
Abstract
This study assessed the prevalence of Adverse Childhood Experiences (ACEs) among Home Care Aides (HCAs) and explored the relationship between ACEs and mental health. A 2017 survey of 424 HCAs assessed childhood trauma using the CDC-BRFSS ACE module. Approximately 27% of HCAs had a high ACE score (between 4 and 10). There were no associations found between ACE score and respondent demographic characteristics. HCAs with high ACE scores reported lower rates of social and emotional support and higher rates of past-month hopelessness compared with those with no or limited experience of adverse childhood events. This research suggests that HCAs have higher than average rates of ACEs, known to be linked to various negative physical and mental health outcomes.
Keywords
Introduction
Adverse Childhood Experiences (ACEs) are traumatic events in childhood—such as abuse, neglect, or growing up in a household with people experiencing mental health disorders. ACEs are strongly related to health problems later in life including health risk behaviors, chronic health conditions, and mental illness.1-4 The greater the number of adverse experiences in an individual’s childhood, the higher their ACE score and the higher their risk for health problems later in life.1-4
ACEs are linked to various chronic health problems, such as respiratory disease, pain, diabetes, and cardiovascular disease.1,3,4 In addition to physical health issues, ACEs are associated with increased risk of developing psychological disorders from childhood through adulthood. Toxic stress, which occurs when a child experiences strong, frequent, and/or prolonged adversity without adequate support, can change brain development and affect how the body responds to stress. 5 Individuals who have experienced ACEs are at an increased risk of depression, anxiety, psychological distress, suicide, and behavioral disorders.1-4,6-10 There is a need for research identifying protective factors against depression and other mental health challenges, given their widespread prevalence and impact on quality of life. Various studies have found low social support to be associated with depression,7,11-17 and it is theorized that the presence of strong social support may buffer against depression. Unfortunately, those with high ACE scores often report low levels of social support.7,8,16,18,19
Approximately 61% of U.S. adults reported at least 1 ACE and 16% reported 4 or more ACEs. 4 Studies have found being female, identifying as Black, Indigenous, or other person of color, younger age, low socioeconomic status, unemployment, and less formal education are associated with higher ACE scores.3,4,19-21 ACEs also have been shown to affect the health of the workforce and have a negative impact on adult employment status.19,22 Adults who experienced child abuse have lower levels of education, lower wages, and fewer assets when compared with those who did not experience abuse or neglect as children. 23
Home Care Aides (HCAs) are members of a critical workforce who provide essential in-home care services and assistance with activities of daily living to older adults and people with disabilities. 24 The services provided by HCAs often allow their clients to remain at home rather than necessitating a move to an institutional setting. Maintaining independent living is a common goal for older adults and people with disabilities. In 2050, the population aged 65 and over in the United States is projected to be about 84 million, up from 43 million in 2012. 25 Due to the increasing aging population, the home care industry is growing rapidly and the demand for home care services is likewise increasing.
Many of the social factors associated with high ACE scores are common in this population. HCAs are disproportionally female, low-income, people of color, and with low educational attainment. 26 The median annual income for an HCA in the United States is $19,100, resulting from low wages and part-time hours. Over half have no formal education beyond high school. Additionally, providing care is an emotionally and physically stressful job.27-29 HCAs frequently work in isolation, in that they often work in the homes of their clients and do not have the assistance of another HCA. HCAs experience high rates of work-related hazards, including falls, musculoskeletal injuries, and abuse by their client,30-32 as well as a high prevalence of chronic pain. 33 There is limited data on mental health issues within the HCA population. However, studies focusing on family caregivers found these individuals had higher levels of anxiety and depression.17,34-36 Family caregivers also had high rates of a range of health conditions and risk factors including obesity, hypertension, insufficient sleep, multiple chronic diseases, and tobacco use.36,37
It is essential to understand and address these and other health issues in this important and growing workforce. Adverse experiences in childhood should be a central area of focus because of the powerful role that childhood trauma plays in determining physical and mental health outcomes in adulthood. The experience of ACEs is particularly relevant for HCAs and the work that they do. Many HCAs provide care for family members, most of whom are their adult parent. For example, in California 37% of personal care assistants provide care to their adult parent, similar to rates found in surveys conducted among Washington State HCAs. 38 Caregivers who experienced abuse by the parent they are caring for have higher rates of depressive symptoms compared with non-abused caregivers. 39 This family history also may create challenges in providing care and coping with stress, and can be re-traumatizing for caregivers.
To better understand how this issue affects HCAs, SEIU 775 Benefits Group (the Benefits Group) fielded an ACEs survey with English-speaking HCAs in Washington State. The Benefits Group is a national leader in providing quality training, health, and retirement benefits to the over 70,000 HCAs who support older adults and individuals with disabilities to live independently at home in Washington State. 40 The Benefits Group also conducts health research and implements health programs for HCAs. The purpose of the survey was to learn more about the early trauma experiences of HCAs to best provide programs targeted to their specific health needs. The organization used the findings to develop behavioral health programs for HCAs in Washington, including increasing investments in more behavioral health resources and self-care trainings for HCAs.
However, additional research was needed to more comprehensively explore the role that ACEs play in the mental health of HCAs and expand the limited literature on this topic. While it was recognized that ACEs were likely high in this population, it was unclear if high ACE scores would be associated with any mental health issues HCAs experience and if there were groups of HCAs in need of targeted interventions. Additionally, understanding potential interventions to lessen the impact of ACEs was critical for future research and program intervention, with the goal of supporting and sustaining this essential workforce. Thus, this current study had several goals: (1) To assess the prevalence of ACEs and ACE subtypes among HCAs in Washington State; (2) Determine if ACE scores differed by demographic factors; and (3) Describe the relationship between ACE score and mental health outcomes and assess if resiliency factors mitigated that relationship.
Methods
Design
For this analysis we used data from the 2017 HCA ACEs Questionnaire. In 2017, the Benefits Group partnered with Kaiser Permanente of Washington Health Research Institute (KPWHRI) to field a cross-sectional survey to inform health care programs. The Benefits Group provided KPWHRI a random sample of 938 English-speaking actively working HCAs. To introduce the project, KPWHRI mailed HCAs an invitation letter with a $2 bill and a unique survey access code. This was followed by an email with an authenticated link to the survey. HCAs could complete the survey online, by phone, or via a paper version sent in the mail. Of the 938 HCAS invited, 424 completed the survey (45% response rate). Half (50%) of those completed it online, 32% by mail, and 18% by phone.
Measures
The survey instrument included the CDC-BRFSS Adverse Childhood Experiences module, which was adapted from the original CDC-Kaiser ACEs Study. 1 The 11-item BRFSS ACEs module assesses the respondent’s childhood experience across 8 categories: abuse (emotional, physical, sexual) and household challenges (partner violence, substance abuse, mental illness, parental separation/divorce, incarceration). 20 Two categories from the original CDC ACEs study (physical and emotional neglect) are not included in the core BRFSS ACEs module, but were added to this survey. An ACE score (range 0-10) was calculated as the number of categories experienced. Higher ACE scores indicate greater exposure to childhood adversity before 18 years of age.
The survey included 2 indicators to assess the impact of childhood adverse experiences on adult social and emotional health. The survey assessed perceived social and emotional support by asking the question “How often do you get the social and emotional support you need?” from the Emotional Support and Life Satisfaction BRFSS module. 41 Responses were divided into 2 categories for analysis: high support (always/usually) and low support (sometimes/rarely/never). Participants’ current feelings of hopelessness were assessed with the question, “During the past 30 days, about how often did you feel hopeless?” from the Mental Illness and Stigma BRFSS module. 41 Responses were divided into 2 categories: high hopelessness (all/most of the time) and low hopelessness (some/a little/none of the time).
Because of the sensitive nature of the questions, all respondents were provided with resources and referral information for a national organization that supports adults who experienced childhood abuse. Respondents were allowed to skip any questions they did not want to answer. All survey responses were deidentified.
Data Analysis
Prevalence of each of the 8 ACEs and 2 neglect component experiences were calculated. The frequency distribution of the total ACE score was generated, and the mean and confidence intervals were calculated. Each respondent was classified into one of the following ACE exposure categories based on the number of adverse childhood experiences they reported: 0 (No ACEs), 1 to 3 (Low ACEs), or 4 to 10 (High ACEs); an ACE score of 4 or more is commonly considered a high level of ACEs. 3 ACE category exposure prevalence estimates were calculated overall and stratified by demographic variables including gender, age group (<50 years, ≥ 50 years), highest level of education (high school or less, some college or higher), and marital status (married, unmarried). Associations between ACE categories and a) demographic variables and b) support and hopelessness were tested using the Mantel-Haenszel chi-square statistic. Associations between ACE categories and hopelessness were stratified by social support to test for potential moderation using ordinal logistic regression.
Data analyses were conducted using SAS version 9.4 and Stata version 14.1. This research was reviewed and approved by the WCG IRB.
Results
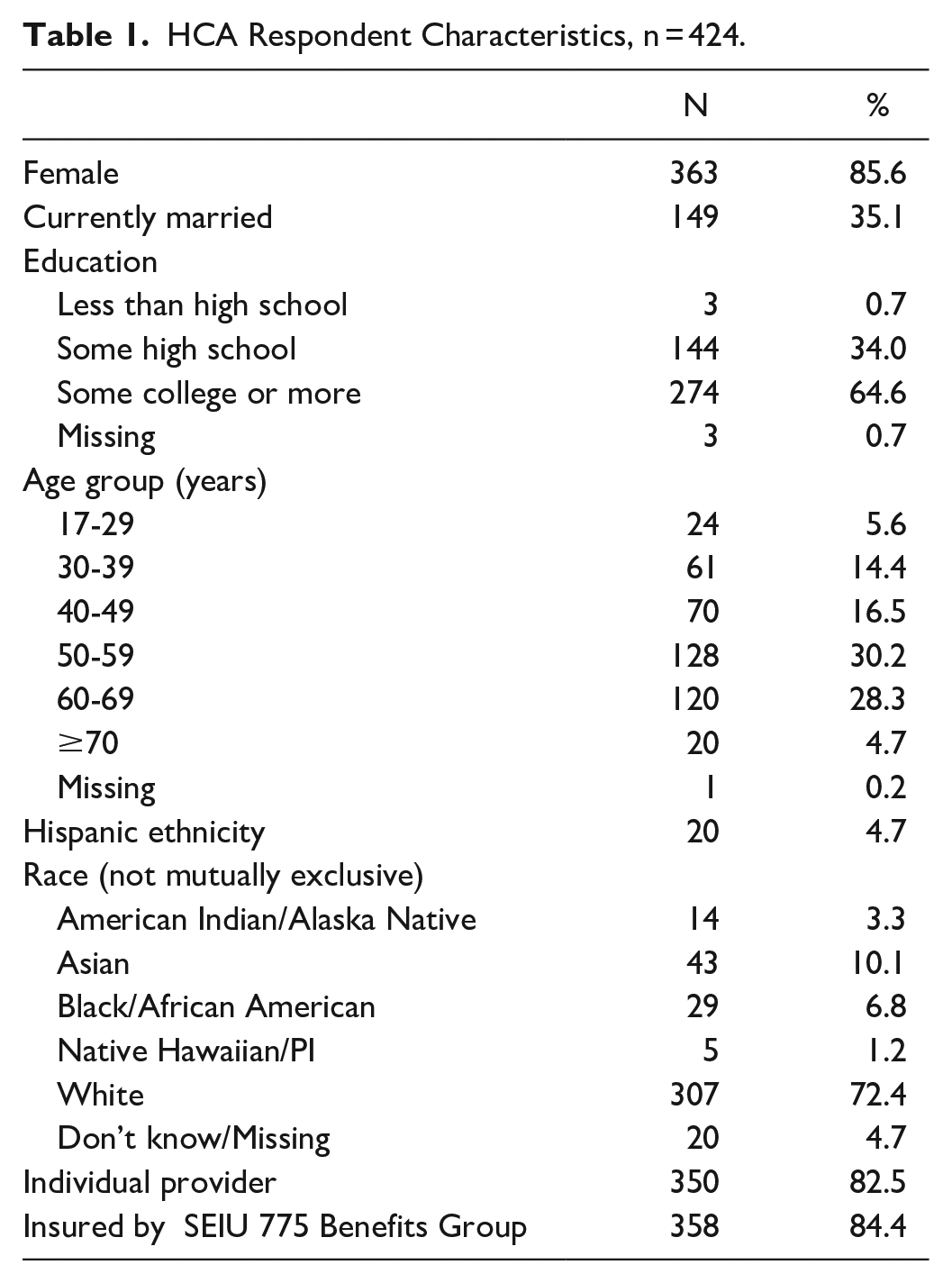
Out of the 424 HCAs who responded to the survey, 86% were female and 63% were age 50 and over (Table 1). The majority (72%) identified as white, 7% as Black/African American, 10% as Asian, and 3% as American Indian/Alaska Native. About two-thirds of respondents had attended some college or more as their highest level of education. Eighty-three percent of respondents were individual providers (IPs), 13% worked for a home care agency (APs), and 3% reported both. The vast majority (84%) reported receiving their health insurance through the Benefits Group. Caregivers eligible for insurance must have worked 80 hours a month for two consecutive months and maintained those hours for continuous coverage.
HCA Respondent Characteristics, n = 424.
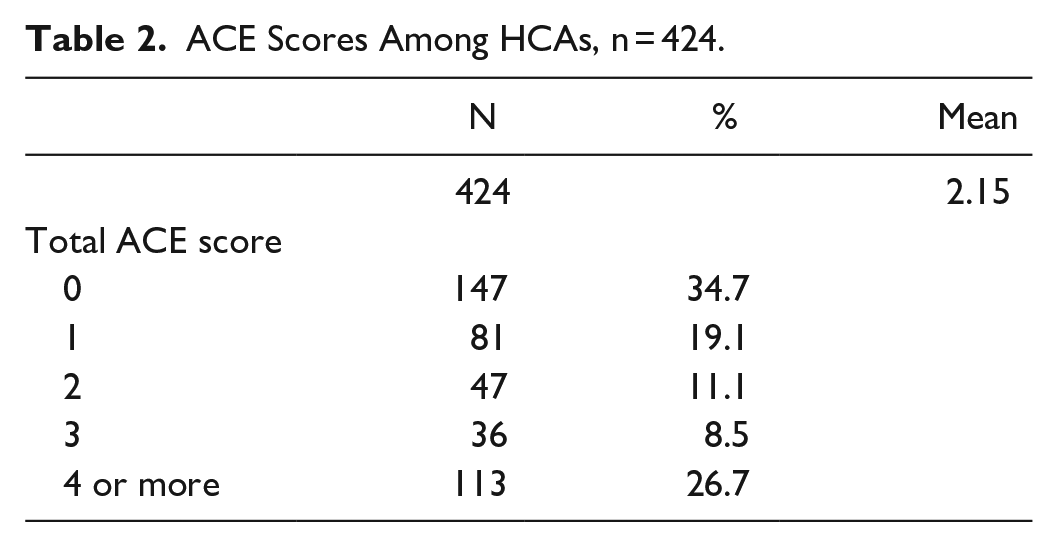
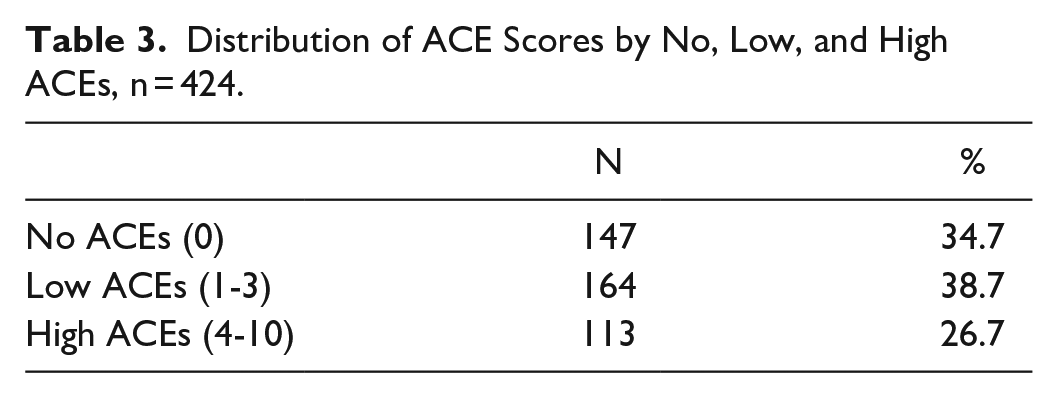
The mean ACE score across all 424 respondents was 2.15 (95% CI: 1.9-2.4; Range: 0-10) (Table 2). Nineteen percent (19%) had an ACE score of 1, 11% an ACE score of 2, and 9% an ACE score of 3. Over a third (35%) of respondents reported no ACEs, 39% a score between 1 and 3, and 27% had what would be considered a high ACE score (between 4 and 10) (Table 3).
ACE Scores Among HCAs, n = 424.
Distribution of ACE Scores by No, Low, and High ACEs, n = 424.
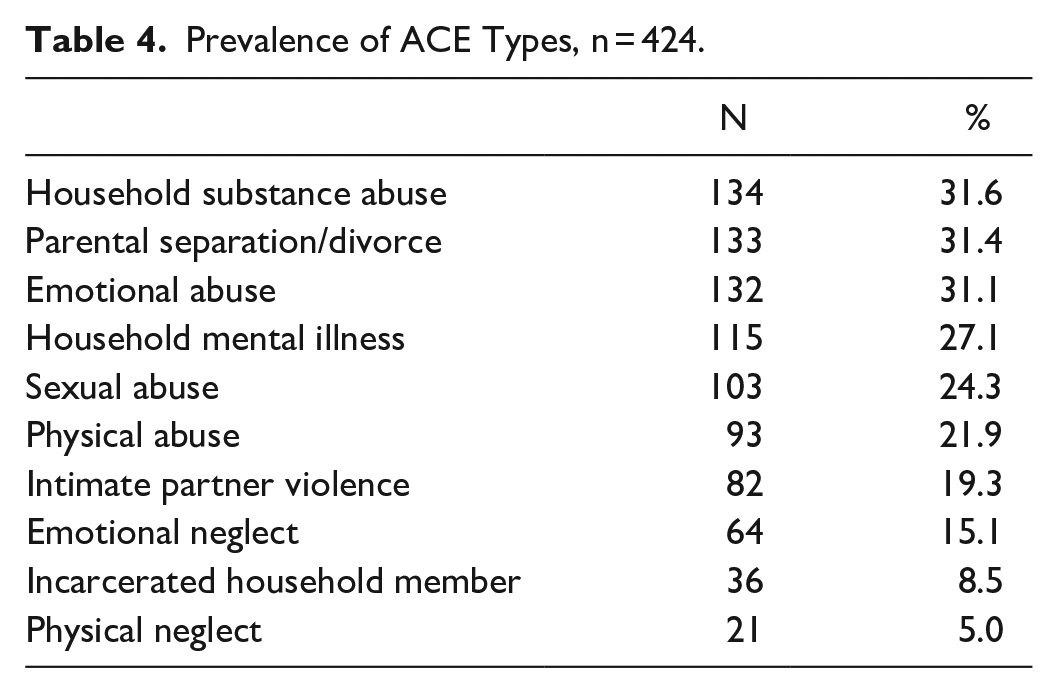
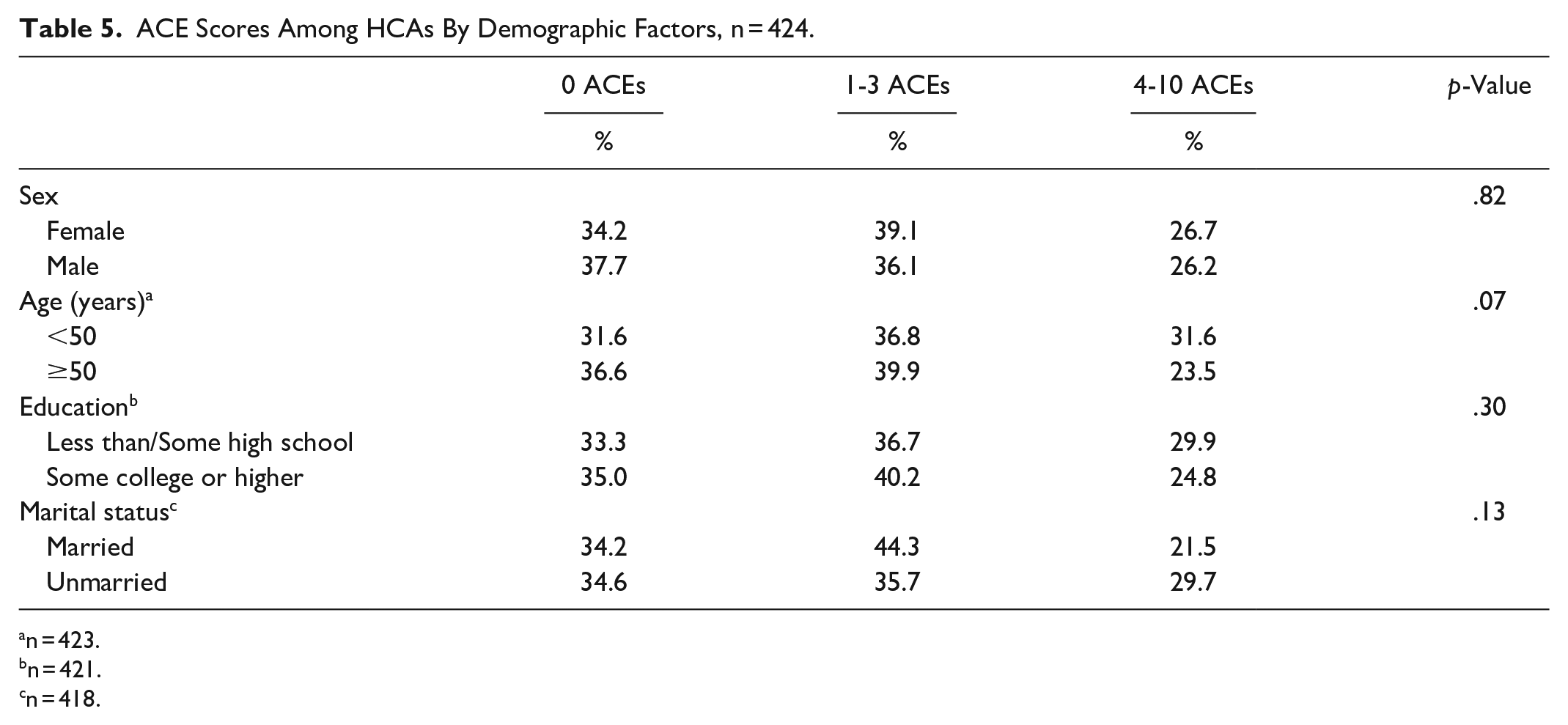
Among the individual ACE types, household substance abuse, parental separation or divorce, and emotional abuse were most reported, each at approximately 31%, followed by household mental illness (27%) and sexual abuse (24%) (Table 4). There were no significant associations found between ACE score and respondent demographics (Table 5). Respondents age 50 and older had lower rates of reporting high ACE scores compared with younger caregivers (24%vs 32%), but the difference was not statistically significant.
Prevalence of ACE Types, n = 424.
ACE Scores Among HCAs By Demographic Factors, n = 424.
n = 423.
n = 421.
n = 418.
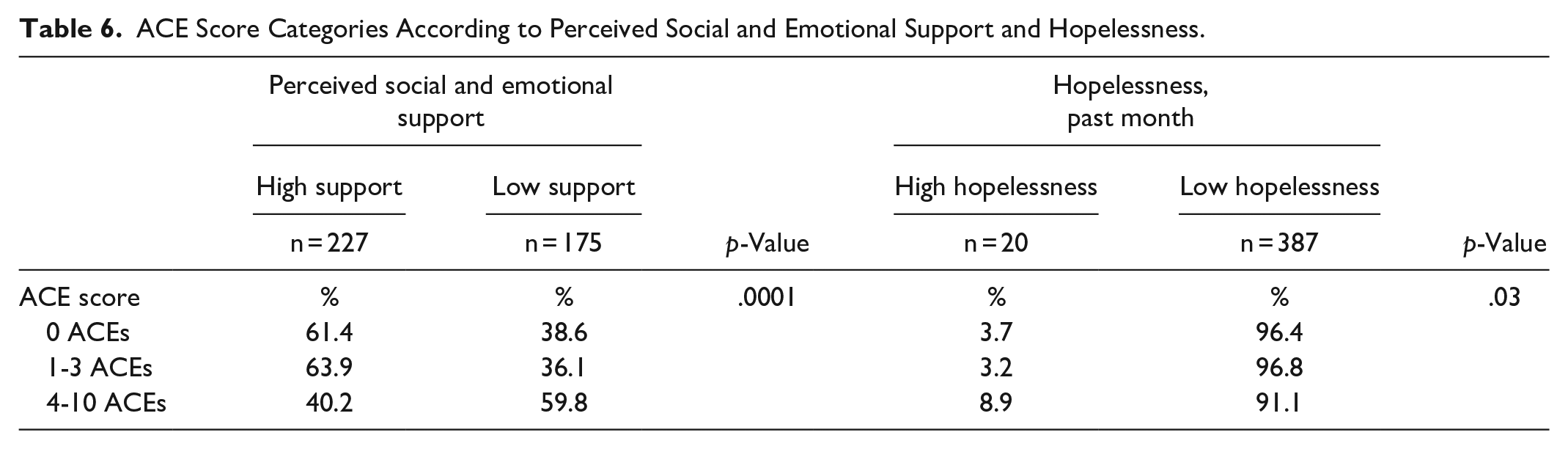
Respondents with high ACE scores reported lower rates of social and emotional support compared with those with no or limited experience of adverse childhood events: 40% of participants with 4 or more ACEs reported high support compared with 61% of those with 0 ACEs and 64% of those with 1 to 3 ACEs (p = .0001) (Table 6). Additionally, respondents with high ACE scores reported higher rates of hopelessness: 9% of participants with 4 or more ACEs reported feeling hopeless all or most of the time in the past 30 days compared with 4% of those with 0 ACEs and 3% of those with 1 to 3 ACEs (p = .03).
ACE Score Categories According to Perceived Social and Emotional Support and Hopelessness.
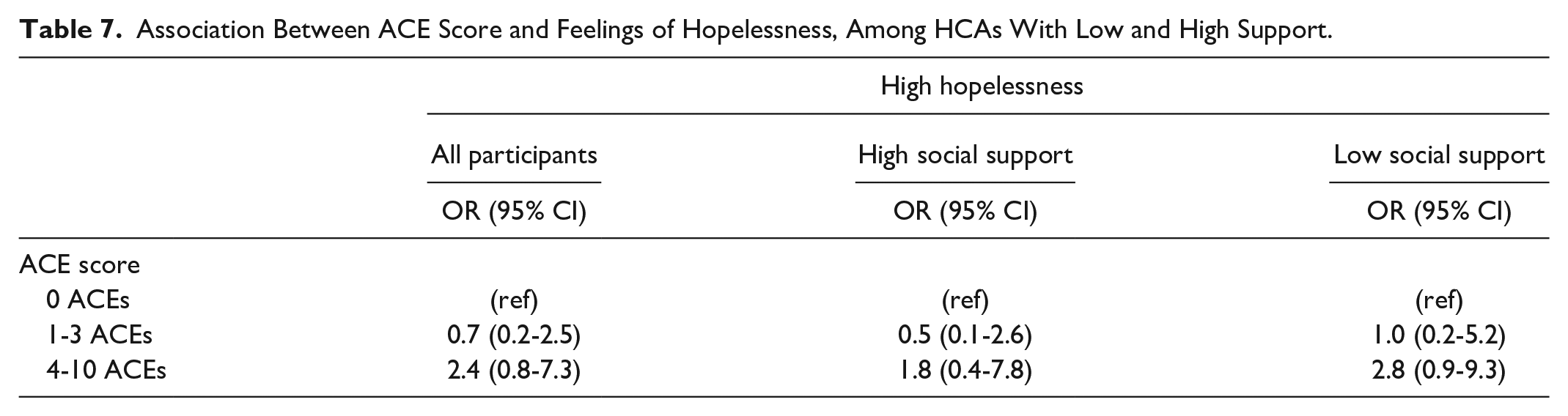
The relationship between ACE score and feelings of hopelessness did vary slightly by a participant’s level of social support, where the relationship between ACEs and hopelessness was mitigated by high support (Table 7). Those participants with a high ACE score and low social support were almost 3 times as likely to have reported high hopelessness (OR = 2.8, 95% CI: 0.9-9.3) compared with those with an ACE score of 0, while those with high ACE scores and high social support were less than twice as likely (OR = 1.8, 95% CI: 0.4-7.8) compared with those with an ACE score of 0. However, this relationship was not statistically significant.
Association Between ACE Score and Feelings of Hopelessness, Among HCAs With Low and High Support.
Discussion
While about 16% of the general population report an ACE score of 4 or higher, 27% of HCAs in this study had high ACE scores. 4 Like other groups with high ACE scores, HCAs are thus at elevated risk of developing chronic conditions, behavioral health issues, and psychosocial outcomes related to mental illness and poor health outcomes.1-4,6-10
In this study, there were no significant associations between ACE score and demographic factors. However, other research has found that people with high ACE scores are more likely to have lower socioeconomic status, lower education, identify as a Black, Indigenous, or other person of color, and be female.3,4,20,21 Although this study’s finding that younger caregivers reported higher ACE scores was similar to other research,4,8,18,20 the difference found between age groups was not statistically significant. Future ACEs research with this population would benefit from more comprehensive measurement of social factors to identify groups potentially in need of targeted intervention.
This study found that HCAs with an ACE score between 4 and 10 were over twice as likely to report recent high hopelessness compared with participants with no reported ACEs. This is in line with other research that found that high accumulation of ACEs increased the risk of feelings of hopelessness, particularly among women. 42 Ongoing monitoring of feelings of hopelessness is important, as it is an indicator of depression and can be associated with suicidality.43,44 Additionally, HCAs with high ACE scores had lower rates of perceived social and emotional support compared with those with no or low ACE scores. These findings are consistent with other research showing a relationship between low social support and ACEs.7,8,16,18,19
Our findings suggest that the relationship between ACEs and feelings of hopelessness may be moderated by perceived social support, where those who reported high levels of emotional and social support experienced less hopelessness, even if they reported adverse events as a child. Although our findings were not statistically significant, they are consistent with other studies that found perceived social support was a protective factor against depression among adults with ACEs.7,15,16 Comprehensive research with individuals experiencing mental health challenges would more effectively assess the role that social support might play in mitigating the impact of ACEs.
Limitations
This study had several limitations. First, the majority of survey respondents received their health benefits through the Benefits Group. As there is a monthly work hours requirement to maintain health insurance benefits, there is the potential that the rates of ACEs may be higher among those HCAs with inconsistent work hours, who are not enrolled in the health insurance plan. Second, the survey was conducted in 2017 and it is possible mental health rates have changed since that time. Third, this study did not collect information on many important health outcomes known to be associated with ACEs, including chronic disease indicators. Finally, validated scales with multiple items might be more comprehensive in the measurement of mental health outcomes.
Recommendations
The HCA workforce provides essential care, and their health is important not only so that they can lead full lives but also because of the high value of their work. Affordable, high quality comprehensive health care is an important benefit for a low-wage workforce with high ACE scores to address the complex and varied health needs common among those with a history of childhood trauma. Robust programs that focus on mental health for this population are also essential. To respond to this need, in 2017 the Benefits Group invested in Ginger, a convenient on-demand mental health support service that includes coaching, therapy, psychiatry, and self-care resources. The Benefits Group continues to explore options for supportive services that can help HCAs best utilize their comprehensive, low-cost health benefits.
These findings suggest social support may have a protective effect against a stressful event. HCAs could benefit from programs that increase social support, which may mitigate the risks associated with higher ACE scores. Increasing social support outside the family may be of particular value for those HCAs who are caring for a parent who abused them as a child. Further research exploring this association is recommended and may yield more peer-support models targeted to HCAs.
Conclusion
These findings fill a gap in our understanding of the role ACEs play in the health and wellness of HCAs. This information is critical for those working with this population in Washington State and in other states with similar direct care worker populations.
HCAs are a vital part of the healthcare system—they provide care for some of the most vulnerable members of our society and allow people to receive care within their own homes, preserving people’s dignity and ultimately lowering long-term care costs overall. The work HCAs do is low paying, and while some have access to health care benefits through their work, many throughout the country do not. With the ever-growing need for HCAs due to the rapidly increasing population of older adults who need care, and the shortage of people to provide that care, it is important that HCAs have access to affordable, high quality health care, especially for mental health. This research suggests that HCAs have higher than average rates of ACEs, which are known to be strongly linked to a range of negative physical and mental health outcomes. However, providing stable healthcare, social supports, and mental health support may help mitigate the level of risk associated with ACEs and ensure that these essential care providers are receiving needed care themselves.
Footnotes
Acknowledgements
We thank all study participants for sharing their experiences. We also thank Al Hansell, MPH for their valuable contributions to the early phase of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by SEIU 775 Benefits Group.