
Abstract
There is a gap in the evidence on telerehabilitation (TR) for people with fragility fractures. It is unclear whether this group with recent falls who are often frail with cognitive changes will accept tele-rehabilitation and functional gains can be achieved using this approach. Prospective observational study of consecutive patients admitted with femoral or pelvic fracture to a hospital-based home rehabilitation service (HRS) between January and November 2017. Using tablets, multidisciplinary rehabilitation was provided via videoconferencing and use of exercise apps. Patients chose a face-to-face visit or TR. Information on demographic characteristics, functional levels, the total number of therapy sessions, TR episodes, reasons for non-acceptance of TR, and patient-reported experience using TR was collected. Fifty-two patients with hip and pelvic fractures were admitted to the HRS and 35 (67.3%) received TR. Patients who did not accept TR were older, frailer and more likely to be female than those who received TR. Of the 17 who did not receive TR, 6 were deemed unsuitable by staff due to hearing, vision or cognitive problems and 3 refused. The TR group achieved acceptable functional gains. In the TR group on average, participants had 13.63 (± 7.29) home visits however they only elected to have 3.43 (± 2.48) sessions delivered via TR. TR was acceptable to a subset of hip fracture patients but face-to-face was the preferred mode of delivery. More research is needed to understand patients’ preferences and beliefs, and the influence of clinician attitudes on uptake of TR.
Keywords
Introduction
The incidence of hip and pelvic fracture is increasing as the population ages1,2 and up to 40% of older adults who suffer hip fractures have some degree of cognitive impairment. 3 Older people with hip and pelvic fractures struggle to recover their premorbid level of function and are then more at risk of falls. 4 Frailty contributes to a decrease in physiological reserves leading to a poor recovery from illness and an increased reliance on external supports.5,6 Following fractures, rehabilitation assists with recovery 7 but there is rationed access particularly for those with cognitive impairment. The current rehabilitation model for people with fragility fractures, characterized by expensive specialized expert-driven face-to-face care delivery, looks unlikely to accommodate the growing demand.
Tele-rehabilitation (TR) refers to the provision of rehabilitation services at a distance using technologies such as videoconferencing, remote monitoring, wearable technologies and the use of therapeutic apps and has been suggested as a method of service delivery that may maximize access to rehabilitation and manage demand.8,9 The evidence on the effectiveness of TR for frail aged adults remains limited and nuanced.
It is often assumed by clinicians that older people will not or cannot engage with the technology. 10 Older people are generally less familiar with technology and have different cognitive and physical abilities.11,12 They may have more difficulty processing complex information and learning new skills, and training and support needs may differ from those of younger patients. Although older people may be willing to give new technologies a try, they remain reluctant if they cannot clearly see that the technology will achieve a purpose which is meaningful to them, for example assisting them with everyday life tasks. 13 Similarly, they decline to use technology if the relative advantage, that is, the time and effort required to use the item versus the benefits obtained is not clearly demonstrated. 14 When considering the uptake of technology by older patients, the literature suggests that value (usefulness) and usability (ease of use) act as determinants for the adoption of technology, but other factors including technical support, social support, confidence, age, gender, and experience are also considered as important factors. 13
Technology anxiety or low self-efficacy can be a barrier to the initial uptake of technology. 12 Patients with higher self-efficacy will engage more frequently in technology related activities. Hence, older patients with lower self-efficacy need sufficient technological support and coaching to alleviate their anxiety.15-17 Social influence, particularly from peers and a patient’s professional team, may also influence the uptake of technology by the patient.15,18 Therefore, for patients to benefit from the increased access to rehabilitation afforded by TR, clinician acceptance and uptake of technology are of paramount importance.
Prior work in TR and the elderly has demonstrated that delivering TR for general rehabilitation post hospital admission 19 is feasible and that older people accepted and enjoyed the technology. 20 There is limited evidence, however, for the use of TR in frail elderly, such as those with mild dementia and there is a gap in the TR evidence regarding its usefulness for people with fragility fractures. No studies have evaluated the acceptability of TR in the immediate post discharge phase following hip or pelvic fracture where dependency needs are high.
The aim of this study was to evaluate the provision of TR to older people with recent hip or pelvic fractures as they are discharged from hospital and enter a home rehabilitation service. Study objectives were to determine the demographic characteristics and functional levels of patients who received TR compared to those who did not, and to explore the reasons why TR was declined or not offered to some patients.
Materials and Methods
This prospective observational study was conducted at a Home Rehabilitation Service (HRS) of a metropolitan hospital in South Australia, including all patients sequentially admitted to the service following femoral or pelvic fracture between January and November 2017. HRS is a home-based multidisciplinary rehabilitation service, which enables early discharge from hospital and provides an alternative to inpatient rehabilitation. The service provides daily nursing, allied health, personal care assistance and short-term equipment loan. Patients receive an environmental assessment and falls prevention advice, nursing for wound care and/or medication management, and physical therapies including lower limb strengthening, balance, and mobility progression. Multidisciplinary rehabilitation and care is provided as required, based on the assessment and clinical reasoning of the clinicians. Rehabilitation goals and plans for discharge are discussed in weekly case conferences.
TR is offered to all patients considered suitable and admitted to HRS, excluding those residing in residential aged care facilities. Suitability for TR is decided at the discretion of the treating clinicians based on cognitive, hearing, visual, or language capabilities. The rehabilitation elements of the TR rehabilitation package are the same as provided in usual face-to-face rehabilitation. All participation is voluntary and patients can choose which elements of TR they utilize. Together, clinicians and patients decide when and how frequently TR interventions are provided based on rehabilitation goals and progress. At all times, patients are given the option of a home visit rather than a virtual visit.
Patients receiving TR are loaned a 4G enabled tablet on an adjustable stand. The tablet is configured with commercially available apps and a videoconferencing platform that can be used to provide all or some of the rehabilitation interventions. The exercise app allows the remote prescription of standard exercises accompanied by a demonstration video and the ability for clinicians to track adherence. Clinicians introduce the tablet during their first visit to the patient and provide basic training to the patient and their carer. A simple instruction booklet acts as a reminder for tasks such as turning the tablet on and off, opening apps and how to participate in a video call. Clinicians, supported by an IT professional, then use clinic-based VC equipment including desk top and wall mounted screens, cameras, microphones, and headsets. Remote access to tablet-based apps via a mobile device manager is available.
All study data obtained for analysis consisted of information routinely collected as part of HRS usual practice, including demographic information, measures of functional level, cognition and frailty.
Baseline measures at admission included the Clinical Frailty Scale, 5 the Mini-mental State Examination (MMSE) 21 and the Short form Mini Nutritional Assessment (MNA-SF). 22
Both at admission and discharge scores from the Functional Independence Measure (FIM), 23 the De Morton’s Mobility Index (DEMMI), 24 and the Timed Up and Go (TUG) 25 were collected. The FIM scores 18 functional items using a 7 level scale with a maximum score of 126. A lower score indicates a lower functional level.
Finally, at discharge, length of stay (LOS) in HRS, the number of face-to-face home visits and number of virtual therapy sessions were collected. In addition, patients who received TR reported on their impressions of the technology using the System Usability Scale (SUS). 26 The SUS is a 10 item, 5 point Likert scale measuring aspects of technology functionality such as ease of use and the need for technical support.
Statistical analysis was conducted using IBM SPSS statistics software. For all data, normality of distribution was confirmed by analysis of Z-scores for skewness and kurtosis. Gender distribution between groups was assessed using chi-squared tests. Independent sample t-Tests were used to investigate differences in group baseline characteristics. For all statistical analyses alpha was set at 0.05
The study was approved by the Southern Adelaide Clinical Human Research Ethics Committee.
Results
Between January and November 2017, 52 patients with femoral or pelvic fracture were admitted to HRS. Of those, 35 (67%) patients were considered suitable for TR and agreed to receive their rehabilitation services by using TR (TR group). The remainder 17 (33%) HRS patients did not receive TR (nTR group). Of those in the nTR group, 6 patients lived in residential care, 2 were readmitted within 48 hours, and 6 were considered by the therapists as unsuitable for TR due to hearing, vision or language deficits. An additional 3 people refused TR. Reasons for refusal were a dislike of new technology, a preference for face-to-face home visits only and feeling overwhelmed on discharge from hospital.
The demographic characteristics and clinical presentation on admission of patients in the TR and nTR groups are presented in Table 1. Patients in the nTR group, with a mean age of 81.35 years (±11.46 years), were older (p = .014), frailer (p = .003), and had a significantly lower functional level (p = .012), as per the FIM, than the TR group. They were also more likely to be female (p = .016). There were no significant differences between groups in cognition nor nutritional status. In the TR group, 3 patients (8.6%) had a MMSE score between 13 and 20 indicating moderate cognitive impairment and 3 patients (17.6%) in the nTR had a mild cognitive impairment.
Characteristics and Functional Scores on Admission for TR and nTR Groups.
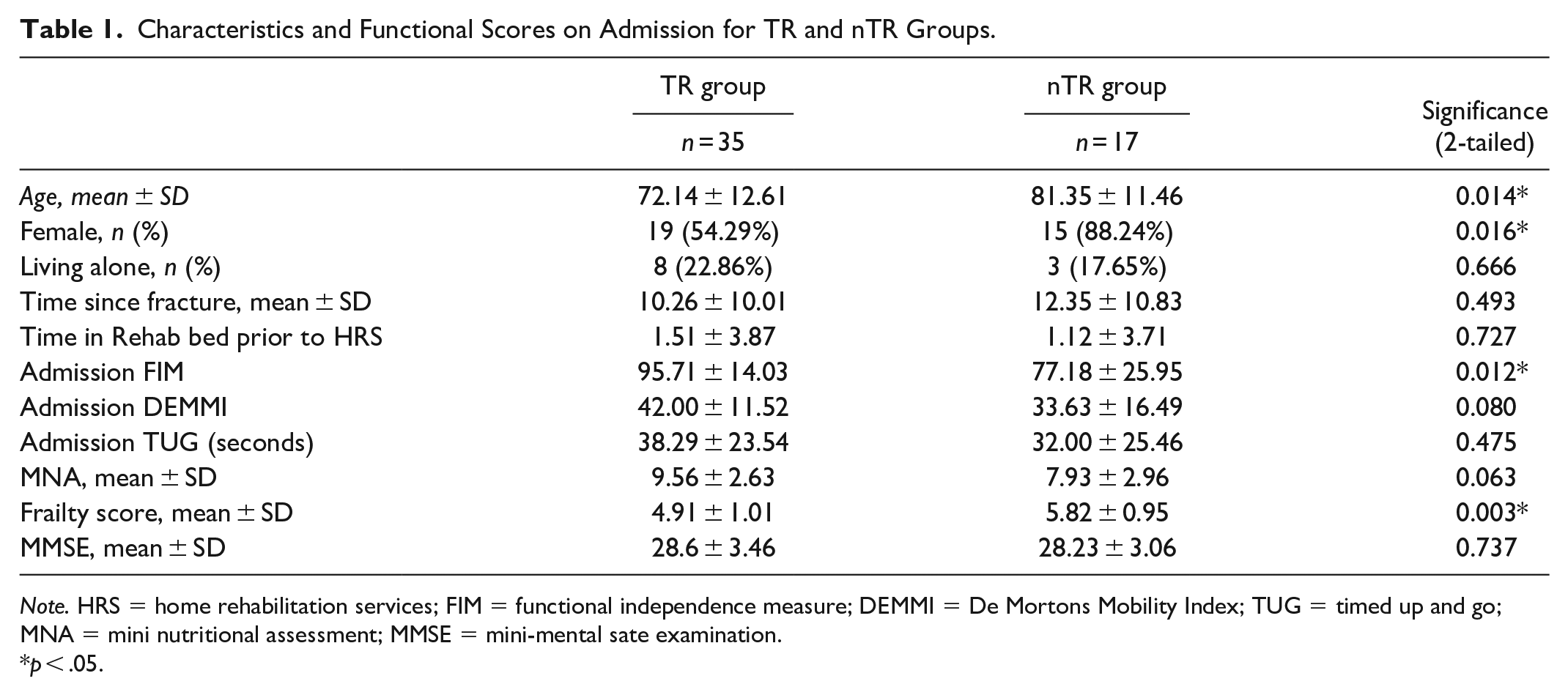
Note. HRS = home rehabilitation services; FIM = functional independence measure; DEMMI = De Mortons Mobility Index; TUG = timed up and go; MNA = mini nutritional assessment; MMSE = mini-mental sate examination.
p < .05.
Outcome measures on discharge for the TR group are presented in Table 2. Amongst those who agreed to TR there was a clear preference for face-to-face therapy. On average they had 13.63 (± 7.29) visits with only 3.43 (± 2.48) delivered via TR.
Outcome Measures on Discharge for TR Group.
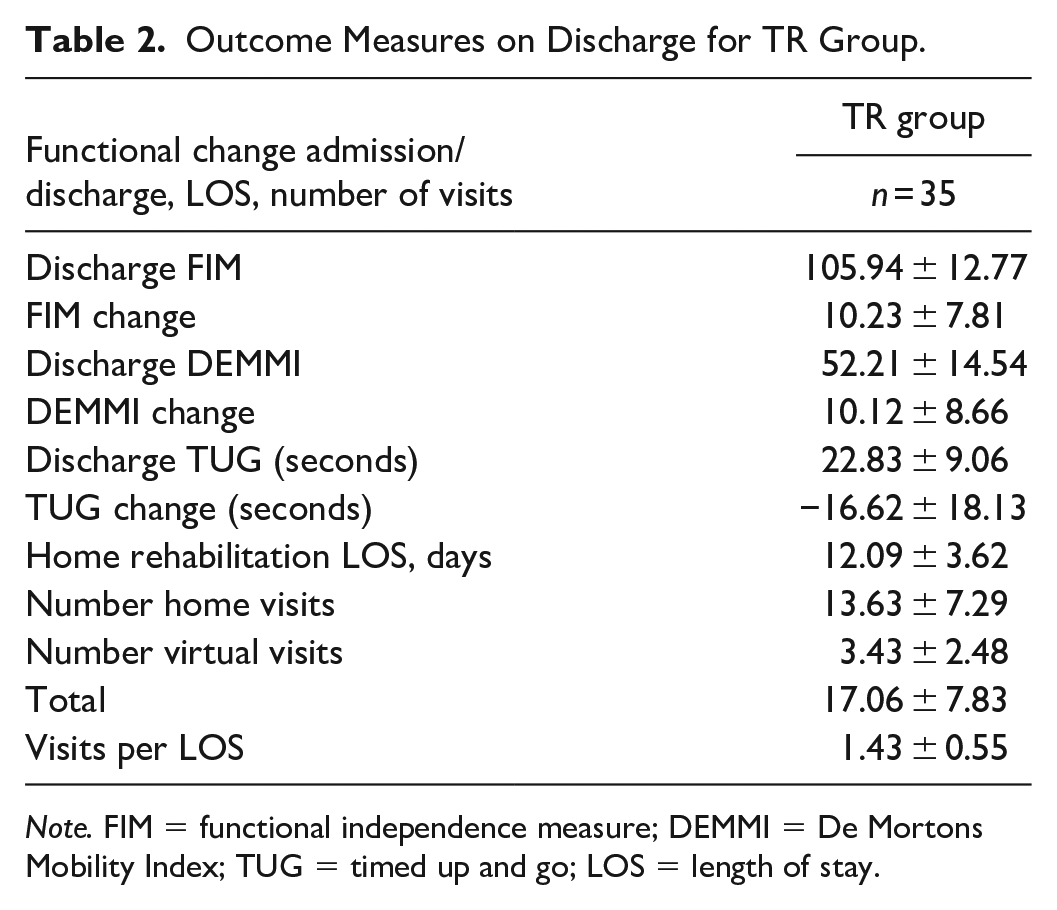
Note. FIM = functional independence measure; DEMMI = De Mortons Mobility Index; TUG = timed up and go; LOS = length of stay.
The TR group achieved a 43% change in TUG scores (−16.62 ± 18.13 seconds) exceeding the MCID change of 31% 27 and achieved an average 10 point increase on the DEMMI (10.12 ± 8.66), which is greater than the MCID of 6 points, representing a clinically important change in mobility. 24
TR substituted an average of 3 home visits for virtual visits. The average length of stay for TR patients in this study was 12.09 ± 3.62 days.
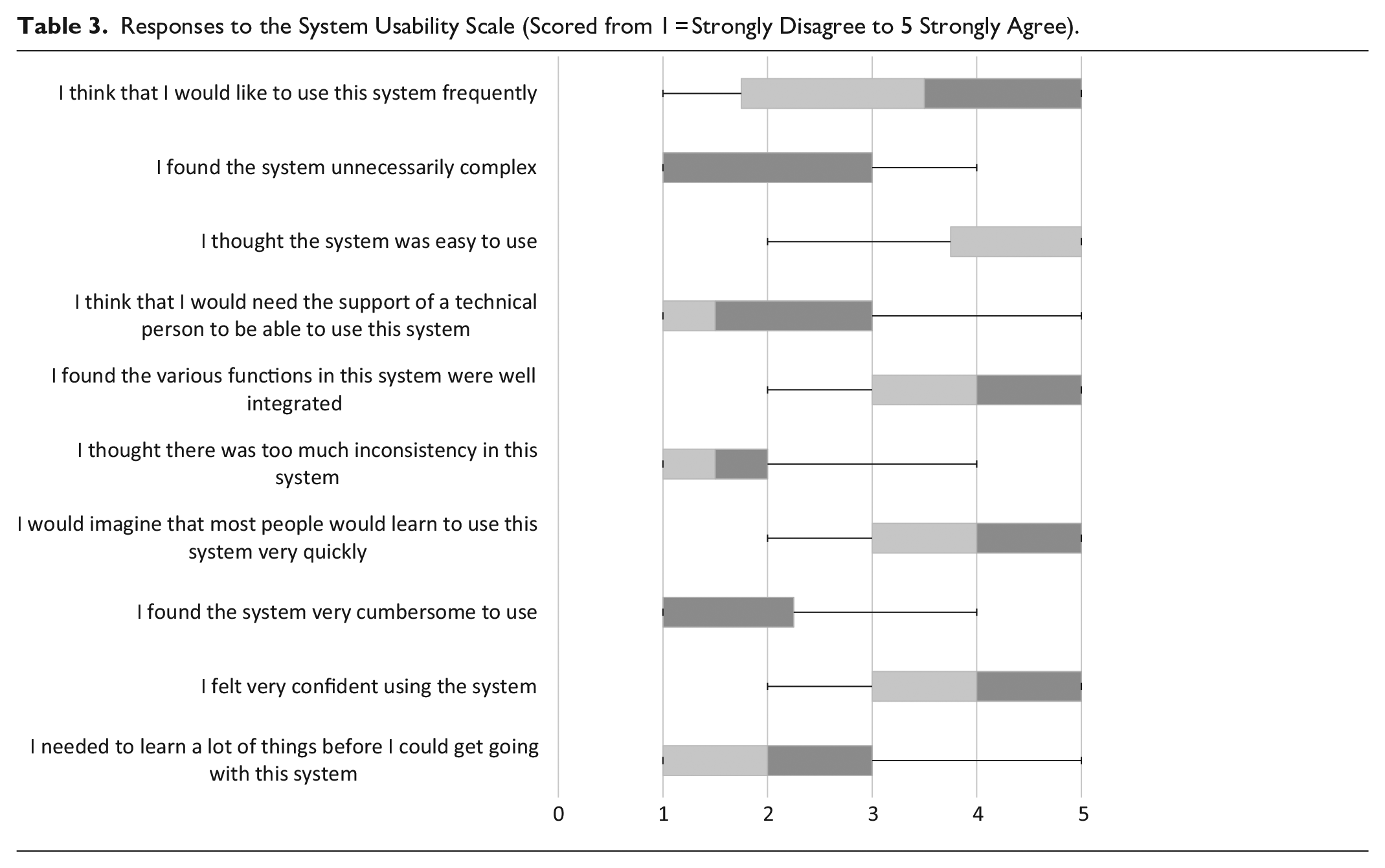
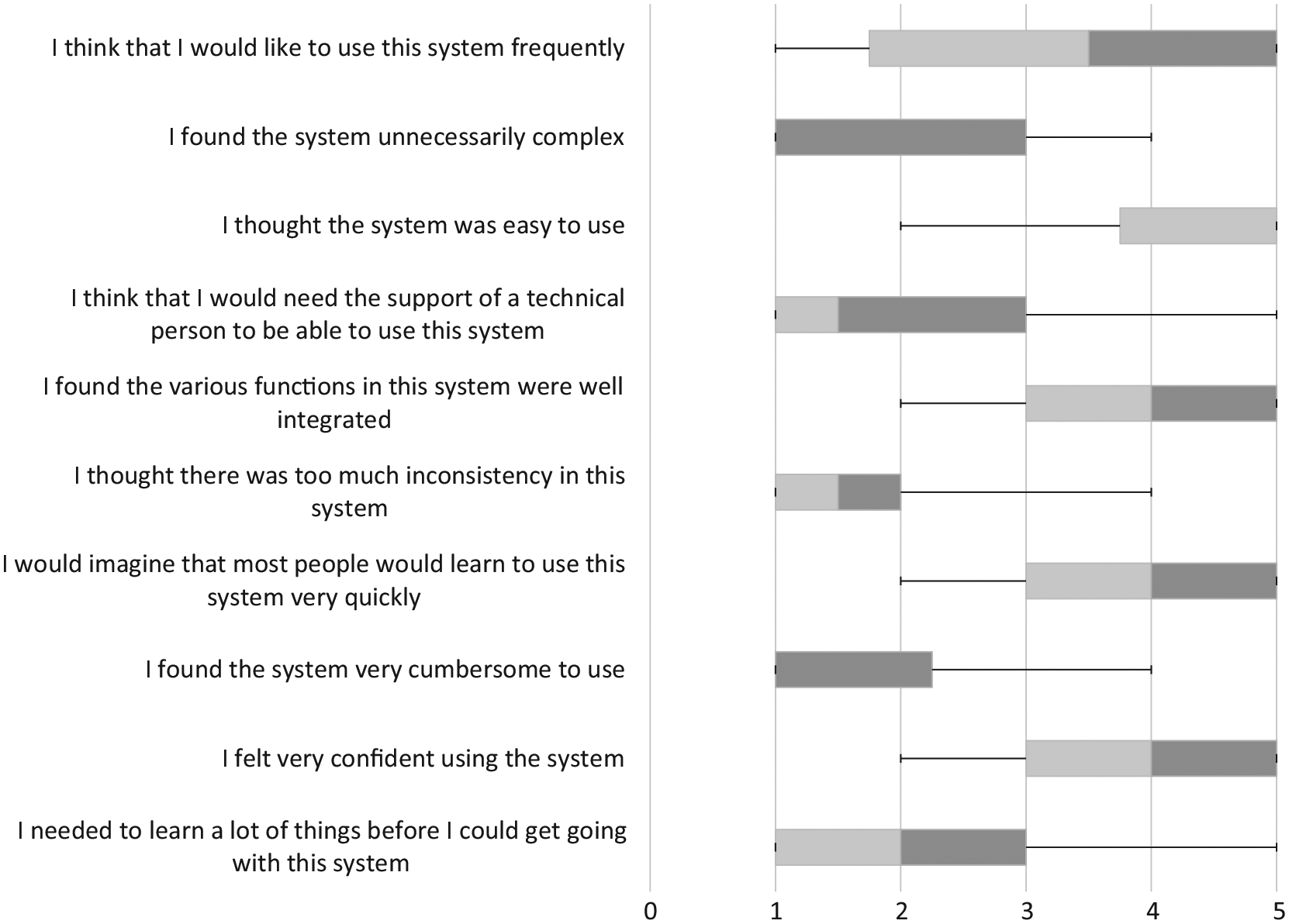
Twenty-two patients in the TR group (63%) completed the SUS questionnaire at discharge from HRS (Table 3). The mean score was 75.23 ± 19.44 with 13 (59%) of the respondents scoring >68, considered to be indicative of above average usability of a system. 26 Scores obtained indicated that patients were comfortable with the technology, did not find it complex, and agreed that users would be able to learn to use the equipment fairly quickly.
Responses to the System Usability Scale (Scored from 1 = Strongly Disagree to 5 Strongly Agree).
Discussion
This study aimed to evaluate the provision of TR to older people in a home rehabilitation service with recent femoral or pelvic fractures and to determine the characteristics of patients who received TR compared to those who did not. Results showed that patients who received home rehabilitation services through TR were younger, less frail and more likely to be male, when compared to those who did not receive TR. Usability of TR scored highly but only a small proportion of the service delivery was via TR with face-to-face visits remaining the preferred method of delivery. However, replacing face-to-face sessions did not have a detrimental effect on results and patients were able to achieve clinically important improvements in outcomes.
Six patients (11.54%) were not offered TR by the clinicians on the basis of sensory or cognitive problems. However, 3 patients who received TR had MMSEs below 24 suggesting that cognitive impairment is not necessarily a barrier to participation in TR programs. Some assumptions regarding the acceptability or suitability of patients for TR may have been made due to clinician attitude and/or bias. 28 Similarly, TR may not have been “promoted” or encouraged by some clinicians based on those assumptions. As clinician acceptance and uptake is deemed vital in the uptake of technology by patients, lack of professional endorsement may also have been a factor in the low frequency of TR provision.
Only 3 patients (5.8%) declined the offer of the TR service choosing the traditional home visits instead and positive responses to the System Usability Scale indicate that TR patients were comfortable using the system. However, the uptake of TR was low in those patients who initially agreed to receive it. All patients in this study were given the option of a home visit rather than TR at any time during their home rehabilitation program, and they or their carers elected to receive the majority of their sessions face-to-face. Our results indicate that TR is more acceptable as an adjunct to conventional face-to-face therapy sessions.
The low uptake of TR is consistent with other studies involving older people. An evaluation of TR provided to older people post hospitalization19,20 demonstrated that the delivery of TR to older people was feasible and acceptable. However, although patients found TR convenient and motivating, they preferred face-to-face contact and the physical presence of the therapist. 20
Low uptake may reflect reduced experience with technology, lack of perceived usefulness, or lower self-efficacy 12 which may also have an impact of functional outcomes. 29 The technology used in our study was affordable (provided at no cost to the patient) and simple (a simple interface with no log in and passwords and minimal choices to make) and those patients who “choose” TR may also be more confident in participating in the rehabilitation program in general.
With the growing number of fragility fractures, greater pressures on acute hospital services and a stronger emphasis on early supported discharge, it is likely that more use of novel approaches to rehabilitation will be needed. Whilst the number of TR virtual visits per patient was modest, this still represents a saving for the service in staff time spent driving and allows more people to be treated.
Fragility fractures such as hip fractures have a significant impact on quality of life in the medium to longer term, and structured exercise programs that continue for at least 12 weeks can make improvements in overall mobility and quality of life. 30 Of note, the average length of stay for participants in this study was 12.09 ± 3.62 days. Access to cheap affordable technologies could allow patients to continue with their rehabilitation via use of exercise apps and access to remote clinical advice well beyond the time-frame of traditional service provision.
A number of limitations were associated with the design of this study. This was a small sample in a pragmatic evaluation of actual TR implementation in an existing HRS. The results may not be generalizable to other services with different videoconferencing platforms, organizational support and staffing levels. However, the study does provide insights into areas requiring further investigation for the implementation of this technology for fragility fracture patients in health services.
Conclusion
The delivery of TR embedded in a home rehabilitation model to patients with hip and pelvic fractures appears acceptable to a small sub-group of patients. Acceptable functional gains were made by those who received TR rather than face-to-face for a portion of their home rehabilitation program. Our results suggest that older patients with hip and pelvic fractures who do agree to have TR as alternative to conventional home rehabilitation, will opt for face-to-face sessions, if given a choice. TR may prove to be a useful method to increase access to rehabilitation for people with fragility fractures and allow patients to receive cost effective programs for longer. Further research into the barriers to uptake of TR by older patients and clinicians is warranted.
Footnotes
Acknowledgements
We thank the SA Health patients and rehabilitation clinicians.
Author Contributions
CM initiated the study. All authors contributed substantially to the design and planning of the study. CM, MvdB and CB contibuted to the subsequent analysis and interpretation of the data. CM drafted the first version of the paper, and CB, MC, SG and MvdB critically revised it. After revision, the final version of the paper was approved by all authors for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.