
Abstract
This paper is an examination of the relationship between continuity of care with home health physical therapists following hospitalization and the likelihood of readmission. We conducted a retrospective cohort study. Using rehospitalization as the dependent variable, a continuity of care indicator variable was analyzed with a multivariable logistic regression. The indicator variable was created using the Bice-Boxerman Index to measure physical therapist continuity of care. The mean of the index (0.81) was used to separate between high continuity (0.81 or greater) of care and low continuity of care (lower than 0.81). The sample included 90,220 patients, with data coming from the linking of the Outcome Assessment and Information Set (OASIS) and an administrative dataset. All subjects lived in the NYC metro area. Inclusion criteria was a patient’s admission to their first home health care site following discharge occurring between 2010 and 2015, and individuals who identified as Male or Female. In comparison to low continuity of physical therapy, high continuity of physical therapy significantly decreased hospital readmissions (OR = 0.74, 95% CI 0.71-0.76, p ≤ .001, AME = −4.28%). Interpersonal continuity of physical therapy care has been identified as a key factor in decreasing readmissions from the home care setting. The research suggests an increased emphasis in preserving physical therapist continuity following hospitalization should be explored, with the potential to reduce hospital readmissions.
Keywords
What Is Known on This Subject
• Home-based physical therapy is a key function of recovery following hospitalization when addressing activities of daily living.
• Continuity of care has been shown to be an important metric across multiple disciplines in preventing rehospitalization.
What This Research Adds
• This study shows that when compared to low interpersonal continuity of care, high interpersonal continuity of care between the physical therapist and patient significantly decreased hospital readmissions.
• Future research should examine the strength of such relationships as a predictive factor via measures such as communication and trust.
Introduction
Home-based physical therapy has shown to be effective in improving physical function across a variety of patient populations by leveraging patients’ everyday environments to address activities of daily living.1 -3 Exercise delivered at home has shown to be more effective than standard of care at improving quality of life and patient mobility, particularly among older adults. 4 An advantage of home-based physical therapy involves the assessment and treatment of multiple body functions, including strength and balance, within a familiar and meaningful environment. This has been shown to help prevent traumatic events, such as falls, or hospital readmissions. 5
Extensive utilization and documentation of home health care services have produced large datasets to understand the characteristics of an effective home-based physical therapy episode of care. 6 These large administrative datasets have allowed for secondary analysis to illuminate associations between patient outcomes and characteristics of home-based physical therapy. Reducing hospital readmissions is a critical goal in home-based physical therapy, as hospital readmissions significantly increase the risk of patient morbidity and mortality.7,8
Continuity of care has been shown to be a promising characteristic to promote greater patient satisfaction and functional outcomes across a variety of populations and physical therapy settings.6,9 -11
Continuity of care includes informational, managerial, longitudinal, and interpersonal components.12,13 Informational continuity includes the consistency of patient-centered care via shared information of a patient’s past events, medical history, values, and personal contexts.12,13 Managerial continuity involves consistency and coherence in patient care that is also responsive to changes in a patient’s needs or medical status. 12 Longitudinal continuity implies a “medical home” in which care is accessible and in a familiar environment. 13 Lastly, interpersonal continuity is the consistency of the relationship between the patient and provider.12,13 This final definition, interpersonal continuity, is the one this research focuses on. The metric of interpersonal continuity considers a patient’s total number of home care visits, their total number of visits by a physical therapist, and the total number of physical therapists who provided care. 6 As such, a lower number of physical therapists who provide care to a single patient would result in a higher level of interpersonal continuity of care. This measure is often the focus in continuity of care research,6,10,11 as it can be more easily tracked via administrative and clinical data when compared to other forms of continuity. Additionally, the evidence delivers a clear message for implementation purposes—achieving a one-to-one patient-to-therapist ratio has the potential to promote greater functional outcomes and prevent adverse events over the course of care. 6
To our knowledge, only one study has investigated the associations between home-based physical therapy interpersonal continuity of care and hospital readmission. 6 Above average continuity of care produced significantly lower odds of hospital readmission and higher odds of improving physical function when compared to below average continuity of care. 6 That study included a dataset from 2009. Since then, clinical documentation systems in home health care have been updated, physical therapy practice patterns have advanced, and substantial progress has been made toward doctoral credentialing of physical therapists. Current documentation systems include updated activities of daily living and fall assessments that may be relevant covariates when assessing associations between continuity of care and hospital readmission.
Recognizing the strong potential of continuity of care to prevent hospital readmission, 6 and the deleterious effects of hospital readmission on health,7,8 it is critical have a more current understanding of the association between these 2 factors. The purpose of the current study was to examine the association between interpersonal continuity of care in home-based physical therapy and hospital using a large homecare dataset between 2010 and 2015. It was hypothesized that lower levels of interpersonal continuity of care would be associated with higher risk of hospital readmission.
Methods
We utilized an observational, retrospective cohort study of patient outcome and home health care visit data to determine the role of interpersonal continuity of care (COC) in reducing hospital readmission risk. An urban, non-profit home health care agency on the East Coast of the US generated a dataset to connect human resources data with electronic health record data. This data was collected between 2010 and 2015 in the NYC Metro region and was provided for the study.
Ethics Approval
The study was approved by the Institutional Review Board of the study lead’s home institution (#IRB-FY2018-1562) along with the partner home health care agency (#796572-15) as part of a larger parent study examining inequities in 30-day readmission from home health care. Extensions were granted for the ethics approval during the COVID-19 pandemic which had slowed the analyses.
Data Sources and Searches
Administrative data and the Outcome Assessment Information Set (OASIS) were used in the study, with all subjects living in the New York City metro area. OASIS is a Medicare-mandated measure of patient health that is completed at the start and end of each patients’ home health care (HHC) episode. During the timeframe of the study, OASIS version C was used as the tracking set. OASIS dataset availability, and its ability to be merged with the home health care dataset provided at the appropriate timeline, led to the necessary use of our data from over 5 years ago. Prior to being attained by the university partner, the dataset was cleaned and deidentified, with the home health partner using encrypted data transfer to do so. After pandemic associated delays, analyses took place between August 2022 and May 2023. After being linked to the OASIS data, the administrative data included the required information to calculate the raw continuity of care score, which was created using the Bice-Boxerman index. Four commonly used measures of continuity of care (Bice-Boxerman, Herfindahl Index, Usual Provider of Care, Sequential Continuity Index) were highly correlated and it is recommended that the choice of indicator should be driven by practical and conceptual concerns. 9 We chose the Bice-Boxerman as it has been demonstrated to be associated with outcomes in Visiting Healthcare Personnel, 10 the equation for which is shown in Figure 1.
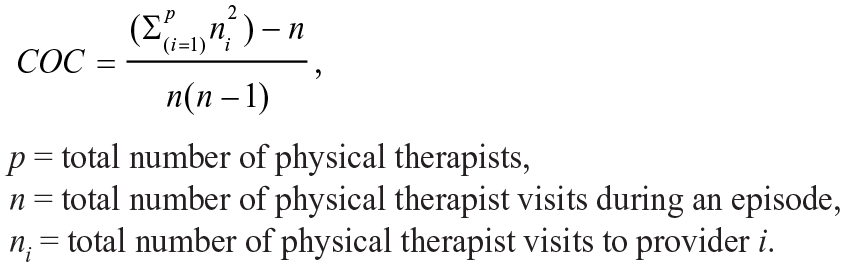
The Bice-Boxerman continuity of care index.
Study Selection
The following criteria was necessary for patient data to be included in the model. First, patients had to be admitted to their first home health care site following discharge between January 1st, 2010, and March 31st, 2015. The available data necessitated this criterion. Second, all patients with missing data (<2%) were excluded. “Missing” was defined as participants who did not record values for a variable of interest. Finally, self-reported “Female” and “Male” patients were included, with persons identifying as ‘U’ (n = 1) removed. ‘U’ patients did not have an adequate sample size for analysis. This also allowed gender to be analyzed as a binary variable.
Variables
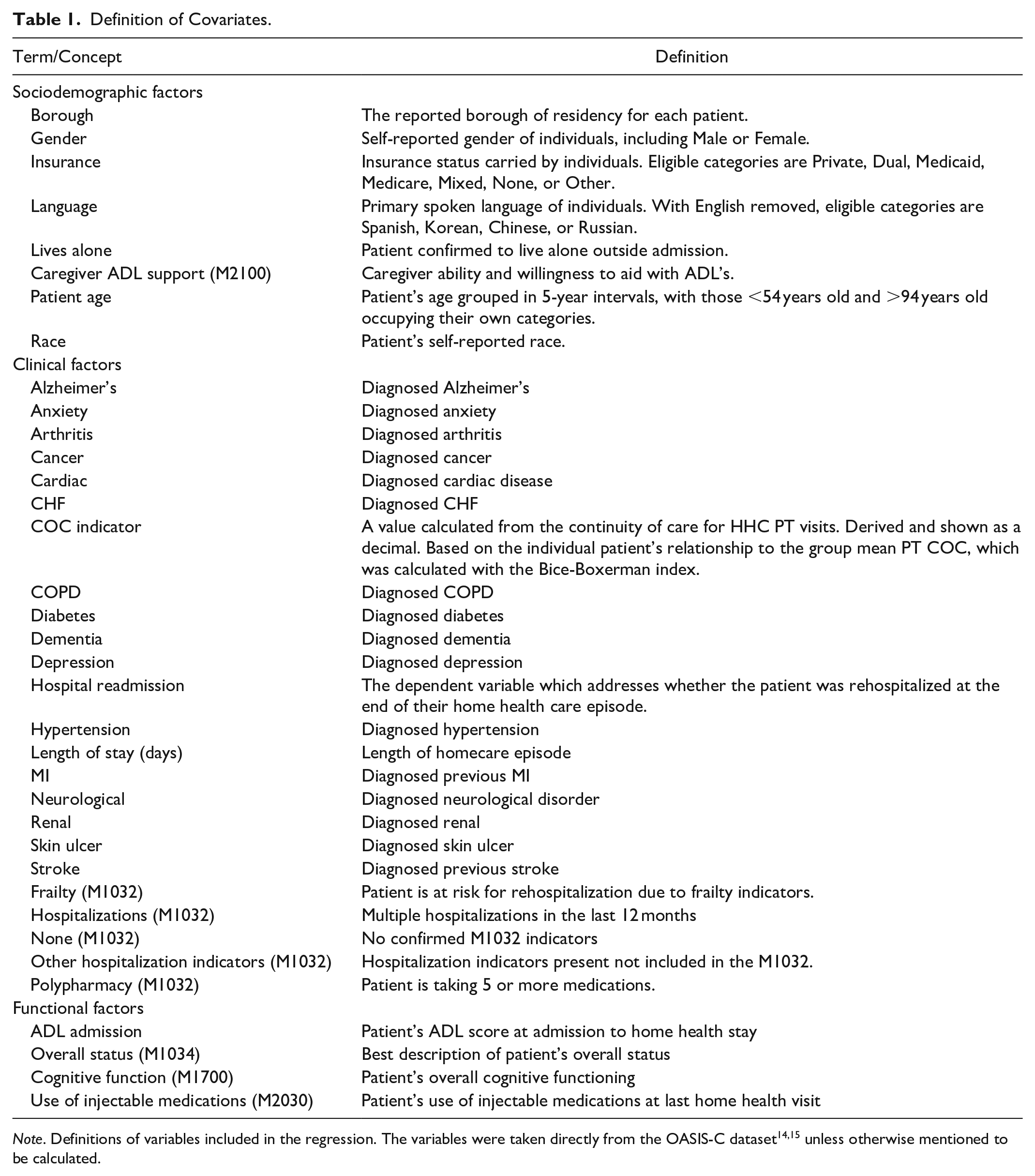
The final model included 36 variables, all of which are defined in Table 1. Further discussion of dependent variable and covariate adjustments follow below.
Definition of Covariates.
Hospital readmission: The OASIS-C dataset determined hospital readmission. The value defined the resolution of each patient’s home health care experience. There were 2 potential outcomes: Hospital readmission occurred, or the home health services ended without readmission.
Covariates: Multiple variables were modeled as factors to help avoid non-linear relationships between the independent and dependent variables. “ADL Admission” was grouped in quartiles to be modeled as a factor. “Length of stay days” underwent the same process. The age of patient’s was grouped under “Patient Age” with patients < 54 years old in a group, those >94 years old in a group, and all individuals between 54 and 94 years old grouped in 5-year intervals. All included variables were now able to be analyzed as categorical variables.
Data Extraction and Quality Assessment
Using R (version 4.1.2) for analysis, a multivariable logistic regression model with readmission acting as the dependent variable was created. The aim was to look at the influence of continuity of care in the model, while addressing sources of bias.
First, we addressed variables needing transformation. The variable of interest, “COC Indicator,” utilizes data from the existing variable: “PT Continuity of Care,” which was created using the Bice-Boxerman index. We aimed to group the “PT Continuity of Care” variable appropriately to indicate different levels of continuity. The first effort to do so, utilizing quartiles, was not usable because of the large number of patients with complete continuity of care (1.0). We then tried to use the median value, however the large amount of complete continuity resulted in a median of 1. We ultimately used the mean (0.81) to separate continuity of care into 2 groups, despite the known limitations of this method. This decision was made after consultation with Simon Jones, an expert in biostatistical modeling.
Following this, we looked to dismiss variables with a high level of multicollinearity. To begin this process, a starter logistic regression model with all potential variables (n = 39) was created. Using the preliminary model, the variance inflation factors (V.I.F.) was calculated using the vif command within the “car” package. 2 Variables with a V.I.F. >10 were to be removed, however all covariates met this criterion. ADL (M2100) and Cognitive (M1032) were removed due to redundancy with M2100 and M1032 factors, which are described in Table 1. Finally, diagnosed genitourinary disease was removed due to inadequate sample size (n = 3).
The included variables (n = 36) then had the appropriate reference set. For the variable of interest, “Low Continuity of Care” was set as the reference as we hypothesized that this was the most likely course to readmission.
Data Synthesis and Analysis
Interpretation was aided by the “margins” package, where the Average Marginal Effect for each variable was calculated. This allowed the analysis of how the dependent variable (rehospitalization) changed when an independent variable changed from group to group. This model reports the likelihood of rehospitalization for each group when compared to the reference categories. Negative values indicate a decreased hospitalization risk, while positive values indicate an increased hospitalization risk. The model fit was confirmed with Hosmer-Lemeshow plots, as shown in Figure 2.
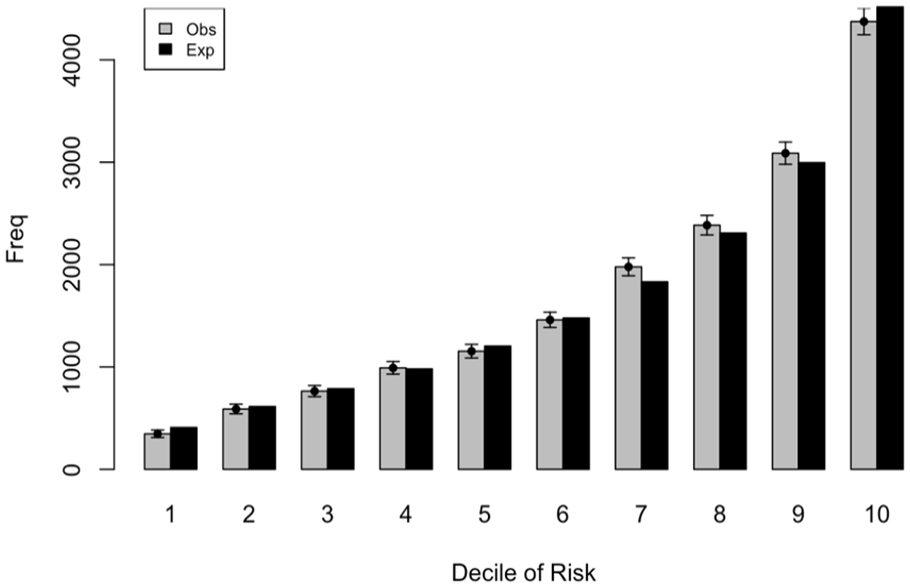
Hosmer-Lemeshow plot displaying model fit.
Results
The logistic regression model had a sample 90,220 with 36 covariates included. Of the included persons, 73,090 (81.0%) ended their home health time without a rehospitalization while 17,130 (19.0%) were rehospitalized. A summary of the study patients, along with results from the regression, is shown in Table 2.
Full Model.
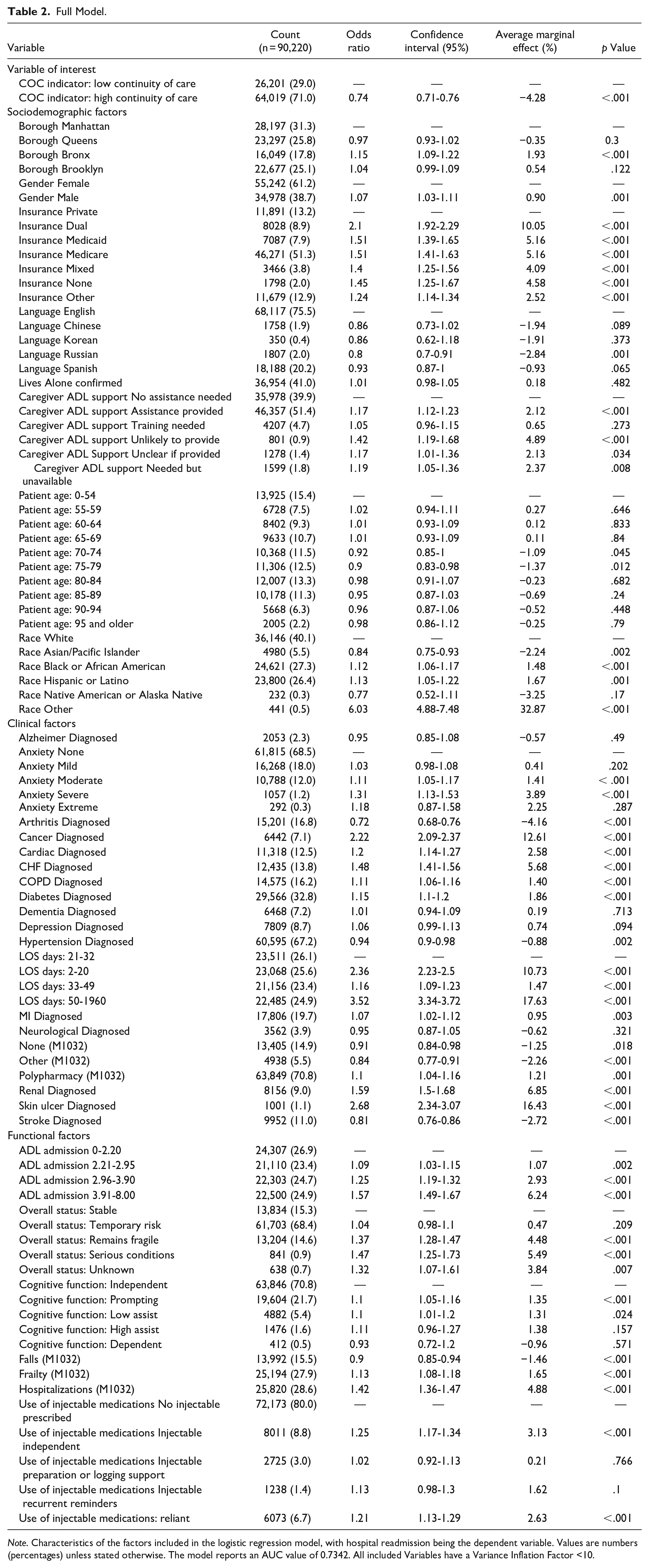
Note. Characteristics of the factors included in the logistic regression model, with hospital readmission being the dependent variable. Values are numbers (percentages) unless stated otherwise. The model reports an AUC value of 0.7342. All included Variables have a Variance Inflation Factor <10.
With low PT continuity of care as the reference and readmissions as the dependent variable, high PT continuity of care had a lower average marginal effect (OR = 0.74, 95% CI 0.71-0.76, p ≤ .001, AME = −4.28%), meaning that rehospitalization was less likely to occur when the patient received a high continuity of care.
Discussion
Hospital readmission was significantly less likely to occur when patients received a high continuity of care from physical therapy services. These findings align with the current literature that has linked higher interpersonal continuity of care in home-based physical therapy to lower odds of hospital readmission. 6 Of note, a larger odds ratio was found in the study by Russel et al 6 (OR = 2.06, 95% CI 1.90-2.23) when comparing above and below average continuity of care.
Continuity of care has been shown to be a promising characteristic to reduce hospital readmission, and promote greater patient satisfaction and functional outcomes across a variety of populations and settings.6,11 -13,16 -18 Higher levels of continuity of care have been consistently associated with reduced healthcare utilization and costs across medical, nursing, and physical therapy services.13,17,19 -22 Prior literature has pointed to the importance of sustained patient-clinician relationships in providing consistent communication, education, and plans of care. 23 It is possible that with multiple clinicians the differing plans and different assessments causes variance in knowledge of what the patient should be capable of, or what their baseline is. As such, the lack of continuity may make decline more difficult to recognize and hospitalization more likely. Although the current study indicates the importance of a consistent relationship in home-based physical therapy, future research may consider examining the strength of such relationships as a predictive factor via measures of therapeutic alliance, communication, and/or trust.
Limitations
Limitations from the current study involve generalizability and the study design. This study analyzed a large dataset of patients from an urban area, receiving home-based physical therapy from a single homecare agency. It is unclear whether the same results would present with alternate homecare agencies or would be generalizable to suburban or rural areas. Additionally, by separating continuity of care by the mean, the analysis is open to strong bias from skewed data. Also, the lack of data available on the total number of PT visits does not allow the analysis to weigh the value of short episodes of PT versus those with a larger frequency of episodes. Next, the 30- and 60-day rehospitalization rates were not calculable given the data available, which would have been useful as a key clinical and administrative rate. Furthermore, the role of resumptions of care, and its potential negative impact on continuity of care, cannot be considered as we do not have data available for type of hospitalization. Lastly, our variables are weakly associated with continuity of care (Table 3), but endogeneity and confounders may distort our result.
Bivariate Correlation Table.
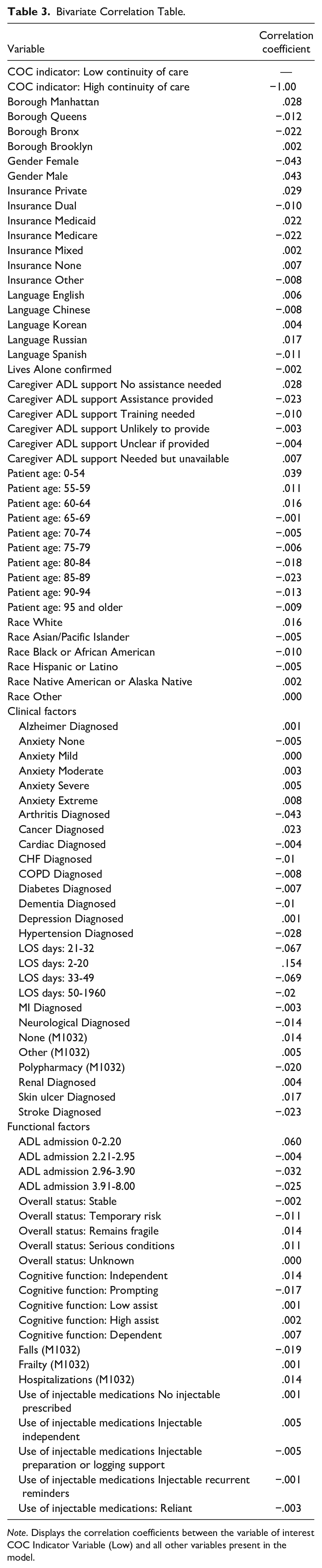
Note. Displays the correlation coefficients between the variable of interest COC Indicator Variable (Low) and all other variables present in the model.
Suggestions for Home-Based Physical Therapy
There are no known policies in homecare that incentivize higher levels of interpersonal continuity of care, despite the ubiquitous benefits on outcomes and costs.6,11 -13,16 -22 This is the second study to indicate the criticality of continuity of care for the prevention of hospital readmissions using a large home-based physical therapy dataset. Unfortunately, staffing, and logistical complications could make an emphasis on continuity of care challenging. Additionally, different forms of insurance available to patients could greatly influence the level of physical therapist continuity available due to what is and what is not covered—because of this, the role of financial feasibility serves as a major barrier. Currently for home-based physical therapy, Medicare reimbursement is based on a prospective payment system, the Patient-Driven Groupings Model. 24 In this system, patients are provided 30-day periods of care and reimbursement is based on case-mix groups involving admission source and timing, clinical grouping from primary diagnosis, functional impairment level, and adjustments for secondary comorbidities. 24 This reimbursement model primarily considers the patient’s individual health and functional status; however, there is minimal to no emphasis on the characteristics or performance of the homecare agency. We suggest creating reimbursement incentives for agencies that can deliver high interpersonal continuity of care because it has a strong potential to reduce hospital readmissions and could incentivize agencies to overcome the logistical issues that come with emphasizing interpersonal continuity of care.
Conclusion
The current study identified higher levels of interpersonal continuity of care in home-based physical therapy as a significant factor to reduce risk of hospital readmissions. This study affirms interpersonal continuity of care as a critical characteristic in home-based physical therapy.
Practical Implications
An emphasis should be made in home health care for physical therapist continuity of care to reduce negative outcomes such as hospital readmissions. This may require home health care agencies to invest in retention efforts of physical therapists to ensure continuity of care and reduce the use of per-diem personnel.
Footnotes
Author Contributions
Patrick Engel wrote the paper and performed the analysis. Mark Vorensky wrote the paper. Allison Squires contributed data or analysis tools and wrote the paper. Simon Jones concieved and designed the analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Agency for Healthcare Research and Quality (R01#HS023593). Dr. Vorensky’s effort is supported by the University of Michigan HEAL National K12 Clinical Pain Career Development Award, K12NS130673.