
Abstract
The objective of this study is to categorize the home health nursing care activities and hazards applicable to Indian settings, into high, medium, and low priority levels with the help of risk assessment table and risk matrix. The research design is exploratory and the study is cross-sectional, A self-administered questionnaire is prepared for Indian settings based on the literature review; the content validity and the internal consistency were ensured; the mean scores and the frequencies for the activities were calculated. The severity scores for the identified 14 perceived high-risk activities were assigned with the help of the brainstorming session. The hazard of slippery floors and exposure to blood fell into high priority area (denoted by red area) with high severity and high occurrence score, similarly overloaded and unsafe electrical outlets, rushing with clients, time pressure for reaching the client’s home, and contact with chemicals fell into medium priority category (denoted by yellow area). Finally, hazards such as uncontrolled pets and verbal abuse from patients fell into low priority levels. The providers should take measures for hazards such as slippery floors, overloaded and unsafe electrical outlets, rushing with clients, time pressure for reaching the client’s home, exposure to blood, and contact with chemicals, as these hazards fell into high-medium severity rating with high-medium probability.
Introduction
Home health care is a new concept for India and India’s aging population is pushing the growth of home health care market. 1 It is majorly present in metro cities such as New Delhi, Kolkata, Mumbai, Chennai, Hyderabad, and Bangalore. The home health service providers exist in two forms in India, that is, standalone units and as extended service in hospitals. In India, the home health providers deliver general health care services such as nursing care, medical care, physiotherapy, diet consultations, and sample collection; moreover, under specialty services, few home health service providers have started to provide sophisticated services such as dialysis at home, chemotherapy at home, and intensive care unit (ICU) at home. Home health care is not a new concept for developed countries, and in a study, it was found that home health nursing as a service segment comprised 67 present of total home care segment in the United States. 2 One decade earlier in the United States, it was considered as one of the fastest-growing sectors of the health care industry with 66% projected growth in the next 10 years; this sector even employed around 1,10,000 registered nurses in the year 2008. 3 However, the number of nurses working in the home health sector in India is not currently available but as per some reports, the home health care market in India is going to double in a year, 4 the numbers of nursing staff working in home health segment are surely going to increase in the coming times. Home health care as a sector currently in India is in nascent stage and mostly unregulated, hence there are not enough measures to implement and ensure occupational safety measures for health care workers working in this sector; hence, to get an overview of the current situation about the home health nurses occupational safety in India, the starting point can be an assessment of home health nurses perceived risks and hazards together with the experienced frequency of nursing tasks carried out by them every day for delivering care at home.
Literature Review
The probability of home health workers getting injuries is double than of hospital workers.
5
The home health nurse’s job gets more difficult as they have to work in an environment where they have very little control, and the home environment of clients may contain many health hazards. As per Occupational Safety and Health Administration (OSHA),
6
the home health hazards include bloodborne pathogens and biological hazards, latex sensitivity, ergonomic hazards from patient lifting, violence, hostile animals and unhygienic and dangerous conditions.
Some of these hazards are unique to home health care, such as animals, loaded firearms, violence in the home and neighborhood, and persons other than patients residing at home also can be a risk to the home health workers. 7 However, ergonomic hazards arising from patient lifting can lead to musculoskeletal injuries, such as sprains and strains, although this risk is there with traditional health care workers also, in the case of home health workers, it is higher as they have to do the heavy lifting alone and without the assisting devices. Moreover, it was found that in the United States, the rate of injury from lifting for home health care workers was 20.5% per 10,000 workers. 8 Similarly, home health workers are also at a great risk of infections from sharp injuries as they do not have proper access to sharp disposal bins and use whatever is available at home, such as mugs and plastic jars. In addition to that, they get distracted because of the presence of children and pets at home, thus increasing the chances of getting sharp injuries. 7 In a study, it was found that nurses working in developed countries’ home health organizations have also felt that the safety culture in the organization is compromised and the major reasons for that were lack of leadership, lack of routines, obsolete and irrelevant procedures, and lack of knowledge among home health nurses. 9 Similarly, in another study, the occupational health of home health aides was evaluated, and it was found that the most frequent hazards were related to musculoskeletal strain, exposure to potentially infectious agents, and experience of violence. 10 In another study focusing on home health care personnel dilemmas about the home hazards, the home hazards were classified into three categories electrical/fire, slip/trip/lift, and environmental exposures. 11
This study was planned to assess the perception of home health care nurses toward hazards associated with care delivery at home and the objective was to categorize the tasks associated with care delivery at home into different risk categories with an attached priority level for the management to address them.
Method
Sample and Procedure
The research design chosen for this study is exploratory; the primary objective of exploratory research is to explore a problem to provide further insights. This study is a survey-based cross-sectional research whereby a predesigned, structured questionnaire with face-to-face interview techniques is used for data collection. The sampling frame included home health nurses working in Bangalore, Delhi, and Mumbai; 425 home health nurses working in different organizations in these cities were approached with the help of home health organizations they were working with. The inclusion criteria were home health nurses with a minimum of 6 months of experience in the home health care industry. The systematic random sampling method was used after acquiring the list of nurses working in home health organizations. Out of 425 nurses approached, 397 nurses agreed to fill the questionnaire, with a response rate of 93%, out of the 397 filled questionnaires, 19 questionnaires were discarded because of incomplete responses to more than 40% questions, so finally 378 filled questionnaires were considered for the analysis, and out of the 378 filled questionnaires, 135 were from Bangalore, 109 from Mumbai, and 134 were from Delhi.
Instrument
The survey questionnaire consisted of three sections: Sections A, B, and C. Section A comprised of demographic questions, and section B consisted of a list of 28 hazardous tasks associated with home health nursing profession, which were supposed to be categorized into different risk categories ranging from no risk (1), mild risk (2), moderate risk (3), and high risk (4). It was decided that the activities having a mean score above 3.5 will be categorized as high-risk activities. In Section C, the respondents were asked to give a score based on the frequency they have to perform these home health nursing-related activities, where never = 1, sometimes = 2, and frequently = 3, the scoring system is used.
The questionnaire is prepared after reviewing the previous research studies done in other countries that have covered about hazards related to home health care professional’s tasks and tried to measure the perception of nursing students, 12 nursing aides,5,10 and home health nurses. 5 One study about the hazards associated with hospital-based nurses from Cyprus was also considered, 13 the relevant items for Indian settings were chosen for the study, and to ensure content validity, the questionnaire was reviewed by seven subject experts and the suggested changes were incorporated. The questionnaire was standardized by a pilot test on 50 patients and the required changes were done. The internal consistency of the questionnaire is measured by Cronbach’s alpha, which was found to be .77 higher than the threshold of .7.
Results
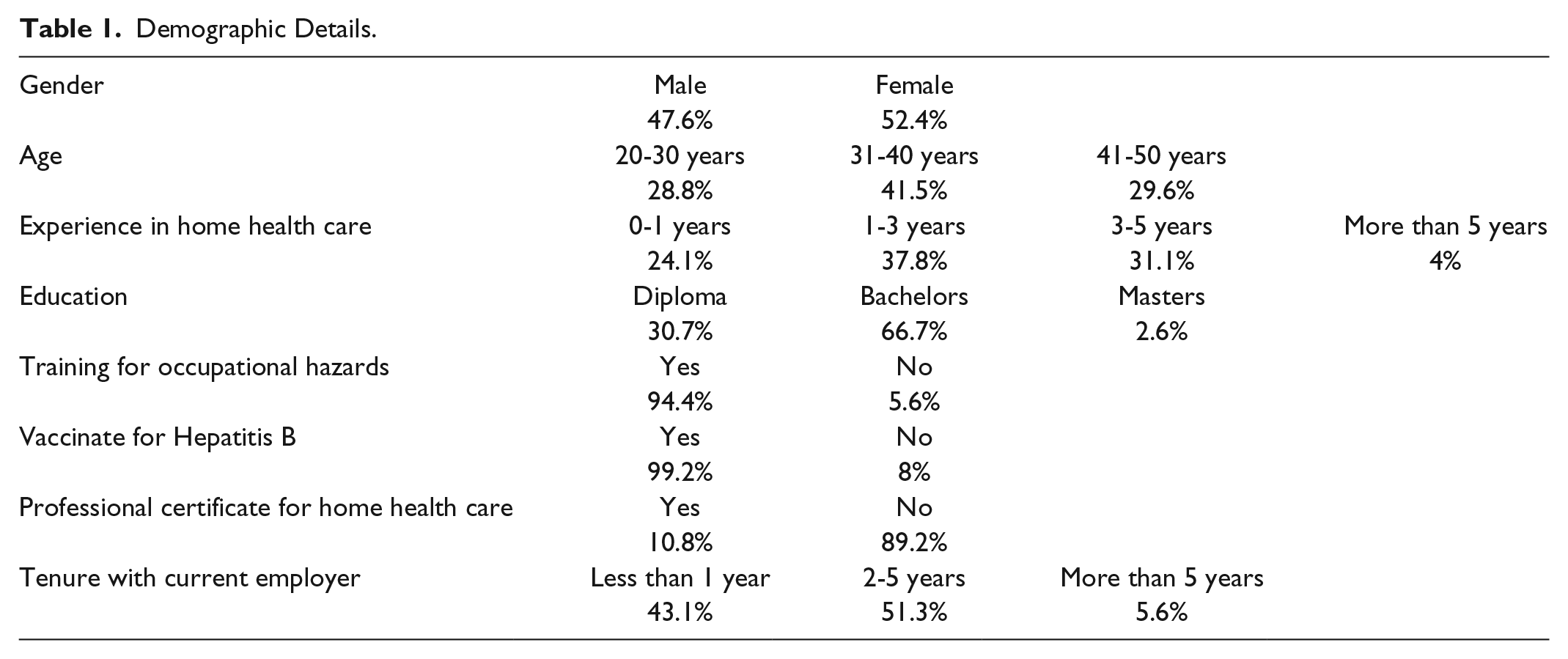
The descriptive analysis of all the respondents revealed that, on an average, each home health nurse has visited 2.7 patients per week, similarly the average hours worked per week came to 29.20 hours. The demographic analysis revealed that 47.6% of the respondents were male and 52.4 respondents were female. From which, majority of the respondents (i.e., 41.5%) were in the age bracket 31 to 40 years. Moreover, the highest percentage for experience in the home health industry was 37.8% for the experience bracket 1 to 3 years, followed by 34% in the experience bracket 3 to 5 years. Most of the home health nurses had done bachelors in nursing, that is, 66.7%. Almost 95% of home health nurses have reported about receiving training for occupational hazards. Moreover, the compliance for Hepatitis B vaccination was very good among home health nurses of India, that is, 99.2%. In contrast to that, only 10.8% of nurses have done some certification courses for professional home health nursing. Majority of the nurses were having the work tenure with the current employer in the range of 2 to 5 years with 51.3% followed by the year range of 0 to 1 year with 43.1% (see Table 1).
Demographic Details.
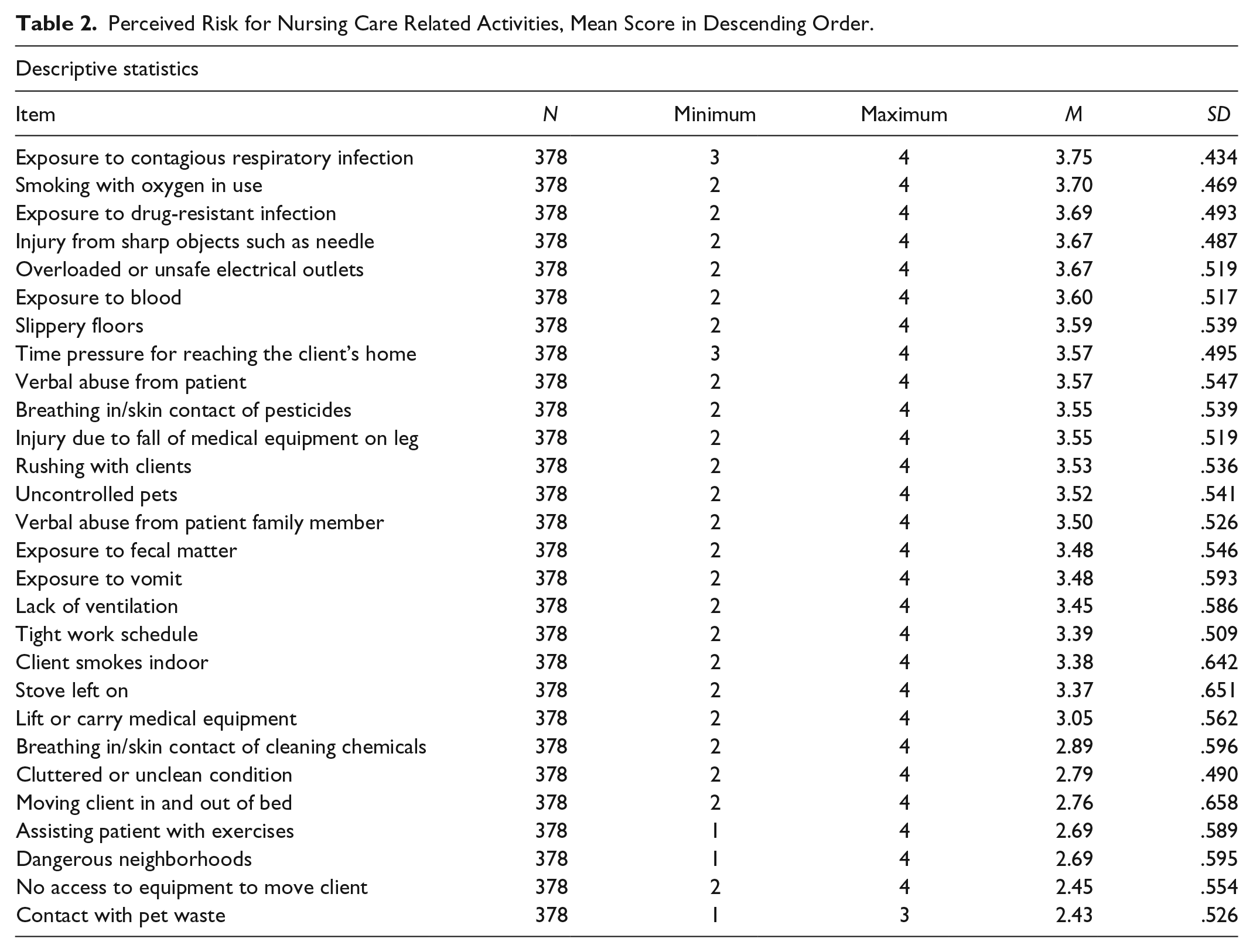
The analysis of perceived risk items revealed that out of 28 hazards associated activities, 14 activities (exposure to contagious respiratory infection, smoking with oxygen in use, exposure to drug-resistant infection, injury from sharp objects such as needle, overloaded or unsafe electrical outlets, exposure to blood, slippery floors, time pressure for reaching the client’s home, verbal abuse from patient, breathing in/skin contact of pesticides, injury due to fall of medical equipment on leg, rushing with clients, uncontrolled pets, verbal abuse from patient family member) were perceived high-risk activities with a mean score of 3.5 and above out of 4, a cutoff decided before getting results (see Table 2).
Perceived Risk for Nursing Care Related Activities, Mean Score in Descending Order.
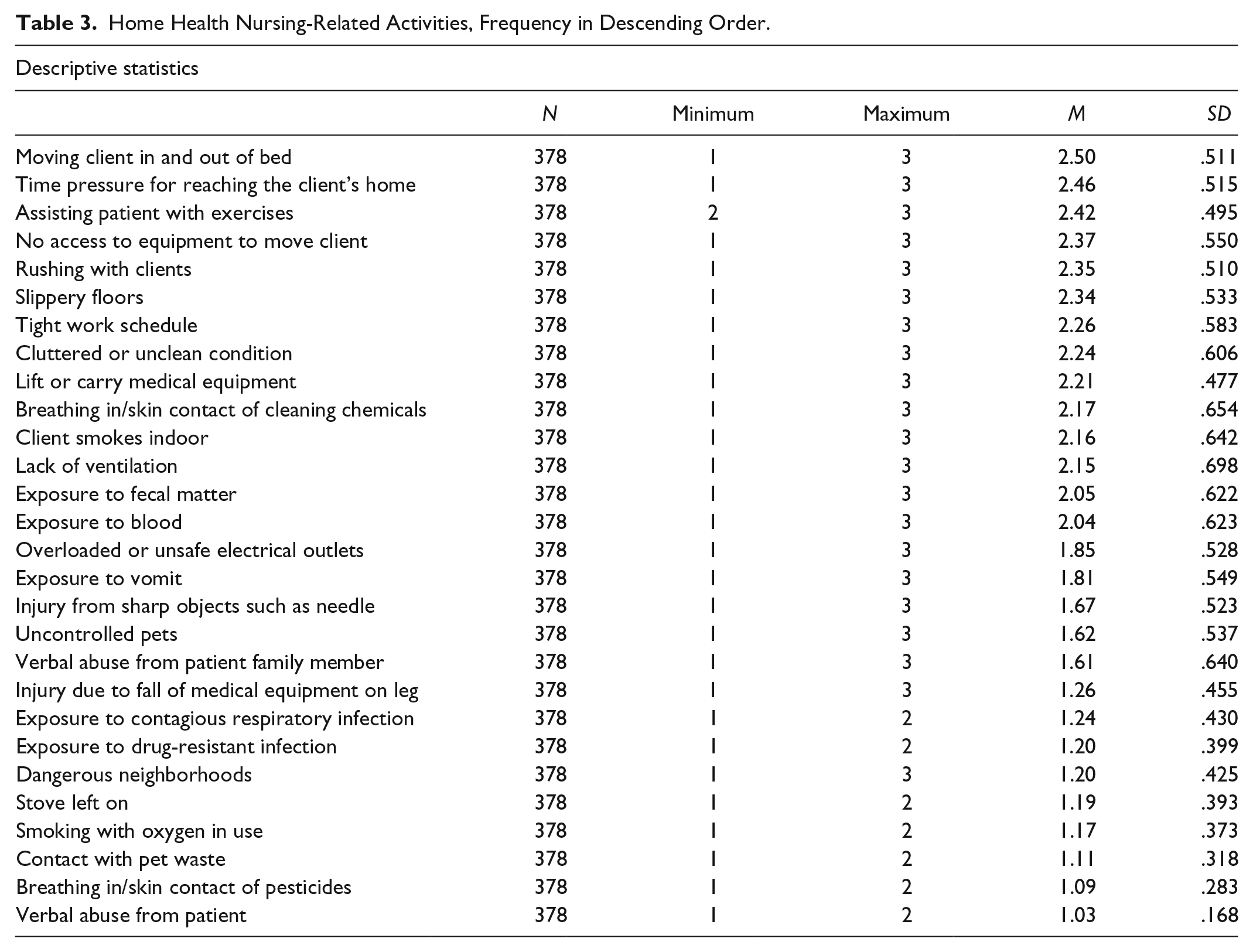
Similarly, the analysis of the nursing activities based on the frequency of times the nurses have to carry out that activity revealed that moving client in and out of the bed is the most frequent activity followed by other 13 activities (time pressure for reaching the client’s home, assisting patients with exercises, no access to equipment to move client, rushing with clients, slippery floors, tight work schedule, cluttered or unclean condition, lift or carry medical equipment, breathing in of cleaning chemicals, client smokes indoors, lack of ventilation, exposure to fecal matter, exposure to blood). In India, the metropolitan cities have high population density and the cities are also expanding due to migration of people from rural to urban areas, resulting into congestion in the city thus making time pressure to reach client’s home and lack of ventilation a common phenomenon, In this case, the cutoff score for deciding the highly frequent activities was 2, again decided before getting results (see Table 3).
Home Health Nursing-Related Activities, Frequency in Descending Order.
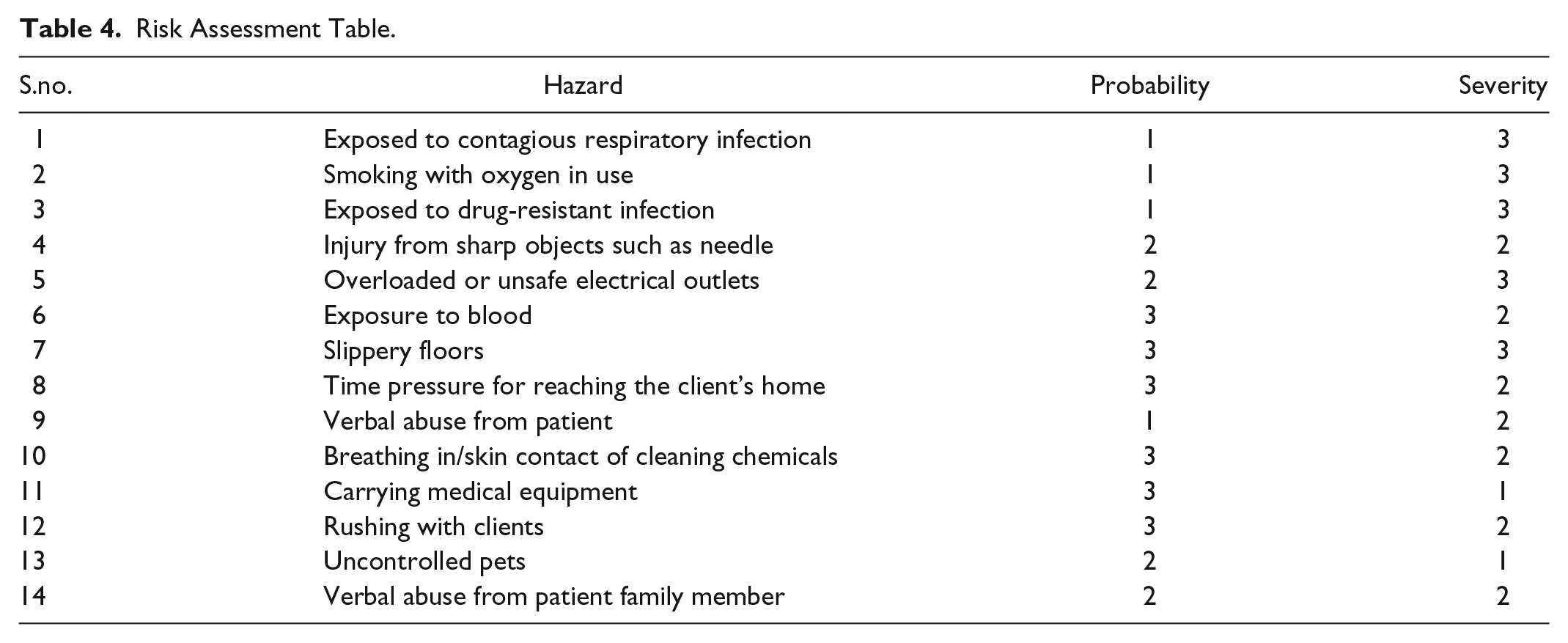
Finally, risk matrix is prepared for the identified 14 home health nursing-related activities based on the perceived risk level and the frequency with which they were carried out, to do that a risk assessment Table 4 (Risk Assessment Table) is prepared in which the probability scores were assigned based on Table 3 (home health nursing-related activities, frequency in descending order) mean score items, the scores were re-coded by using the scoring system 0 to 1.5 = low (1), 1.5 to 2 = medium (2), and more than 2 = high (3), similarly the severity scores were assigned after the brainstorming session with 25 senior home health nursing care experts (see Table 4).
Risk Assessment Table.
A risk matrix is prepared from the risk assessment table with the help of MS Excel 2016, and the results are shown in Figure 1; in this matrix, a color gradient system is used where red color denotes high risk with high priority area, yellow color denotes medium priority area, and green color denotes low priority area.
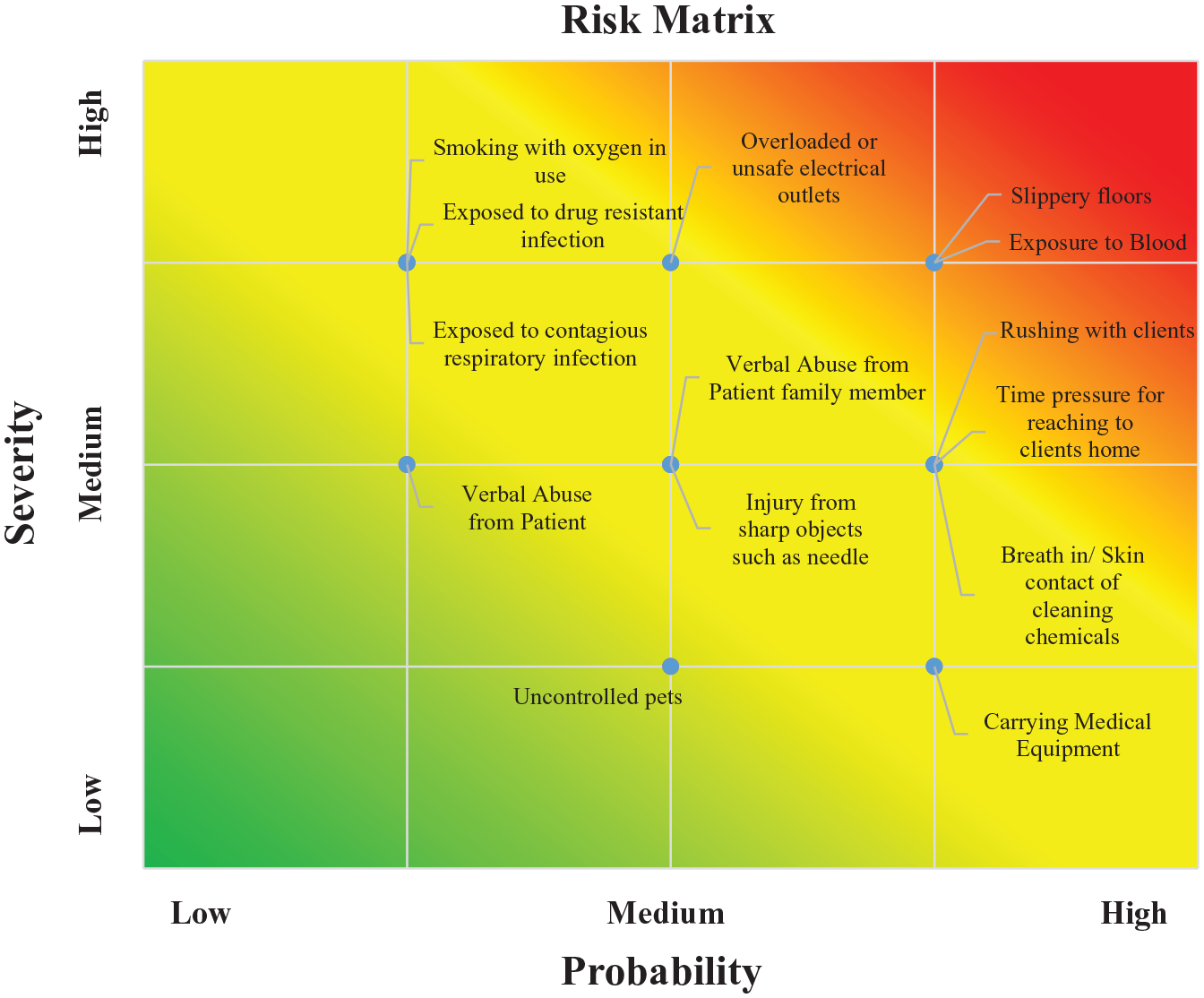
Risk matrix.
From the Figure 1, it can be seen that hazards such as slippery floors, overloaded and unsafe electrical outlets, rushing with clients, time pressure for reaching the client’s home, exposure to blood, and contact with chemicals had high-medium severity rating with high-medium probability levels.
Discussion
In this study, it is found that the gender composition in the home health nurse’s workforce is nearly equal, which is different from countries such as Canada and the United States, where female nursing staff composition was on the higher side.5,14 The majority of respondents belonged to the age bracket of 30 to 41 years. Moreover, the Indian home health nurses on average were attending 2.7 patients per week, which is on the lower side in comparison to the study done in Canada, where home health nurses attended an average of four patients per day. In addition, in this study, the most frequently reported task by home health nurses was moving client in and out of bed which is not the case in a study done in United States, 5 where the most frequent task was walking to and from the patient’s house and the task of moving a patient in and out of bed fell into the sixth rank. Similarly, the home health nurses perceived risk was highest for the hazard exposure to contagious respiratory infection, which was not the case in the study mentioned earlier in which again the hazard of exposure to blood had the highest mean score (3.10) and the hazard exposed to contagious respiratory infection was at eighth rank with mean score (1.80). However, the findings of risk matrix commensurate with previous research study 13 found that 39% hospital nurses have reported that they perceive slippery floors as high-risk factor, which is also one of the significant findings of this study; however, there is a difference of work environment, as the risk matrix prepared in this study is based on Indian home health nurses reported responses and it shows slippery floors at patients’ house in high priority area as it has high severity level and high probability of occurrence based on the experience of the home health nurses; moreover, in a previous study, the home health nurses have reported that bathrooms are one of the main safety areas and many home health nurses have got injuries there. 14 Similarly, exposure to blood is a serious concern for all the health care workers including home health nurses as there are many factors at a client’s home which diverts the attention and affects the concentration leading to such events. In the risk matrix developed in this study, the hazard exposure to blood also fell into high priority category with high severity and high occurrence ratings. Apart from that hazards such as overloaded and unsafe electrical outlets, rushing with clients, time pressure for reaching the patient’s house, breathing in/skin contact with chemicals, verbal abuse from patients, and injury from sharp objects fell into medium priority category.
Implications
This study identifies the relevant hazards associated with the home health nursing profession in the Indian setting and prioritizes the hazards based on the home health nurse’s perceived risk associated with the hazards and the experienced frequency. In addition to that, a risk matrix for hazards with high perceived risk is prepared to classify them based on the severity and probability ratings into three categories high priority, medium priority, and low priority. This study proposes that Indian home health providers should make adequate provision at the earliest for hazards with high and medium priority levels mentioned in this study to ensure the occupational safety of home health nurses in India.
Conclusion
This study finds that in India currently the client base for home health care is small but increasing, as the number of clients attended by home health nurses is very less in comparison to developed countries. Moreover, in the last 45 years, the nursing staff working in the home health segment in India has increased, as more than 90% of nurses were having experience in the range of 1 to 5 years. If this trend persists more and more, nurses will join the home health organization in the coming times. Home health care in India is although a new vertical but the workforce in this segment is increasing, however, the safety of the staff is the responsibility of the organization. The risk factors vary from place to place and there is not much research done to identify the risk factors associated with home health nursing profession in India in relation to the patient’s home as work environment. This study is first of its kind in India which has attempted to identify the perceived high-risk hazards and classified them into different risk categories with priority levels attached, this study proposes that home health providers should take measures for hazards such as slippery floors, overloaded and unsafe electrical outlets, rushing with clients, time pressure for reaching the client’s home, exposure to blood, and contact with chemicals as these hazards fell into high-medium severity rating with high-medium probability levels. The findings of this study can be used by the management of home health providers as a starting step to develop the policies and safety programs for home health nurses in India.
Application to Practice
The findings of this study will assist the management of the home health providers in India, in identifying the focus areas, that is, the priority-related hazards, and to develop the appropriate safety and training programs considering specifically the high and medium priority related, by doing that they can expect the occupation-related injury levels to go down and the nursing staff satisfaction with the organization to go up.
Footnotes
Author’s Note
Ankit Singh is now affiliated with Symbiosis Institute of Health Sciences, Symbiosis International (Deemed University) Pune, India.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.