
Abstract
Workplace violence (WV) is a significant occupational hazard for home health care workers (HHCWs). HHCWs are frequently exposed to Type II (customer/client) WV incidents but minimal evidence exists about exposure to Type III (coworker) WV and exposure to Type IV (personal relationship) WV is unknown. Furthermore, exposure to WV incidents is often underreported by HHCWs. The Haddon Matrix guided this research study. A cross- sectional research design was used with HHCWs (n = 50) working in Southwest Ohio in April 2020. HHCWs completed the Workplace Violence Reporting Survey, a 76-item tool used to estimate the frequency and reporting of WV incidents. Data were analyzed using frequencies, percentages, means, and standard deviations. HHCWs were 86% female (n = 43). Patients (28.3%) followed by their families (17.4%) and intimate partners (10.9%) are the primary aggressors of verbal abuse. The incident was too minor (6.5%), no action would be taken (6.5%), and it’s part of the job (4.3%) are major reasons HHCWs underreported WV. Type II WV is most pervasive when the aggressor is the patient. HHCWs experience physical assault and sexual abuse in their work environment. HHCWs underreported verbal abuse and physical assault when the aggressor was an intimate partner.
In the U.S., home health care is the fastest growing industry, with a projected growth of 33% by 2030. 1 Home health care is a convenient and less expensive option for patients to receive complex medical treatments and skilled care in the comfort of their homes. 2 Although patients benefit from home health care services, workers are at increased risk for workplace violence (WV). Results from previous survey research indicated the percent of home health care workers (HHCWs) who reported exposure to any form of WV range from 2.5% to 65.1%.3 -5 Given variations in sample size, methodology used, and the specific forms of WV investigated in previous research studies it is difficult to determine a precise prevalence of WV incidents experienced by HHCWs.
Non-physical aggression was most pervasive, with the highest percentage reported by HHCWs 65.1% during a study that asked about HHCWs personal experiences of emotional abuse (e.g., name calling) committed by a client or someone else in the home. 5 Physical violence was less reported by HHCWs in a study that investigated HHCWs’ experience of physical violence perpetrated by clients. 3 In 2 previous studies, HHCWs 27.6% 4 and 41% 5 reported incidents of WV in the form of sexual harassment. While these percentages are lower compared to other at-risk occupational groups working in healthcare environments, such as the hospital, HHCWs do work in environments that are unpredictable, potentially dangerous, and where resources and assistance are less accessible.
Additionally, HHCWs reported WV is a primary safety concern among other concerns for weapons in the home, neighborhood crime, and working evening shifts.5,6 WV in healthcare is recognized as a serious occupational hazard by both professional and federal regulatory organizations.7,8 WV is defined as the “act or threat of violence ranging from verbal abuse to physical assaults directed toward persons at work or on duty.” 9 It includes acts of incivility, bullying, verbal and physical aggression, and sexual harassment. 10
Workplace Violence Typology
In order to classify the relationships between the victim and the perpetrator and direct intervention efforts, the WV typology was developed. WV can be classified into 4 categories: (1) Type I, criminal intent, when an employee is robbed or their property is vandalized; (2) Type II, patient/client assaults an employee; (3) Type III, coworker threatens to attack another coworker; and (4) Type IV, personal relationship, an employee’s significant other threatens them while at work.11,12 Evidence shows that HHCWs are exposed to Type II WV, primarily verbal abuse.5,13,14 On the other hand, there is minimal evidence to show that HHCWs are exposed to Type I and III WV, and exposure to Type IV is unknown.15,16
Previously, researchers found WV was underreported, because HHCWs believe that only severe WV injuries need to be reported, beliefs that WV is part of the job were real, and their perceived barriers to reporting WV incidents. 5 Also, the Bureau of Labor Statistics (BLS) primarily reports on nonfatal injuries that require time off from work or medical treatment; thus, verbal abuse and near misses are not reported.8,17 Yet the majority of WV research in the home care setting indicates verbal abuse and nonfatal injuries that do not require time off and do not require medical care beyond first aid are mainly experienced by HHCWs.13,14 Existing research does not underscore the magnitude of WV in the home care setting, let alone the reporting of WV incidents. To overcome the gaps in research, a descriptive cross-sectional research study was conducted to describe WV among HHCWs and WV reporting. The aims of this research study are twofold: (1) describe the prevalence rate of HHCWs exposure to WV incidents; (2) describe the reporting behaviors of HHCWs exposed to WV incidents.
Methods
Research Design
A descriptive, cross-sectional design was used to investigate the prevalence rate of WV among HHCWs and their reporting behaviors of WV incidents. This research study was approved by the Institutional Review Board.
Conceptual Framework
The Haddon Matrix was used to guide this study. The Haddon Matrix has 2 dimensions that combine public health constructs of host-agent/vector-environment as the objects of change based on interventions that can be used by the host to protect themselves from injury. The columns in the Haddon Matrix represent the public health constructs and the rows represent interventions targeted at different phases of injury. 18 When applied to WV in the home care setting, the host is the HHCW who is the victim of WV and is susceptible to physical and psychological injury. The agent of injury impacts the host through its vectors. Vectors are patients, patient’s family members, visitors, coworkers, supervisors, and intimate partners. For this study, the constructs of host and vectors will be used to describe WV incidents experienced by hosts (HHCWs) and perpetrated by vectors. The host will be measured using the demographic form and the Workplace Violence Reporting survey. The vectors will be measured using the Workplace Violence Reporting survey.
Setting of Research Study
There were 2 partnering sites for this study, both located in Southwestern Ohio. The first partnering site is a home care agency comprised of HHCWs employed as advanced practice nurses (APNs), physician assistants (PAs), and social workers (SWs) who provide skilled care, health risk assessments, acute health care services, social support, and specialized disease monitoring during pandemics. The second site included home care agencies registered with the Ohio Department of Medicaid (ODM), participating in the home and community-based waiver programs. HHCWs for the second partnering site are employed by an agency, a hospital, or self-employed, are geographically dispersed throughout Southwestern Ohio, and may be employed as an APN, SW, PA, nurse, home care aide, or certified nursing assistant. The listserv of HHCWs registered to provide home care services in Southwestern Ohio was obtained from a gatekeeper employed by the home care agency and ODM.
Subject Sample
After IRB approval was granted, researchers distributed the demographic form and the survey via email to a convenience sample of 254 HHCWs. Potential participants included 48 HHCWs at the partnering home care agency and 206 HHCWs from home care agencies registered with ODM. The participants who were registered with ODM were employed; however, their specific employer was unknown. Participants were identified on the listserv received from ODM who met inclusion criteria for this study; no other criteria or reasons were used. To be invited to participate in this research study, HHCWs were 18 years or older, employed by the home care agency or registered with ODM, and English speaking.
Subject Recruitment
Recruitment for this study occurred online. The principal investigator worked closely with the gatekeeper to ensure accurate email addresses. An initial recruitment email was sent to 254 employee/registered email addresses in April 2020. Three follow-up emails were sent to each participant as a reminder to complete the study surveys. The recruitment email included a letter of information to participate in research and a link to the surveys. The letter explained the study purpose, procedures, risks/benefits for participation, the process for compensation, contact information for study personnel, rights as a research participant, and a statement indicating no identifying information connecting the participant to survey responses would be obtained. Reminder emails were sent once per week for 3 consecutive weeks after the initial recruitment email to increase response rates. The analytical sample size was 50 (19.7%).
Data Collection Procedures
After IRB approval, data were collected online using the REDCap website. A uniform resource locator (URL) link was sent to the participant’s employee email address. If the participant agreed to participate in this study, they could click the link and complete the demographic form and the survey. Upon completion, participants submitted the demographic form and the survey to the REDCap website. After submission, participants could receive a $20 Amazon electronic gift card for participating in this study by providing their email address using a separate survey. Using 2 separate surveys allowed participants’ responses and email addresses to remain separate, thus, maintaining confidentiality. Participants were referred to the Employee Assistance Program or their private healthcare provider if they felt sad or distressed while completing the survey. The estimated completion time for the survey was approximately 20 minutes.
Instrumentation
To collect data on lifetime exposure to WV, number of WV incidents experienced in the past 12 months, and reasons why incidents were or were not reported to the employer, the 76-item Workplace Violence Reporting Survey was used. 19 Using the Haddon Matrix, the survey contained questions organized by categories of WV such as verbal and sexual abuse, threats of violence, and physical assaults as perpetrated by potential vectors (e.g., perpetrators) of patient, patient’s family member, visitor, coworker, supervisor, or intimate partner. To promote consistency among participant responses, the following definitions for various forms of WV were embedded in the survey. Verbal abuse was defined as cursing, cussing, yelling at or berating a person in front of another, racial slurs, or humiliating and patronizing actions while at work. Sexual abuse was defined as unwelcome sexual advances, requests for sexual favors, and other verbal or physical conduct of sexual nature, insulting gestures, whistling, jokes of humor about gender-specific traits, offensive pictures, and offensive contact such as patting, pinching, brushing against body, attempted or actual fondling, or kissing while at work by any person. Threats of physical violence were defined as actions, statements, written, and nonverbal messages conveying threats of physical injury. Finally, physical assaults were defined as hitting, slapping, kicking, punching, pinching, scratching, biting, pulling hair, hitting with or throwing an object, spitting, beating, shooting, stabbing, squeezing, and twisting.
There are 2 sections of the Workplace Violence Reporting Survey that screen for reporting of WV incidents. 19 HHCWs were asked about their lifetime exposure to WV incidents while working in a home health care setting. HHCWs who reported a lifetime exposure to any form of WV were asked follow-up questions asking them to report the number of WV incidents experienced during the past 12 months. The survey was pretested before administration in a sample of HHCWs (n = 5) whose data were not included in this study.
Data Management
REDCap was used to manage the study data. REDCap was monitored daily to ensure it captured data entry. When the study period was completed, data were exported into the International Business Machines, Statistical Package for Social Sciences version 24.0 software for statistical analysis.
Data Analysis
Participants were asked about any exposure to WV incidents during their lifetime employment as a HHCW and the number of WV incidents experienced during the past 12 months employed as a HHCW. To determine the lifetime prevalence of WV exposure in our sample, the proportion (e.g., percentage) of HHCWs who reported “yes” to exposure to a WV incident at some point during their employment was calculated. To determine the average number of WV incidents during the past 12 months, HHCWs who reported “yes” (e.g., positive exposure) to a form of WV were then asked to report the number of incidents experienced during the past 12 months. Data were analyzed to generate means and standard deviations. Finally, data about reasons for reporting and reasons for not reporting were analyzed to generate frequencies and percentages.
Results
The objectives of this study were to (a) estimate HHCWs exposure to WV incidents during their lifetime employment and during the past 12 months; (b) Describe reasons for reporting and not reporting WV incidents. Primarily HHCWs are female (n = 43, 86%). For race, Black, Indigenous, and other people of color were collapsed into a single category of BIPoC. Race includes 2 categories, BIPoC (n = 26, 52%) and Caucasian (n = 24, 48%). Most respondents (n = 29, 58%) held an advanced degree. Occupational status of most respondents was APN (n = 27, 54%) and employed per diem (n = 19, 40.4%), see Table 1 for demographics.
Demographics of the Study Sample (n = 50).
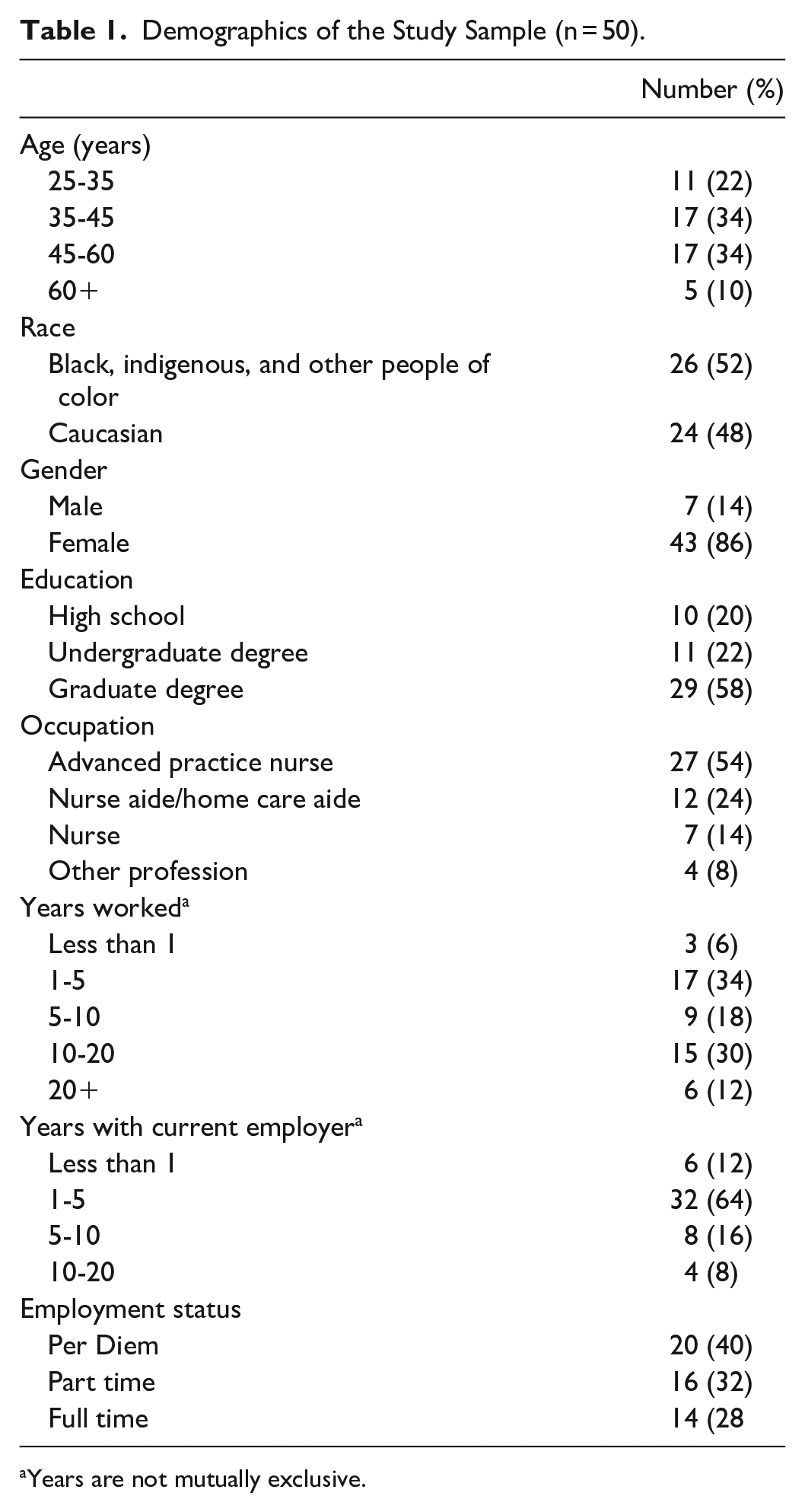
Years are not mutually exclusive.
Lifetime Prevalence of WV Experienced by HHCWs
WV incidents that were experienced by HHCWs during their lifetime employment are displayed in Table 2 using the Haddon Matrix framework. Participants (n = 50) who indicated experiencing WV incidents during their lifetime employment as a HHCW, verbal abuse was primarily experienced when the vector was a patient (n = 13, 28.3%), followed by the patient’s family member (n = 8, 17.4%) or intimate partner (n = 5, 10.9%). Participants (n = 4, 8.7%) indicated physical assault when the vector was an intimate partner or patient (n = 3, 6.5%).
Haddon’s Matrix Representing Lifetime Prevalence of WV Experienced by HHCWs (n = 50).
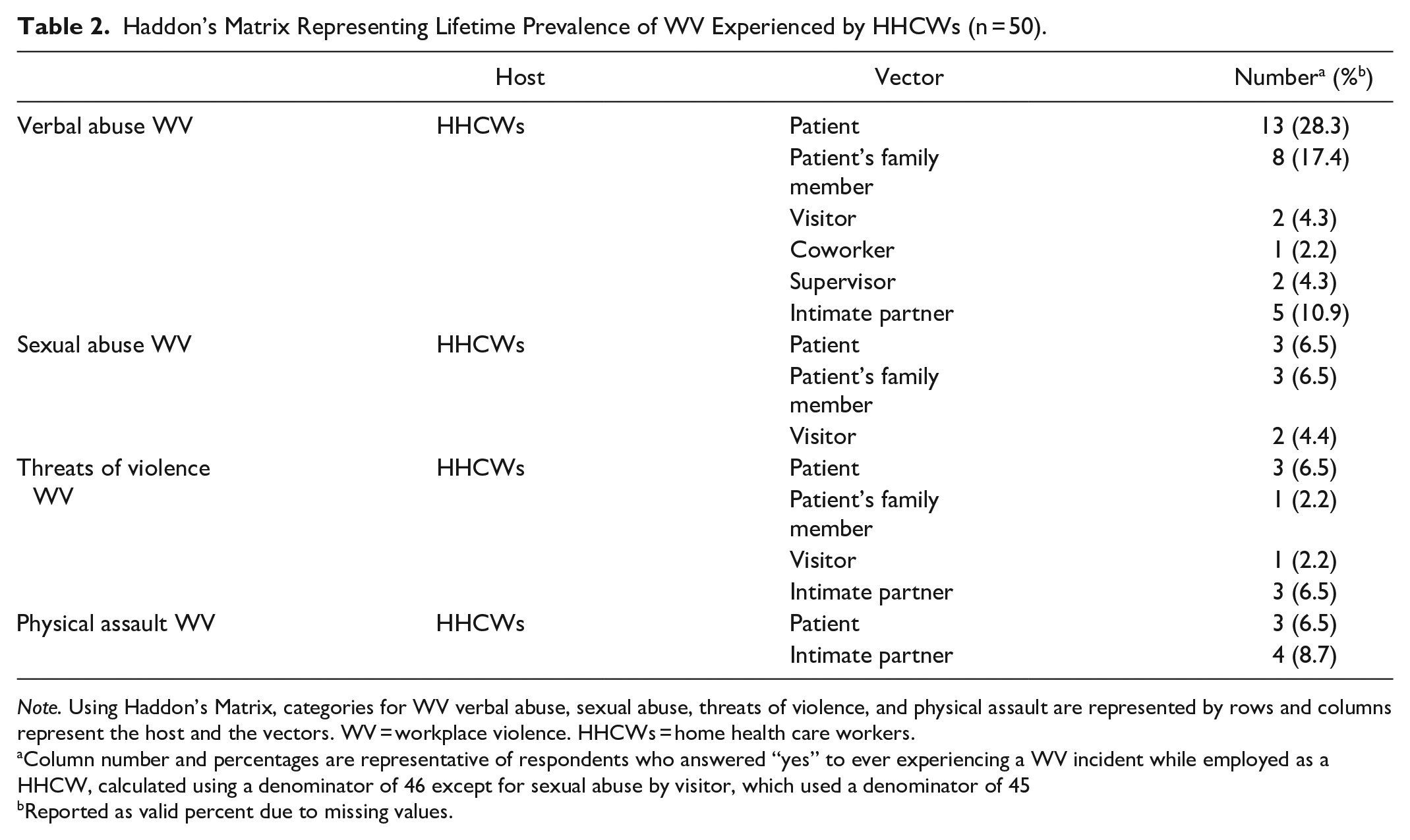
Note. Using Haddon’s Matrix, categories for WV verbal abuse, sexual abuse, threats of violence, and physical assault are represented by rows and columns represent the host and the vectors. WV = workplace violence. HHCWs = home health care workers.
Column number and percentages are representative of respondents who answered “yes” to ever experiencing a WV incident while employed as a HHCW, calculated using a denominator of 46 except for sexual abuse by visitor, which used a denominator of 45
Reported as valid percent due to missing values.
Verbal and sexual abuse incidents experienced during the past 12 months
WV incidents that were experienced by HHCWs during the past 12 months are displayed in Table 3 using the Haddon Matrix framework. The average number of verbal abuse incidents reported in the past 12 months was 3.08 (SD = 2.29) when the vector was a patient, 2.50 (SD = 2.20) by patient’s family members, 0.50 (SD = 0.71) by visitors, 0.50 by supervisor (SD = 0.71), or 2.20 (SD = 3.03) by an intimate partner. The average number of sexual abuse incidents reported in the past 12 months was 2.00 (SD = 1.73) when the vector was a patient, 1.33 (SD = 1.15) by patient’s family member, or 2.00 (SD = 0.00) by a visitor. Participants did not report any incidents of sexual abuse in the past 12 months when the vector was a coworker, supervisor, or intimate partner.
WV Incidents Experienced by HHCWs During the Past 12 months (n = 50).
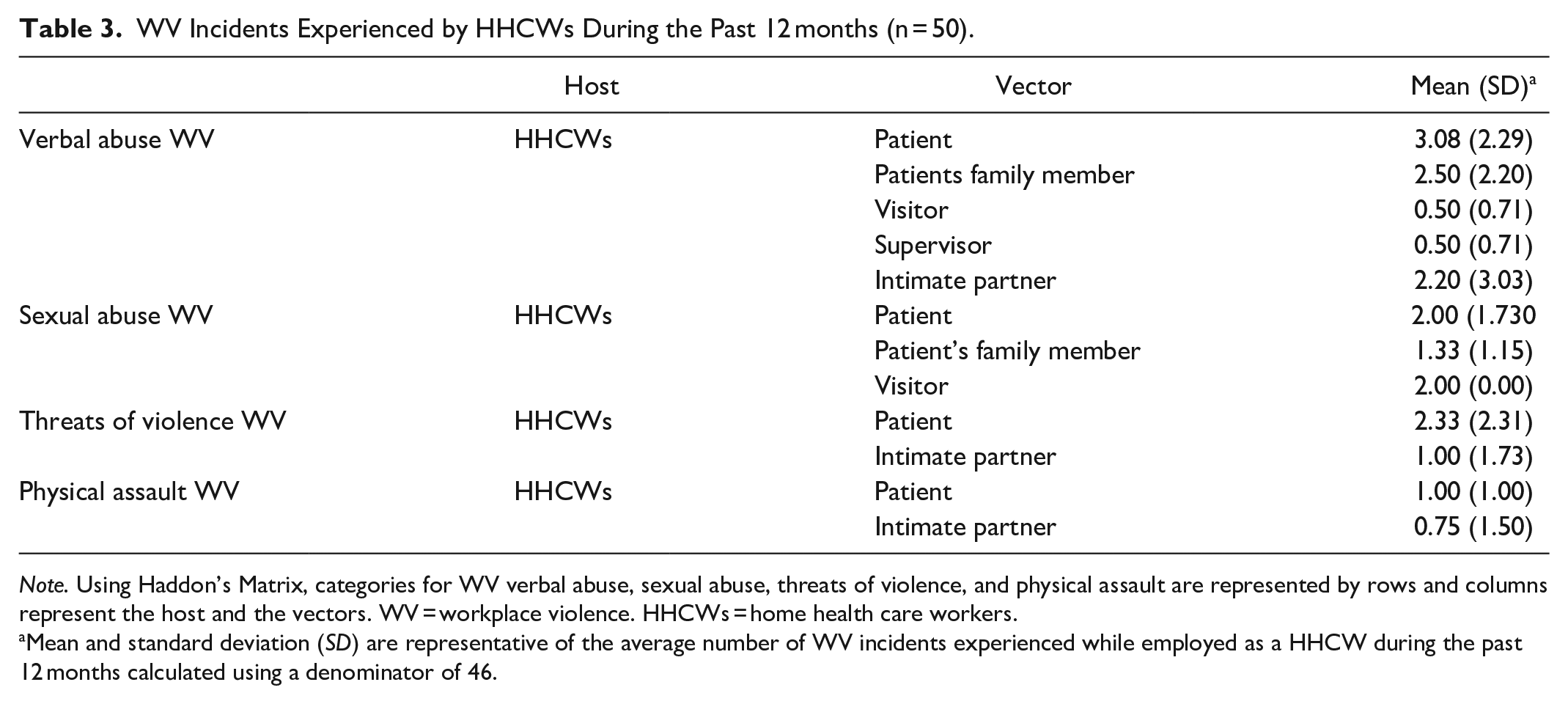
Note. Using Haddon’s Matrix, categories for WV verbal abuse, sexual abuse, threats of violence, and physical assault are represented by rows and columns represent the host and the vectors. WV = workplace violence. HHCWs = home health care workers.
Mean and standard deviation (SD) are representative of the average number of WV incidents experienced while employed as a HHCW during the past 12 months calculated using a denominator of 46.
Threats of and actual physical assault incidents experienced during the past 12 months
WV incidents experienced by HHCWs during the past 12 months are displayed in Table 3 using the Haddon Matrix framework. The average number for threats of physical assault incidents reported in the past 12 months was 2.33 (SD = 2.31) when the vector was a patient or 1.00 (SD = 1.73) by an intimate partner. Participants did not report experiencing threats of physical assault when the vector was a coworker or a supervisor. The average number for actual physical assault incidents was 0.75 (SD = 1.50) when the vector was an intimate partner or was 1.00 (SD = 1.00) by a patient. Participants did not indicate experiencing any incidents of physical assault when the vector was a patient’s family member, visitor, coworker, or supervisor.
HHCW Reporting of WV Incidents Experienced
Participants reported their incidents of verbal abuse when the vector was a coworker (n = 1, 2.2%) or supervisor (n = 2, 4.3%). Three respondents (6.5%) reported sexual abuse when the vector was a patient or the patient’s family member. Two (4.4%) participants reported sexual abuse when the vector was a visitor. One participant (2.2%) reported one incident of threats of violence when the vector was a patient’s family member or visitor.
Reporting of verbal and sexual abuse incidents during the past 12 months
The average number of participants reporting an incident of verbal abuse when the vector was a patient was 1.46 (SD = 2.11) or the patient’s family member was 1.38 (SD = 1.85). The average number of participants reporting verbal abuse when the vector was an intimate partner was 0.50 (SD = 1.00). Participants reported each verbal abuse incident when the vector was a coworker or supervisor. The average number of participants reporting an incident of sexual abuse when the vector was a patient was 1.00 (SD = 1.73), patient’s family member was 1.33 (SD = 1.15), or visitor was 2.00 (SD = 0.00).
Reporting of threats and physical assault incidents during the past 12 months
The average number of participants reporting incidents of threats when the vector was a patient was 2.33 (SD = 2.31). The average number of participants reporting incidents of physical assault when the vector was an intimate partner was 0.67 (SD = 1.16).
Reasons HHCWs Report and Do Not Report WV to Employer
Among the 7 participants who did report a WV incident, reasons for reporting varied, see Table 4. These reasons included the severity of the incident, participant was asked to report the incident, participant was required to report due to workplace policy, and the WV incident resulted in emotional or physical injury, see Table 4. Five participants disclosed that they did not report WV incidents. Reasons selected for not reporting WV were the WV incident was too minor or not serious, participant believed no action would be taken by their employer, and the view that WV is part of the job, see Table 4.
Reasons for Reporting and Not Reporting WV Incidents to the Employer (n = 50).
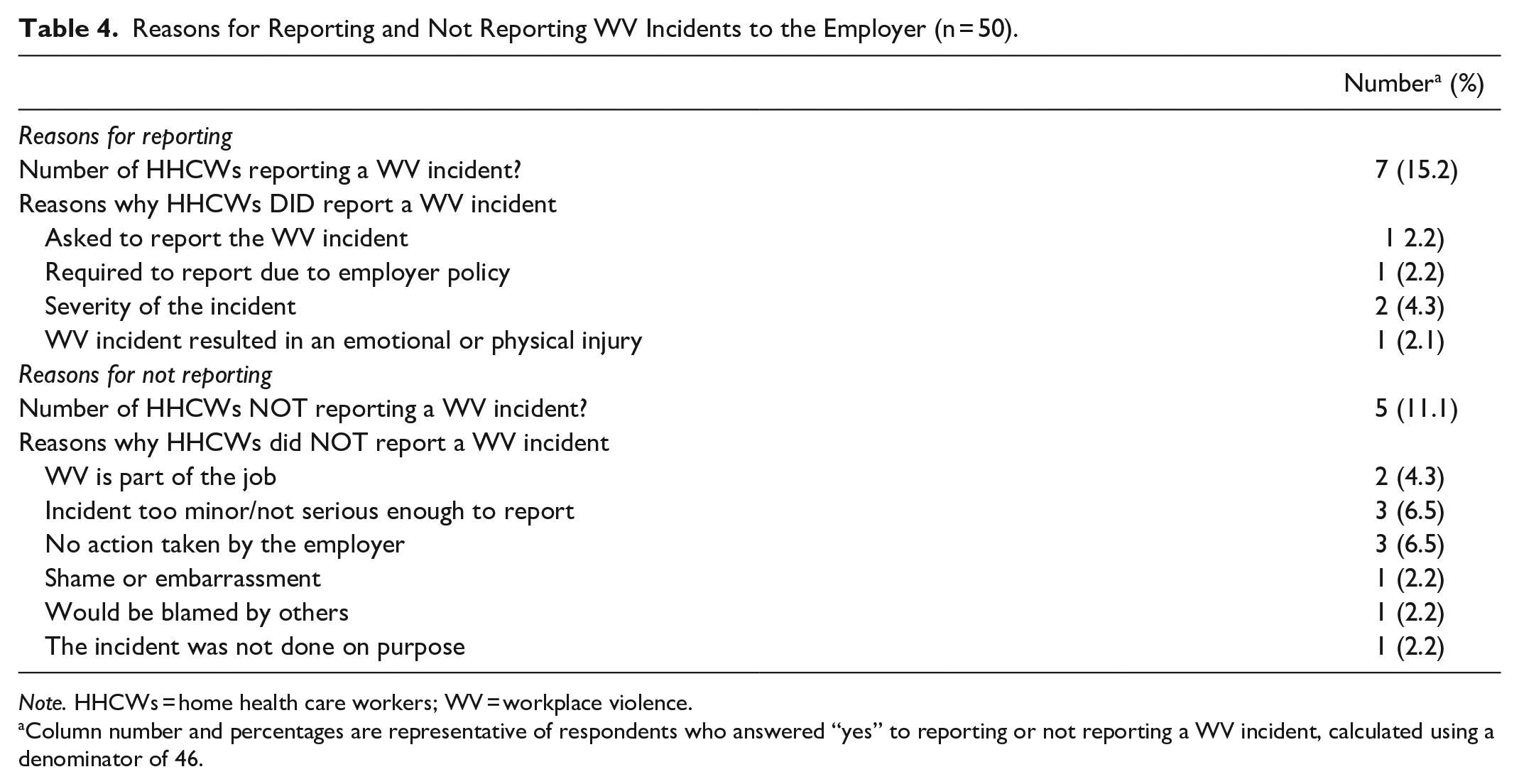
Note. HHCWs = home health care workers; WV = workplace violence.
Column number and percentages are representative of respondents who answered “yes” to reporting or not reporting a WV incident, calculated using a denominator of 46.
Discussion
WV Incidents
The results of this study support previous findings that indicate HHCWs are at risk for verbal abuse when patients are known vectors.3-5,13-16,20,21 In a recent meta-analysis, Byon et al 13 found the 12-month prevalence rate for WV was greater for verbal abuse when patients were known vectors and higher than physical violence for professional HHCWs (e.g., physicians, nurses, therapists, social workers) compared to nonprofessionals (e.g., home health aides, nursing assistants, personal care workers).13 Likewise, Hanson et al 4 found 50.3% of participants experienced verbal abuse.4 Similar to previous studies, our study demonstrates participants experienced greater verbal abuse than physical assaults and that patients are the primary vector. In a Sentinel Event Alert, Issue 59, it was recognized that verbal abuse has been tolerated far too long, is often overlooked, and exceeds all other categories of violence. 22
In our study, when the vector was a coworker, participants indicated WV exposures, with verbal abuse experienced on average one time in the past 12 months. Similarly, Ridenour et al 16 found HHCWs experienced verbal abuse when the vector was a coworker. Although HHCWs work alone, it is possible that HHCWs may have contact with other workers in the field, at the office, or engage in some form of communication; such encounters could lead to WV given a hostile work environment.
Lanza et al 23 found a significant relationship between physical and non-physical violence (e.g., verbal abuse), signifying that non-physical violence is a risk factor for physical assault. Recognizing that verbal abuse precedes physical assaults, there is an opportunity to mitigate the risk of physical assault by being proactive and addressing problems early. 19 When verbal abuse is recognized, workers can monitor patients for signs of imminent physical assault, which include pacing, mumbling, and persistent staring. 19 When verbal abuse is present, both preventative and early interventions should be implemented. For HHCWs, prevention should begin with risk assessments that include a patient history of violence and safety concerns in the patient’s home and surrounding neighborhood. 15 Also, workers should become aware of their own behavioral responses when confronted with verbal abuse. 19 This is especially important, because patients may view a HHCW as a “guest” in their home; thus, a certain level of respect or politeness may be expected from the HHCW regardless of the patient’s behaviors or language. Furthermore, both professional and accrediting agencies recommend reporting verbal abuse.7,22
In our study, participants reported exposure to Type II WV incidents of sexual abuse when the vectors were patients or the patient’s family member. Barling et al 20 initially identified HHCWs exposure to sexual abuse in the home care setting. Although WV and sexual abuse are theoretically distinct constructs, Barling et al 20 found that WV and sexual abuse empirically co-occur. In a study conducted by Nakaishi et al 5 findings indicate HHCWs reported incidents of sexual abuse were 14%. For HHCWs, WV, including sexual abuse, predicts fear of their reoccurrence in the workplace, thus further predicting anxiety and perceptions of injustice. 20 Barling et al 20 predicted HHCWs who experienced WV incidents have decreased commitment and increased withdrawal intentions, poor interpersonal job performance, greater neglect, and increased cognitive difficulties. To reduce the risk of sexual abuse in the workplace, it must first be recognized as WV. 20 HHCWs should receive training on how sexual abuse presents in the home care setting and that subtle remarks about the worker’s appearance, displaying pornographic magazines/movies, or inappropriately being touched should not be excused but regarded as WV. Policies and procedures on WV prevention should include information on sexual abuse and the reporting process. Nielsen et al 24 found that HHCWs received insufficient information on guidelines, policies, education, and training on preventing sexual abuse. In addition, management did not consider sexual abuse a serious problem, and too much attention could provoke negative emotions. 24 Valente and Bullough 25 recommend reliable policies and procedures, education, follow-up, and a “zero-tolerance policy” to mitigate sexual abuse, psychological consequences, and adverse employment outcomes. Conversely, there is concern that “zero-tolerance policies” are unequally enforced and fail to address the root causes of WV, such as workplace stress or conflict in the workplace. 12
Reporting WV Incidents by HHCWs
Our study findings demonstrate that HHCWs report some forms of WV and underreport other WV incidents. Meaning, HHCWs who experienced WV incidents in their lifetime employment and during the past 12 months, not all WV incidents were reported to the employer. It appears that HHCWs reported an WV incident based on timing of occurrence (e.g., lifetime or past 12 months), the type of WV (e.g., II, III, or IV), the vector, and category (e.g., verbal abuse, sexual abuse, threats of physical violence, and physical assault). During the past 12 months, HHCWs reported Type II WV incidents of verbal, sexual abuse, and threats were primarily reported when the vector was a patient, patient’s family member, or visitor. Whereas, during lifetime employment as a HHCWs, Type II WV incidents, sexual abuse, and threats were reported to the employer, thus under reporting verbal abuse. It is reasonable to believe verbal abuse was underreported due to recall, verbal abuse may have been less traumatizing so there was not a need for the HHCW to report, or HHCWs may tend to minimize the extent of verbal abuse and its consequences on their emotional health.
Type III and Type IV WV incidents were less prevalent among HHCWs. However, Type III WV incident, verbal abuse was underreported during a 12 month period when the vector was a supervisor. This is the first study to ask HHCWs about their exposure to Type IV WV; their experiences and underreporting behaviors should be further investigated. During lifetime employment, HHCWs underreported Type IV WV incident, physical assault. Based on findings from our study, it is reasonable to believe that when a vector is an intimate partner HHCWs may be at increased risk for IPV given the unsupervised and solitary work environment. When a vector is an intimate partner, the risk of assault may be higher for a HHCW who works outside the institution’s safeguards.
The workplace cultural norms and the environment has an essential role in reducing the risk of Type IV WPV through prevention, early identification, and intervention among workers who are victims of Type IV. 26 To provide a supportive work environment, workers who are victims of Type IV should have access to education, support from management and coworkers, and resources.24,26,27 All workers and managers should participate in education and training on the identification, treatment, and referral options for coping with victimization, which will promote a caring attitude and skillful approach with coworkers who are victims of Type IV WV incidents in the workplace. 26 Workers who are victims of Type IV WV incidents benefit from training in several ways: examining personal experiences, taking measures to ensure psychological stability and safety, and awareness of guidelines for dealing with Type IV in the workplace. 26
Byon et al 28 indicate that HHCWs are motivated to report WV incidents when reporting behaviors are perceived as beneficial, accepted as workplace cultural norms, and supportive management. Byon et al 28 recommended a simple, shortened reporting process for HHCWs, recognizing the distant and the peripatetic nature of home health care. The reporting process for WV incidents should be written and conveyed to HHCWs. In the context of home health care work, it may be reasonable to develop a universal and standard reporting process that is fast, simple, efficient, and requires HHCWs, regardless of employer or self-employed, to report WV incidents may streamline the reporting process.
Limitations
Our study was conducted during a time of national turmoil with racial injustice, a looming pandemic, lockdowns, and economic shutdowns, it is possible that participating in a research study was not on the forefront of potential participants’ minds and likely contributed to low response rates. Given the low response rate, the prevalence rate of WV experienced by HHCWs may have been underestimated in our study. Based on the information the investigators obtained, HHCWs were employed by a home care agency or employed by a home care agency registered with ODM. The response rate was 19.7% resulting in a relatively small sample size limited to one geographical region in Ohio. In addition, other occupations conducting home care visits were underrepresented such as social workers and therapists. A large sample with broader representation of all HHCWs would increase generalizability.
Self-reports based on the past 12 months may be subject to recall bias of events that were less at the forefront of the HHCW, resulting in underreporting. This may have been the case for verbal abuse which may be more prevalent and routine but was the most prevalent in this study. More extreme incidents such as physical assault may be remembered due to trauma. Type I (criminal-intent) WV incidents and reporting were not solicited in this study, which may underestimate WV incidents that occur in the community. Overall, the study has limitations that are typical with the methods utilized. These results do provide additional insight into WV for HHCWs and should be further explored.
Conclusion
The present study findings advance the understanding and knowledge of WV using the Haddon Matrix by identifying vectors that are the primary source for Types II (customer/client), III (coworker), and IV (personal relationship) WV in the home care setting. HHCWs in this study reported experiencing verbal and sexual abuse, threats of violence, and physical assault when the vector was a patient, patient’s family member, visitor, coworker, supervisor, or intimate partner. Future research should continue to examine WV among HHCWs; findings from this study show when vectors are intimate partners, Type IV WV does exist in the home health care work environment. Furthermore, HHCWs do underreport WV incidents. Although HHCWs in this study underreported WV, further investigation is required to fully understand underreporting in this population of workers.
Footnotes
Authors’ Note
Institution at Which the Work Was Performed: The University of Cincinnati
Author Contributions
Dr. Small conceptualized the research idea, selected and constructed study instruments, contributed to the study design, data collection, analysis and interpretation of data, manuscript development and preparation, and revisions for important intellectual content. Dr. Small agreed to be accountable for all aspects of the work and approved the final version of this manuscript to be published. Dr. Gordon Gillespie contributed to the study design and the analysis and interpretation of the data. He also revised the paper critically for important intellectual content, approved the final version to be published, and agreed to be accountable for all aspects of the work. Dr. Hutton contributed throughout the project, assisted in data interpretation, intellectual content and manuscript development. Dr. Davis contributed throughout the project, assisted in data interpretation, and manuscript development. Dr. Smith contributed throughout the project and assisted in interpretation of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this manuscript was provided by the Wekselman Dissertation Award and the National Institute for Occupational Safety and Health through the targeted research training program of the University of Cincinnati Education and Research Center Grant #T42OH008432
Institution and Ethics Approval and Informed Consent
The methods and materials for this research study were approved by the University of Cincinnati Institutional Review Board, Protocol Number: 2019-0550. All participants were provided an Information Sheet for Research.
Disclaimer
The views expressed here are those of the authors and do not necessarily reflect the position of the National Institute for Occupational Safety and Health.