
Abstract
As individuals age, changes in their health status and functional level may begin to require caregiving from family caregivers. The role of caregiver can be taxing, a well-established phenomenon known as caregiver burden. While many studies have examined the factors within the caregiver that can be predictive of caregiver burden (or burnout), relatively few have examined the factors of the care recipient that predict caregiver burden. Using a sample of individuals enrolled in the Department of Veteran’s Affairs Home Based Primary Care program, we collected data on demographic, psychological (i.e. mood and cognitive) and nursing (e.g. ADL/IADL, fall risk, etc.) factors. Using stepwise regression modeling, we discovered that only care recipient’s age, IADL impairment, and gender predicted caregiver burden. We discuss possible causes of the relationships and implications for nursing and homecare practice.
Introduction
The Aging Population
The United States population is aging due to advances in rehabilitative medicine and effective health coverage.1,2 With life expectancy rising, it is important to consider physical, functional, and mental health issues commonly associated with aging.2,3
Issues Associated With the Aging Population
Changes in physical health and activity, functional capabilities, cognition, and other domains are inevitable to the aging process. 4 Change, often decline, in physical activity is most affected by health problems such as chronic disease, arthritis, and chronic pain. 5 Functional declines—reduced ability to perform activities of daily living (ADLs) independently—can also have a negative impact on physical activity as well as mental health. 6 The aging process is complex and multifactorial and declines in physical health and activity, functional ability, and cognition have a significant impact on functioning. 7
The prevalence of health problems and frailty increases as an individual ages.8,9 A major concern with decreases in functional mobility is an increased risk of falls, often due to impaired balance. 10 As individuals age, ADLs, such as bathing, grooming, and self-care may become difficult to independently complete. 11 While some older adults maintain a level of independence in completing ADLs, the ability to independently complete tasks related to instrumental activities of daily living (IADLs), such as shopping, making appointments, and managing medication regimens may become impaired due to cognitive declines (i.e., neurocognitive disorders 12 ). Limitations in physical health, functional abilities, and cognition—as well as longer lifespans - often mean that older adults require additional support. 13
Defining Caregivers and Caregiver Responsibilities
Attempts at defining the term “caregiver” has been somewhat problematic in the literature, given the wide variety of circumstances that can be given that label.14 -16 In general, a caregiver is someone who provides support to an ill patient or a patient with a disability.14,17 Caregivers assist with actions that an individual is no longer able to do for themselves. 18 Caregivers can be a spouse or partner, other family member, friend, or professional (i.e., aid or nurse 14 ).
The type of support varies, but can include physical, mental, emotional, and/or social support. 19 Caregivers often assist with ADLs or IADLs, cleaning, and/or shopping.17,19,20 Other types of support include emotional support and safety precautions.19,20
The amount of support depends on the needs of the individual requiring assistance. While the amount of assistance varies, day-to-day responsibilities of caring for another person can have an impact on the caregiver and can lead to a broad range of negative impacts.14,16,21
Impact of Caregiving on Caregivers
Caregiving is a multidimensional concept and can have both positive and negative impacts.22,23 Caregivers typically provide long-term care and support in addition to their roles as spouses, parents, children, and friend. 23 Caregiver burden is often viewed as perceived and/or observables consequences that caregivers experience as a result of providing direct care for a family member or friend. 22 Caregiver burden can be objective (observable, concrete, tangible aspects that have an impact on caregivers physical and psychological health, social connections, and finances) and/or subjective (positive or negative feelings), with subjective caregiver burden being associated with higher risks for negative health (i.e., depressive symptoms 22 ). Caregivers are susceptible to declines in their own health, both psychological and physical. 24 Chronic stress can result in poor quality of life, emotional distress, depressive symptoms, and isolation while the physical demands increase the risk for poor physical health. 25
Caregivers of Military Veterans
Since the establishment of specific programs addressing the informal care of military veterans in the United States in 2010, greater attention has been paid to these caregivers. 26 Furthermore, previous demographic studies have shown that military veterans are more likely to require caregiver support due to the greater incidence of medical and mental health issues, as well as the greater proportion of military veterans that are elderly. 27
Caregivers of veterans are also highly likely to be impacted by the burdens of providing that care. A cross-sectional survey of 1509 caregivers enrolled in the Department of Veteran’s Affairs (VA)’s caregiver support program found that they experienced significant levels of caregiver burden and depression. Loneliness and financial burden were also high among these caregivers to military veterans. 28
Aim of Current Study
As Veterans age, independence often declines, resulting in a dependence on a caregiver. 11 Caregivers play a vital role in assisting Veterans with cognitive impairments, ADLs, and IADLs, often sacrificing their own health and well-being. 25 Caregivers experience unique challenges and are at higher risk for negative emotional outcomes and problems.25,29 While caregiving can be stressful, it is also viewed as rewarding 20 . However, caregiver burden depends on many factors, including amount of physical and mental support the care recipient requires. Research exploring causes and predictors of caregiver burden has yielded mixed results. 30
Many family members are advised or choose to keep their loved one at home instead of placing them in a care facility, which often results in higher levels of caregiver stress and burden. In order for caregivers to provide effective support, it is important to consider their health and well-being. 25 Home-Based Primary Care (HBPC) is a service for veterans who are unable to travel to a VA facility for health care services. 31 HBPC providers travel to the veteran’s home in order to treat ongoing diseases and illnesses. 31 This program offers services to veteran’s who are homebound, isolated, or have caregivers that are experiencing caregiver burden. 31 HBPC helps to decrease some stress and increase well-being in both the veteran and caregiver. 25
Support through VA HBPC can maximize the well-being of both veterans and their caregivers by offering interdisciplinary interventions and services at the veteran’s home. While results from studies demonstrate measurable decreases in caregiver burden for veterans and caregivers enrolled in HBPC, little research examines caregiver burden predictors within this context. 25
The objective of this project is to identify factors that impact caregiver burden within caregiver dyads enrolled in one of the VA's HBPC program teams to help facilitate effective support for the caregiver.
Method
Current Sample
The current sample included veterans and veterans’ caregivers that were enrolled in a home based primary care (HBPC) program in an urban/suburban area in the northeast United States between October 2020 and February 2022. Information was gathered over the normal course of admissions to the program and pulled from medical records by the authors, all of whom are HBPC clinical team members, for a quality improvement project. This was study was exempted from institutional review board (IRB) review by permission by the IRB as it is considered secondary data analysis. Data were anonymized by the clinical team members prior to analyses and stored in encrypted network drives accessed only through VA computers.
Chart Review
Data collected through an extensive chart review of veterans enrolled in the program include demographic information, age at admission, caregiver relationship to veteran, mental health diagnoses, number of active medications, Zarit Burden Interview-12 (ZBI-12), Missouri Alliance for Home Care (MAHC-10), Braden Scale, Geriatric Depression Scale–Short Form (GDS-S), Saint Louis University Mental Status (SLUMS) Examination for Detecting Mild Cognitive Impairment and Dementia, amount of assistance veteran requires, and level of independence in ADLs and IADLs.
Missouri Alliance for Home Care (MAHC-10)
Falls are one of the most common issues among older adults, resulting from increased age and decreased reaction time, medications, medical conditions, decreased physical strength, impaired vision, and cognitive disorders. 32 The MAHC-10 is a validated fall risk tool that aims to reduce falls, improve patient outcomes, and establish a baseline of falls. 33 A score of 3 or less suggests that the patient is not at risk for falls while a score of 4 or above indicates that the patient is at-risk for falls. 33 The MAHC-10 has construct validity that distinguishes fall-risk versus non-fall-risk patients. 33
The Braden Scale
Pressure injuries, external pressure that damages skin and underlying tissues, are often preventable problems within the healthcare setting. 34 The Braden Scale can identify level of risk for pressure injury development and is comprised of 6 subscales (sensory perception, skin moisture, activity, mobility, friction and shear, and nutritional status) that have demonstrated reliability and validity. 34 Each subscale can be used independently, can identify specific preventative interventions, and have established validity. 34
Geriatric Depression Scale–Short Form (GDS-S)
The GDS-S is a screening measure that assesses depression in older adults.35,36 Scores range from 0 to 15 with scores of 0 to 4 suggesting a within normal limits range, 5 to 8 indicating mild depression, 9 to 11 moderate depression, and 12 to 15 suggesting severe depression. 36
Saint Louis University Mental Status (SLUMS) Examination for Detecting Mild Cognitive Impairment and Dementia
The SLUMS is comprised of 11 questions that is clinician-administered. 37 It assesses orientation, memory, attention, and executive functioning and is used to identify individuals who have mild cognitive impairment. 37 Scores on the SLUMS are based on 30-points. Cut-off scores take education level into account. 37 For individuals with a high school education, cut-off scores are as follows: 27 to 30 suggests within normal range, 21 to 26 is indicative of mild neurocognitive impairment, and 1 to 20 suggests dementia. 37 For individuals with less than high school education level, cut-off scores are: 25 to 30 is within the normal range, 20 to 24 is suggestive of mild neurocognitive impairment, and 1 to 19 is indicative of dementia. 37 The SLUMS has been found to have excellent convergent validity (r = 0.91) and strong sensitivity (0.742) when compared to the Montreal Cognitive Assessment (MoCA; 0.677 37 ).
Activities of Daily Living (ADL)/Instrumental Activities of Daily Living (IADL)
ADLs and IADLs were measured during the HBPC initial consult assessment by a member of the HBPC team. ADLs were assessed through the Veterans ability to perform the following activities: bathing in tub/shower, sponge, dressing, toileting, bed/chair transfers, and eating either independently, with assistance, or dependent on caregivers, additional notes may include Veterans compliance with the activities as well. 38 IADLs were measured by the Veterans ability to complete light housework, heavy housework, laundry, meal preparation, shopping, telephone use, and managing finances. 39
Zarit Burden Interview-12 (ZBI-12)
The ZBI was originally developed in 1980 as a self-report measure that evaluated a caregiver’s perceived impact of providing care. 40 The original ZBI had 29-items that was originally developed to assess caregiver burden in caregivers of Alzheimer’s Disease patients. 25 The original ZBI was later shortened to 22-items (ZBI-22) and was revised and expanded to measure caregiver burden for caregivers of other health conditions.25,40 Due to some difficulty understanding items and the duration of administration, a 12-item version (ZBI-12) was created to evaluate caregivers. 40 The ZBI-12 uses a 5-point Likert Scale (never = 0; nearly always = 4), where higher scores indicate higher caregiver burden. 25 It has been found to be both sensitive and effective in evaluating caregiver burden in those caring for older adults. 40
Procedure
Data already collected as part of ongoing clinical work was used to explore predictors of caregiver burden. No new data was collected for this project. Data was gathered via chart review utilizing VA’s CPRS system. All new admissions to the HBPC program occurring between October 2020 and April 2023 within the catchment area were included in the dataset. Veterans with missing data—either because the individual refused or was unable to provide the data—were excluded. Data was password protected and only identified team members had access to data.
Results
Participants
Participants were 201 individuals enrolled in an HBPC program. Individuals were military veterans who had been referred to HBPC due to established medical conditions requiring extensive follow-up that also made it difficult or impossible to attend in-person office visits. Average age of the sample was 83.3 (SD 9.0). The sample was predominantly male (97.5%) and white non-Hispanic (79.6%). Demographic information about the caregivers was not collected, but the most common relationship to their respective veteran was significant other (e.g., spouse, wife, husband, girlfriend; 55.2%), followed by child (e.g., son, daughter, step-son, daughter-in-law; 38.8%).
Analyses
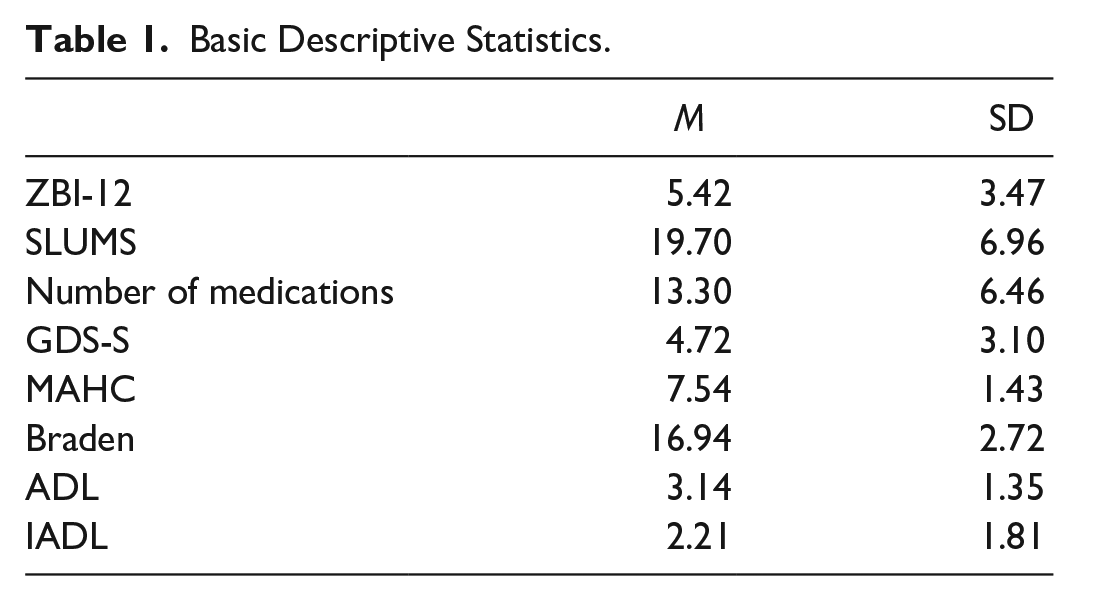
Basic descriptive statistics for the collected measures are presented in Table 1.
Basic Descriptive Statistics.
Multiple Regression Results
We utilized step-wise regression with backward elimination to determine the significant predictors of caregiver burden. This method allowed us to gradually refine the statistical model by eliminating non-contributory predictor variables based on specific criteria. In the first model, all predictor variables were included to establish a baseline understanding of their individual contributions. To address multicollinearity concerns, the second model excluded predictor variables with a variance inflation factor (VIF) greater than 2. Finally, in the third model, only predictor variables with a significant P-value (<.05) remained, ensuring that we considered only those variables that displayed a strong association with the outcome of interest.
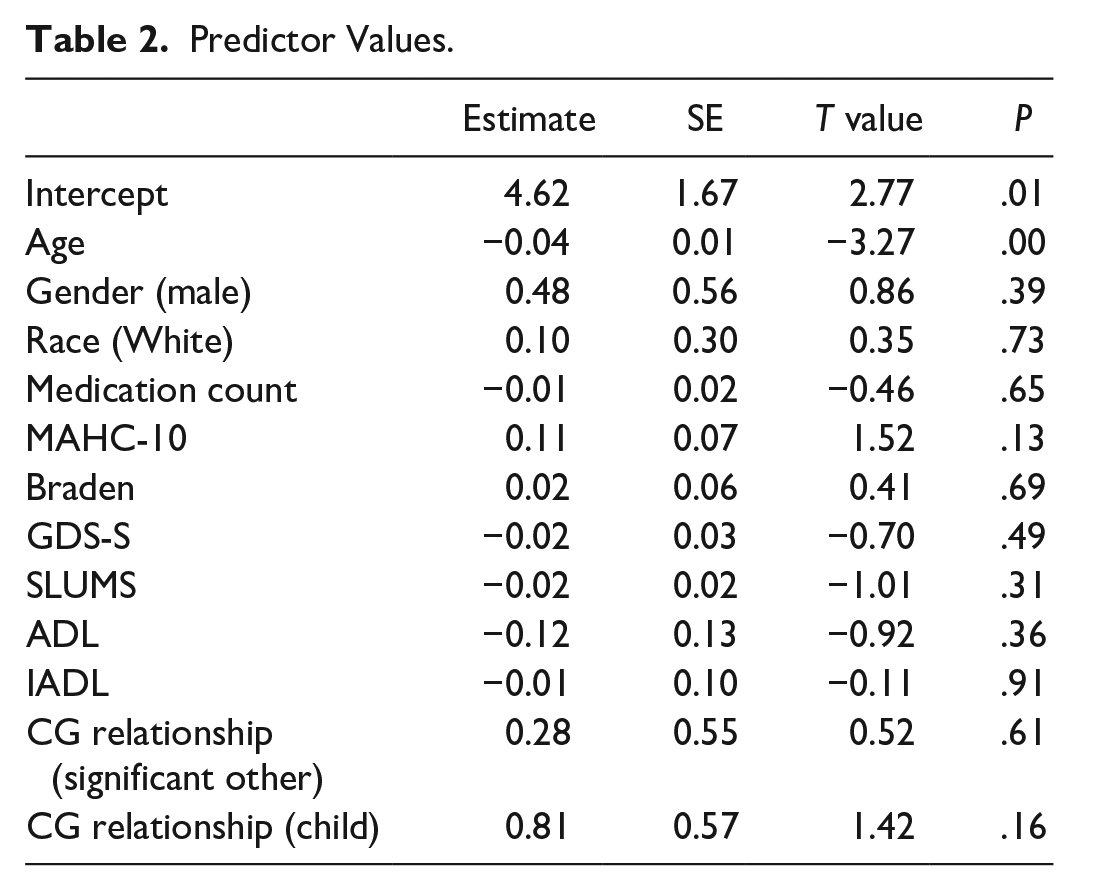
One hundred twenty-two observations were deleted in Model 1 due to incomplete data. The model was non-significant, explaining 22.3% of the overall variance, R2 = 0.223, F(12,66) = 1.622, P = .107. Specific predictor values were mostly non-significant, with the exception of age, and can be seen in Table 2.
Predictor Values.
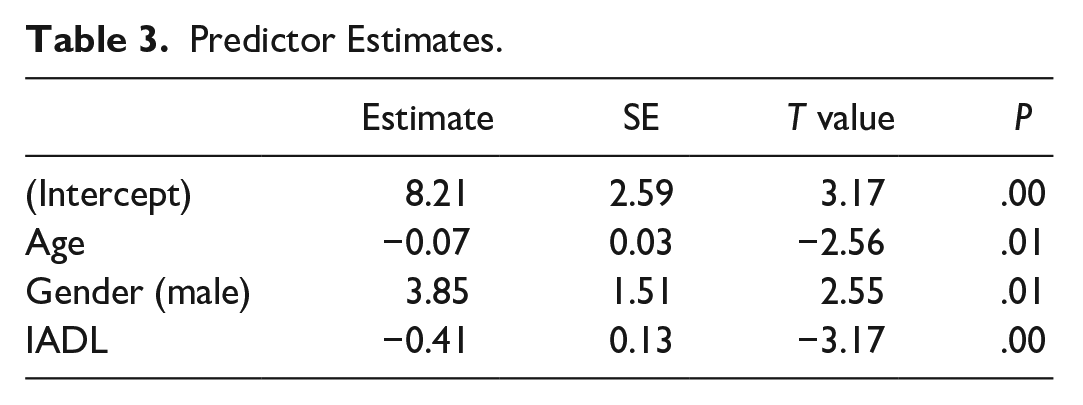
For Model 2, variables with expected significant multicollinearity such as IADL/ADL, and caregiver relationship (significant other)/caregiver relationship (child) were reduced based on higher VIF score, and other variables with VIF > 2 (medication count and Braden) were removed. Model 2 was significant, R2 = 0.20, F(8, 72) = 2.26, P = .03. For Model 3, variables with P > .1, namely variables not approaching significance, were removed. These were GDS-S, SLUMS, race, MAHC-10, and caregiver relationship. Notably, GDS-S and SLUMS were both removed, and as these were the variables with most missing data Model 3 was run with 197 observations. Model 3 was significant, R2 = 0.10, F(3, 194) = 7.39, P < .01. Predictor estimates can be seen in Table 3.
Predictor Estimates.
Discussion
Our study’s aim was to discover what individual characteristics would predict their caregiver’s level of burden in our sample of homebound elderly veterans. We examined data gathered from individuals enrolling in one of the VA’s HBPC program teams and completed step-wise multiple regression analyses. We tested such predictor variables as demographic factors, fall risk, skin integrity, mental status, depression, ADLS, and IADLs. Among our sample of 201 individuals, we found that caregiver burden was reliably predicted by veteran’s age, gender, and level of impairment in IADLs. The preponderance of our predictors were not significant predictors of caregiver burden. As with any null result, the absence of evidence (of a predictive relationship) is not evidence of absence.
Three predictors were found to have significant relationships with caregiver burden—care recipient age, gender, and level of IADL impairment. Of these the most straightforward relationship is for IADLs. As a care recipient’s ability to complete their own IADLs diminishes, their caregiver’s burden increases, which indeed has been observed in other studies.41,42
Age showed a negative relationship, indicating that as age increased caregiver burden decreased. This would seem to be counter-intuitive, as one would think that a younger care recipient would be more vital, more able to participate in their own care, even as IADL impairment is accounted for in the model. Indeed, previous results 43 show a positive relationship between care recipient age and caregiver burden. However, studies examining the components of caregiver burden have found that care recipients’ age negatively correlated with caregiver’s feelings of guilt, 44 so it is reasonable to suggest that this decreased guilt could in turn lead to the decreased burden seen in our sample.
Gender should be interpreted with caution, given our highly unbalanced sample population. However, it is also this imbalance that makes this result so striking, given the magnitude of the difference between men and women in our sample. In a previous study of partner caregivers—that is individuals who provide care for their partner or spouse—a similar gender gap was found, although it may be more related to the fact that female caregivers experience more secondary stressors. 45
Limitations
The conclusions that may be derived from this study are limited by the nature of its design as a small-scale analysis of secondary data gathered from a single group. A larger sample size may have uncovered further relationships than we were able to determine, and we were necessarily limited in our ability to choose which variables we would analyze. We would certainly have benefitted from examining caregiver variables, including demographic variables such as age and gender, information about the caregiver’s own health and mental status, or further information about other supports available in the home. However, this information was not available for the current study.
Furthermore, our convenience sample comprised only homebound military veterans enrolled in a specific care program through the VA, only in 1 geographic location, and during the COVID-19 pandemic. Although some of the related populations—older adults, homebound adults, individuals requiring care for chronic conditions—are large and likely to continue to expand, the ability to generalize to any of these greater populations is largely limited.
Conclusion
Despite the limitations of this preliminary study using extant data, we were able to uncover that caregiver burden is negatively predicted by care recipient age, and positively predicted by level of IADL impairment, and care recipient gender (male). Given that to our knowledge there are no other studies examining the relationship between care recipient factors and caregiver burden for homebound adults, we felt that these limitations were outweighed by the value of providing a first glimpse of these intriguing connections.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.