based on the stage at diagnosis, with the earlier stage having a much improved overall survival. 1
A multiple number of screening modalities have been studied (see Table 1). The most common of these are self breast examination (SBE), clinical breast examination (CBE), mammography, ultrasound, and magnetic resonance imaging (MRI). Each has its own unique risk-benefit ratio. Certain patients may benefit from one or more of these screening modalities more than others.
Recommendations for Screening of Average Risk Women.
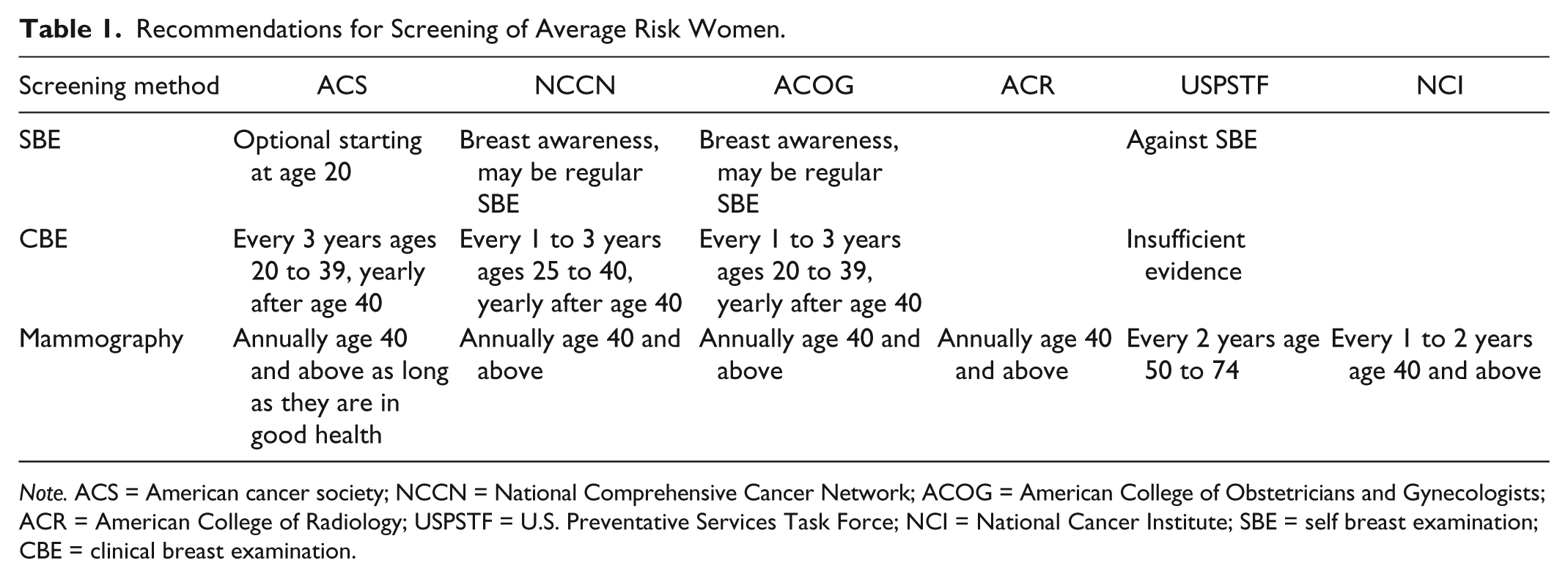
Note. ACS = American cancer society; NCCN = National Comprehensive Cancer Network; ACOG = American College of Obstetricians and Gynecologists; ACR = American College of Radiology; USPSTF = U.S. Preventative Services Task Force; NCI = National Cancer Institute; SBE = self breast examination; CBE = clinical breast examination.
SBE
Although this is arguably the simplest and least invasive form of screening, it is generally not recommended. There were two large population studies from Shanghai and Russia that looked at more than 380,000 women comparing SBE with no intervention that showed no statistically significant difference in the groups in terms of breast cancer detection; however, there were twice as many biopsies for benign lesions. 4 Although the cost of self breast exams is low, the potential harm in terms of increased number of biopsies for benign lesions led the U.S. Preventative Services Task Force (USPSTF) to recommend against SBE. 5 The American Cancer Society (ACS) states that SBE is optional. 6 The National Comprehensive Cancer Network (NCCN) and American College of Obstetricians and Gynecologists (ACOG) recommend self breast awareness, which may include SBE.7,8
CBE
There is very little data on the efficacy of CBE. In fact, the USPSTF states there is insufficient evidence for recommendation. 5 The cost of a CBE is only the cost for a clinical exam with risks of false-positive results that can lead to anxiety, unnecessary clinician visits, and biopsies. The exam is rather noninvasive and can be done in a matter of minutes. The ACS recommends a CBE every 3 years from age 20 to 39 and yearly thereafter. 6 Similarly, the NCCN and the ACOG recommend CBE every 1 to 3 years from ages 25 to 39 and 20 to 39, respectively, then annually.7,8
Mammography
Mammography is the most tested and the generally preferred method for breast cancer screening as it is the only modality to show a decrease in mortality. 9 The controversy lies in what ages to screen and how often screening should be performed. The risks of mammography include radiation risks, increased number of biopsies, and undue anxiety from false-positive results, not to mention the monetary costs.
There have been several studies looking at mammographic screening for breast cancer for various age groups. A Cochrane review of eight eligible trials and 600,000 women aged 39 to 74 estimated a 15% risk reduction in mortality among all age groups; however, this only corresponds to an absolute risk reduction of 0.05%. 10
The age group for average risk women that is most debated is ages 40 to 49. It is well known that breast cancer risk increases with age and the probability of a woman in her 40s developing breast cancer is 1 in 69. 5 The USPSTF recommends against routine mammographic screening for women in this age group. 11 Although there is a mortality benefit in the age group, it is estimated that 1,904 women need to be invited for screening in this age group to prevent one breast cancer death. Furthermore, there are more false positives in this group with a longer survival period after screening, which increases radiation risk, number of biopsies for benign lesions, and anxiety. However, there is a mortality benefit for mammographic screening in women of ages 40 to 49, which is likely the reason most other groups recommend mammograms in this age group. The ACS, NCCN, ACOG, and the American College of Radiology (ACR) recommend yearly mammographic screening in this age group.6,7,8,9 The National Cancer Institute (NCI) recommends screening mammograms every 1 to 2 years for this age group. 12
In women of ages 50 to 69, there is general agreement that mammographic screening is beneficial. The risk of a woman developing breast cancer is 1 in 38 in her 50s and 1 in 27 in her 60s. 11 ACS, NCCN, ACOG, and the ACR all recommend yearly screening, whereas the USPSTF recommends biennial mammograms.5,6-9, The NCI recommends screening mammograms every 1 to 2 years. 12
Most groups do not give an upper age limit for screening. The biggest concern with screening for elderly individuals is over diagnosis, or finding cancers that would never contribute to morbidity or mortality, as older women tend to have lower risk breast cancers. 13 There is, however, a high incidence of breast cancer in elderly women. Unfortunately, there are no large randomized trials for breast cancer screening for women above 70 to 74 years. The ACS suggests screening for “as long as they are in good health.” 6 The USPSTF has no recommendation above age 75 and states that the evidence of benefit is lacking. 5
Breast Ultrasound
Breast ultrasound is sometimes used in average risk individual breast cancer screening for women with dense breasts, those with abnormalities found during other screening modalities, or used to aid in localization for biopsy. It is generally not used alone for screening purposes in average risk individuals, although studies are ongoing, especially for women with dense breasts.
Breast MRI
Breast MRI is a newer exam and is generally not used for screening average risk women. The cost of breast MRI is quite prohibitive and is only used for screening high-risk individuals; however, it is sometimes used diagnostically if an abnormality is found using other screening methods. 9
Screening High-Risk Individuals
Risk assessment is generally based on medical history, family history, and sometimes genetic analysis. There are multiple medical history factors that can contribute to increased risk of breast cancer. For example, prior thoracic radiation below the age of 30 poses a significantly increased risk of breast cancer. Other risk factors are less so. Obesity, hormone replacement therapy, younger age of menarche, older age at menopause, nulliparity, race, and dietary factors are known to increase breast cancer risk, but not as substantially as BRCA mutations.
Genetic counselors play a key role in helping decide on testing for genetic factors as well as screening. NCCN criteria for further genetic risk evaluation in an unaffected individual include the following family history: a known mutation in a breast cancer susceptibility gene within the family, more than one breast primary in a single individual, more than one breast primary on the same side of the family, one or more ovarian cancers in the same side of the family, a first or second degree relative with breast cancer below the age of 45, one or more family members on the same side of the family with breast cancer and pancreatic cancer, aggressive prostate cancer, sarcoma, adrenocortical carcinoma, brain tumor, endometrial cancer, leukemia, lymphoma, thyroid cancer, specific dermatologic manifestations, macrocephaly, hamaromatous polyps of the gastrointestinal (GI) tract or diffuse gastric cancer. In these patients, referral to a genetic counselor or other health care professional with expertise in cancer genetics is highly recommended. The counselor can then assess the risk and recommend possible testing for BRCA1/BRCA2 mutations, Li-Fraumeni Syndrome, Cowden Syndrome, and others. However, even if the specific known mutation or syndrome is not present, these individuals often still have a higher than average risk for breast cancer.
Risk assessment estimates are based on available models utilizing many risk factors listed above, such as the Gail model, the Claus model, and the BRCAPRO model. 6 Higher risk individuals are candidates for more aggressive screening. Depending on the risk for breast cancer and the patient age, some or all of the screening modalities listed should be used. Often it is recommended to do yearly mammograms at an earlier age in addition to more frequent clinical breast exams and possibly MRI screening. The ACS recommends yearly mammogram and MRI for women with a >20% lifetime risk and consideration of yearly MRI on top of mammogram for women with >15% lifetime risk. 6 Similarly, the NCCN recommends yearly mammograms and clinical breast exams every 6 to 12 months beginning at age 30 for those with >20% risk and considering breast MRI beginning at age 20. For those with prior thoracic radiation between the ages of 10 and 30 or those with known or suspected genetic predisposition, the NCCN recommends clinical breast exam every 6 to 12 months, and the NCCN and ACR recommend annual mammogram starting at age 25 as well as annual breast MRI.7,9 For high-risk women, it is also recommended to discuss risk reduction strategies.
Conclusion
Breast cancer screening saves lives. With the average U.S. woman having a 1 in 8 lifetime breast cancer risk, screening should be a part of routine medical care. Although there is some controversy about exact screening ages and intervals, most major medical societies in the United States agree that breast cancer screening is important. Screening generally involves clinical breast exams and mammograms for women aged 40 or 50 to 70 or above in average risk women. In high-risk individuals, earlier screening with more frequent intervals and breast MRI is recommended. Exact recommendations for an individual should be personalized and discussed with a patient’s physician.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.