
Abstract
Heart failure (HF) affects 5.7 million Americans and is the most common reason for 30-day readmissions. While evidence supports incorporating home telehealth (HT) programs within health care organizations to support HF patient care, it is essential to carefully map HT into existing care pathways to promote successful outcomes. The purpose of this evidence-based project was to increase enrollment in an existing Veteran’s Administration HT HF program through a strategically designed HT program plan. The outcomes included a 300% enrollment and no project participant readmissions during the 9-month project. Given the competency development in strategic and program planning, advanced practice registered nurses are ideally suited to provide the leadership in designing, implementing, and evaluating HT programs.
Keywords
Introduction
Heart Failure (HF) affects 5.7 million Americans and costs health care systems approximately 39 billion dollars every year. 1 In the Medicare population, HF is the leading cause for hospitalization with 1 million admissions per year. 2 The management of HF is difficult due to the complexities of the required lifestyle changes, medication regimen, laboratory monitoring, and interactions with other comorbid conditions. 3 Furthermore, HF patients experience the highest readmission rate of all medical conditions due to complications and exacerbations that ultimately have a negative impact on quality of life resulting in significant health care risks. 4
Home telehealth (HT) programs have proven to be both efficient and effective in managing HF self-care as there is a connection of patient and provider in a coordinated system of care. 5 To be successful, a HT program must be strategically planned utilizing an interprofessional team approach with careful mapping of the HT program into the organization’s existing care pathways. Failure to incorporate these essential organizational factors into the design and implementation of the HT program will significantly hinder HF patient enrollment and the sustainability of the HT program.
Background
The Centers for Medicare and Medicaid Services6,7 report the national HF 30-day readmission for hospitals, including Veteran Affairs (VA) hospitals, ranges from 20.1% to 31.4% with a median of 24.7%. According to the Department of Veterans Affairs Quality Enhancement Research Initiative, 8 the expense of treating HF Veterans has grown steadily for the last several years costing millions of dollars per year due to recurrent emergency room visits, hospitalizations, and readmissions. The 30-day readmission rate for HF at the project facility, a VA in southern California, was 26%, 9 or one in four Veterans, and the rate of readmissions within 60 days was even greater.
In response to the epidemic proportion of HF hospitalizations and readmissions along with other costly, common chronic diseases, the Veterans Health Administration (VHA) developed a national HT information technology infrastructure to support the ongoing care of Veterans with chronic diseases. The program was designed “to improve the efficiency, effectiveness, coordination, and continuity of care” by requiring patient participation in the management of their chronic disease. Given the growing body of literature10-13 that supports the evidence base for the incorporation of HT to decrease the incidence of 30-day HF readmissions as well as successful management of other chronic diseases, the entire VHA organization incorporated HT training for 5,000 staff and subsequently analyzed the data obtained for 17,025 patients. The HT program included a telephone educational intervention in addition to an electronic device placed in the Veterans home for monitoring daily weights, blood pressure, heart rate, and blood glucose. Data were relayed and reviewed daily by registered nurses (RNs) and advanced practice RNs (APRNs) resulting in the provision of services such as education, medication adjustments, and referrals. The outcomes included a 25% reduction of inpatient hospital days, 19% reduction in hospital readmissions, and overall patient satisfaction.
The project VA had recently initiated HT training for the nursing staff and ordered HT equipment for HF patient care. However, only a small percentage of HF patients were enrolled. In fact, there were 6 patients enrolled in the HT program during the past 6 months. Administration had concluded that the lack of provider commitment, time for patient screening, and restrictive scheduling were the primary factors contributing to the low enrollment. Therefore, the purpose of this evidence-based practice project was to design and implement a process that would increase enrollment of Veterans with HF in the existing HT program. The secondary goal was to decrease the number of 30-day HF-related readmissions at the project facility. The project benchmark was established at a 100% increase in number of patient enrollments over a 9-month period.
Practice Change Process/Methods
The enrollment of HF patients into the existing HT program had been initiated through primary care provider (PCP) consultation to the HT case managers but referrals had been minimal. Using the Logic Model (1999) 14 as a basis for performing an evaluation, the project director collected data pertaining to the resources, activities, and outcomes of the existing program. A gap analysis was conducted and the findings were used by the project director in planning and implementing the proposed program plan. For example, the project director determined that the PCPs (i.e., resources) previously had received minimal information regarding the operationalization of the HT program (i.e., activities) and subsequently did not clearly comprehend the enrollment process for their patients. In contrast, the project director planned for PCPs to learn the essentials about the enrollment process during the planned in-service. Prior to the in-service, interprofessional team members consisting of the HT RN case managers, pharmacists, and informaticists were consulted regarding their organizational perspectives on strategies to enhance enrollment in the HT program. These comments were shared with the PCPs such as confirmation from the pharmacy team that 24-hour pharmacy consultation for medication-related issues was available in instances that the HT case manager was challenged and could not obtain a response from the PCP.
The emphasis of the in-service was on the primary outcome of increasing patient enrollment in the HT program. Proposed secondary outcomes included decreased readmission rates and costs, increased medication compliance, patient and provider satisfaction, and improved quality of life. An educational brochure and recruitment flyer were also distributed. All of the providers were employed by the VA and had received communication from the cardiology department head that participation was mandatory. Each PCP was required to participate in one of the three (90-minute) sessions that had been scheduled on three different weekdays and at different times of the day. A total of 15 PCPs were trained to correctly enter the accurate diagnosis code into the encounter sheets that were later cross-checked by coders. Overall, the PCPs responded favorably to patient enrollment but confirmed that lack of time to screen patients for program eligibility was a major deterrent. The project director, a seasoned family nurse practitioner, anticipated that time would be the major deterrent from the PCP perspective and would therefore function in the role to enroll patients after obtaining PCP permission to screen provider panels. For sustainability purposes, the plan was to train additional nurse practitioners who would screen and enroll Veterans in the HT program.
Project approval had been obtained from the facility’s Safety Committee, Resource and Development Committee, and the VA facility and University of San Diego Institutional Review Boards. The baseline project time frame extended for a period of 2 years (March 2012-March 2014) even though enrollment for this project only occurred from June 2013 through March 2014. This extended time frame was included to review the pre-project data of all HF patient enrollments, length of enrollment, and readmissions during the HT program.
For the purpose of this project, patients initially were identified using VISTA, the VA’s electronic medical records system. The project director, a full-time VA Family Nurse Practitioner (FNP) employee, had received authorization to access all patient electronic medical records along with all provider patient panels. In addition, the project director had established a collegial relationship with the information technology department head who had enthusiastically agreed to support the project director, PCPs, and HT RN case managers. Veterans with HF who met the following inclusion criteria were enrolled in the HT program: (1) willingness to participate, (2) verbal commitment to comply with treatment, (3) cognitive ability to use a touchtone screen or a phone, (4) ability to step on a scale, and (5) phone access. Exclusion criteria included Veterans who (1) lived in a nursing home, (2) were homeless, (3) had a significant history of non-compliance with management, and/or (4) had connectivity issues (e.g., no telephone or unreliable mobile phone coverage). Eligible patients were referred within 24 to 48 hours to the HT program.
A HT RN made two attempts to contact the patient to proceed with enrollment. The facility policy was that following two unsuccessful attempts, no additional calls were made but the project director was informed through monthly generated reports as to which patients were enrolled as well as those patients not enrolled due to inability to establish communication with the patient. Veterans contacted and who continued to have interest in participation were enrolled in the HT program by the HT RN. Initially, a convenient time was determined for device installation. All patients also received an educational intervention via telephone that was conducted on an individual “needs basis.” This consisted of reviewing the “standardized” VA HF patient education handbook provided to each patient. Typically, these calls lasted approximately 10 minutes. Daily monitoring of clinical data included vital signs, weight, and pulse oximetry. In instances whereby clinical data were outside the parameters, the HT RN would contact the patient to determine possible rationale and proceed with activities within the scope of their role. Otherwise, the RN would contact the PCP. There were those occasions in which APRNs, who were the designated PCP for a patient enrolled in the study would make patient care management decisions. In addition to individual patient clinical parameters that had been established by the PCP, the HT RN used an evidence-based American Heart Failure Association algorithm to guide decision making that was inclusive of self-titration of medications, scheduling an appointment with their PCP at the VA clinic, and/or seeking emergency room care.
Throughout the project period, monthly reports were generated by the HT department regarding the percentage of Veterans participating on a daily basis in the HF HT program. These data included both enrolled and disenrolled patients, logged on a spreadsheet, and maintained by the HT RN. The number of Veterans who were referred versus actually enrolled in the HT program was collected through the HT software program accessed by HT RN case managers. Data regarding readmission rates were analyzed throughout the project. At the completion of the project, readmission rates of those Veterans who participated in HT were analyzed.
Results
There were a total of 99 patients referred to HT from June 2013 through March 2014 through the newly established process. Thirty-two patients were enrolled in the program whereas 67 patients were not enrolled due to one or more of three patient-related factors: (1) lack of telehealth adoption/acceptance, (2) cultural and ethnic differences and needs, and/or (3) monotony of schedule using devices. There were five patients who emphatically stated that they could not “trust” the devices. As the HT RN team was fluent in English and/or Spanish only, 7 patients could not be enrolled whereas the remaining 55 patients refused “having to use” the devices on a daily basis. Of the 32 patients who did enroll, 10 patients had a history of 30-day readmission whereas the remaining 22 patients had a history of hospitalization or emergency room visit for HF. Eight of these patients were disenrolled due to lack of participation either by choice or by worsening of disease within 1 to 2 weeks of enrollment.
Based on the review of pre-project patient enrollments extending from October 2012 through June 2013, there were only 6 patients enrolled during the 9-month time frame in contrast to the 24 patients enrolled during the 9-month project. As for readmissions, 3 of the 6 (50%) pre-project patients had readmissions during their enrollment in the “former” HT program whereas none of the 24 patients enrolled in the “project” HT program were readmitted to the hospital (see Figure 1). Furthermore, data for the enrolled 24 HF patients in the project were collected from March 2012 through March 2014 that included both the pre-project and project time frames. The control chart (see Figure 2) displays weeks between hospitalizations for HF patients enrolled in this project. The first phase, or baseline, which is approximately the first third of the moving average control chart, reflects the numerous admissions and readmissions prior to the implementation of the project. The middle phase, or implementation phase, represents the fluctuations due to the staggered enrollment of HF patients into HT over a 6-month period showing that some of the early patients were doing better whereas other patients were frequent admissions recently being enrolled. The final phase demonstrated the statistically significant effect of the practice change, namely, no admissions, whereby the entire cohort has increased the interval between hospital readmissions.
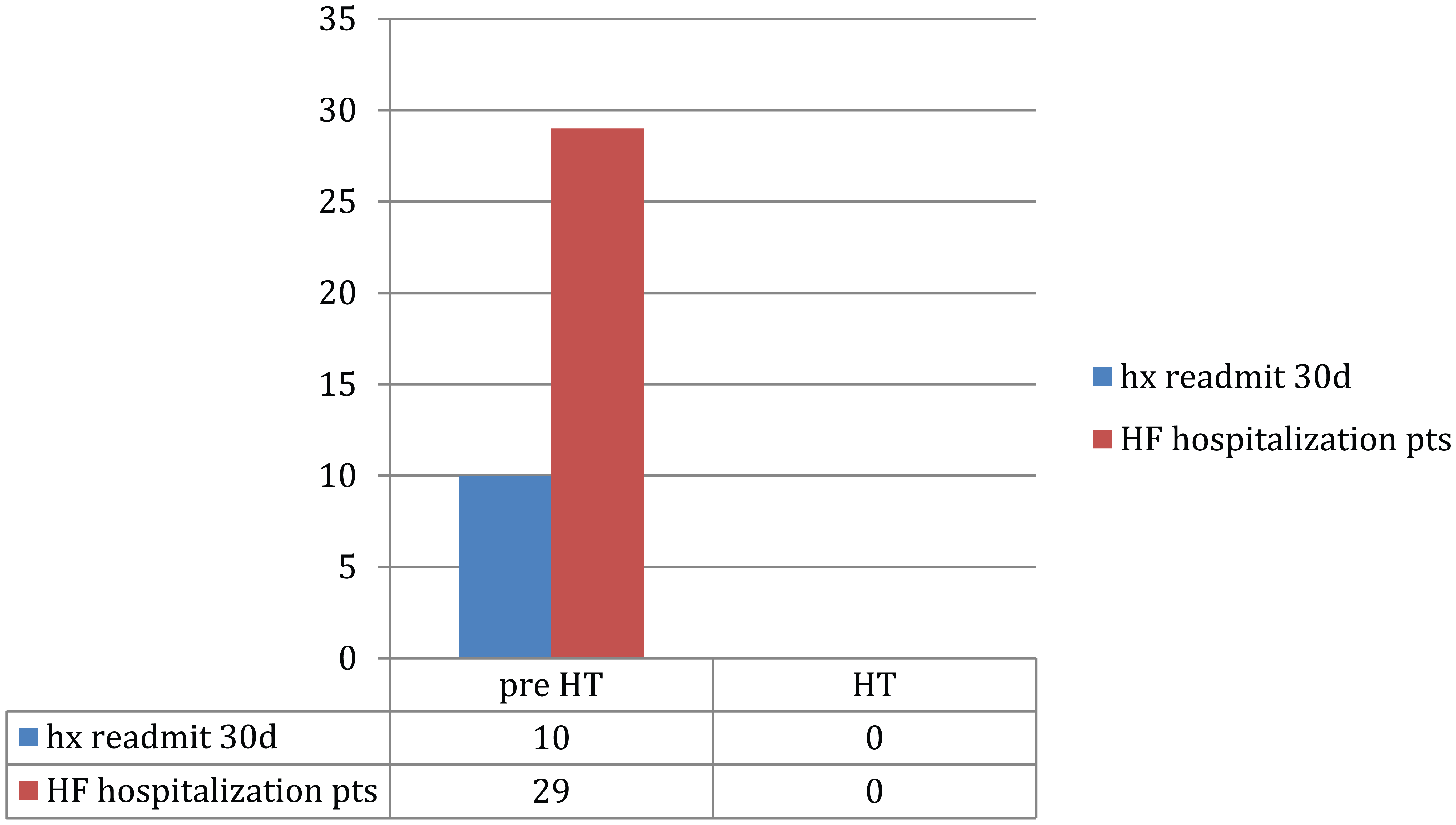
Patient hospital admissions before and after home telehealth.
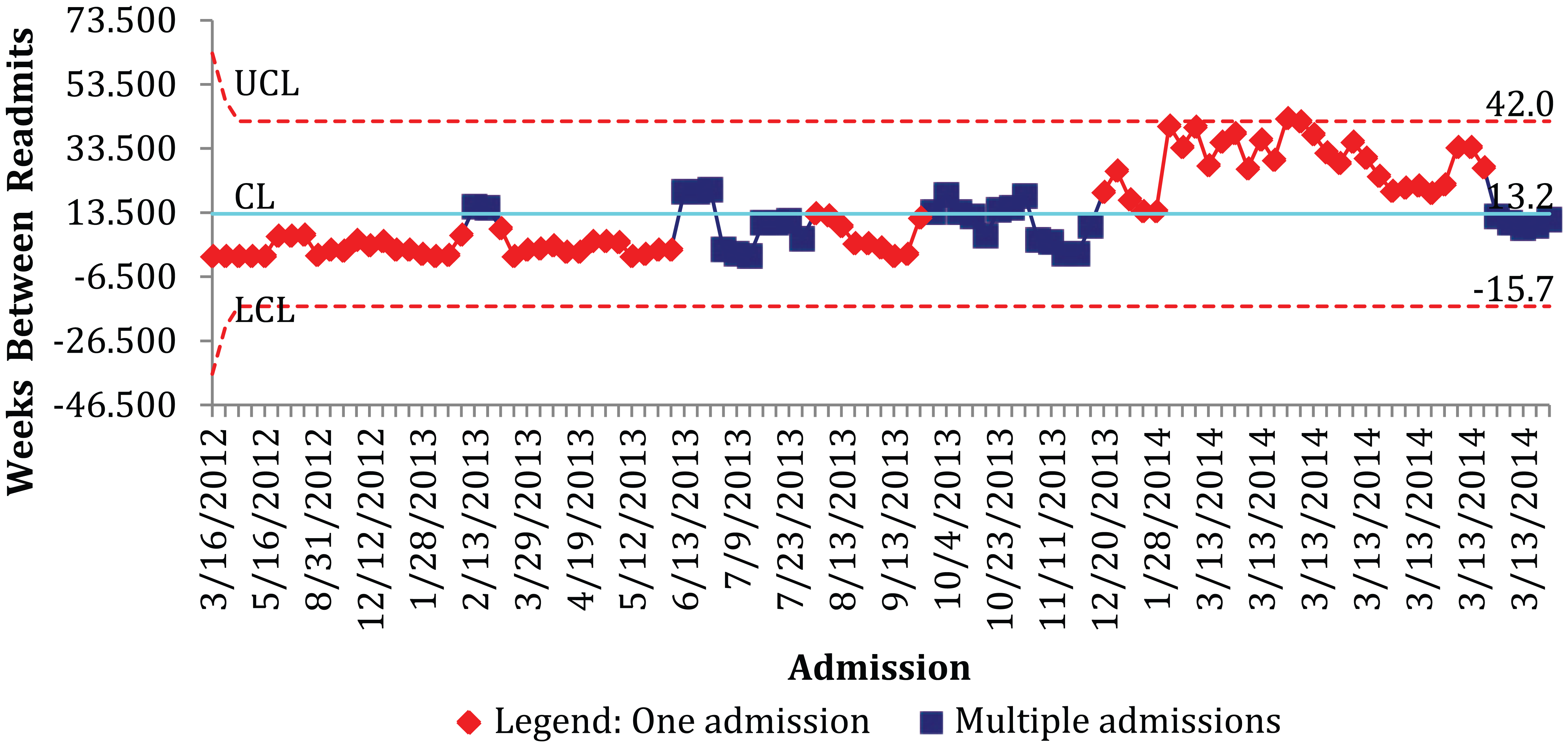
Weeks between admissions before and after home telehealth for Veterans with heart failure.
Discussion
The findings from this evidence-based project emphasize that strategic planning is essential to increase and sustain enrollment in a VA HT program. Using the existing HT resources within this VA hospital, a program plan using an interprofessional team (nurses, physicians, informaticists, pharmacists, patients) perspective was designed and implemented to increase TH HF patient enrollment. Secondary outcomes were also achieved as none of the 24 VA HF patients had readmissions during the 9-month project when these patients had previously been plagued with frequent and recurring readmissions and hospitalizations.
Although the evidence base supports incorporating HT for enhancing HF patient care management,12,15 and the VA has been perceived as a leader in designing and implementing effective HT services for HF patients, there were barriers specific to this VA setting prohibiting successful incorporation and implementation. The HT resources were available but there lacked a “champion” or project leader who would assimilate evidence-based guidelines on how to implement the HT HF program. This required active participation of all key stakeholders in making important decisions about program design and implementation.
The timeliness of this project was further supported by a financial incentive on behalf of the VA that “awarded” PCPs who did refer patients for HT. The cost-benefit analysis presented to PCPs during the project director’s in-service was motivational and communicated the overall benefits to the VA. Specifically, the in-service proved valuable to enhancing the understanding of telehealth, its aims, and purposes. However, even though there was an overall improvement in PCP participation, all PCPs were still not fully committed with the HT program, which was primarily attributed to the additional time commitment for screening patients and lack of experience using HT to provide interventions. However, for those PCPs who accepted/adopted HT as a modality for enhancing patient care, they were able to utilize the patient’s biometric data to make meaningful patient care decisions that prevented acute cardiac decompensation and subsequent readmission.
Similarly, patient participation must be enhanced to more fully incorporate HT. Even though the benefits of a HT program were explained to the patients, there were a significant number of Veterans who were not willing to participate. For those Veterans who did participate in the HT, the absence of readmissions and hospitalizations was so convincing that these data should be shared with future Veterans when approached about HT enrollment. In addition, the “lack of patient interest” on behalf of some Veterans must be further explored within the context of “patient selection” 16 and refinement of a HT “template” for patient identification and selection within the VA system.
Implications for Clinical Practice
HT, or any health care information technology, must be adopted with system-wide objectives from the outset and with careful mapping into existing care pathways. 16 As described in this project, nursing at various levels can have a leadership role in implementing an effective HT service for HF management along with other chronic disease HT management programs. Doctorate APRNs possess the leadership skills along with a substantial knowledge base in health care informatics, program planning and evaluation, strategic planning, and financial management that makes them ideally suited for initiating, implementing, and evaluating telehealth services within an organization. 17 An essential component of the project planning and development includes the identification of barriers related to the patient, health care organization, technology, and economics in order that these challenges can be understood and managed to the greatest extent possible prior to developing a telehealth service model and its deployment. It is essential that a detailed cost-benefit analysis that highlights the financial outcomes associated with reduction of readmissions is offered and consistently updated in order that the financial benefits accompanying a reduction in HF readmissions are recognized by all VA employees. 16
The health benefits and cost savings that accrue to patients and providers by using HT are of paramount importance to nursing. The necessity for PCPs, including APRNs, to contain HF patient health care costs requires solutions that can be realistically incorporated into their practice. APRNs are integrally involved with making decisions regarding the clinical data gathered by the HT monitoring. There may be medication adjustments and/or recommendations for the patient to go to the ER. RNs frequently conduct the daily HT monitoring to obtain the clinical data while ensuring that the technology is functioning effectively. The depth and breadth of clinical knowledge that RNs possess concerning HF affords them the skill set and knowledge base necessary for successful incorporation of HT into patient care management. This alternative approach to gathering and monitoring patient clinical measurements along with offering an educational pathway for nurses to conduct patient education regarding HF enhances their ability to be more efficient and effective in their roles. 15 Nurses can champion the use of HT to maintain frequent and regular contact with patients who are at risk of hospitalization and/or emergency room visits.
From a nursing education perspective, there has been an increased emphasis on inclusion of health care informatics content in both graduate and undergraduate nursing education programs. However, the application of knowledge with a planned experiential component, or clinical experience, is clearly lacking. 18 There are several contributing factors including lack of faculty with the expertise in health care informatics, curriculum “crowding,” and/or expenditures associated with technology. For those nursing programs that have a health care informatics program, faculty should collaborate and use the resources available to develop experiential learning experiences for students. By increasing exposure to health care informatics, and specifically telehealth, students will have an increased understanding and comfort with telehealth.
Summary
Nursing can assume a key role by providing the leadership necessary to successfully design, incorporate, and evaluate sustainable HT HF programs in clinical organizations. This requires successful program planning based on a comprehensive strategic evaluation of all components of the organization. Ultimately, positive outcomes for both the patient and organization can result from a strategically designed HT program.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.