
Abstract
The present study aimed to identify the structure of advance care planning (ACP) practices implemented by home health nurses (HHNs) for multigenerational families with dependent children and terminally ill grandparents. Interviews of 20 HHNs were conducted. The grounded theory approach was used to describe the interactions among families with dependent children, terminally ill grandparents, and HHNs. The results showed that the structure of ACP practices for multigenerational families with dependent children and terminally ill grandparents was composed of 2 levels. First, HHNs were providing the underlying foundational “Practice of supporting end-of-life care (EOL care) at home” for family members from 2 generations: sandwich generation caregivers (SGCs) and terminally ill grandparents. Second, they were providing “Practices that connect multiple generations,” “Practices that address the children,” and “Practices that involve hands-on experience and communication” for multigenerational families with dependent children and terminally ill grandparents. Practices based on providing stability among family members from 2 generations, SGCs and terminally ill grandparents, were the nursing practice structure that activated ACP for multigenerational families with dependent children and terminally ill grandparents.
Keywords
Introduction
In the next half century, population aging is expected to advance rapidly around the world, 1 and ahead of the world, Japan is about to enter the next phase characterized by a high prevalence of deaths, referred to as a Society with Numerous Deaths. 2 In response to this, advance care planning (ACP), involving sustained and spontaneous ongoing dialogue among patients, their families, and healthcare providers to discuss how patients can spend the end-of-life phase in a manner true to themselves, is being recommended, 3 along with improving home medical care during the end-of-life (EOL) phase (hereafter referred to as EOL care). 4 However, EOL care is left to medical institutions these days, and with the decline in 3-generation households and education that views death as a taboo topic,5,6 individuals aged between their 30s and 50s become parents and then caregivers for their own parents without having had an opportunity to experience death up close. In the United States (US), one in 4 people are sandwich generation caregivers (SGCs), who are adults involved in caregiving while also parenting their children. 7 In Japan, 83.5% of caregivers aged between their 30s and 50s are also in the child-rearing stage, 8 and many parents are worried about how to talk to their children about their terminally ill grandparents. 9
The death of a close member of the family has the potential of profoundly affecting a child, leading to lifelong consequences. When the process of how to live the EOL phase is not openly discussed within the entire family, it has been suggested that it may contribute to prolonged grief, depression, and trigger self-injurious behaviors in children. 10 Therefore, support for ACP from a whole family perspective is important, since terminally ill grandparents affect not only the parents’ generation caregivers, but also the parents’ children, in other words, the generation of the grandchildren.
ACP practice requires ongoing conversations and decision-making support. 11 In this context, nurses play crucial roles as information providers, educators, and facilitators. 12 In home EOL care, there has been an increasing number of studies in recent years that have focused on ACP practice provided by home health nurses (HHNs) targeting patients and caregivers.13,14 However, very few studies have focused on nursing practices from the perspective of patients and their entire families. With the anticipated increase in the number of SGCs aged between their 30s and 50s, 15 the need for support that allows the entire family to continue discussing openly how to spend the EOL phase has been suggested.16,17
The present study aimed to identify the structure of ACP practices implemented by HHNs for multigenerational families with dependent children and terminally ill grandparents.
Definitions of Terminology
Advance Care Planning
ACP is a process through which medical professionals, family members, and patients of any age or stage of health can understand and share values, life goals, and preferences regarding future medical care. 3 In the present study, ACP was defined as the process that involved sustained and spontaneous ongoing dialogue among HHNs, families with dependent children, and terminally ill grandparents in their EOL phase for about a month before their death.
Families With Dependent Children
In Japan, Western countries, and the European Union (EU), families with dependent children refers to households with students under the age of 19 or under the age of 24 years.18 -20 Since approximately 80% or more of 9-year-olds understand death, 21 the present study defined “families with dependent children” as households with children between the ages of 9 and 22 years.
Sandwich Generation Caregivers
SGCs are individuals in the generation caught between caring for their children in the child-rearing stage and their aged parents who require nursing care. 15 The present study defined SGCs as individuals in the generation who are caring for terminally ill grandparents while also raising children aged between 9 and 22 years.
Child or Children
In the present study, the child or children referred to in the present study were the offspring of SGCs and simultaneously the grandchild or grandchildren of terminally ill grandparents.
Methods
Sample
The inclusion criteria for participants were: (i) 5 or more years of experience as an HHN, (ii) experience in providing EOL care, and (iii) an individual practicing ACP for families with dependent children and terminally ill grandparents.
Requests to participate in the study were sent by mail to 106 home nursing stations in the nationwide Welfare and Medical Network System in Japan that practice ACP with additional terminal care services, providing 24-hour support for EOL care in the home. The snowball sampling method was used.
Data Collection
Interviews were conducted by the author between January 2022 and January 2024. The interviews were conducted either in person or online, with each interview lasting an average of 86 ± 12 minutes. The interviews were recorded and transcribed into transcripts. When creating the transcripts, all personally identifiable information was anonymized by the primary author using letters.
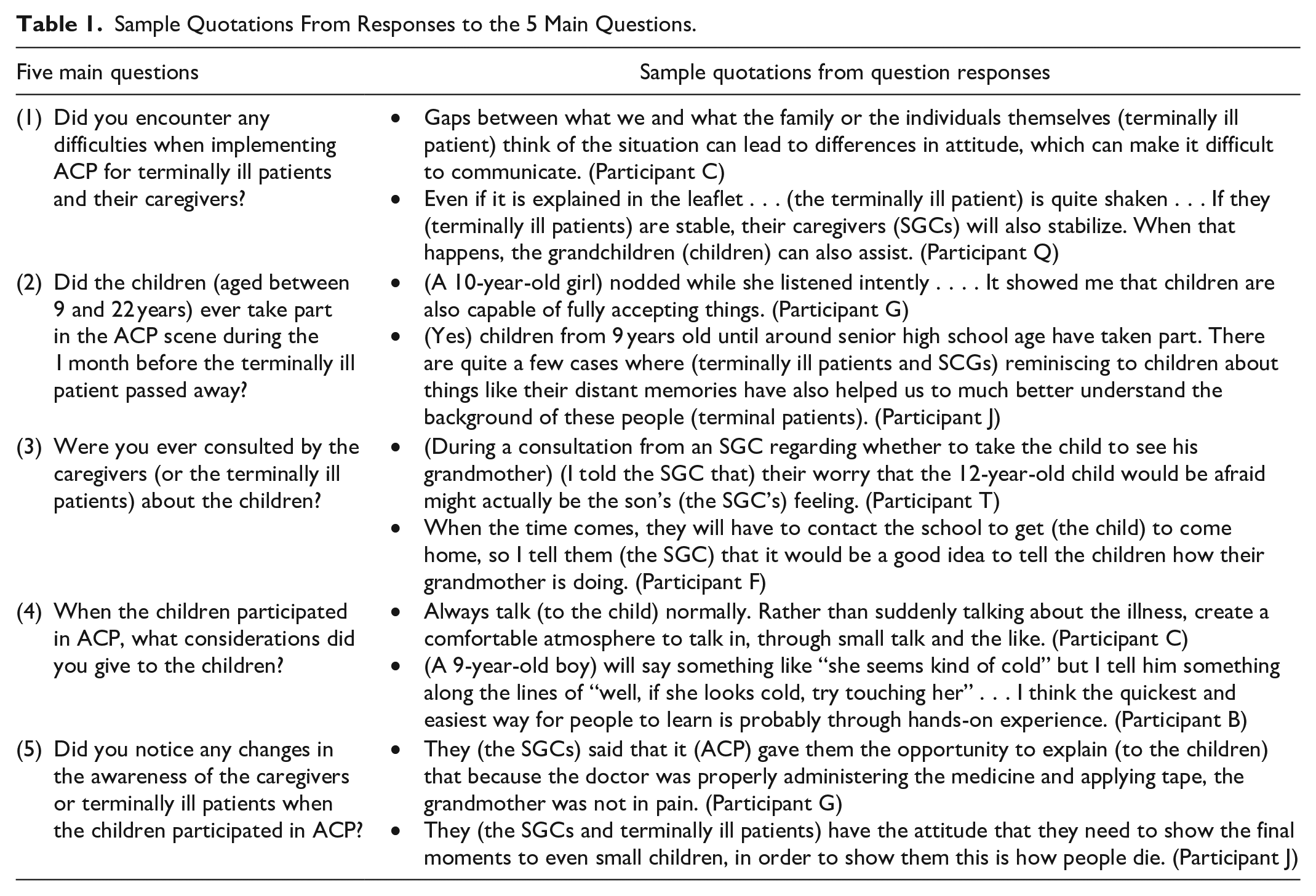
To standardize data collection, an interview guide was used. In the semi-structured interviews, an interview guide that consisted of open-ended questions related to ACP practice for families with dependent children and terminally ill patients was used. The interviewer posed 5 main questions: (1) Did you encounter any difficulties when implementing ACP for terminally ill patients and their caregivers?; (2) Did the children (aged between 9 and 22 years) ever take part in the ACP scene during the 1 month before the terminally ill patient passed away?; (3) Were you ever consulted by the caregivers (or the terminally ill patients) about the children?; (4) When the children participated in ACP, what considerations did you give to the children?; and (5) Did you notice any changes in the awareness of the caregivers or terminally ill patients when the children participated in ACP?
Aided by the iterative process of the grounded theory approach, interview questions became more specific and precise as the data analysis progressed.
Ethical Considerations
Approval to conduct the study was obtained from the Ethics Review Board Osaka University Hospital (No. 21241). All participants provided written, informed consent to participate in the study before interviews were conducted. Access to the demographic information linking each participant to the anonymized transcripts was restricted to the primary author. Recorded interview audio data were stored by the primary author in a locker in the university research laboratory.
Data Analysis
Analysis was conducted using the constant comparative method of the grounded theory approach. 22 The grounded theory approach focuses on the process of interaction with people, and we thought it could be conceptualized for HHNs practice to support ACP interaction between families with dependent children and terminal patients. Consistent with grounded theory procedures, the first author began fragmenting the data from the first interview using open-coding strategies. Subsequently, each interview was coded and compared to the data in previous interviews in an iterative process. As the study progressed, data were categorized into axial codes. During the selective coding process, one core category and 3 themes emerged relating the axial categories to each other. These categories were grouped by theoretical links to provide direction for future data analysis. As the analysis progressed, the knowledge and skills of HHNs were compared for each interview participant to identify the practice structure of HHNs. These abstractions, analyses, and interpretations were reviewed several times by experienced qualitative researchers, and the results of the analyses were subjected to 5-member checking to ensure the validity and truthfulness of the analyses.
Results
Participants
Twenty HHNs participated in the interviews. The mean age of the participants was 47.3 years. The mean number of years of experience as an HHNs was 11.7 years, and the mean number of years of experience working at institutions such as hospitals and facilities was 11.6 years. The numbers of ACP and EOL care cases previously implemented per participant were 10 to 50 (5 participants), 50 to 99 (1 participant), and ≥100 (14 participants). Two participants had experience working on a palliative care ward, whereas 8 participants were certified by the Japanese Nursing Association as either Certified Nurse Specialists (gerontological nursing, 1 participant) or Certified Nurses (palliative care, 1 participant; visiting nursing, 6 participants).
Practice Structure
Sample quotations from responses to the 5 main questions are shown in Table 1.
Sample Quotations From Responses to the 5 Main Questions.
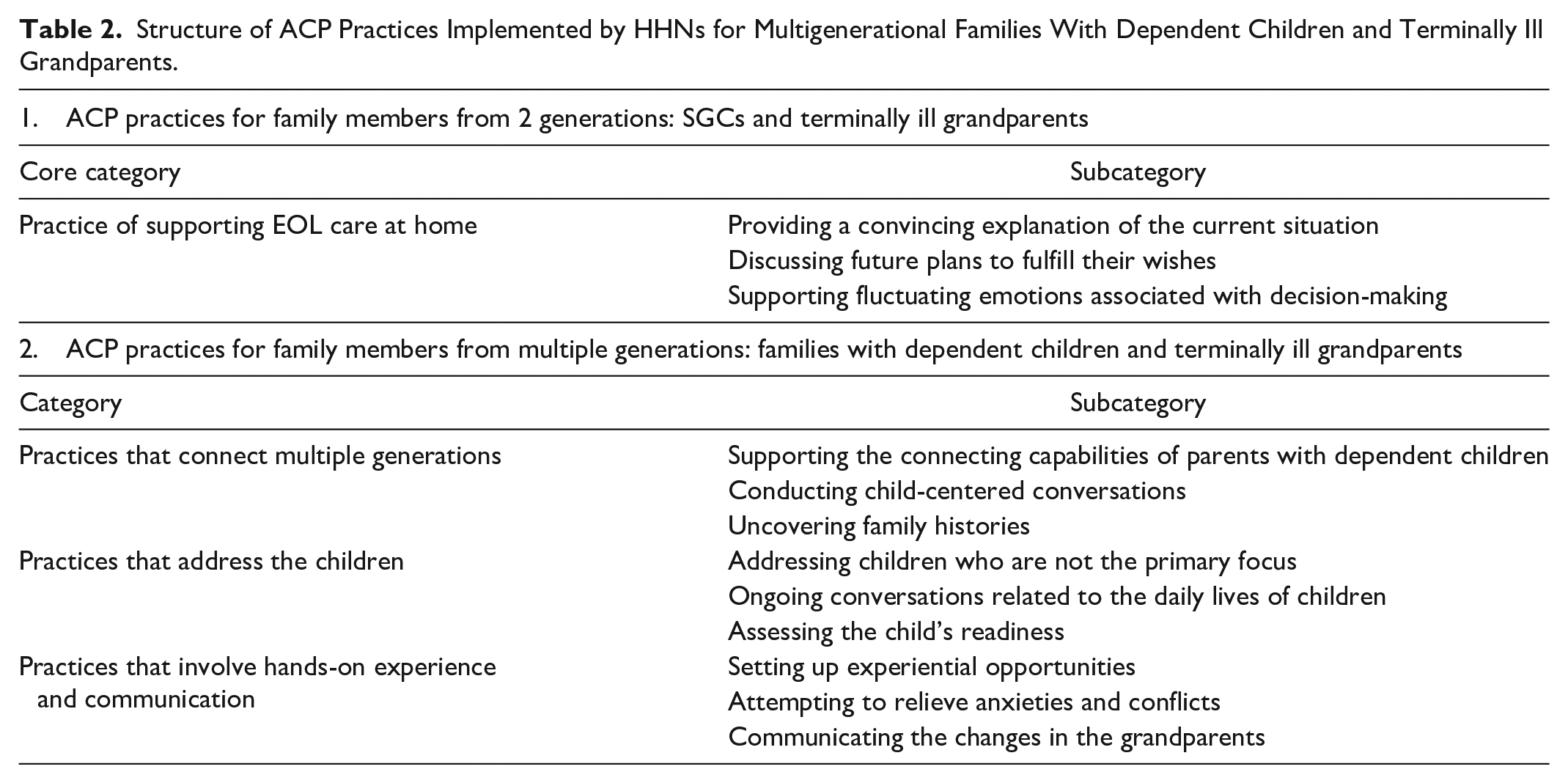
Analysis of these data showed that the structure of ACP practices for multigenerational families with dependent children and terminally ill grandparents was composed of 2 levels. Initially, one core category and 3 subcategories were extracted as the underlying foundational practice from the practices targeting 2 generations: the SGCs and the terminally ill grandparents. Subsequently, 3 categories and 9 subcategories of practices were extracted from the practice targeting multigenerational families with dependent children and terminally ill grandparents (Table 2). The details are described below.
1. ACP practices for family members from 2 generations: SGCs and terminally ill grandparents
Practice of supporting EOL care at home
One “core category” was extracted as an underlying foundational practice. First, the HHNs provided convincing explanations of the current situation to the confused SGCs and terminally ill grandparents. Furthermore, by offering support for the fluctuating emotions associated with decision-making, they provided emotional stability for SGCs and the terminally ill grandparents through “Practice of supporting EOL care at home.” (Regarding ACP practices involving children) The medical condition and current situation were (in disarray and) unclear, making it difficult for even the eldest son and his wife to understand. Also, from her own perspective, she (the terminally ill grandmother) was in no condition to clearly explain her condition to her grandchild . . . (Participant O) When the parents’ generation is convinced (about the medical condition of the grandparents), I think it makes a difference in how it is communicated to the grandchildren’s generation. I believe that the parents’ generation being convinced is quite important (I provide explanations with this in mind) (Participant U) In the case of families experiencing fluctuating feelings (regarding decision-making), it was explained to them each time (Participant S)
Structure of ACP Practices Implemented by HHNs for Multigenerational Families With Dependent Children and Terminally Ill Grandparents.
2. ACP practices for family members from multiple generations: families with dependent children and terminally ill grandparents
Next, the following 3 “categories” were extracted. (1) “Practices that connect multiple generations” for families with dependent children and terminally ill grandparents, children-centered, (2) “Practices that address the children,” and (3) “Practices that involve hands-on experience and communication” were conducted.
(1) “Practices that connect multiple generations”
When SGCs were contemplating whether to allow their children to meet their terminally ill grandparents, HHNs assisted SGCs who were trying to connect the terminally ill grandparents with their children. The HHNs were also implementing “Practices that connect multiple generations,” a factor of ACP involving multiple generations, by engaging in conversations centered around the children.
(Regarding a consultation received from an SGC wondering whether a 15-year-old junior high school boy should be taken to see his grandmother, whose appearance has changed) The child has watched the parents interact (with the grandmother) . . . I asked (the parents) to bring along the child as much as possible (to the grandmother’s house). Then, gradually (the child) began to approach (the grandmother). (Participant H) (Regarding the time a 16-year-old senior high school boy came to see his terminally ill grandmother) I also used prompts such as ‘So, as a grandchild, what kind of grandmother was she?’ . . . connecting it to ACP, to further expand the personality of the person concerned. (Participant S)
(2) “Practices that address the children”
In “Practices that address the children,” the HHNs engaged with the children, who are never the primary focus in caregiving situations and built a trusting relationship through ongoing conversations related to the children’s daily lives. The HHNs also assessed the readiness of the children and whether they were emotionally prepared to participate in ACP.
(Regarding initiating conversations with 9- to 12-year-old children on their return home from school) I try as much as possible to encourage (the child) to join the conversation by asking things like ‘What happened at school today?’ while attending to (the patient). (Participant I) (Regarding observations of a 9-year-old elementary school boy participating in ACP) Through daily observations of (the child), (I) could tell. I believe (the child) was there in a state of readiness, prepared to learn. (Participant S)
(3) “Practices that involve hands-on experience and communication”
Lastly, “Practices that involve hands-on experience and communication” is about practices where HHNs set up opportunities for children to receive care experiences. HHNs noticed how the children perceived the changes in their terminally ill grandparents and did not miss the opportunity to involve the children. They implemented practices to relieve the children’s anxieties and conflicts through hands-on caregiving experiences and conversations.
(Regarding responding to a 20-year-old university school girl who was confused because her grandmother would not wake up) When (a child) mentions something like ‘Grandma won’t wake up’, a nurse could say ‘She will wake up if you call her like this’ and provide an example (Participant S) (Regarding a case where an 11-year-old elementary school boy who was uncomfortable with the physical changes in his grandmother helped the home health nurse give a bed bath) While (giving a bed bath), the changes of (the grandparent) were explained gradually, one by one, to (the boy) . . . we were very happy to hear that that (the bed bath) became an opportunity for (the parents and the child) to talk. (Participant I)
Discussion
The present study aimed to identify the structure of ACP practices implemented by HHNs for multigenerational families with dependent children and terminally ill grandparents. The present study identified 4 practices implemented by HHNs.
First, it was shown that practices that maintain emotional stability in both generations, the SGCs and the terminally ill patients, are essential for the viability of ACP in multigenerational families with dependent children and terminally ill grandparents. Approximately 50% of terminally ill patients are reported to suffer from depression and anxiety. 23 Caregivers themselves are handling caregiving while experiencing emotional instability of fear and grief associated with losing a parent.24,25 Reports suggest that the emotional instability of caregivers, in particular, can result in their offspring’s generation not being identified as persons in need of assistance. 26 The present study also found that, when SGCs are confused, it is extremely difficult for parents to explain the situation to their children. Therefore, the “Practice of supporting EOL care at home” that supports the mental health needs of the SGCs and the terminally ill grandparents is the underlying foundational practice of ACP for families with dependent children and terminally ill grandparents.
Second, practices that recognize SGCs as key players in ACP involving multiple generations were identified. SGCs are often referred to as the middle generation, recognized for their important role in connecting and ensuring a smooth relationship between children and their grandparents. 27 Recent studies have shown that openly discussing death with children by the parents increases the children’s acceptance of the death of a close relative, thereby leading to reducing grief.28,29 As noted above, SGCs play a crucial role in connecting multiple generations and maintaining the emotional stability of the children. In situations where SGCs consulted HHNs, practices that support how SGCs should relate to their children as parents were observed. The background of this practice, which evolved into an opportunity to stimulate multigenerational conversations, stems from HHNs focusing their attention on SGCs who are caregivers, as well as being part of the child-rearing generation. “Practices that connect multiple generations” are practices that recognize the role of SGCs in bridging children with their grandparents, as well as their role as parents to their own children.
Third, although children are not the primary focus in caregiving situations, a practice that involved them recognizing that they are significant members of the family was identified. There is a growing worldwide trend to recognize the right of children to participate in matters that affect them. 30 In ACP, children are also said to have the right to participate and contribute to the family decision-making processes. 31 However, despite half a century having passed since children’s rights were brought to light, very few specific practices have been suggested. When children participate in their family’s ACP, it can have various effects, such as reducing grief and improving self-efficacy.16,32 However, it is said that opportunities for children participating in ACP are influenced by the attitudes of parents or healthcare providers.33 -35 In the present study, HHNs were able to assess the children’s emotional readiness to participate in ACP by continuously addressing and communicating with the children, who are members of the family. Thus, “Practices that address the children” refers to the involvement of HHNs with an awareness of the best interests and rights of the children.
Last, it is a practice that addresses what the child wants to discuss and finds ways to help the child understand. Though it is believed that proper explanations from healthcare providers can influence the emotional stability of children, identifying a suitable method of explanation considering the child’s developmental stage has been a challenge. 36 In the present study, HHNs responded to confusion regarding grandparents’ physical changes by sharing information regarding their medical condition through hands-on caregiving experience and conversation with children of any age. The American Academy of Pediatrics (AAP) suggests that, when discussing death with children, engaging in activities such as drawing together during the conversation can be an effective technique for children to express their emotions. 10 It can be said this supports “Practices that involve hands-on experience and communication” by helping to bring out the children’s feelings and subsequently activating ACP between families with dependent children and the grandparents.
Limitations
The HHNs participating in the present study constituted a group with a relatively high number of years of experience (mean 11.6 years) working at institutions such as hospitals and facilities, in addition to the number of ACP cases handled. Further studies are needed to investigate the relationship between clinical experience and the number of practical years of experience as an HHN. Moreover, more than half of the children who were the subjects of the practice of the HHNs were cohabiting with their grandparents. Those children who were not living with their grandparents also had a relatively close relationship with them. In the future, more research is needed to examine the factors of patient and family backgrounds that influence the practice, including the perspective of families in the child-rearing stage. In the present study, which encompassed children aged 9 to 22 years, one common practice was identified. Further study comprising interview surveys focusing on developmental age is important to potentially identify novel practices.
However, the fact that it was possible to demonstrate in this study how ACP has been implemented by HHNs for multigenerational families with dependent children and terminally ill grandparents is a novel finding.
Conclusion
Interviews were conducted with 20 HHNs working across Japan, aiming to identify the structure of ACP practices implemented by HHNs for multigenerational families with dependent children and terminally ill grandparents. Three subcategories for one core category and 9 subcategories for 3 categories were identified. Given the increasing prevalence of SGCs in the future, we hope that this will facilitate multigenerational ACP practices. When implementing ACP for families with dependent children and terminally ill grandparents, maintaining the emotional stability of both SGCs and terminally ill grandparents is of primary importance. Once this is achieved, ACP should then support SGCs as connectors among multiple generations, give attention to the children, and provide opportunities for children to experience caregiving. Given the anticipated increase in prevalence of SGCs in the future, we hope the present findings will help facilitate multigenerational ACP practices.
Footnotes
Acknowledgements
The authors are grateful to the study participants.
Author Contributions
All authors (1) made substantial contributions to the study concept or the data analysis or interpretation; (2) drafted the manuscript or revised it critically for important intellectual content; (3) approved the final version of the manuscript to be published; and (4) agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Yuumi Memorial Foundation for Home Health Care.