
Abstract
Up to 25% of patients hospitalized with heart failure (HF) are re-admitted within 30 days. The highest risk of re-admission is within the first days after discharge. Transitional care programs usually only involve nurses and physicians. The purpose of this study was to describe a post–acute care program including physical therapists and to evaluate re-admission rates following program implementation. The program provided HF-specific training encouraging nurses and physical therapists to assess HF status and instruct on self-monitoring. Thresholds for communication with medical providers were established. Patient groups before (n = 162) and after implementation (n = 300) were similar. Following implementation, there was a 16% decrease in re-hospitalization with little change in the number of visits. Similar multidisciplinary programs may impact re-hospitalization rates and health care costs for HF.
Keywords
Introduction
The first days after transitioning from hospital to home can be a vulnerable time for patients with heart failure (HF). An estimated 5.7 million Americans have HF. 1 Projections show prevalence of HF in the United States will increase to 46% by 2030,1,2 and direct medical costs of HF to increase from $31 billion in 2012 to $70 billion in 2030. 2 Elders with HF have the highest re-hospitalization rates of all adult patient groups. 1 Up to 25% of patients hospitalized with HF are re-admitted within 30 days,3-5 and the highest risk of hospital re-admission is within the first 2 to 5 days. 5 With increased attention to re-admission rates over the past several years, the HF population has become a focus of policy and programming. In 2012, the Centers for Medicare and Medicaid Services initiated use of 30-day re-hospitalization rates as a health care metric, incentivizing health systems to reduce re-admission rates for persons with HF. 4 In response to this policy and with increased focus on value-based care, health systems look to develop programs to improve outcomes and reduce re-admission rates for persons with HF. The term transition of care is often used for programs designed to reduce re-admissions by helping patients transition from one setting to the next setting, most often hospital to home.4,6,7 Transitional care interventions, in general, focus on coordinated and integrated care among health professionals and patient or caregiver education.4,6
In HF, most transitions are from hospital to home, and re-hospitalization is the most common outcome assessed in the literature. 6 Nurses are cited as the providers and coordinators of care, with patient assessment occurring shortly after the patient returns home. 6 Recommended strategies to reduce re-hospitalization include systematic planning and implementation with clear communication and collaboration between health care providers, patients, and families. Programs consistently incorporate monitoring and managing signs and symptoms of worsening HF.6-8 Also emphasized is the importance of specialized trained professionals managing and monitoring signs and symptoms of HF and providing appropriate self-management training. In most published programs, the specialized trained professionals are physicians and nurses. 7
Multidisciplinary management programs are included in the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) practice guidelines for patients at high risk for hospital re-admission. 9 Although multidisciplinary collaboration is shown to decrease all-cause 30-day re-hospitalization, less than half of transitional programs are interdisciplinary. Most interdisciplinary programs describe collaboration between physicians and nurses although a broader list of professionals has been suggested to provide education to patients.7,10 Most home care agencies include physical therapy professionals in the multidisciplinary team for their patients, but HF literature describing transitional care programs does not include the physical therapist (PT) as part of the multidisciplinary team.
Functional limitations associated with HF,11,12 the need to monitor activity,9,11 and the AHA recommendations for regular physical activity 9 suggest that physical therapy referral is appropriate. No studies were found, however, documenting the PT as part of a multidisciplinary transition to home program. The PT was not included in monitoring or educating patients on HF signs and symptoms, nor in providing ACCF/AHA recommended monitoring of activity tolerance. 13 Studies support exercise14-16 and functional training17,18 for patients with HF; however, most do not report re-hospitalization as an outcome. The few reporting this outcome found decreased hospitalizations when PTs provided these interventions in clinics,10,19 but they do not address the home care setting.
The purpose of the study was to describe a standardized multidisciplinary post–acute transitional care (MDTC) program that included PTs and to evaluate the effect on all-cause re-admission rates in patients with HF. A secondary aim was to evaluate the effect of the MDTC program on visit number and pattern of visit delivery.
Methods
The MDTC program was designed based on literature supporting specialized interdisciplinary care and collaboration, with frequent and early monitoring of HF signs and symptoms, and systematic implementation. The program included referring physicians, nurses, and PTs within a suburban hospital home care agency. The major components of the MDTC program included two education sessions for therapy and nursing staff, coordination of home visits between nursing and therapy, automatic physical therapy referrals, and standardization of documentation and interdisciplinary communication. The study was approved by the Abington Health Institutional Review Board.
The program was implemented on October 1, 2009. Data were collected from medical records for patients discharged from the home care agency July 1, 2009, through March 1, 2010, providing data 3 months before program implementation and 6 months following implementation. Patients referred to the home care agency who were 18 years of age and older and had a primary diagnosis of HF were included. HF diagnosis was determined by having an International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code of 428.x. Patients on hospice care were excluded. Any patients admitted to the agency prior to protocol implementation but discharged after October 1 were also excluded.
Description of the MDTC Program
Education
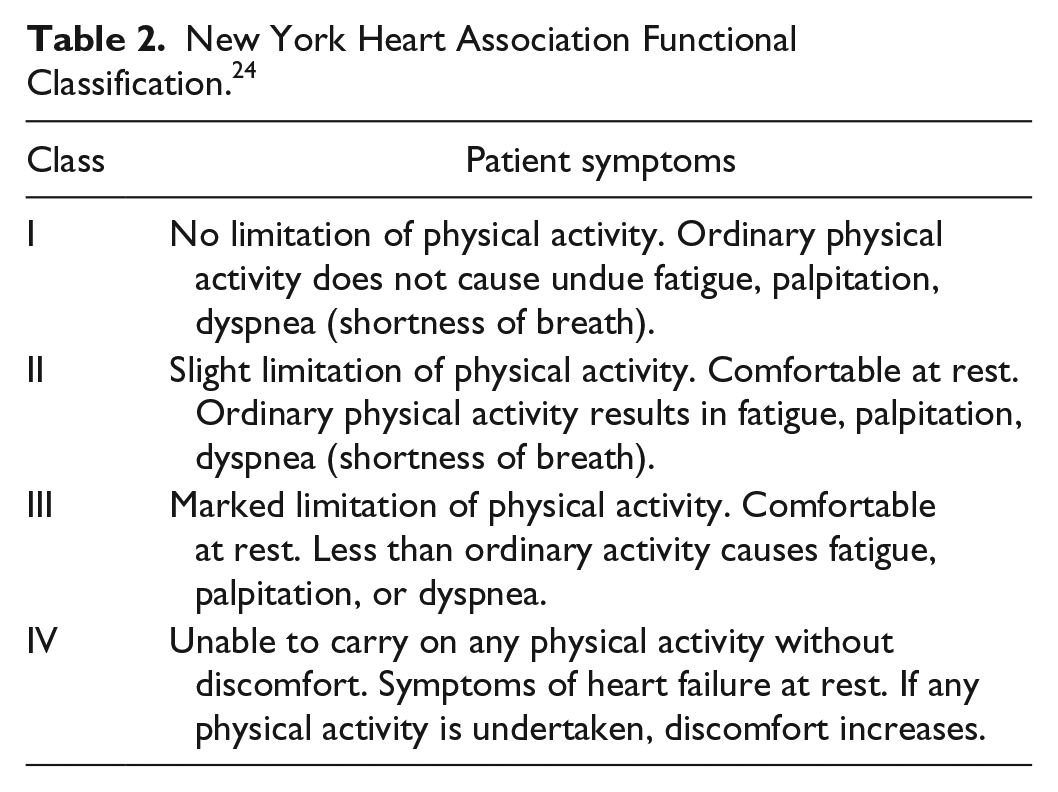
Managers from physical therapy and nursing provided educational sessions during two, 1-hour agency staff meetings. Education sessions for the PTs included a general review of pharmacological and medical management of HF and focused training on recognizing signs and symptoms of exacerbation of HF as outlined by the AHA20-22 and home health best practices. 23 In the MDTC program, PTs were trained and expected to assess and document vital signs and HF symptoms during each visit (in addition to nurses) and to communicate as needed to medical providers. Table 1 lists expected HF assessment items including classifying the patient, based on the New York Heart Association’s (NYHA) functional classification 24 that was embedded within the electronic medical record (Table 2). Table 1 illustrates the established thresholds for HF signs indicating communication to medical providers.20,24 Therapists were also trained to educate patients on self-monitoring and when to contact the nurse or physician. The PT’s plan of care for the patient visit was modified based on these signs and symptoms. To standardize documentation of activity tolerance, the therapists were trained to use the 6-minute walk test19,25 and the Borg Perceived Exertion Scale.26,27 All 24 PTs within the agency received the education. Education sessions for all nurses on the HF team included review of HF assessment items (Tables 1 and 2), the role of therapy in assessing and managing patient activity level, and the role that the PTs play in also assessing signs and symptoms of HF.
MDTC Program: Expected Assessment Items and Thresholds for Communication.
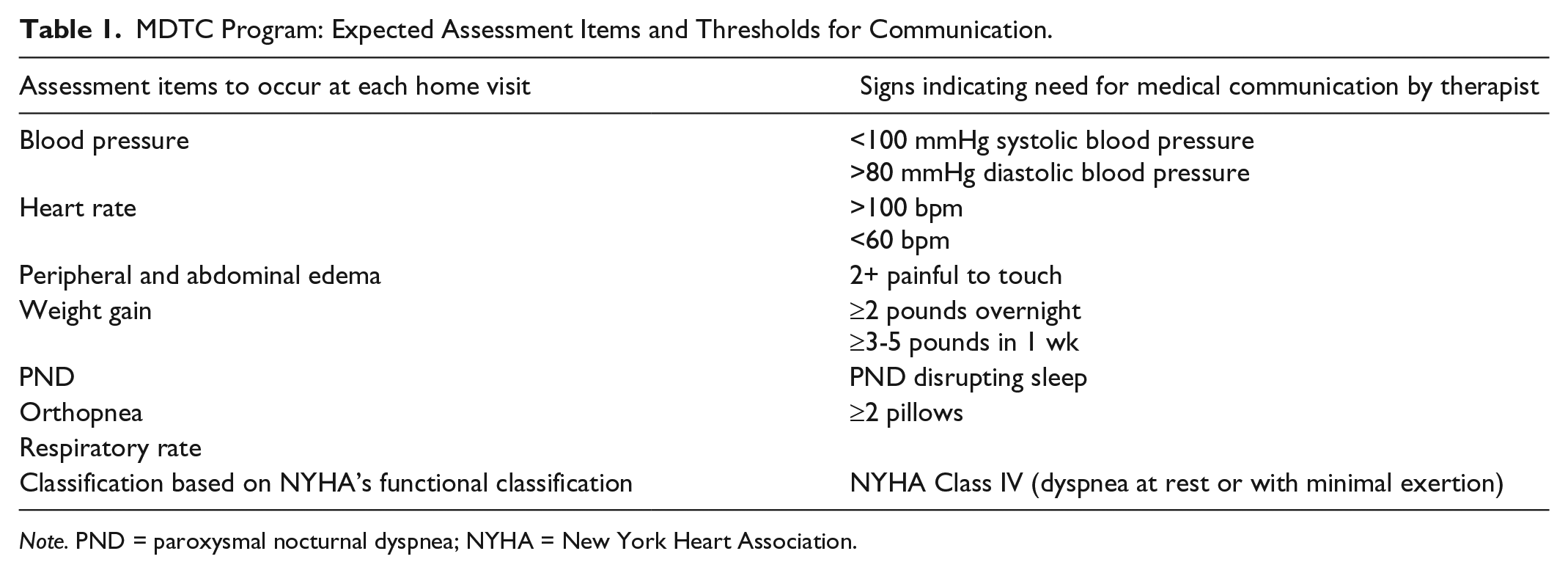
Note. PND = paroxysmal nocturnal dyspnea; NYHA = New York Heart Association.
New York Heart Association Functional Classification. 24
Agency admission, scheduling, and documentation
To address the high-risk re-admission period during the week following hospital discharge, 5 a coordinated visit pattern was implemented during the first 2 weeks after hospital discharge. The goal was to maximize the number of professional visits in the early weeks of home care. In the first 2 weeks, therapy and nursing staff provided care on alternate days. The MDTC program implemented new agency admission protocols. Based on recommendations supporting patient education on activity levels22,23 and the value of exercise for patients with HF,9,14,18,19 all patients referred to the home care agency with a diagnosis of HF received a consult for physical therapy services in addition to nursing visits. Documentation was standardized within the electronic medical records so that both therapists and nursing staff could easily view patient status during prior visits. The NYHA HF scale was embedded within the electronic medical record for use in patient classification.
Data collection and analysis
Data were obtained through de-identified reports created using the Crystal data extraction tool linked to the McKesson electronic documentation system. The reports extracted data and created spreadsheets. Based on established predisposing factors, patient demographics5,28 and disease severity, according to the dyspnea scale, were obtained from the Outcome and Assessment Information Set (OASIS). Demographic data included, gender, age, race, insurance, and comorbidities. Re-hospitalized records were obtained from the OASIS transfer forms. Re-hospitalization was tracked during, but not beyond, the agency episode of care. Patient visit numbers and admission and discharge dates were acquired from home care documentation.
To describe the sample, means with standard deviations and ranges were calculated for discrete and continuous data. Frequencies were determined for nominal and ordinal data. To determine whether the samples before and after program implementation were similar, characteristics were compared using a two-tailed independent t test or chi-square analysis. Re-hospitalization for the two groups was compared using chi-square analysis. The number of visits for each patient during the first 2 weeks was counted with group means calculated and comparison made using an independent t test. All statistical analyses were performed using SPSS version 19, with p values less than .05 considered to indicate significance.
Results
A total of 462 patient records were included in the study, 162 records prior to implementation and 300 records after program implementation. The sample had a mean age of 81 years, and was 51% female and predominantly Caucasian. The five most frequent conditions were hypertension, atrial fibrillation, coronary artery disease, diabetes, and chronic obstructive pulmonary disease. The average number of comorbidities for each group was 5.3 (range, 1-11). Nearly half of the patients were enrolled under Medicare (48.4%). The most common score reported for OASIS M1400 Dyspnea Scale was 2 (dyspnea with moderate exertion). Table 3 provides demographic characteristics for the group as a whole and for groups before and after the MDTC program. Based on independent t tests and chi-square analysis, no statistical difference was found between the two groups.
Sample Demographics.
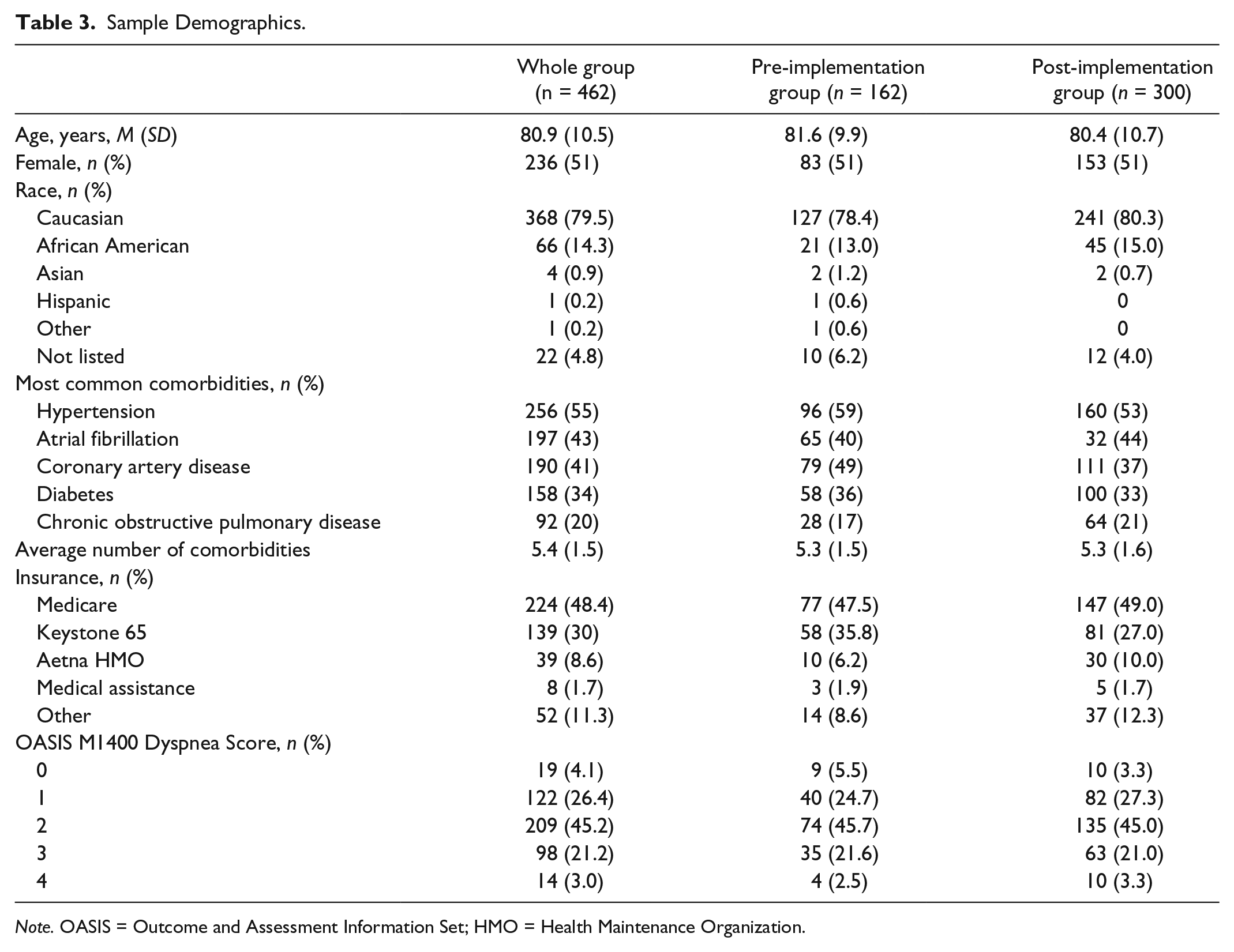
Note. OASIS = Outcome and Assessment Information Set; HMO = Health Maintenance Organization.
All cause hospital re-admission during agency episode of care was significantly reduced after the MDTC program, χ2(1, N = 462) = 13.36, p < .001. Re-hospitalization rates for the group receiving the MDTC program (23.4%) was 16.1% less than for the group prior to implementation (39.5%). Results of t tests, comparing the number of patient visits, indicated that during the first 2 weeks of care, there was a significant decrease in the total number of nursing and PT visits combined (p = .007). There was also a significant decrease in visits by each discipline, PT (p = .008), nursing (p = .026), and the total days of care provided to the patient (p < .001). The decrease, however, was less than a single visit for each comparison (Table 4).
Patient Visit Patterns for Nursing and Physical Therapy During the First 2 Weeks.
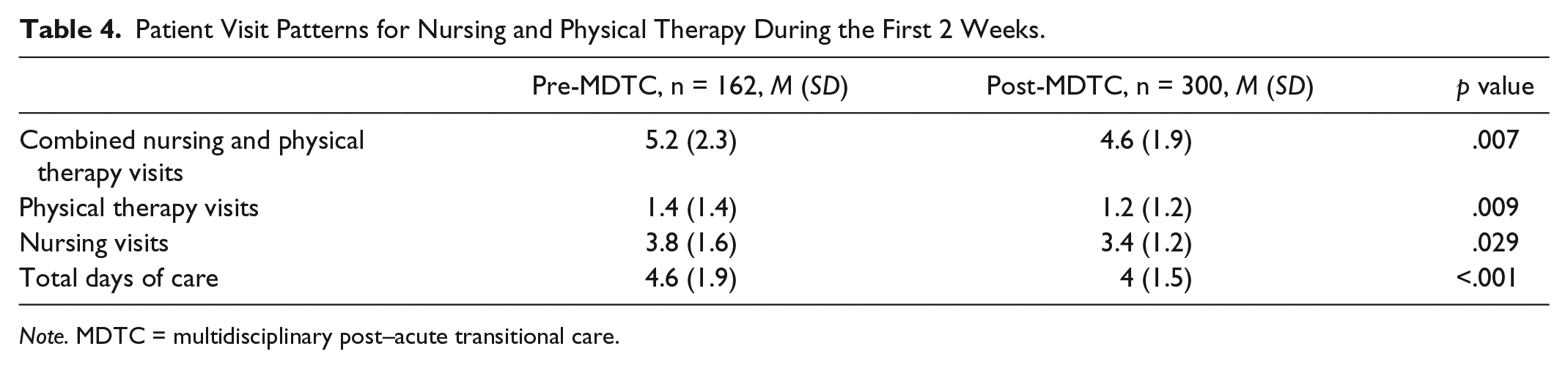
Note. MDTC = multidisciplinary post–acute transitional care.
Discussion
This study examined changes in re-hospitalization rates and visit patterns before and after implementing a new MDTC program. Fewer patients were re-hospitalized during the new program. The results also indicated fewer home care visits were provided, with a difference of less than 1 visit. Our mean nursing visit intensity is similar to intensities associated with improved patient status. 28 These results suggest the content of each visit during the MDTC program changed, providing greater benefit than visits prior to program implementation. It is believed that there was more focus on patient education during these visits. The staff training sessions for both nurses and PTs focused on encouraging patient education and self-monitoring at each visit. Patient education is a class I recommendation in the ACCF/AHA guidelines for management of HF 22 and has been reported to decrease re-hospitalization in HF. Even a single one-on-one patient education session by a nurse educator showed a 51% reduction in re-hospitalization when compared with a standard discharge process. 29
The MDTC program also added specialty training for signs and symptoms of HF to PTs as well as nurses. Perhaps more professionals specifically monitoring HF symptoms enhanced early recognition of decline and the defined triggers for medical communication to enhance medical management of HF symptoms. Our results are consistent with literature supporting the importance of early monitoring and effective inter-professional communication following hospital discharge.4,6 Although the studies did not include physical therapy, multiprofessional teamwork and communication was a major theme that emerged from Albert’s systematic review of transitional care programs aimed at reducing re-hospitalizations. 6 There are few published studies including the PT in the multidisciplinary transitional care team for individuals with HF. Naylor et al 30 included PTs in the team of HF experts used to train advanced practice nurses helping patients with HF during home follow-up. Results showed an increased length of time to hospital re-admission. When PT was included in daily multidisciplinary meetings for hospital patients with HF, transition to skilled nursing facility was lower, but 30-day re-admission rate did not differ. 31 Our results support professional perspectives encouraging PTs take a more active role in monitoring and communication during transitions to home. 32
The MDTC program training sessions may have enhanced therapist’s confidence in monitoring patients during functional training and exercise and to report on changes in status. Although physiologic changes from exercise would not be expected before 8 to 12 weeks,15,17 comfort in monitoring and adapting activities during sessions and in instructing the patient on activity monitoring may have enhanced patient mobility and function. Standardized functional assessment tools are recommended in the literature, 32 and their use in our MDTC program may have enhanced monitoring and communication. Explicit attention to functional deficits is lacking in transitional care models32,33 even though evidence links functional abilities, in the immediate post-hospitalization period, to re-admission risk.11,15,31,32,34 This study supports the role of physical therapy in the multidisciplinary care of patients with HF recently discharged from the hospital to home. It encourages further research on collaborative care models in the home care setting.
Several limitations should be considered when interpreting results of this study. Although the patients in the sample were consistent with HF populations in literature, the results represent a single home care agency during a limited time frame and may not be generalizable to other populations. Data were dependent on the accuracy of medical records and extraction from those records. Specifics about what occurred during individual sessions were not available from the medical record. Although training was provided to all staff, there was no method utilized to measure compliance with training expectations. Also, no post-training assessment was included. Visit patterns could have been affected by issues surrounding reimbursement policy (managed care co-pays encourage PT and nursing visits on the same day) and by difficulty obtaining proper authorization.
There is general support for a multidisciplinary approach to help patients with HF transition to home, but additional research is necessary to address the role and interaction of the various disciplines, including physical therapy. Unique and important elements that different disciplines bring to transitional care need to be studied to address critical health care professionals who should be included into care models. For physical therapy specifically, studies emphasizing the role of the PT in addressing activity and function during transitions need to be conducted. Our study did not address program costs or financial impact. Future work should include methods addressing value-based transitional care.
The purpose of the study was to evaluate the effect of MDTC program on all-cause re-admission rates. Our MDTC program included PTs along with nurses and physicians in providing care to patients with HF recently discharged from the hospital to home. Re-hospitalization rates were lower for the group admitted after implementation. Results point to the potential value of including PTs in post–acute care for homebound patients with HF. Results also suggest the value of specialty training sessions, frequent assessment of HF symptoms by multiple professionals, and clarity on when to communicate with medical staff. Similar multidisciplinary care programs may impact re-hospitalization rates and ultimately patient outcomes and health care costs for the HF population.
Footnotes
Authors’ Note
Project presented at the Combined Sections Meeting for the American Physical Therapy Association meeting February 2011, Home Health Section Platform Session.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.