
Abstract
Medicare requires that home health patients have a face-to-face visit with a physician when services are initiated and that physicians provide certification of this encounter before home health agencies (HHAs) can be reimbursed. We assessed an intervention to increase completion of face-to-face certification by hospital physicians at discharge using a retrospective chart review. We found a shift in the source and timeliness of certification among intervention hospitals. Pre-intervention, hospital physicians completed face-to-face certifications for 18.7% of patients and community physicians completed certifications for 47.2% (p < .001), compared with 44.4% and 24.3% (p < .001) post-intervention. Shifting the source of certification from community to hospital physicians helped HHAs by reducing the burden of tracking down certification from community physician offices and facilitating timely care for recently hospitalized patients.
Keywords
Introduction
Home health agencies (HHAs) support millions of Medicare beneficiaries each year during vulnerable transitions to home after hospital discharge. 1 In 2014, approximately 3.5 million beneficiaries received home health services from nearly 12 000 HHAs, 2 allowing individuals to remain in their homes and prevent the complications, stress, and costs associated with unplanned hospital readmissions.3,4,5
Home health documentation requirements have evolved over time to prevent fraud and to promote communication during transitions between health care settings. For example, the Centers for Medicare & Medicaid Services (CMS) has required since 2011 that patients receiving home health services have a face-to-face encounter with a physician shortly before or after initiation of services. Physicians must provide certification of these face-to-face encounters to HHAs before the agencies can be reimbursed. 6 However, HHAs often begin their home visits without all the paperwork needed for reimbursement so they can provide timely support for patients recently discharged from the hospital.
While hospital physicians often initiate home health referrals at the time of hospital discharge, they usually defer completion of the face-to-face certification to community physicians. As a result, HHAs may expend substantial resources tracking down the face-to-face certification from a community physician after the patient has been discharged from the hospital. A collaborative of HHAs in Rhode Island partnered with Healthcentric Advisors, the Medicare Quality Innovation Network-Quality Improvement Organization (QIN-QIO) in New England, to raise awareness about face-to-face certification requirements among hospitals in the state. The goal of the hospital outreach was to increase completion of face-to-face certification of HHA referrals by hospital physicians at the time of discharge. In response, most hospitals in Rhode Island modified their discharge processes to embed face-to-face certification into the routine discharge paperwork for patients referred for home health services.
The purpose of this study is to examine whether the hospital intervention increased completion of face-to-face certification by hospital physicians who referred Medicare beneficiaries for home health services. We hypothesized that modifying the hospital discharge process to include face-to-face certification would increase the timeliness of referrals and the percent of referrals with complete paperwork, thus removing a barrier to safe care transitions for recently discharged patients.
Methods
Intervention
Healthcentric Advisors, in its role as the New England Medicare QIN-QIO, collaborated with a group of HHAs to increase completion of face-to-face certification by hospital physicians. A group of health care leaders and stakeholders known as the Rhode Island Healthcare Advisory Board, convened by Healthcentric Advisors, sent a letter to executives at every nonfederal acute care hospital in Rhode Island in August 2015. The letter described the patient safety concerns related to incomplete face-to-face certification and suggested that hospital physicians complete the required paperwork when they make the home health referral at discharge.
Healthcentric Advisors tracked the implementation of new discharge processes in the state’s hospitals through periodic communication with hospital staff. Eight of the 11 hospitals in the state reported implementing new processes at discharge to incorporate face-to-face certification into the routine discharge paperwork for patients being referred for home health services. Some of the hospitals modified their paper transition of care summary forms to include certification of a face-to-face encounter. For example, one hospital using paper forms at discharge added new fields to their forms based on the HHAs’ recommendations. These fields prompt the discharging physician to provide the needed information for face-to-face certification, such as the date of the most recent face-to-face encounter, why the patient is homebound, and the need for skilled home services. When the physician signs the discharge paperwork, the face-to-face certification is included. Other hospitals modified the discharge module in their electronic health record (EHR). For example, a hospital linked the “home with services” order in their discharge module to a new screen that prompted the discharging physician to specify that there was a face-to-face encounter with the patient, that the patient is homebound, and that there is a need for skilled home services. A message then appears in the physician’s EHR inbox, requesting their signature to complete the certification. The eight hospitals implemented these changes at varying time points throughout the study period.
Participants
We recruited a convenience sample of HHAs in Rhode Island to measure the impact of the changes to the hospital discharge process. All HHAs in the state were invited by email to participate. Recruitment presentations were also delivered to home health care trade association members and to participants in a statewide home health collaborative. The collaborative is convened quarterly by the New England QIN-QIO to provide a forum for home health professionals to participate in shared learning and quality improvement activities.
Data Collection
Staff at each recruited HHA collected data by retrospective chart review monthly from July 2015 to May 2016. Each HHA was instructed to abstract data from the charts of the first 10 Medicare beneficiaries each month who were referred from a hospital for home health services and who had at least one completed home care visit. HHAs used a standardized data collection tool to determine whether the face-to-face certification had been completed within 30 days of hospital discharge. The tool could be completed on paper or in Excel. Patient-level information abstracted from the charts consisted of the following:
Date of home health referral
Discharging hospital and whether the patient was discharged from an inpatient medical service, inpatient surgical service, or the emergency department
Payor
Date face-to-face certification was received by the HHA (if applicable)
Source of face-to-face certification (discharging hospital physician vs. community physician)
Date of the first home care visit
Number of home care visits completed in the first 30 days after discharge.
HHA characteristics (type of ownership and Quality of Patient Care Star Rating) are publicly available and were downloaded from CMS’s Home Health Compare website. 7
Data Analysis
We categorized each home health referral as either a pre-intervention referral or a post-intervention referral. Pre-intervention referrals were referrals sent from hospitals prior to implementation of any change in their discharge process and from hospitals that did not modify their discharge process at all during the study period. Post-intervention referrals were referrals originating from hospitals after they modified their discharge processes to include face-to-face certification. We excluded referrals originating from any site other than a hospital.
Our primary outcome was the percent of referrals with complete face-to-face certification within 30 days of hospital discharge. Chi-square tests were used to compare the percent of referrals with complete face-to-face certification among pre-intervention referrals versus post-intervention referrals. Descriptive statistics were used to examine characteristics of referrals and to evaluate whether there were differences in the outcome by the hospital setting from which patients were discharged (emergency department [ED], medical, or surgical) or by payor. All analyses were performed using Statistical Analysis Software (SAS) Version 9.3. The study was approved by the Institutional Review Board at Rhode Island Hospital.
Results
Eight HHAs signed participation and data use agreements for the study; one dropped out before collecting data. The majority of participants were privately owned, for-profit agencies (n = 5, 71.4%), and the mean Quality of Patient Care Star Rating was 3.6 Stars at the time of the study. No major differences in ownership or average Quality of Patient Care Star Rating were noted between participating (N = 7) and nonparticipating agencies (N = 20) in Rhode Island (private ownership, 75.0%, and mean Quality of Patient Care Star Rating, 3.5). The seven agencies audited 495 charts from July 2015 to May 2016. Referrals originated from all 11 nonfederal acute care hospitals in Rhode Island. Most referrals were from medical inpatient wards, followed by surgical wards, with no major differences by intervention status. Approximately half of all referrals (n = 243) were pre-intervention referrals. Referral characteristics by intervention status are found in Table 1.
Home Health Referral Characteristics, Stratified by Intervention Status (N = 495).
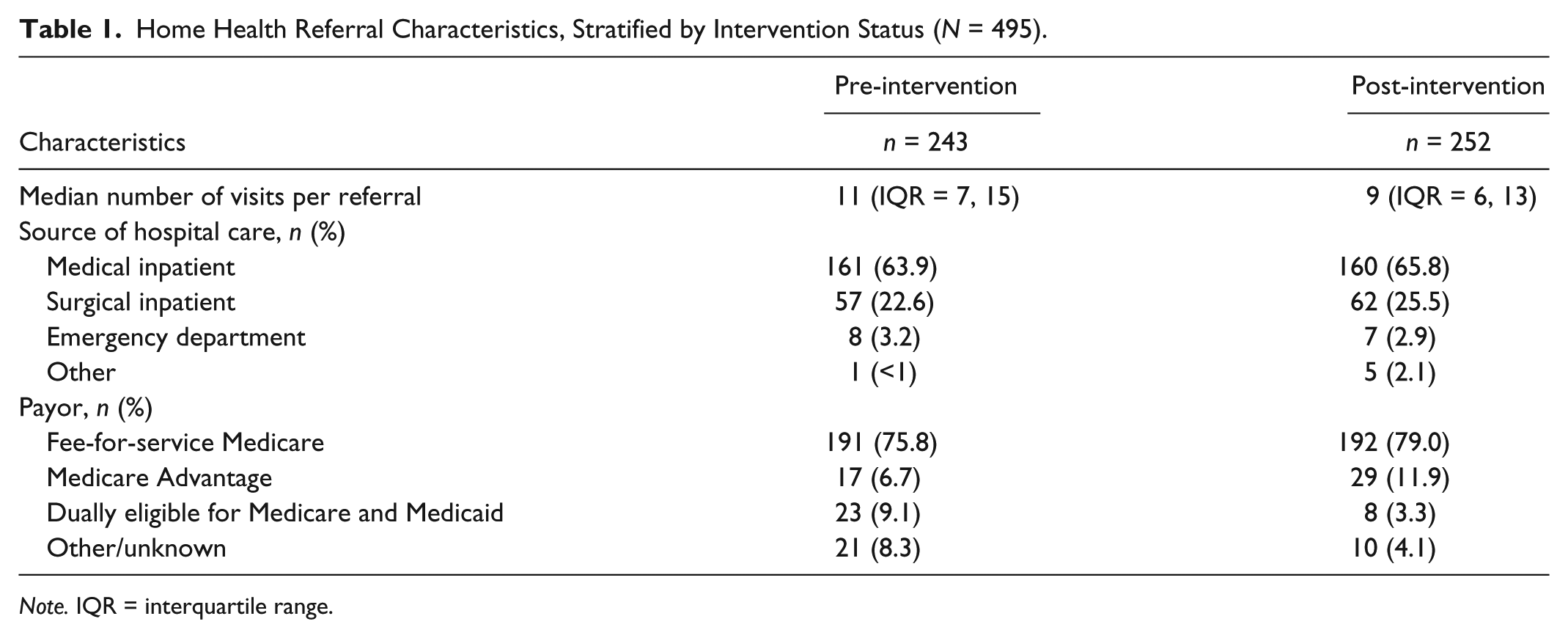
Note. IQR = interquartile range.
The percent of referrals with complete face-to-face certification remained unchanged after the intervention (65.9% pre-intervention vs. 68.7% post-intervention). However, there was a shift in the source of face-to-face certification among hospitals that implemented the intervention. Specifically, pre-intervention, hospital physicians completed face-to-face certifications for 18.7% of home health referrals, while community physicians completed certifications for 47.2% of referrals (p < .001). Post-intervention, hospital physicians completed certifications for 44.4% of referrals, while community physicians completed certifications for 24.3% of referrals (p < .001) (Figure 1).
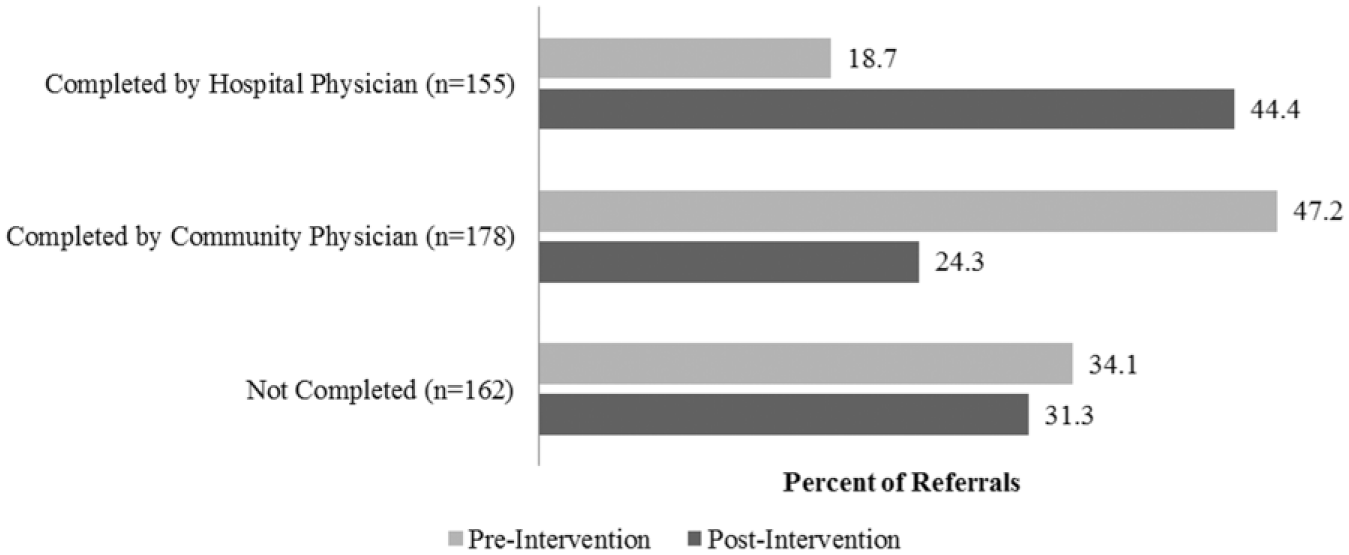
Source of face-to-face certification, pre-intervention versus post-intervention (N = 495 referrals).
Face-to-face certifications by hospital physicians were more likely to be completed within 4 days of the initial home health referral; 82.6% of face-to-face certifications from hospital physicians were received by the HHA within 4 days of the referral versus 19.0% from community physicians (Figure 2). On average, it took longer for HHAs to receive the face-to-face certification when completed by community physicians (a mean of 4.7 days for hospital physicians compared with a mean of 30.2 days for community physicians).
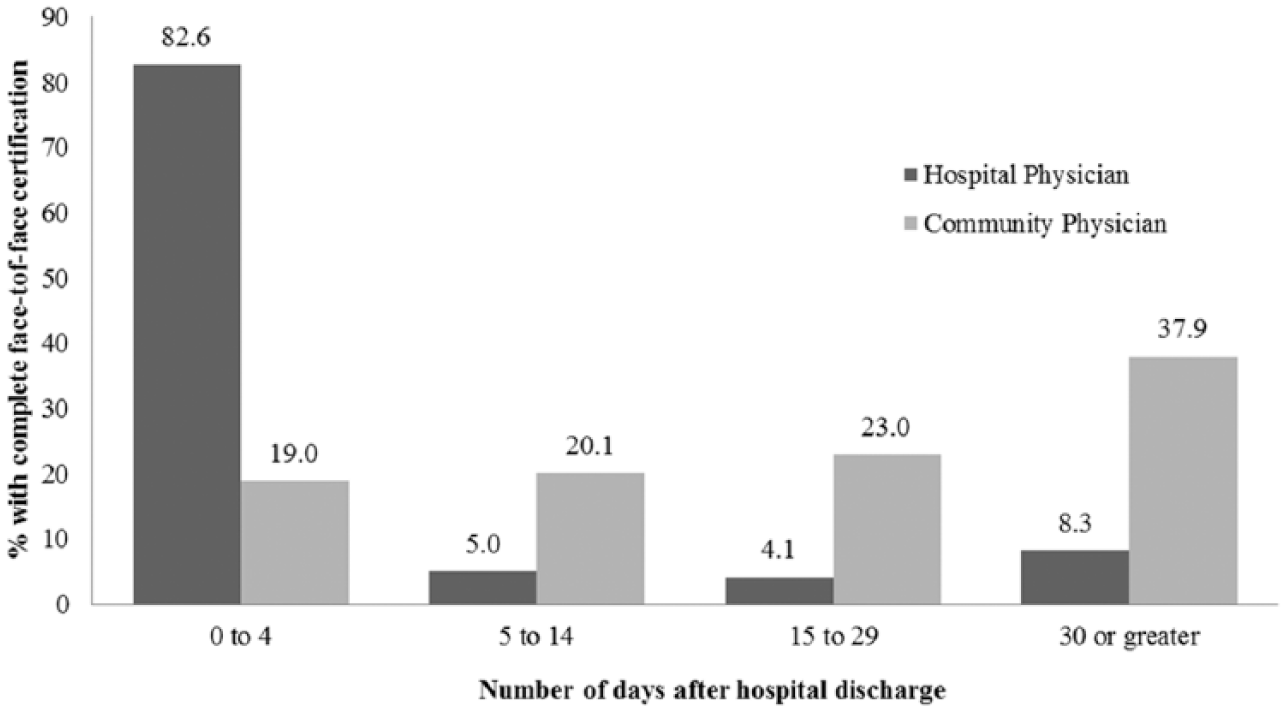
Number of days after hospital discharge for home health agencies to receive complete face-to-face certification, by source of certification (N = 292).
HHAs made home visits regardless of whether they had received the face-to-face certification, as shown in Figure 3, which depicts the number of home visits within 30 days of discharge, stratified by certification completion status. The seven participating HHAs completed 1,795 home visits within 30 days of patient discharge without face-to-face certification.
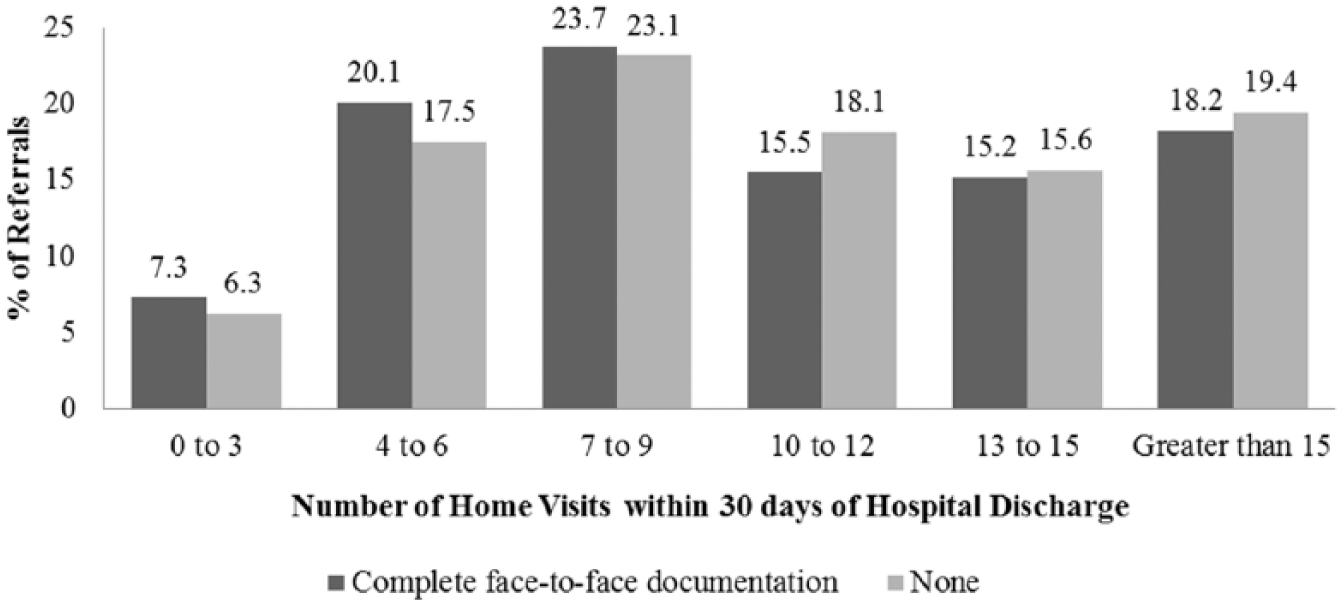
Number of home visits per patient within 30 days of discharge, by completion status of face-to-face certification.
Discussion
We observed an increase in the percent of face-to-face certifications provided by discharging hospital physicians after hospitals changed their discharge processes; the certification source shifted from the community physician to the discharging hospital physician, with the overall completion rate remaining at around two-thirds of referrals. Despite the overall completion rate remaining at two-thirds post-intervention, the shift in source of the certification to hospitals means that HHAs were more likely to receive the paperwork needed for reimbursement within a few days of receiving the referral. This shift reduced the substantial effort needed to track down certifications from community physician offices.
Little is known about the impact of the face-to-face certification on HHAs or patient care. One study found that a similar requirement for Medicare’s hospice benefit may decrease hospice use. 8 A 2014 report by the Office of the Inspector General found that more than 30% of submitted HHA claims had insufficient documentation of a face-to-face encounter, 6 which is consistent with our findings. A number of home health trade associations and other key stakeholders have addressed face-to-face certification as a barrier, arguing that aspects of the requirement inhibit HHAs’ ability to provide timely care to patients and that agencies have little control over whether physicians provide needed paperwork.9,10,11
Participating HHAs reported spending considerable time and money tracking down physicians to request face-to-face certifications when it was not provided in the initial referral. These added expenses and allocation of clinical staff may threaten agencies’ solvency and may impact their ability to seamlessly care for patients during vulnerable transitions. Even with the hospitals’ efforts, about one-third of referrals still lacked the necessary certification 30 days after hospital discharge, putting the agencies at risk for not receiving reimbursement for services already rendered. We found that participating HHAs completed 1,795 home visits for patients whose referrals lacked face-to-face certification. Those 1,795 visits represent more than $220 000 in at-risk payments, based on an average Medicare skilled nursing visit reimbursement of $125 in calendar year (CY) 2015. 12 If the HHAs in this study had declined to provide care to patients without complete face-to-face certification, almost a third of patients in this sample would have been left without timely home care, putting them at risk for readmission or potentially delaying their discharge back to the community.
Why are face-to-face certification rates so low? We suspect that the etiology is multifactorial. With the rise of hospitalists, many hospital physicians have never worked in the primary care setting and may not be aware of the documentation required for home health services. They may also assume that because they will not be following the patient in the community that they should not complete the certification or that there is a liability concern. Although community physicians as a group have more experience completing home health documentation, they may not know about this relatively new requirement. They may lack the information needed to complete the face-to-face certification if they have not seen the patient recently and may not be able to get patients in for a visit within the required time frame. In addition, the face-to-face certification process may feel time-consuming, burdensome, and not clinically useful. Community physicians may feel that completing the face-to-face certification is the hospital physician’s responsibility because the referral was initiated in the hospital. Finally, physicians in both settings have no financial incentive to comply because lack of certification does not affect their own reimbursement and traditionally HHAs have continued to see recently discharged patients without completed paperwork.
Despite these barriers, our findings demonstrate the value of collaboration, facilitated by a neutral convener (the regional QIN-QIO), among two traditionally siloed providers (HHAs and hospitals). This type of cross-setting partnership can help hospitals and HHAs to adapt in a rapidly evolving payment landscape and to align to provide high-quality patient care. Hospitals reported integrating face-to-face certification into their EHRs or discharge paperwork with minimal disruption, demonstrating that if hospitals are willing, the process is not a burden. Our results stress the continued need for ongoing collaboration between hospitals and community physicians, as well as more widespread education for all physicians about evolving home health documentation requirements.
Limitations
We note several limitations. First, the HHAs that chose to participate may be inherently different from those that did not, and therefore, our sample may not be representative of all agencies. Second, generalizability may be limited beyond Rhode Island due to the state’s small size and limited number of hospitals. Finally, bias may have been introduced into the data collection process; HHAs were not blinded to the purpose of the study. We instructed them to audit the charts of the first 10 Medicare beneficiaries referred for home health services meeting the inclusion criteria each month, but project staff did not validate adherence to the protocol. An interpretation issue was identified early on in our data collection form: “Discharge date” was updated to “hospital referral date” for consistency. Project staff regularly reached out to participating agencies to answer questions and to reinforce data collection protocols.
Conclusion
These findings are relevant at multiple levels. First, a Medicare policy affecting home health reimbursement has potential patient care implications if it leaves patients at risk of not receiving needed services. Second, when hospitals modified their discharge process in response to HHA concerns, they removed important barriers to transitions between care settings. The former demonstrates the unintended downstream impact of a policy aimed to improve coordination, while the latter offers insight into cross-setting collaboration to improve patient safety. Ultimately, we hope these findings can raise further awareness and encourage additional research on the implications of the face-to-face certification requirement on HHA solvency and, most important, on patient care.
Footnotes
Acknowledgements
The authors thank the participating home health agencies for their time and commitment to this study.
Authors’ Note
The content of this publication does not necessarily reflect the views or policies of the U.S. Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsements by the U.S. government. The authors assume full responsibility for the accuracy and completeness of the ideas presented.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The analyses upon which this report is based were performed under IDIQ contract number HHSM-500-2014-QIN014I, Task Order Number HHSM-500-TMA01, funded by the Centers for Medicare & Medicaid Services, an agency of the U.S. Department of Health and Human Services.