
Abstract
In Thailand, individuals with stroke prefer to return home after being discharged from hospital and most of them have inconveniences to get to hospitals or clinics to receive physical therapy. Thus, home-based physical therapy (HBPT) might be an option. A retrospective pre-test and post-test study was conducted among 2,412 individuals with first stroke after receiving HBPT. It showed significant (p < .0001) improvement in voluntary movement, postural balance, and activities of daily living (ADLs) in individuals with after-stroke duration of ≤20 years. Those with after-stroke duration of >20 years demonstrated significant development in voluntary movement (p = .005) and postural balance (p = .037), but not ADLs. In conclusion, HBPT improves voluntary movement, postural balance, and ADL in individuals following any period of first stroke, and might be an alternative service for them in Thailand.
Introduction
Stroke is a common cause of death and a long-term disability throughout the world. In Thailand, the estimation of stroke prevalence is 1.88% among adults of 45 years and older. 1 Cerebral infarction is the most common stroke subtype with a prevalence of 122 patients per 100,000 population and with a mortality rate of 7%. 2 Thus, stroke is the main disability burden in Thailand, that is, the first in female and the third in male. 3
In Thailand, most individuals with stroke prefer to return home, and family members or caregivers take care of them after being discharged from the hospital. 1 Individuals with stroke are recommended to receive early rehabilitation to regain physical abilities, 4 with the hope to reduce the burden on family and society. In Thailand, the majority of individuals with stroke cannot receive physical therapy because they cannot afford to travel nor have anybody to take them to the physical therapy department in a hospital or private clinic. Several studies have found similar improvement in activities of daily living (ADLs) in individuals with stroke receiving physical therapy in hospital or at home.5-7 Studies on home-based physical therapy (HBPT) have demonstrated that ADLs of individuals with stroke could be improved.8-11 In addition, HBPT reduces tension and supports emotion of individuals with stroke better than physical therapy in hospitals.6,7,11 Therefore, in Thailand, HBPT may be an option for individuals with stroke who cannot receive physical therapy in a hospital or private clinic.
The Project of Stroke Care in Community in Thailand, a government-based project by National Health Security Office, was launched in 2006. It aimed to deliver physical therapists to visit individuals with stroke, who are unable to receive physical therapy in hospitals or private clinics, at home. Physical therapists prescribe exercise program and teach stroke patients to follow; in addition, they educate their family members and caregivers about the program. The program is tailored for each individual with stroke according to goals of individuals or family. By this method, physical therapists act as coaches or supervisors. At the time of the completion of this study, effect of the service had not been demonstrated. Therefore, the objective of the study was to determine the enhancement in voluntary movement, postural balance, and ADL ability before and after receiving HBPT in individuals with stroke in Thailand. The study provides information about benefits of HBPT for individuals with stroke in Thailand as the service may fill the gap for those who are unable to receive physical therapy at a hospital or private clinic.
Methods
The study had a retrospective pre-test and post-test design and was approved by the university ethic review committee.
Participants
The study obtained data from 2,412 individuals with first stroke (1,293 males, 1,119 females) joining in the Project of Stroke Care in Community between October 2006 and January 2010. The data were from those with first stroke, with no head surgery, who had a caregiver at home to do the exercise program, who had no complications interrupting physical therapy during receiving HBPT, and who gave permission to use data by signing written consent form or allowing a relative to sign the document if he or she could not sign. Individuals with stroke joining the project lived in Bangkok, Nonthaburi, Pathum Thani, Samut Prakarn, and Nakhon Pathom. They received the information about the project via poster, brochure, television, and radio. Then they contacted the project to receive the service.
The data were grouped by after-stroke duration: (1) ≤30 days, (2) 31 to 60 days, (3) 61 to 90 days, (4) >3 to 6 months, (5) >6 to 12 months, (6) >1 to 2 years, (7) >2 to 5 years, (8) >5 to 10 years, (9) >10 to 20 years, and (10) >20 years. The reason for grouping was that the first 30 days after stroke showed improvement the most; then there was gradual development until 90 days post-stroke, and hardly demonstrated recovery from 91 days onward. 12 Therefore, the duration of recovery was considered to be longer for more chronic stroke.
Home-Based Physical Therapy Service
Thirteen physical therapists who had experience of 2 to 5 years were trained in assessment, body function impairment analysis, and designing therapeutic exercise for 6 months before they visited individuals with stroke in their homes. They were blinded about the study. They visited their own patients at the maximum of 15 visits in 7 months. The visit frequency was one visit per week for 2 months (eight visits), alternate-week visits for 2 months (four visits), and visit once a month for 3 months (three visits). Individuals with stroke who had reached their goal or the highest physical ability could ask to stop the service before the completion of the 15 visits.
In each visit, a physical therapist assessed voluntary movement by Stroke Rehabilitation Assessment of Movement (STREAM),13-15 postural balance by Postural Assessment Scale for Stroke Patients (PASS), 16 and ADLs by Barthel Index (BI). 17 After that, the physical therapist who did the assessment designed exercise to reduce spasticity, increase muscle strength, and/or train normal movement pattern and postural balance, according to the body impairments. The objective of the exercise was to improve ADLs. In addition, the therapists taught individuals with stroke, family members, and/or caregivers to do the exercise until they understood how to do. Individuals with stroke and caregivers performed such program continuously until the next visit. Each visit took about 30 to 45 minutes.
Outcome Measures
Stroke Rehabilitation Assessment of Movement
The STREAM13-15 measures voluntary movement and basic mobility. It contains 30 items among three subscales; 10 items for upper extremity movement (STREAM-UE), 10 items for lower extremity movement (STREAM-LE), and 10 items for basic mobility (STREAM-BM).
For STREAM-UE and STREAM-LE, each item is a 3-point ordinal scale ranging from 0 to 2. For STREAM-BM, each item is a 4-point ordinal scale ranging from 0 to 3. At score 1 of each subscale, there is a 3-point scale of quality of movement that is not considered in the calculation. A total score is 20 points each for STREAM-UE and STREAM-LE, and is 30 for STREAM-BM. Each subscale score is converted to a percentage score out of 100. The final score of STREAM is the average of the scores from the three subscales. Scores can range from 0 to 100. The higher the score is, the better the voluntary movement.
For individuals with stroke, the internal consistency of STREAM is .98, the intra-rater reliability ranges from .96 to .999, and the inter-rater reliability is .98 to .995. 14
Postural Assessment Scale for Stroke Patients
The PASS 16 is a postural measurement containing 12 items in two domains; 5 items maintain position (PASS-MP) and 7 items changing posture (PASS-CP). Each item has a 4-point ordinal scale ranging from 0 to 3. Therefore, the total score is 36 with 15 for PASS-MP and 21 for PASS-CP. The score can range from 0 to 36. The higher the score is, the better the postural balance.
For individuals with stroke, the internal consistency of PASS is .95, and the intra-rater and inter-rater reliabilities are .72 (0.45-1) and .88 (.64-1), respectively. 16
Barthel Index
The BI 17 is a measurement of ADLs consisting of 10 items; feeding, bathing, grooming, dressing, bowels, bladder, toilet use, transfer, mobility, and stairs. Scores can range from 0 to 100, where 0 means complete dependence, and 100 means absolute independence.
For individuals with stroke, the intra-rater reliability of BI is .89, 18 and the inter-rater reliability is .99. 19
Data and Statistical Analysis
Statistical analysis was performed using SPSS 18.0 software package (SPSS, S/N 5089368) and was done on age, visit frequency, and scores before and after HBPT on subscale and complete STREAM, PASS, and BI. The scores before and after were from the assessment at the first and last visits.
The Kolmogorov–Smirnov test was conducted to test the normal distribution of age, visit frequency, and scores of STREAM-UE, STREAM-LE, STREAM-BM, complete STREAM, PASS-MP, PASS-CP, complete PASS, and complete BI before and after HBPT.
One-way independent analysis of variance or Kruskal–Wallis test was performed appropriately to determine difference in age and visit frequency among 10 subgroups. If there was significant difference, pairwise comparison was conducted to observe group difference.
A paired-sample t test or Wilcoxon signed-rank test was used appropriately to compare scores of STREAM-UE, STREAM-LE, STREAM-BM, complete STREAM, PASS-MP, PASS-CP, complete PASS, and complete BI before and after HBPT within groups.
The level of statistical significance considered was less than 5%.
Results
The Kolmogorov–Smirnov test showed that there was normal distribution in the age of the group with after-stroke duration of 91 to 180 days, >1 to 2 years, >5 to 10 years, >10 to 20 years, and >20 years. Data of visit frequency did not show normal distribution. Only data of subscale and complete STREAM, PASS, and BI in group with after-stroke duration of >20 years had normal distribution.
Figure 1 shows boxplot of age and visit frequency of all participants. No outlier was shown in age and visit frequency. Some participants were deemed to be outliers in age. As shown in Table 1, the average age of all participants was 65 years (age range = 19-99 years). The mean age of most subgroups was approximately 65 years, whereas that of groups with after-stroke duration of >10 to 20 years and >20 years was around 71 years. However, no significant difference in the age among subgroups was shown. The range of visit frequency was 2 to 15 times in all participants and subgroups. The average visit frequency for all participants was 8 times. In groups with after-stroke duration of ≤30 days, 31 to 60 days, 61 to 90 days, >3 to 6 months, >6 to 12 months, >1 to 2 years, and >20 years, the average visit frequency was approximately 8 times, whereas in groups with after-stroke duration of >2 to 5 years and >5 to 10 years, it was around 7 times and that for >10 to 20 years was 6 times. The Kruskal–Wallis test showed no difference in the visit frequency among subgroups.
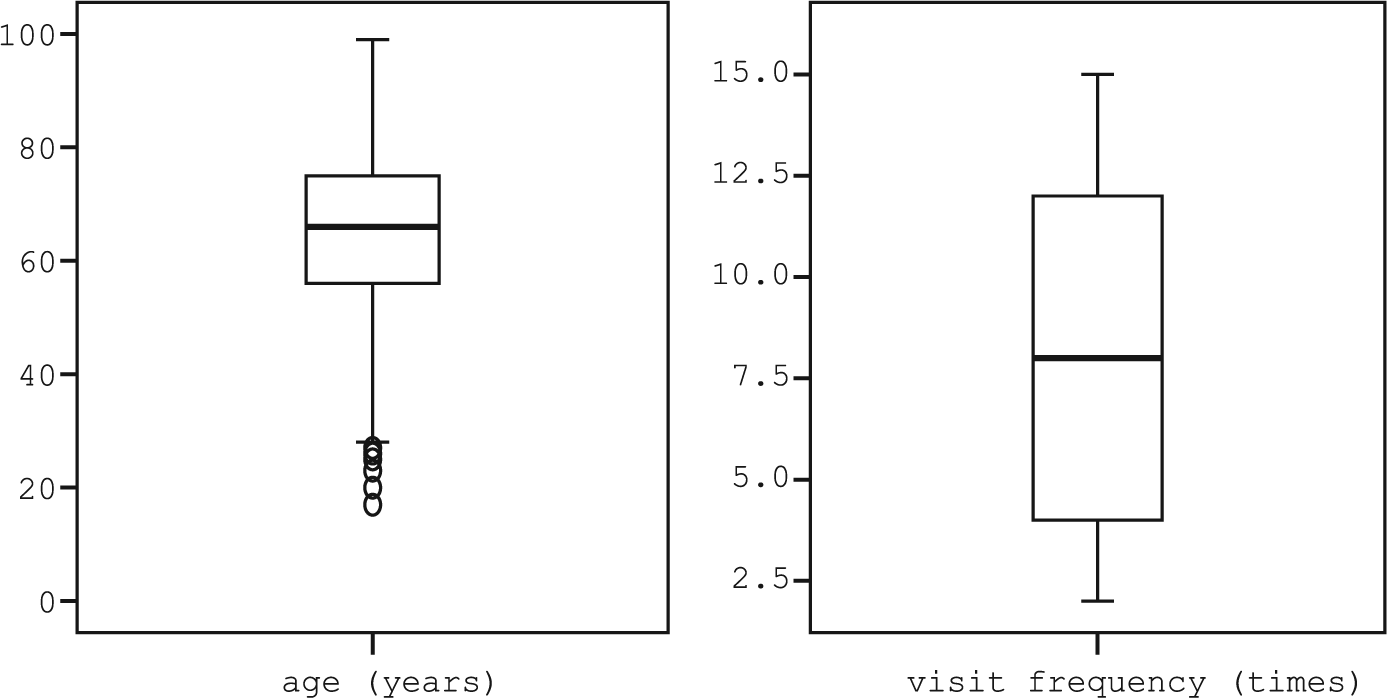
Boxplot of age and visit frequency for all participants.
Characteristics of Participants.
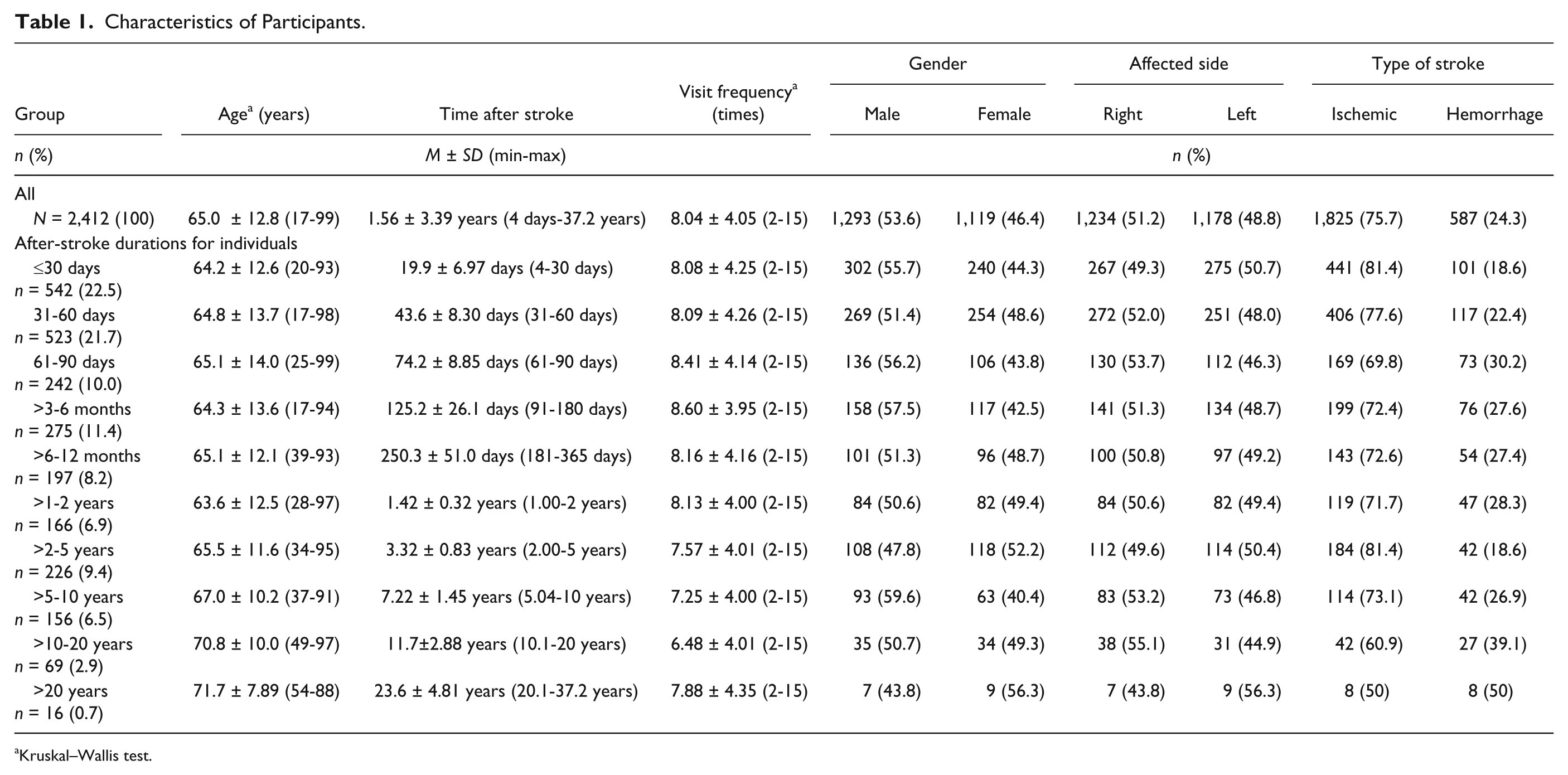
Kruskal–Wallis test.
The average duration after stroke for the whole group was 1.56 years. The number of males was close to females in the whole group and subgroups. The quantity of the affected side on the right was almost equal to that of the left. Most participants had ischemic stroke (Table 1).
As shown in Table 2, groups with after-stroke duration of ≤30 days, 31 to 60 days, 61 to 90 days, >3 to 6 months, >6 to 12 months, >1 to 2 years, >2 to 5 years, >5 to 10 years, and >10 to 20 years showed significantly (p < .0001) higher scores of STREAM-UE, STREAM-LE, STREAM-BM, complete STREAM, PASS-MP, PASS-CP, complete PASS, and complete BI after HBPT. Group with after-stroke duration of >20 years demonstrated a significant increase in scores of STREAM-LE (p = .027), STREAM-BM (p = .012), complete STREAM (p = .005), PASS-CP (p = .015), and complete PASS (p = .037) after HBPT.
Comparison of STREAM-UE, STREAM-LE, BM, and Complete STREAM; PASS-MP, PASS-CP, and Complete PASS; and BI Before and After Home-Based Physical Therapy Within Groups.
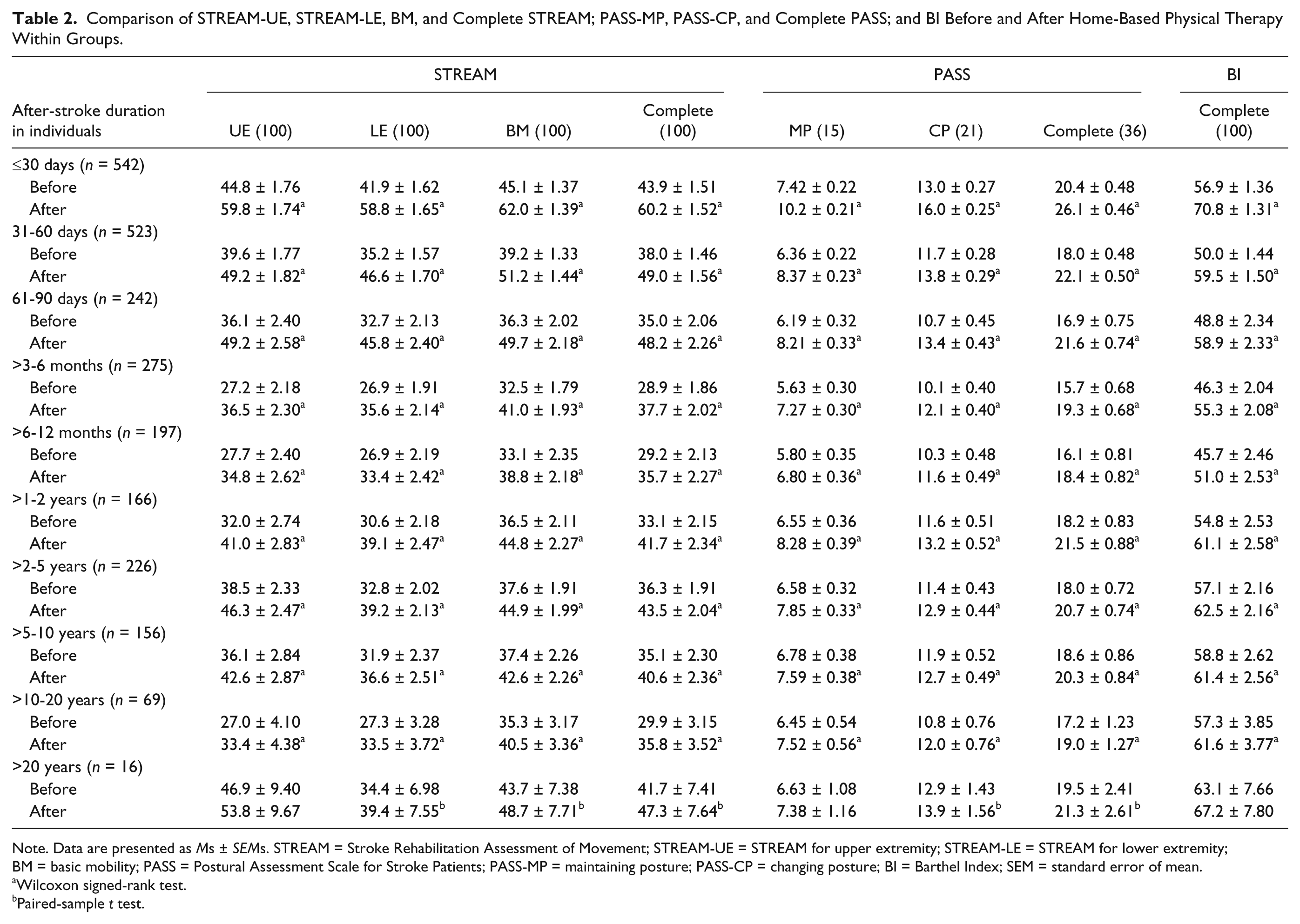
Note. Data are presented as Ms ± SEMs. STREAM = Stroke Rehabilitation Assessment of Movement; STREAM-UE = STREAM for upper extremity; STREAM-LE = STREAM for lower extremity; BM = basic mobility; PASS = Postural Assessment Scale for Stroke Patients; PASS-MP = maintaining posture; PASS-CP = changing posture; BI = Barthel Index; SEM = standard error of mean.
Wilcoxon signed-rank test.
Paired-sample t test.
Discussion
The study found that after HBPT individuals with after-stroke duration of ≤30 days, 31 to 60 days, 61 to 90 days, >3 to 6 months, >6 to 12 months, >1 to 2 years, >2 to 5 years, >5 to 10 years, and >10 to 20 years gained movement of upper and lower limbs and basic mobility, maintaining and changing posture, and ADLs, whereas those with >20 years had increased lower limb movement and basic mobility, and changing posture.
An increased score in STREAM, PASS, and BI revealed improvement in voluntary movement, postural balance, and ADLs, respectively. The finding showed benefit of HBPT for individuals with stroke, similar to previous studies.8-11 Moreover, the improvements demonstrated in all groups implied that HBPT was an advantage to individuals with stroke from early sub-acute to more chronic stage.
In the present study, physical therapists prescribed exercise to reduce spasticity, strengthen muscles, and train normal movement pattern. The finding showed movement, balance, and ADLs improvements that may be resulted from decreased muscle tone. A previous study showed that physical function improved if spasticity decreased. 20 In addition, physical therapists taught individuals with stroke, family members, and/or caregivers to do static or dynamic sitting and standing balance to enhance balance performance. Doing ADLs requires balance in sitting and standing while upper and lower limbs are moving. An increase in ADLs performance in the present study was comparable with several previous reports.8-10 The finding might be from the progression in voluntary movement and postural balance. This might be explained by interaction between body function impairment and activity limitations in the International Classification of Functioning, Disability, and Health model,21-23 and a good relationship between motor performance and ADLs in individuals with stroke. 24 However, in this study, individuals with post-stroke duration of >20 years demonstrated improvement in lower limb and basic mobility, and changing posture, but not ADLs. This might be because they had the highest or full adaptation in ADLs performance, or changes in lower limb movement, basic mobility, and postural balance might be inadequate to recover a difficult ADLs, for example, using stairs.
The present study obtained data from the actual working situation. Then, physical therapists did both evaluation and exercise prescription. However, they were blinded for the study. Therefore, the findings were reliable. The present data combined any type and severity of stroke and were for those with first stroke. Thus, the results could be generalized to apply to individuals with first stroke receiving HBPT. The number of participants in the group with post-stroke duration >20 years was small. A larger number of those is suggested in a future study to provide a clear effect of HBPT on such individuals. In summary, the study is an evidence to support the advantage of HBPT that it may be an option to access physical therapy after stroke, particularly in Thailand.
Conclusion
HBPT improves voluntary movement, postural balance, and ADLs in individuals with after-stroke duration of <20 years, whereas enhances only voluntary movement and postural balance in those with duration of >20 years. In Thailand, HBPT could promote physical performance in individuals after any period of first stroke and could help those who are unable to receive physical therapy in hospitals or private clinics.
Footnotes
Acknowledgements
The authors thank the following organizations and individuals for their supports of this research: National Health Security Office (NHSO), Bangkok branch, Thailand, for initiation of the Project of Stroke Care in Community and financial support to operate the project; Physical Therapy Council, Thailand, for cooperation to introduce the Project of Stroke Care in Community; all participants; physical therapists: Sompong Pamoncanasavit, Pattarawan Pattamaprapanont, Tippawan Kaewmanee, Sujila Wamaket, Wararat Trakolwitthayakij, Sumitta Pokaew, Patpaphanun Kongranakunroj, Parinya Rachalotorn, Jammaree Masthong, Usa Bonphen, Yodnuchit Loepongsanon, Pannarat Pansamai, and Siwaporn Thobang; Rongrong Maiman for document management in the project; and Thwe Zar Chi Thut for her proofreading.
Authors’ Note
Certificate of study approval: MU-IRB 2008/412.0312.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.