
Abstract
Assessment of caregiver knowledge is an essential part of home healthcare education for pediatric tracheostomy care, however, there is a paucity of evidence in long term. This study aims to determine how caregiver knowledge and misconceptions, as assessed by our knowledge test, changed over a 12-month period following our educational program and whether the test score was associated with any demographics of the caregivers and children with tracheostomy. A prospective cohort study was undertaken to evaluate the knowledge at 3 timepoints after tracheostomy education: baseline (T1), 6 months (T2), and 12 months (T3). Test scores were analyzed for trend and relationship with demographics. Items for which less than 80% caregivers gave correct responses at T1 were considered common misconceptions. Fifty-four caregivers were enrolled. Out of a maximum score of 25, the median (IQR) scores were 22 (21-23), 23 (22-24), and 23 (22-25), at T1, T2, and T3, respectively. The scores at T2 and T3 were significantly higher than at T1 (P ≤ .01). One common misconception “how to manage when suction got less secretion than expected” was found at all timepoints. Caregivers of children with >2 comorbidities scored slightly higher than those of children with 0 to 2 comorbidities (P = .01). In conclusion, our caregivers achieved high knowledge scores which increased over the 12-month study period potentially because of repeated assessment and practical experience. Common misconceptions and a factor associated with the knowledge were also identified. These advantages highlighted the importance of knowledge assessment for quality improvement.
Introduction
Tracheostomy is a life-saving procedure that assists in bypassing an upper airway obstruction, long-term use of mechanical ventilation and toileting airway secretion. Over recent decades, there have been increasing numbers of children with complex respiratory conditions requiring tracheostomy as part of the management.1-3 Unfortunately, 8% to 65% of patients with long-term presence of a tracheostomy tube experience at least 1 adverse event including tube obstruction, hemorrhage, airway granulation, and accidental decannulation.4-7 The common adverse events in children were similar to adults with roughly double the incidence of tube obstruction. 5 Therefore, ongoing follow up by a multidisciplinary team is required to ensure appropriate care and minimization of tracheostomy-related complications.8-10
The quality of long-term care, including home tracheostomy care, is shaped by multiple factors, including patient and caregiver characteristics, nature of care tasks, physical environment, medical technology, social, and community environment.11,12 Knowledge can impact the caregiver’s performance of tracheostomy care and should be assessed as a part of caregiver characteristics. Knowledge assessment not only confirms whether certain educational outcomes have been established but can also provide the educator with an opportunity to identify areas of concern in each individual and the educational program. 13
Although, there are several popular methods to assess knowledge, such as peer/self-assessment, direct observation, quiz, and examination, we found no published study indicating a recommended best method in health education. Moreover, there is limited evidence underlining the importance of knowledge assessment in home tracheostomy care. A wide inter-personal variability in tracheostomy care due to different care settings and personal backgrounds 14 possibly plays a part in the variation in assessment. Since there was no identified best tool to assess the knowledge, we developed our own test for the assessment of caregiver knowledge of pediatric home tracheostomy care. The test was also leveraged to determine caregivers’ common misconceptions and to guide feedback to the caregiver.
The primary aim of this study was to determine how caregiver knowledge and misconceptions, as assessed by the knowledge test, changed over a 12-month period following our pediatric home tracheostomy care educational program. The secondary aim is to determine whether the test score was associated with any demographics of the caregivers and children with tracheostomy. It is hoped that data derived from this study will highlight the importance of regular knowledge assessments for a better care and education.
Methods
Study Design
The Institutional Review Board of Faculty of Medicine, Chulalongkorn University, provided ethics approval for the study (approval no. 025/60). A prospective cohort study was undertaken at King Chulalongkorn Memorial Hospital from May 2017 to April 2018. Written informed consent was obtained from all caregivers and assent from all children aged >12 years.
Participants
All primary caregivers of children with tracheostomy who completed our home tracheostomy care educational program and whose children were followed up clinically at our center were eligible. The caregivers were enrolled in the educational program as soon as their children underwent tracheostomy. The educational program consisted of 6 hands-on sessions.
Equipment introduction: how to use and maintain tracheostomy tube and respiratory care devices, home environment preparation
Tracheostomy care simulation 1: stoma care, suction at pre-measured depth, nebulization therapy
Tracheostomy care simulation 2: how to change tracheostomy tube and tie, checking the correct placement of tracheostomy tube
Emergency management simulation: recognizing and responding to deterioration, basic life support for children with tracheostomy
Observation and practice tracheostomy tube change and tracheostomy care in patients under direct supervision
Chest physiotherapy: postural drainage, manual percussion and vibration, physiotherapy devices, specific respiratory exercises, cough technique
Each session was facilitated by the respiratory nurse and/or physiotherapist and took up to 2 or 3 hours. Additionally, we provided extra sessions including medication administration, gastrostomy tube care and home mechanical ventilation to some caregivers as per their child’s requirement. Following the hands-on sessions, coordinating nurses at pediatric wards would reinforce the care at bedside where the caregivers could practice caring their own children. Finally, independent 24-hour in-hospital practice was evaluated over 2 to 3 days and a debrief was provided for 1 last time before the children were discharged.
Exclusion criteria were caregivers who (1) did not give consent, (2) withdrew from caregiver role, or (3) were caregivers to children who were deceased, transferred to other centers or were undergoing elective tracheostomy decannulation.
Assessment of Knowledge
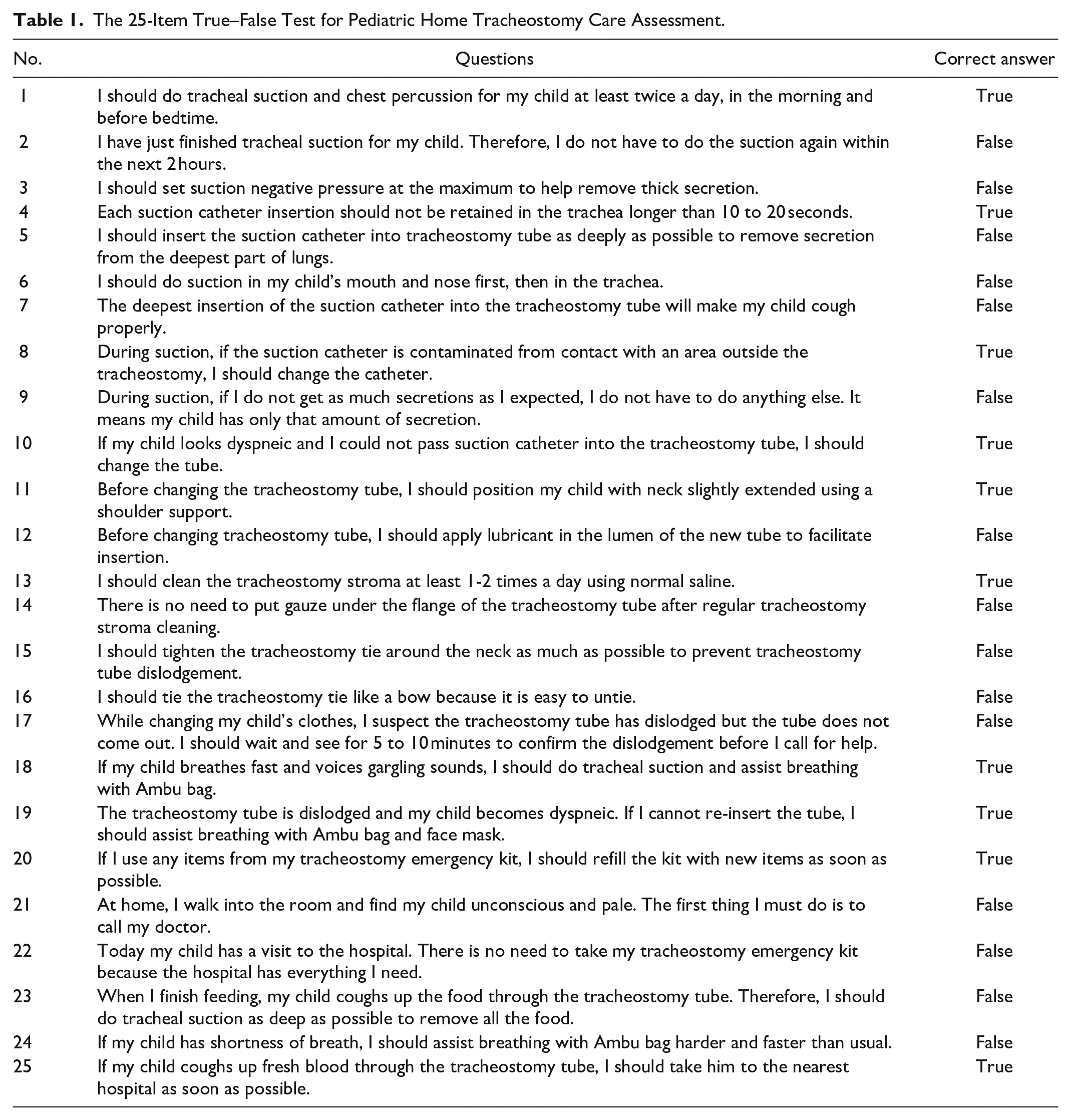
The 25-item true-false test of pediatric home tracheostomy care knowledge was used to assess knowledge of caregivers and is shown in Table 1. The test was devised based on academic principles and validated by all pediatric respiratory consultants to incorporate crucial knowledge in tracheostomy care including suction, tracheostomy tube change, tracheostomy stroma care, tie care, and emergency management. Each correct answer scores 1 point, so the range of the score is 0 to 25.
The 25-Item True–False Test for Pediatric Home Tracheostomy Care Assessment.
The assessment was undertaken either during outpatient visit or hospitalization after the caregiver had completed the 6-session educational program. All caregivers completed a hard copy version at baseline (T1) and then another 2 occasions 6 and 12 months later (T2 and T3). After each knowledge assessment, one of the investigators immediately checked to identify any incorrect answers, provided feedback and corrected the knowledge pitfalls by a brief review with the caregiver or hands-on simulation as needed.
To identify common misconceptions in pediatric home tracheostomy care, the percent of correct response to each item at each timepoint were examined. The items showing correct responses by less than 80% of the caregivers were considered as common misconceptions.
Statistical Analysis
Categorical data are presented as frequency and percentage and continuous data are presented as median with interquartile range given non-parametric distribution of the data. The scores between assessment occasions were compared using related-samples Wilcoxon signed-rank test. Demographics were examined for a relationship with the score at baseline (T1) using Spearman’s correlation, Mann-Whitney U test or Kruskal Wallis test, depending on data characteristics. SPSS Statistics for Windows version 25 (Armonk, NY: IBM Corp) was used for statistical analysis and P < .05 was considered significant for all analyses.
Results
There was a total of 63 eligible caregivers of children with tracheostomy at our center. However, 9 caregivers were excluded (2 whose children had recently died, 4 whose children were transferred to other centers, and 3 whose children were undergoing elective tracheostomy decannulation). Thus, 54 caregivers were enrolled in the study. Demographics of the caregivers and children with tracheostomy were shown in Table 2.
Demographics of the Caregivers and Children With Tracheostomy.
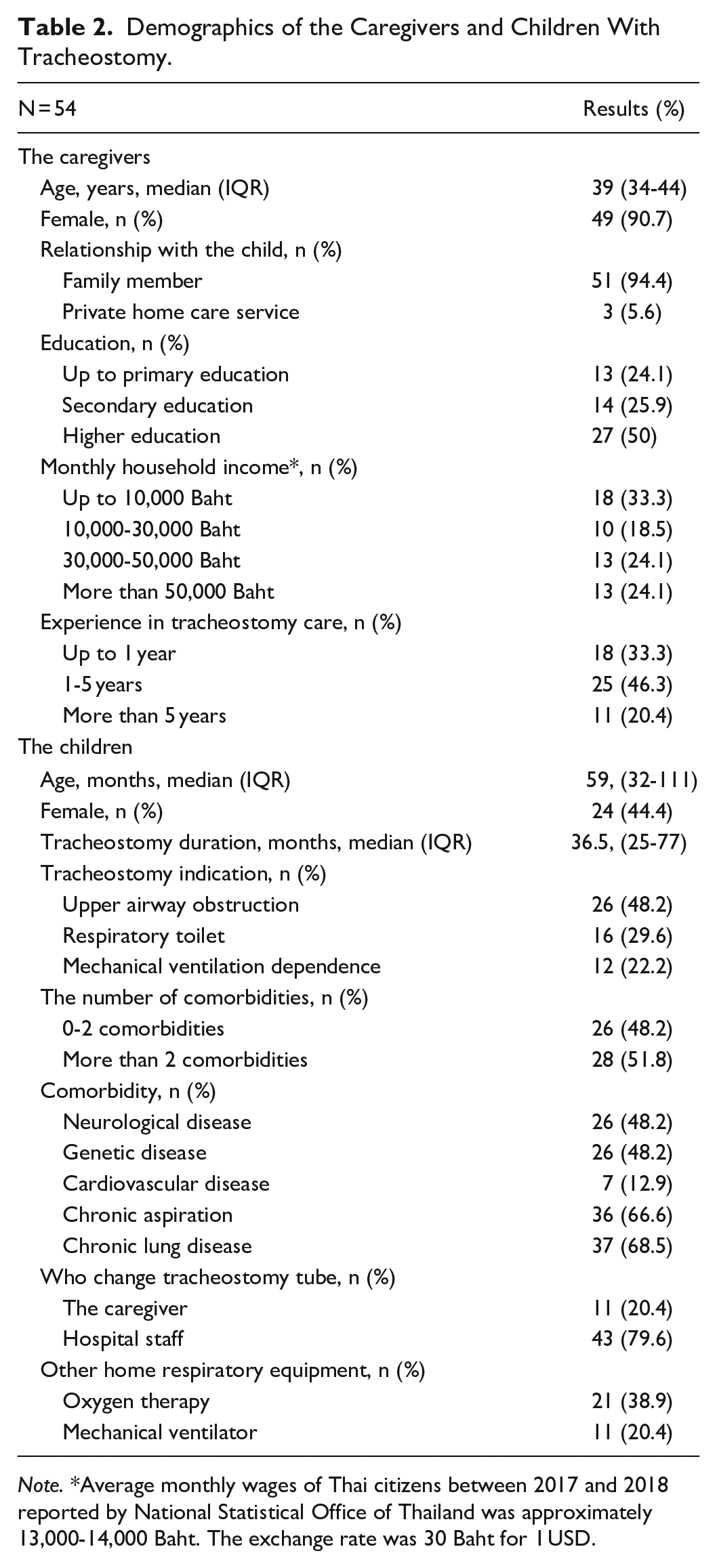
Note. *Average monthly wages of Thai citizens between 2017 and 2018 reported by National Statistical Office of Thailand was approximately 13,000-14,000 Baht. The exchange rate was 30 Baht for 1 USD.
At all 3 assessments, the median scores were higher than 80% of the maximum 25-point test score. Nine caregivers at T1, 2 caregivers at T2, and 1 caregiver at T3 scored less than 80% (ie, less than 20 points). The minimums were 18 points at T1 and T2 and 19 points at T3; and the maximums were 25 points. The median score (IQR) the caregivers achieved was 22 (21-23) at T1, 23 (22-24) at T2, and 23 (22-25) at T3. There was significant improvement of the median score from T1 to T2 and from T1 to T3 (both P ≤ .01), but no significant difference between T2 and T3.
At T1, less than 80% (ie, less than 43) of the caregivers correctly responded to item 4, 9, 10, 12, and 21. Overall, there were increasing numbers of correct answers to these items from T1 to T3. However, item 9, 10, 21 were still common misconceptions at T2 and item 9 persisted as the only common misconception at T3. The number of caregivers who correctly responded to each item from all assessments were shown in Figure 1.
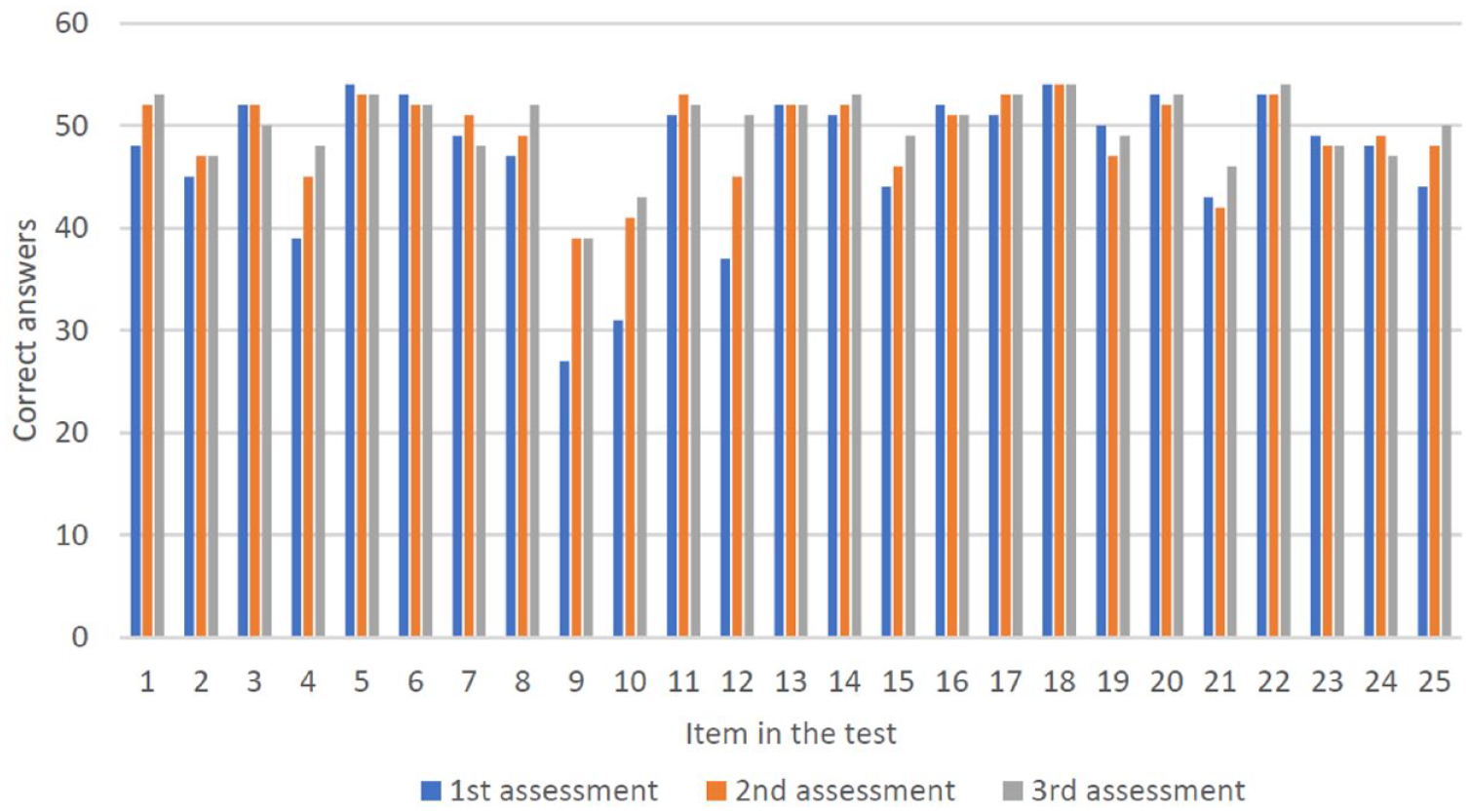
The number of caregivers who correctly responded to each item of the total of 54 caregivers from all assessments.
The following items were common misconceptions at T1:
Item number 4 “Each suction catheter insertion should not be retained in the trachea longer than 10 to 20 seconds.”; 15 caregivers (27.8%) incorrectly answered “false” indicating they did not know how long they should retain the catheter inserted for tracheal suction. Reducing suction time to less than 10 to 20 seconds is recommended to prevent hypoxemia.
Item number 9 “During suction, if I do not get as much secretions as I expected, I do not have to do anything else. It means my child has only that amount of secretion.”; 27 caregivers (50%) incorrectly answered “true” suggesting they would not be concerned if they got less amount of secretion than expected. Given that the situation could be a sign of retained secretion due to several causes, the caregiver must be cautious of risks or dangers.
Item number 10 “If my child looks dyspneic and I could not pass suction catheter into the tracheostomy tube, I should change the tube.”; 23 caregivers (42.6%) incorrectly answered “false” suggesting they failed to recognize that the inability to pass suction catheter indicates that the tube may be blocked or displaced. This situation is a red flag and requires quick attention.
Item number 12 “Before changing tracheostomy tube, I should apply lubricant in the lumen of the new tube to facilitate insertion.”; 17 caregivers (31.5%) incorrectly answered “true” suggesting they were not aware that lubricant must be applied on the external surface of tracheostomy tube only. Filling the lumen with lubricant could occlude airway patency and cause breathing difficulty.
Item number 21 “At home, I walk into the room and find my child unconscious and pale. The first thing I must do is to call my doctor.”; 11 caregivers (20.4%) incorrectly answered “true.” The correct response is to start basic life support immediately as a cardiopulmonary arrest is suspected. A series of cardiopulmonary resuscitation skills should be performed simultaneously along with emergency response system activation.
The score at T1 was analyzed for a relationship with demographics of the caregivers, that is, age, level of education, monthly household income and care experience; and the children, that is, age, tracheostomy indication, the number of comorbidities, tracheostomy tube changer and use of home ventilation. There was neither significant correlation nor difference of the score with continuous data nor difference of the score between different demographics, except for the number of children’s comorbidities. A Mann–Whitney U test showed that the score was significantly higher for whose children have >2 comorbidities (Median = 22, IQR 22-24) than whose children have 0 to 2 comorbidities (Median = 21, IQR 19-23), U = 225.5, P = .01.
Discussion
In this study we assessed the knowledge of caregivers after they took part in our educational program for pediatric home tracheostomy care. At the first assessment, the caregivers achieved a relatively high median score of 22 out of 25 that increased to 23 on the following 2 assessments. Despite of the high scores, some common misconceptions were found, and the caregivers consistently missed how to manage less-than-expected secretions during suction. The caregivers of children with >2 comorbidities scored 1 point higher in the test than those of children with 0 to 2 comorbidities.
Following our home tracheostomy educational program, the majority of caregivers displayed satisfactory level of knowledge by scoring over 20, that is, 80% of the maximum score. Although there is no definite cut-off value to classify an acceptable knowledge level, around 80% is widely applied and accepted in educational system as representing high proficiency. Hence, we presumed that passing 80% of the assessment could adequately ensure the knowledge acquired.
Knowledge assessment not only determines educational outcomes and ranks learners in term of competence, but also provides several additional benefits to both the learner and educator. For the learner, the assessment could enhance mastery of content since it offers an opportunity to practice knowledge retrieval. Regular knowledge retrieval is beneficial in later retention, organization and transfer of the knowledge. 15 It also improves confidence and raises an awareness of what the learner knows and needs to know.15,16 As a result, we believed that our regular assessments may have contributed to the improvement in knowledge as suggested by the higher scores that were observed at the later assessments. For the educator, the assessment helps to identify misconceptions which may possibly relate to individual or program shortcomings. Recognizing shortcomings in an educational program is an important part of course revision and improvement. 15 Another possible contributor to improved results in the knowledge assessment at T2 and T3 is that caregivers would have been becoming more familiar with the concepts and principles of tracheostomy care over time as they put it into practice caring for their children.
Some common misconceptions in home tracheostomy care were present at the first assessment, despite the caregivers having completed the educational program. Identifications of these and other incorrectly answered questions prompted appropriate discussion to correct caregiver knowledge. However, the caregivers still failed to answer 1 item while other common misconceptions were solved. We assume that the persistent flaw could be either that we failed to educate the caregivers or that there is lack of clarity in the question in the test. Hence, we could plan to discuss with caregivers and use their feedback to rectify both the educational program and the assessment to overcome these possible problems.
Among the demographics studied, the caregivers of children with >2 comorbidities were associated with slightly higher test score than those of children with 0 to 2 comorbidities. This finding may be explained by the fact that children with tracheostomy who have multiple complex conditions usually require high-level respiratory care. Therefore, taking care of children with more comorbidities possibly resulted in a better caregiver competency. However, Kun et al 17 found a different result in their study assessing knowledge in tracheostomy and home mechanical ventilation emergency; they found no significant differences of the knowledge between caregiver groups categorized by speaking languages, experience of the caregiver, and being trained as a licensed nurse. The difference in findings between our study and that of Kun et al 17 are likely explained by differences in test content, care complexity and caregivers who were health professionals.
Although the assessment in this study revealed important information, there can be issues when a test-based assessment is employed. Given that a test tends to generate idealized responses, the knowledge translated into a real-life practice may be less than the test result. Therefore, the good level of knowledge may not always guarantee the good quality of care. Several studies also highlight that poor outcomes in pediatric tracheostomy care are associated with other factors including neurologic impairment,18,19 failure to thrive, 19 and infancy. 20 However, none of these studies included assessment caregiver knowledge of tracheostomy care. We utilized the test developed which had the advantages of specific content relevant to tracheostomy care and of enabling simple standardized scoring. Future studies are needed to validate the relationship between test score and tracheostomy care delivered by a caregiver.
The other limitation of our study is that this is a single-center study with small sample size of children with tracheostomy. Our test and/or the test-based strategy may not be transferable to different home tracheostomy educational programs or services. We suggest that the assessment should be tailored to achieve feasibility of a local setting. Future multi-center studies are warranted to confirm benefits of the knowledge assessment and to propose other helpful tools for evaluating outcomes of health education.
Conclusions
Knowledge assessment after education in pediatric home tracheostomy care is helpful in determining the level of knowledge among caregivers and common misconceptions that need to be corrected. Higher scores achieved in 2 further assessments over 12 months suggest that regular assessment and practical experience are important factors improving caregiver knowledge. The number of children’s comorbidities was identified as a demographic associated with the knowledge. As these could be beneficial in quality improvement of the care and education, regular knowledge assessments of caregivers of children with tracheostomy are highly advocated.
Footnotes
Acknowledgements
We thank all the pediatric respiratory staff and pediatric nurses of King Chulalongkorn Memorial Hospital for their in-kind support. We would like to pay our special regards to Nuanchan Prapphal and Jitladda Deerojanawong, who are pioneers in pediatric respiratory home care in Thailand, for her mentorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Ratchadapiseksompoch Fund (RA61/017), Faculty of Medicine, Chulalongkorn University. WB is supported by a Charles Darwin University PhD scholarship. The funding sources was not involved in study design; in data collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.