
Abstract
Family caregivers make important contributions to home health care for older adults, but knowledge of the specific roles they assume is lacking. We analyzed data from 1,758 community-dwelling Medicare beneficiaries aged 65+ receiving Medicare-funded home health care between 2011 and 2016, using linked National Health and Aging Trends Study and Outcomes and Assessment Information Set data. Most (86.7%) beneficiaries receiving home health care had an identified need for family caregiver assistance, and nearly 6 in 10 (57.9%) had identified need for caregiver assistance with five or more tasks. After examining significant associations between older adult characteristics and identified needs for caregiver assistance with specific tasks, we identified three profiles of older adults who demonstrate similar patterns of identified need for family caregiver assistance during home health. These profiles include: (1) older adults with greater functional impairment who more often had identified need for assistance with Instrumental Activities of Daily Living, advocacy, or Activities of Daily Living; (2) older adults with cognitive impairment who more often had identified need for assistance with medication administration or supervision; and (3) older adults with greater clinical severity who more often had identified need for assistance with medical procedures and equipment. Findings support calls to develop training interventions and strengthen the partnership between home health providers and family caregivers. These three profiles present a potential framework for the development of family caregiver training programs.
Introduction
Family and unpaid caregivers are a vital source of support to older adults with chronic illness and/or functional impairment.1-3 Family caregivers are especially relevant to home health care. Given intermittent staff presence and the unique nature of providing care in the home environment, home health clinicians often rely on family caregivers to help manage older adults’ conditions and meet their health and functional needs.4,5 An emerging body of literature suggests that family caregiver characteristics and caregiving patterns affect health outcomes for older adults.6-11 This evidence has motivated efforts to assess and support family caregivers12-17 and has contributed to growing interest in understanding how home health providers may partner effectively with family caregivers to meet the demands of an increasingly complex patient population.18,19
The Centers for Medicare and Medicaid Services (CMS) recently enacted a policy that underscores the importance of family caregivers to home health. In 2017, the CMS updated the Conditions of Participation for Home Health Agencies to require that home health providers (1) assess family caregivers’ ability to provide assistance and (2) offer relevant training and education to family caregivers. 20 Unfortunately, there is currently limited quantitative information regarding the scope of family caregiver involvement during home health or the specific roles assumed by family caregivers—information that could help guide home health providers as they respond to this new CMS requirement. The Outcomes and Assessment Information Set (OASIS), filed by home health providers as part of every Medicare-funded home health episode, includes a section in which a home health clinician assesses the patient’s need for family caregiver assistance across a range of specific task categories. 21 However, no previous work has examined OASIS data to determine the prevalence of identified need for family caregiver assistance among older adults receiving home health or to explore associations between older adult characteristics and identified the need for family caregiver assistance.
Our study uses a novel data set, consisting of nationally representative survey data with linked OASIS assessments, to examine identified need for family caregiver assistance among community-dwelling older adults receiving home health. We determine the prevalence of identified need for family caregiver assistance with specific task categories, assess whether identified needs in various categories are correlated with one another, and identify profiles of older adult characteristics that are associated with identified need for family caregiver assistance with specific tasks. Results of this analysis may guide home health providers in developing and prioritizing training and education initiatives for family caregivers and add to the ongoing discussion surrounding the expanding role of home health in the continuum of health care services for older adults.
Methods
Data
We built a unique data set of 1,758 community-dwelling older adults who participated in the National Health and Aging Trends Study (NHATS) and received home health care within 1 year of NHATS interview. The NHATS is a nationally representative survey of Medicare beneficiaries aged 65 and above with rich information on respondents’ sociodemographic characteristics, social supports, and health and functional status. To construct our data set, we pooled the NHATS data from 2011 to 2015 with linked OASIS data from 2011 to 2016. We then identified individual respondents’ OASIS Start of Care filings during this timeframe and matched the OASIS filing for the index home health episode with the NHATS survey immediately preceding the index home health episode. Given our focus on the index home health episode, each respondent appears in the sample only once. We excluded NHATS respondents who did not experience any home health episodes during this period. We also excluded older adults who were identified in their NHATS interview as living in congregate settings such as assisted living and skilled nursing facilities due to the availability of supports that may substitute for or otherwise affect family caregiving.
Measures
Measures of older adult characteristics were drawn from both NHATS survey data and OASIS assessments. In order to understand older adults’ health status and family caregiving context prior to the home health episode, we incorporate self-reported data from NHATS on older adults’ sociodemographic characteristics, social support, cognitive impairment, functional impairment, and health status. Recognizing that there may be changes in health and function resulting from health events immediately preceding the home health episode, we include measures from the OASIS that reflect home health clinicians’ assessments of patients’ overall health status relating to cognitive impairment, functional impairment, clinical severity, and feelings of anxiety, as described in the following paragraph. Given emerging research demonstrating that a growing number of family caregivers are assisting with medically oriented tasks,16,22 we also include clinician reports of the presence of pressure ulcers or wounds from the OASIS. Finally, in response to growing awareness of differences in characteristics of patients referred to home health from the community versus those referred following an inpatient stay,23,24 we incorporate a measure of whether the home health episode is postacute. If the home health episode occurs within 14 days of inpatient acute or postacute care, we define this as a postacute episode.
We construct a measure of cognitive function during the home health episode based on the OASIS item 1700, which queries home health clinicians on “patient’s current . . . level of alertness, orientation, comprehension, concentration, and immediate memory for simple commands.” 21 Patients are considered to have no cognitive impairment if the home health clinician notes that they are “alert and oriented . . . comprehend and recall task direction independently,” moderate cognitive impairment if the home health clinician notes that they “require prompting . . . under stressful or unfamiliar conditions” or “require assistance and some direction,” and high cognitive impairment if the home health clinician notes that they “require considerable assistance in routine situations” or are “totally dependent.” 21 We construct measures of functional impairment and clinical severity during the home health episode using Health Insurance Prospective Payment System (HIPPS) codes in the OASIS data.25,26 These codes represent each patient’s Home Health Resource Group, which is used to adjust home health payments based on the patient’s expected resource use and clinical and functional status. 27 Health Insurance Prospective Payment System codes identify home health patients as falling into low, moderate, or high need in the clinical and functional domains. 26 We construct a dichotomous measure of feelings of anxiety during the home health episode based on OASIS item 1720, equal to 0 if the patient reports never feeling anxious and 1 otherwise.
We measure the identified need for family caregiver assistance during the home health episode using home health clinicians’ reports in the OASIS of patients’ need for nonagency caregiver assistance across seven task categories. 21 Although the OASIS items specify “nonagency caregiver,” we use the term “family caregiver” throughout this article, given that most of our sample reports having no paid caregiver assistance and that previous work demonstrates the important and unique role of family caregivers in home health.4,28,29 The seven task categories are defined in the OASIS as follows: 21
Instrumental Activities of Daily Living (IADLs): assistance with household tasks such as “meals, housekeeping, laundry, telephone, shopping, finances,”
Advocacy: assistance with patient’s “participation in appropriate medical care (for example, transportation to or from appointments).”
Activities of Daily Living (ADLs): assistance with self-care tasks such as “transfer/ambulation, bathing, dressing, toileting, eating/feeding,”
Medication administration: assistance with managing “oral, inhaled or injectable” medications,
Supervision: assistance with supervision or monitoring to ensure older adult’s safety “for example, due to cognitive impairment,”
Medical procedures: assistance with treatments or procedures such as “changing wound dressing, home exercise program,”
Equipment management: assistance with “oxygen, IV/infusion equipment, enteral/parenteral nutrition, ventilator therapy equipment.”
Analysis
We first calculated the percentage of older adults receiving home health who had an identified need for family caregiver assistance in each of the seven task categories, using NHATS survey weights and design variables to adjust for nonprobability sampling and produce nationally representative estimates. We then calculated the percentage with identified need family caregiver assistance in multiple task categories. We also created a correlation matrix of Phi coefficients showing the relationship between identified needs for pairs of task categories.
Next, we identified older adult characteristics associated with identified need for help in each task category. Given the interrelation of many of these variables and the exploratory nature of this work, we sought to assess each characteristic’s individual association with identified need. Therefore, we used bivariate, weighted logistic regression to produce unadjusted odds ratios (ORs). We examined a range of characteristics measured prior to the home health episode (drawn from NHATS), including sociodemographic characteristics and measures of social support and health status, as well as factors of interest measured during the episode (drawn from OASIS), including measures of patient’s cognitive impairment, functional impairment, and clinical severity. We then examined patterns of significant associations between older adult characteristics and identified the need for caregiver assistance with specific task categories to identify commonalities among older adults with an identified need for assistance with a given task category.
Results
Among an estimated 8.5 million older adults experiencing an index home health episode between 2011 and 2016, 39.7% were male, 21.2% were non-white, 16.9% were enrolled in Medicaid, and the average age was 79.5 years (Table 1). Identified need for family caregiver assistance with specific tasks during home health varied from a low of 20.4% for assistance with equipment to a high of 84.7% for assistance with IADLs (Figure 1). Less than 15% of older adults receiving home health were identified as having no need for family caregiver assistance. Most beneficiaries were identified as needing assistance in multiple task categories: 4.5% needed assistance with one to two task categories, 24.3% needed assistance with three to four task categories, and 57.9% needed assistance with five to seven task categories (Figure 2). Correlation in identified need for assistance by task categories ranged from 0.17 (between IADLs and equipment) to 0.77 (between IADLs and advocacy). Strong correlations (phi coefficient greater than 0.70) were found between IADLs and ADLs
Descriptive Characteristics of Community-Dwelling Older Adults Receiving Home Health Care between 2011 and 2016 (n = 1,758).
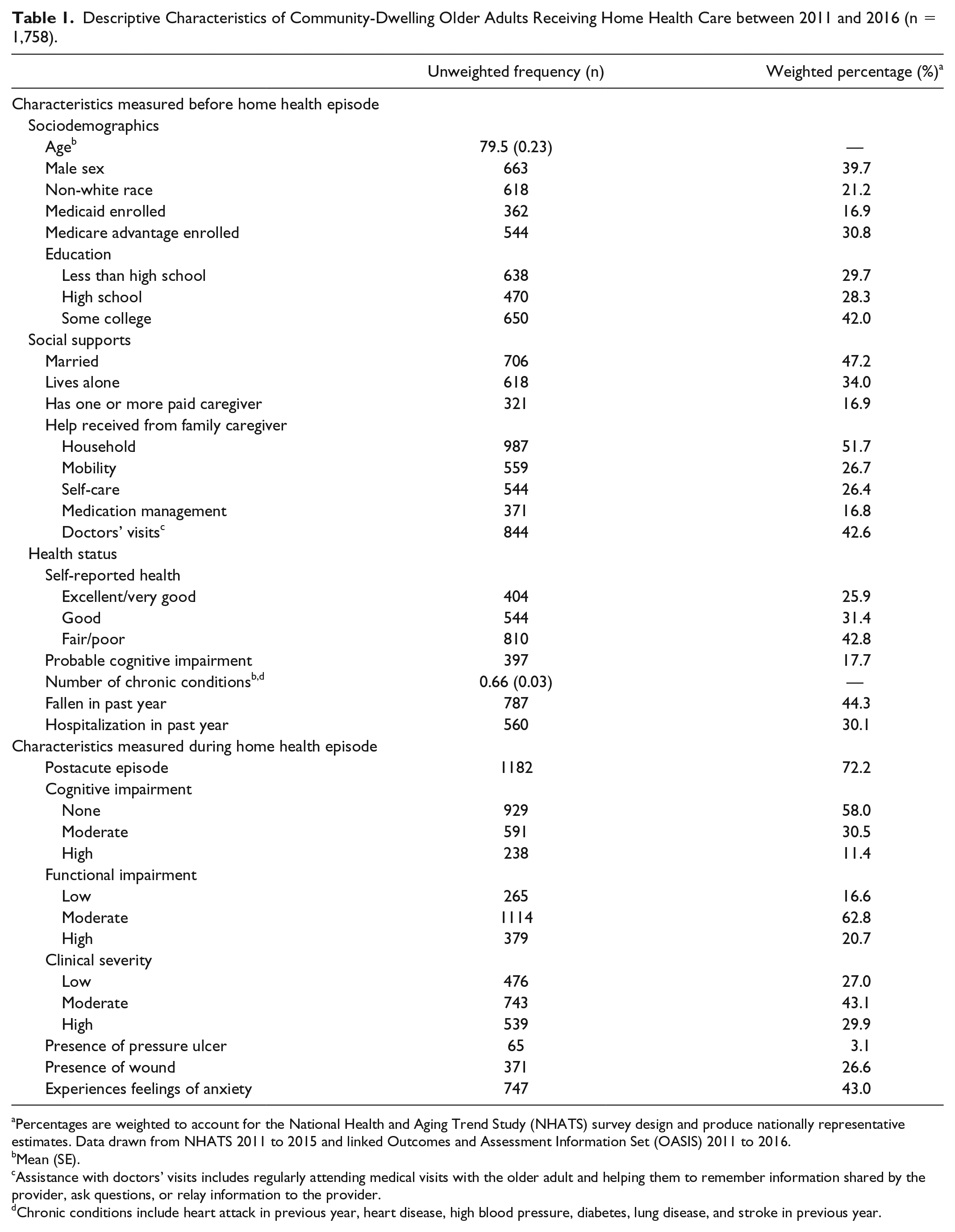
Percentages are weighted to account for the National Health and Aging Trend Study (NHATS) survey design and produce nationally representative estimates. Data drawn from NHATS 2011 to 2015 and linked Outcomes and Assessment Information Set (OASIS) 2011 to 2016.
Mean (SE).
Assistance with doctors’ visits includes regularly attending medical visits with the older adult and helping them to remember information shared by the provider, ask questions, or relay information to the provider.
Chronic conditions include heart attack in previous year, heart disease, high blood pressure, diabetes, lung disease, and stroke in previous year.
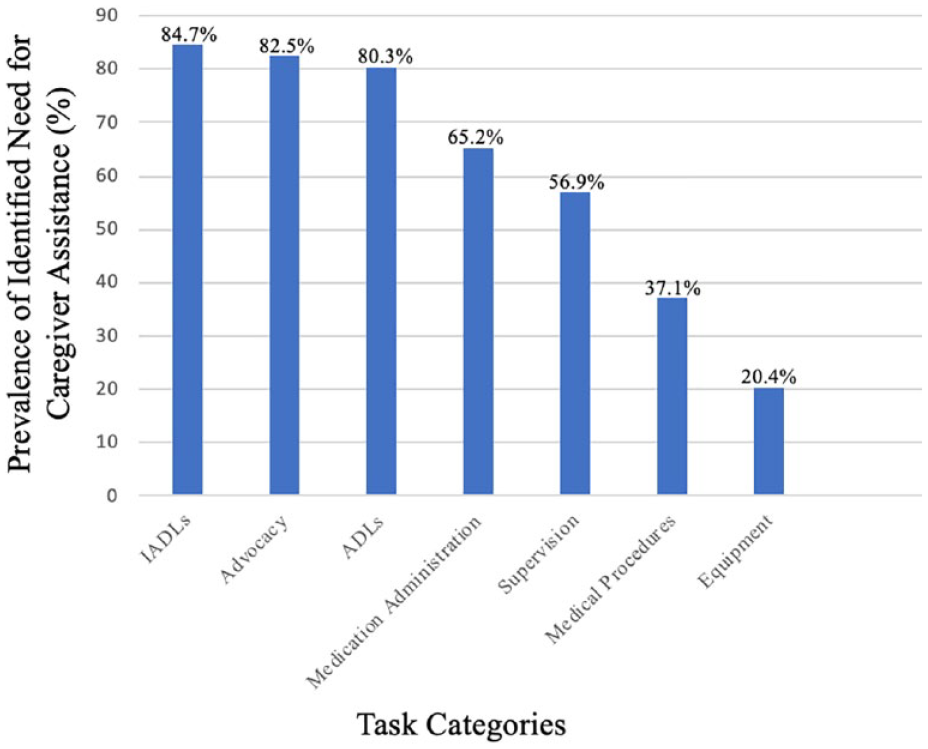
Identified need for family caregiver assistance among community-dwelling older adults receiving home health, by task category (n = 1,758)a.
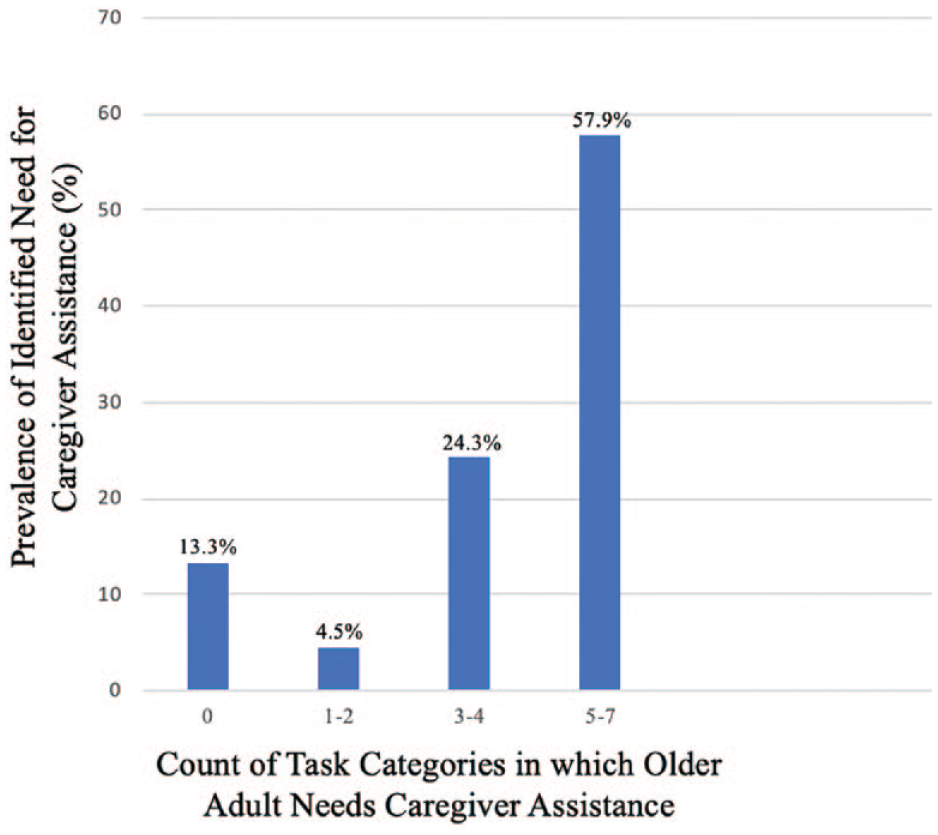
Identified need for family caregiver assistance in multiple task categories among community-dwelling older adults receiving home health (n = 1,758)a.
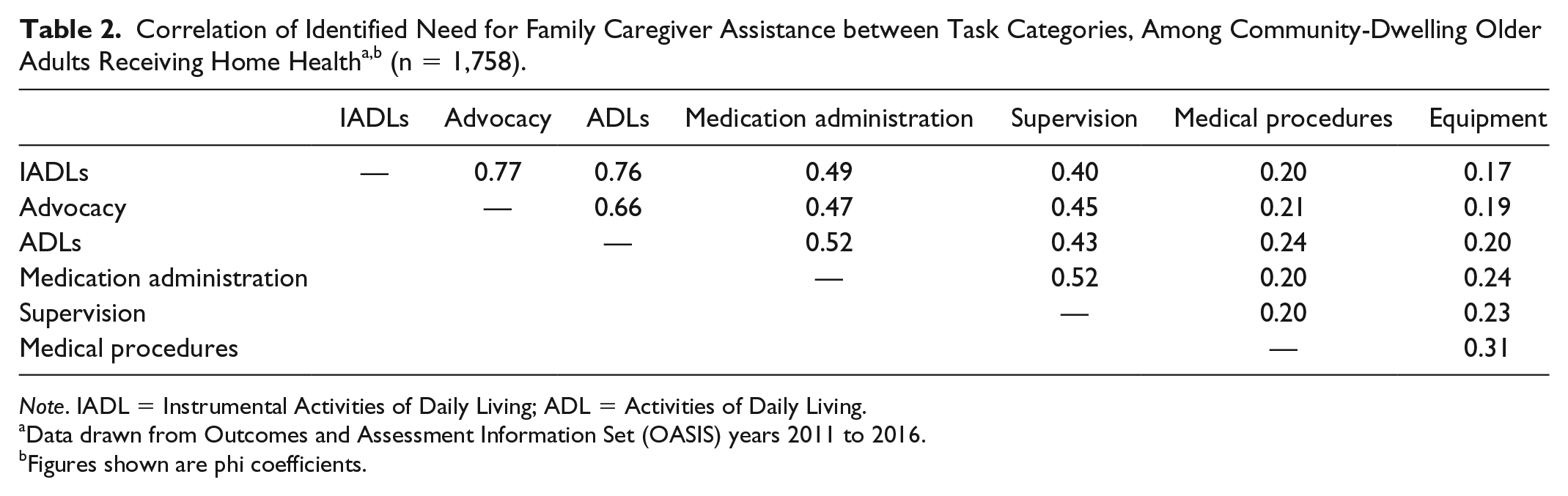
Note. IADL = Instrumental Activities of Daily Living; ADL = Activities of Daily Living.
Data drawn from Outcomes and Assessment Information Set (OASIS) years 2011 to 2016.
Figures shown are phi coefficients.
We observed important similarities in older adult characteristics that are significantly associated with identified need for family caregiver assistance across task categories. In the sociodemographic domain, we found that older age was associated with identified need for family caregiver assistance with ADLs (OR: 1.02, p < .05), medication administration (OR: 1.04, p < .001), and supervision (OR: 1.03, p < .001); that Medicaid enrollment was associated with identified need for family caregiver assistance with IADLs (OR: 2.46, p < .0001), advocacy (OR: 2.22, p < .01), ADLs (OR: 2.15, p < .001), medication administration (OR: 1.63, p < .01), and supervision (OR: 1.50, p < .01); and that higher educational attainment (some college compared to less than high school) was associated with lower odds of identified need for family caregiver assistance with IADLs (OR: 0.63, p < .05), ADLs (OR: 0.64, p < .05), medication administration (OR: 0.56, p < .001), and supervision (OR: 0.69, p < .001; Table 3).
Associations between Older Adult Characteristics and Identified Need for Family Caregiver Assistance During Home Health, Unadjusted Odds Ratios by Task Category (n = 1,758) a .
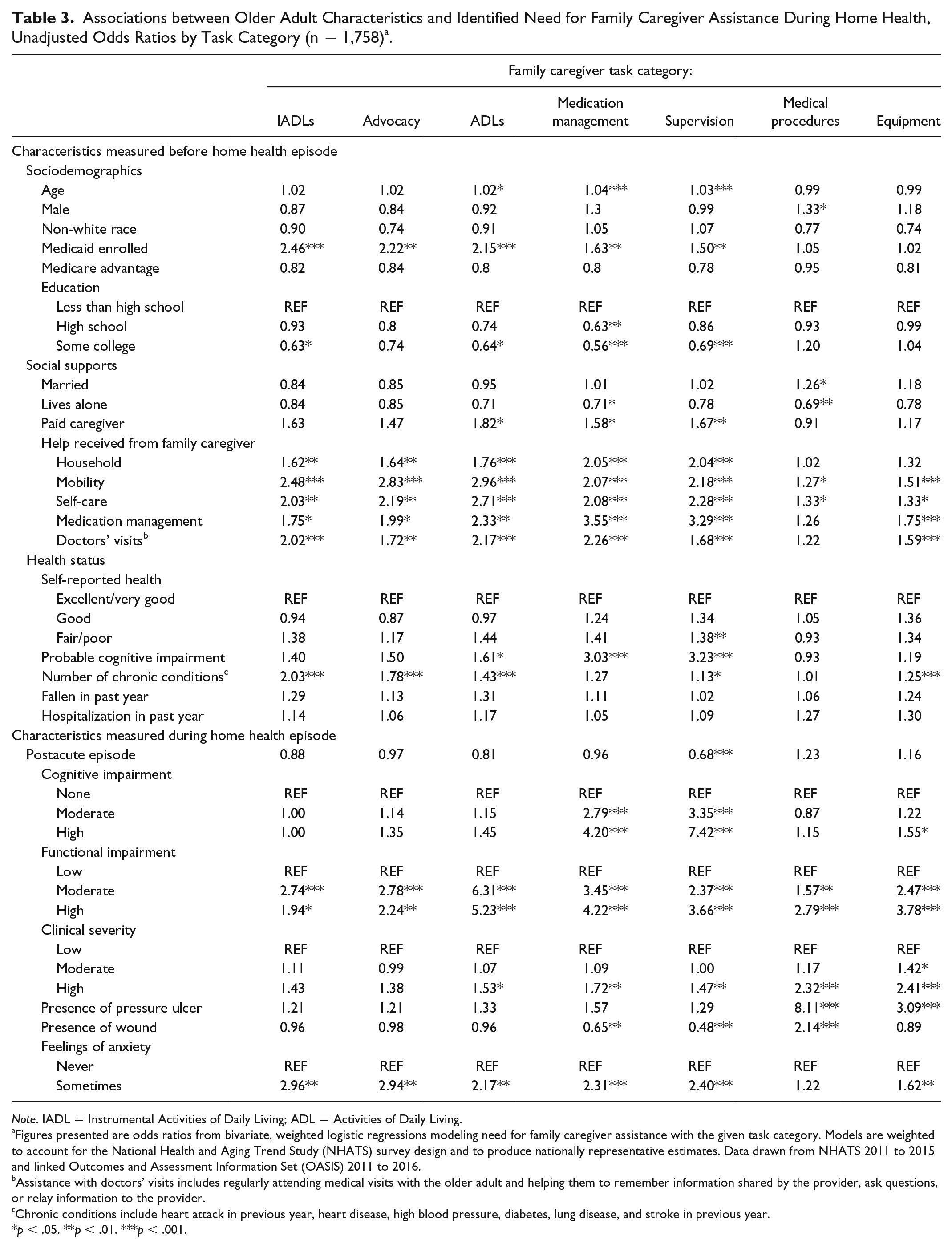
Note. IADL = Instrumental Activities of Daily Living; ADL = Activities of Daily Living.
Figures presented are odds ratios from bivariate, weighted logistic regressions modeling need for family caregiver assistance with the given task category. Models are weighted to account for the National Health and Aging Trend Study (NHATS) survey design and to produce nationally representative estimates. Data drawn from NHATS 2011 to 2015 and linked Outcomes and Assessment Information Set (OASIS) 2011 to 2016.
Assistance with doctors’ visits includes regularly attending medical visits with the older adult and helping them to remember information shared by the provider, ask questions, or relay information to the provider.
Chronic conditions include heart attack in previous year, heart disease, high blood pressure, diabetes, lung disease, and stroke in previous year.
p < .05. **p < .01. ***p < .001.
In the social support domain, we found that living alone before the home health episode was associated with lower odds of identified need for family caregiver support with medication management (OR: 0.71, p < .05) or medical procedures (OR: 0.69, p < .01). In addition, we found that receipt of family caregiver support before the home health episode was associated with identified need for family caregiver assistance across all tasks. Particularly strong associations were found between receiving assistance with mobility before the home health episode and the need for ADL assistance during home health (OR: 2.96, p < .001), receiving assistance with medication management before the home health episode and need for assistance with medication administration during the home health episode (OR: 3.55, p < .001), and receiving assistance with medication management before the home health episode and need for assistance with supervision during the home health episode (OR: 3.29, p < .001). Having any paid caregiver before the home health episode was associated with identified need for family caregiver assistance with ADLs (OR: 1.82, p < .05), medication administration (OR: 1.58, p <.05), and supervision (OR: 1.67, p < .01; Table 3).
In the health status domain, we found that fair or poor self-reported health before the home health episode was associated with identified need for family caregiver assistance with supervision (OR: 1.38, p < .01). In addition, we found that probable cognitive impairment before the home health episode was associated with identified need for family caregiver assistance with ADLs (OR: 1.61, p < .05), medication administration (OR: 3.03, p < .001) and supervision (OR: 3.23, p < .001). Having a greater number of chronic conditions before the home health episode was associated with identified need for family caregiver assistance with IADLs (OR: 2.03, p < .001), advocacy (OR: 1.78, p < .001), ADLs (OR: 1.43, p < .001), supervision (OR: 1.13, p < .05), and equipment (OR: 1.25, p < .001; Table 3).
Of characteristics measured during the home health episode, we found that postacute entry into home health, compared to community entry, was associated with lower odds of identified need for family caregiver assistance with supervision (OR: 0.68, p < .001). High (versus low) cognitive impairment during the home health episode was associated with identified need for family caregiver assistance with medication administration (OR: 4.20, p < .001) and supervision (OR: 7.42, p < .001). High (versus low) functional impairment during the home health episode was associated with identified need for family caregiver assistance with all tasks. High (versus low) clinical severity during the home health episode was associated with identified need for family caregiver assistance with ADLs (OR: 1.53, p < .05), medication administration (OR: 1.72, p < .01), safety and supervision (OR: 1.47, p < .01), medical procedures (OR: 2.32, p < .001), and equipment (OR: 2.41, p < .001). Presence of a pressure ulcer was associated with identified need for family caregiver assistance with medical procedures (OR: 8.11, p < .001) and equipment (OR: 3.09, p < .001), and the presence of a wound was associated with lower odds of identified need for family caregiver assistance with medication management (OR: 0.65, p < .01) and supervision (OR: 0.48, p < .001), but higher odds of identified need for family caregiver assistance with medical procedures (OR: 2.14, p < .001). Finally, feelings of anxiety were associated with identified need for family caregiver assistance with IADLs (OR: 2.96, p < .01), advocacy (OR: 2.94, p < .01), ADLs (OR: 2.17, p < .01), medication management (OR: 2.31, p < .001), supervision (OR: 2.40, p < .001), and equipment (OR: 1.62, p < .01; Table 3).
We identified three distinct profiles of older adults receiving home health who have similar patterns of identified need for family caregiver assistance. Profile 1 includes older adults with functional impairment who more often have identified need for assistance with IADLs, advocacy, and ADLs. Those who fit Profile 1 are more likely to be Medicaid-enrolled, to have received family caregiver assistance before the home health episode—particularly with mobility and self-care tasks—and to have more chronic conditions before the home health episode. Profile 2 includes older adults with cognitive impairment who more often have identified need for assistance with medication administration and supervision. Those who fit Profile 2 are more likely to be older, Medicaid-enrolled, have lower educational attainment, have received family caregiver assistance before the home health episode—particularly with medication management—and to have cognitive impairment both before and during the home health episode. Profile 3 includes older adults with greater clinical severity who more often have identified need for assistance with medical procedures and equipment. Those who fit Profile 3 are more likely to have high clinical severity and to have an ulcer or wound during the home health episode (Table 3).
Limitations
This work is subject to several limitations. First, we are unable to adjust for geographic information, including whether the patient resides in a rural community, which may impact home health access and delivery. Second, we rely on OASIS data to determine identified need for family caregiver assistance as well as patients’ health status during the home health episode. While prior work suggests that measures of cognitive impairment and function included in the OASIS have sufficient reliability and criterion and construct validity,30,31 OASIS measures of specific types of caregiver assistance have not been tested for reliability or validity and there are important gaps in the existing research regarding OASIS item reliability and validity. 31 Third, our study focuses on each beneficiary’s index home health episode and our findings may not be reflective of later episodes in a period of sustained home health use.
Discussion
We found that nearly 9 in 10 (86.7%) community-dwelling older adults receiving home health had an identified need for assistance from a family caregiver, based on home health clinician assessments. More than half (57.9%) were assessed as having an identified need for assistance from a family caregiver with five or more task categories. Identified need for family caregiver assistance was most common for IADLs, advocacy, and ADLs. Our work reveals significant associations between older adult characteristics and need for family caregiver support in specific task categories during a home health episode. Although there is a variation across task categories, overall those with an identified need for family caregiver assistance were more likely to be Medicaid-enrolled, to have lower educational attainment, to have been receiving family caregiver assistance before the home health episode, and to have greater functional impairment and experience anxiety during the home health episode. Study findings demonstrate that family caregivers are indeed crucial contributors to home health processes for older adults and often need to assist with a range of diverse tasks, including healthcare tasks. Study results lend support to growing calls for providers to better assess family caregivers’ needs and to offer appropriate training, education, and other supportive services,12-17 especially in the home health setting.18,20
We identified three distinct profiles of older adults receiving home health who have similar patterns of characteristics and identified need for family caregiver assistance. These include the following: Profile (1) those with functional impairment before the home health episode who are more likely to require family caregiver assistance with IADLs, advocacy, and ADLs; Profile (2) those with cognitive impairment who are more likely to require family caregiver assistance with medication administration and supervision; and Profile (3) those with greater clinical severity during the home health episode who are more likely to require family caregiver assistance with medical procedures and equipment. It is notable that these profiles reflect the relative prevalence of identified need across task categories—the percentage of patients needing family caregiver assistance is highest among tasks associated with Profile 1 (IADLs, advocacy, and ADLs) and lowest among tasks associated with Profile 3 (medical procedures and equipment). Although each patient is unique and a patient may have overlapping needs, our findings may guide providers who seek to develop training and education programs to better support the patients and families they serve. For example, training materials related to providing supervision for an older adult with cognitive impairment could be bundled with instruction on medication administration and a discussion of the medication reconciliation process. In addition, as CMS develops new home health payment models with the goal of better aligning reimbursement with patient characteristics and care needs,24,32 policymakers should consider the role of family caregivers in meeting care needs for certain patient subpopulations. Further research is warranted to better characterize patterns of resource use, as they relate to variation in home health patients’ reliance on family caregiving.
Our findings that Medicaid enrollment and educational attainment, indicators of a patient’s socioeconomic status (SES), are significantly associated with the need for family caregiver assistance across multiple task categories raise important questions about potential subjectivity of determining the need for family caregiver support. Given the correlation of lower SES with disability and poorer health, 33 lower SES may be related to true underlying vulnerabilities that drive the need for additional assistance among older adults. Alternatively, these differences may be the result of clinicians’ unconscious biases 34 when assessing a patient’s ability to independently manage their health and functional needs. This issue is worthy of further consideration, especially given CMS’s new mandate that home health providers assess family caregivers’ capability and need for education and training. 20 Given that family caregivers and care recipients generally share SES, clinical staff—both in home health and other clinical settings where family caregivers play a role—may need additional training to provide an unbiased assessment of family caregivers’ capabilities and needs.
In summary, we find that most of the older adults receiving home health need family caregiver assistance across multiple task categories, in addition to care from home health clinicians and staff. We note that older adults with greater functional impairment before the home health episode often need family caregiver help with IADLs, advocacy, or ADLs, that those with cognitive impairment often need help with medication management or supervision, and that those with greater clinical severity during the home health episode often need help with medical procedures or equipment. Study findings collectively suggest that home health agencies and clinicians would benefit from addressing the needs of family caregivers through assessment, education, and appropriate referrals to supportive services to facilitate delivery of high-quality care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the National Institute on Aging (grant no. R01AG047859) and the Agency for Health Care Research and Quality (grant no. T32HS0000029).