
Abstract
After hospitalizations, many older adults experience a rapid functional decline and rely on home health (HH) care services to regain physical function. Understanding rehabilitation treatment elements that improve physical function is important for optimizing care. Two randomized controlled trials demonstrated similar physical function improvement in older adults (≥65 years, ≥3 comorbidities) receiving either high intensity (n=133) or standardized usual care (n=140) HH approaches in the 60 days following hospitalization. This secondary analysis examined the relationship between patient characteristics, treatment elements, and physical function improvements measured by the Short Physical Performance Battery (SPPB). In the high intensity group, lower baseline SPPB performance was associated with greater improvements (β=-0.23, p<0.01). Completing an additional exercise component per session further increased SPPB scores by 0.65-points (β = 3.94, p<0.01). For every two visits completed, there was an associated with a 0.58-point increase in SPPB (β=0.29, p<0.01), exceeding the small meaningful changes threshold (0.5 points). In contrast, four visits in usual care were associated with a 0.56-point change in SPPB (β=0.14, p<0.05). Neither approach demonstrated an association between environmental challenge exercises and functional improvement, potentially due to lower session frequency and shorter duration. These findings suggest that consistent attendance and full participation in high intensity HH components are critical for maximizing recovery. HH therapists should educate patients to prioritize attending 12 sessions and completing all prescribed treatment components to optimize physical function recovery in the 60 days after hospitalization.[AQ3]
Keywords
Introduction
An estimated 67% of older adults in the United States experience two or more concurrent chronic conditions (multimorbidity), such as cardiovascular disease, arthritis, or lung disease. 1 Thus, when older adults are hospitalized due to an acute event, they often experience a rapid functional decline,2 -4 which elevates their risk of institutionalization and mortality.2,5 The consequences are severe, with as many as 46% of older adults experiencing a decline in activities of daily living after hospital discharge. 6 To recover, many older adults require home health (HH) rehabilitation services to improve functional deficits.7,8 However, there is little evidence describing optimal HH rehabilitation interventions post hospitalization. 9
Rehabilitation interventions are complex; the patient, clinician, environment, and delivery of the intervention all influence outcomes. 10 Traditionally, interventions provided by physical therapists are described by mode, for example, strength or balance training; however, response to interventions vary based on exercise intensity and frequency. To optimize interventions, these elements are best understood through treatment fidelity, which is the degree that the treatment was delivered as intended.11,12 To explore treatment elements associated with improvements in physical function, we focused on fidelity dimensions—adherence and dosage, described by An et al. 13 Examining interventions through these dimensions can define dosage parameters, session frequency, and other elements essential to the intervention. 13 For instance, a physical therapy intervention consisting of high intensity leg strengthening and balance training at home, 3 times a week over 2 weeks can include many interacting elements: dosage (high intensity), session components (strength or balance exercises), frequency of sessions, and home environmental factors. Examining how these elements impact physical function can help clinicians prioritize, prescribe, and deliver a precise and effective treatment plan.
Two recent pragmatic, randomized controlled trials evaluated the effectiveness of a progressive high intensity exercise in comparison to a standardized usual care approach in older adults receiving HH care.14,15 The groups in both trials improved similarly in physical function after 60 days from hospital discharge. However, specific rehabilitation elements contributing to these improvements were unclear. We performed a secondary analysis from these trials to determine the relationships between improvements in physical function with patient characteristics and treatment elements from a high intensity and a usual care approach in a large sample of older adults after discharge from a hospital or skilled nursing facility over a 60-day episode of HH care.
Methods
Study Design
This is a secondary analysis using data from 2 separate randomized controlled trials (ClinicalTrials.gov Identifiers: NCT02905370, NCT02696382) examining the effect of HH physical therapy (PT) on function in older adults discharged home after a qualifying hospitalization. In both trials, participants were randomized to receive a progressive high intensity intervention or to the control- a standardized “usual care” intervention.14,15 Participants receiving high intensity intervention in the 2 trials were collapsed into 1 group as were the participants receiving usual care in the 2 trials.
Selection and Description of Participants
The trials recruited and randomized participants in metro Denver, Colorado, USA, from April 15, 2016, to December 4, 2021. All eligible participants were adults aged 55 years and older with at least 3 comorbid conditions who were referred for HH PT with deconditioning due to an acute hospitalization.16,17 Participants referred by their provider (N = 10), who were comparably deconditioned due to COVID-19 stay-at-home orders, were included beginning August 10, 2020. Exclusion criteria included very low or very high function at baseline (inability to walk 10 feet without human assistance or a gait speed greater than 1.0 m/s), contraindications to high intensity resistance training, 17 acute lower extremity fracture with weight-bearing restriction, recent joint replacement, active treatment for cancer, current dialysis treatment, acute cardiac disease, acute stroke, lower extremity amputation, severe cognitive impairment indicating inability to provide informed consent, hospice care referral, or significant medical complication that precluded safe participation in PT. Participants were included in the secondary analyses if they had a short physical performance battery (SPPB) assessment at baseline (within 72 hours of hospital discharge) and 60-days after hospital discharge. The parent trials were approved by the Colorado Multiple Institutional Review Board, and informed consent was obtained from all participants (COMIRB 15-2125, COMIRB 15-1571).
Progressive High Intensity
The high intensity program was a progression-based physical therapy program based on our prior research.18,19 High intensity visits aimed to achieve progressive overload and consisted of 6 possible components, which included 3 strengthening exercises (leg press, hip extension, plantarflexion), 2 gait training activities (stepping, obstacle navigation), and 1 functional training activity (bed mobility or progressive transfer training). Strengthening exercises were dosed to an intensity of an 8-repetition maximum (8RM) for 3 sets of 8 repetitions to promote progressive muscular overload. 20 resistance bands were changed on the leg press to achieve an intensity of 8RM tailored to each patient. The gait training component included stepping and walking activities that progressed in complexity, speed, and accuracy ensuring an 80% success rate for adequate challenge. The functional training component involved bed mobility, sit-to-stand, and floor-to-stand training. Progression of functional training occurred by making the task or environment more difficult. 17
Standardized Usual Care
Usual care PT visits consisted of 4 possible components, which included active range of motion exercises (seated marching, knee extensions, hip adduction, heel and toe raises; standing hip extension, marching, mini-squats, shoulder flexion; and supine single leg raises and bridging), balance (standing weight shifts, single leg stance), gait training (ambulation inside or outside of the home with or without an assistive device), and functional training (bed mobility, sit-to-stand transfer, or bathroom transfers). Active range of motion exercises were performed without weights for 1 set of 10 repetitions and increased up to 7 exercises per patient tolerance. Balance exercises could be performed with upper-extremity support as needed to maintain safety. Gait training emphasized safety and was tailored to each patient’s functional level; ambulation was performed inside or outside the home, with or without an assistive device. The functional training component included bed mobility, sit-to-stand transfers, and bathroom transfers with an emphasis on safety.
Delivery of Interventions
Participants in both trials were prescribed 12 PT visits. Trial NCT02696382 prescribed 3 visits/week over 30 days, and Trial NCT02905370 was 2 visits/week during the first 30 days followed by 4 visits/week over the next 30 days. Physical therapists delivering high intensity and usual care interventions were trained to ensure delivery of standardized care. The details of interventions and standardization of groups are detailed in the protocol paper and respective manuscripts.14,15,21
Data Collection and Measurements
All measures were collected by research-trained outcomes assessors, who were blinded to intervention assignments. Measures determined at baseline occurred within 72 hours of hospital discharge. Measures collected at the study end point occurred 60 days after baseline assessments. This end point was chosen as it represented the end of Medicare-defined episode of care at the time of the parent trials.
Sociodemographic measures (Table 1) were collected at baseline. The functional comorbidity index (FCI) assesses the presence or absence of 18 comorbidities related to physical function, with higher scores representing a greater number of comorbidities.22,23 The Saint Louis University Mental Status (SLUMS) examination detects mild cognitive impairment and dementia and ranges from 1 to 30 points; 24 normal scores range from 27 to 30 points.
Demographic and Clinical Characteristics.

The primary study outcome used for this analysis was the Short Physical Performance Battery (SPPB), a global measure of lower extremity physical function consisting of walking speed, chair stands, and balance. This composite measure is a strong predictor of disability, institutionalization, and morbidity in older adults.21,22 Scores range from 0 to 12 with higher scores indicating better performance. A 0.5 point change in SPPB is considered a small meaningful effect. 25
Fidelity Dimensions
Fidelity dimensions explored in this study focused on adherence and dosage (Table 2). 13 Adherence measures the adequate delivery of the key components of an intervention. Dosage describes the amount of a specific intervention delivered. We identified treatment elements within these dimensions to determine the relationships with improvements in physical function.
Fidelity Dimensions and Treatment Elements.
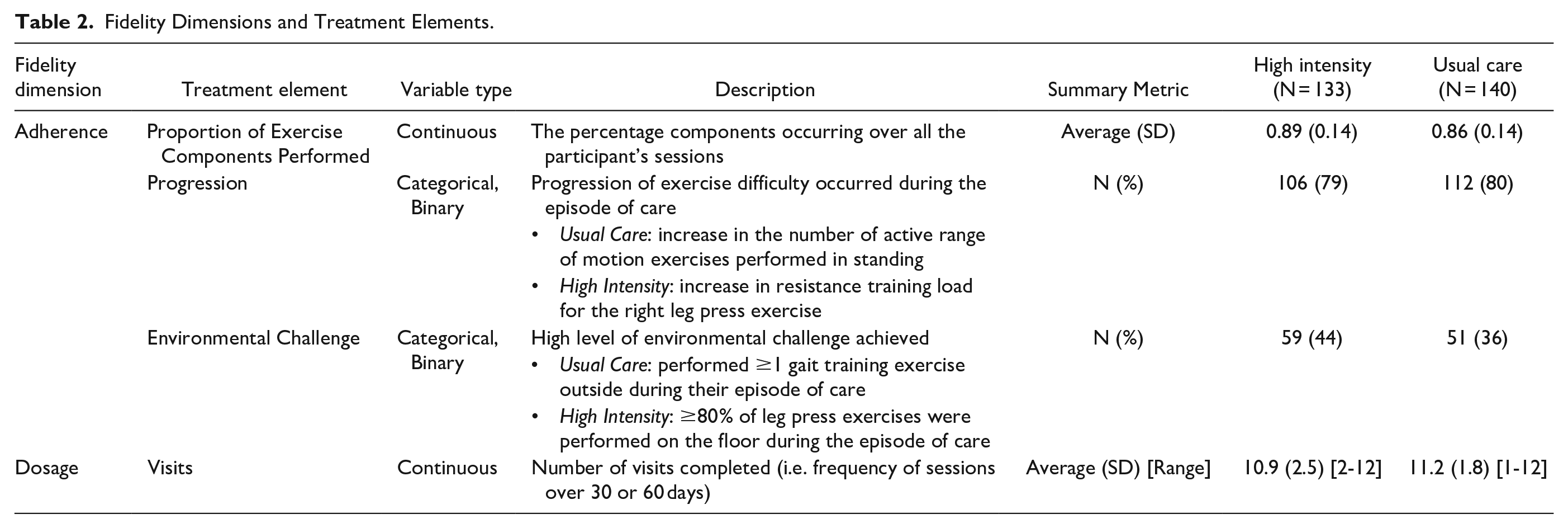
The intervention protocol included performing all components of the treatment, progressing the patients on a regular schedule, and attempting to achieve high functional levels. Therefore, the adherence includes proportion of exercise components performed, whether progressions occurred, and whether the participant achieved the highest level of environmental challenge. The proportion of exercise components performed was the number of visit components a participant performed out of the total number of components (Usual Care: 4; High Intensity: 6). Progression was defined as an increase in the number of resistance bands for the leg press (high intensity) or an increase in the number of exercises performed in the standing position (usual care; Table 2). Environmental challenge was noted if the participants got on the floor to exercise ≥80% of sessions for the high intensity group. The ability to get up from the floor is frequently used as a training strategy to improve functional ability, 18 and is also a reliable and valid measure to indicate physical disability, frailty, and functional mobility. 26 Environmental challenge was noted in the usual care group if the participant performed more than 1 session of outdoor gait training. Outdoor gait training can be a more challenging environment for older adults as it has been shown to significantly impact walking speed and differ between fallers and non-fallers. 26 Lastly, the fidelity dimension of dosage was represented by the number of visits completed by patients during the 60-day HH care period.
Analysis
Descriptive statistics were used to describe the patient characteristics and treatment elements of the sample. For categorical data, we report the percentage within each study and the total sample size. For numeric data, we report the mean and standard deviation (SD). Within the usual care and high intensity groups, we used univariate linear regressions to model 60-day change in SPPB as a function of patient characteristics or treatment elements (1 model for each variable).
Results
Table 1 presents patient characteristics for the study sample by intervention group. In the high intensity group (N = 133) and usual care group (N = 140) more than half participants had congestive heart failure (high intensity: 57%, usual care: 53%), upper gastrointestinal disease (high intensity: 58%, usual care: 57%), and over a third had arthritis (high intensity: 44%, usual care: 38%), COPD or lung disease (high intensity: 37%, usual care 39%), depression (high intensity: 43%, usual care: 41%), or diabetes (high intensity: 45%, usual care: 41%). The average SLUMS score was 23.6/30 (high intensity) and 24.0/30 points (usual care). A total of 243 (89%) participants exhibited some degree of cognitive impairment (score ≤ 26). The average baseline SPPB score indicated functional deficits, with scores of 5.6/12 for the high intensity group and 5.3/12 for the usual care group (Table 1). An SPPB score of less than 10 is predictive of all-cause mortality. 27
The high intensity group participated in an average of 11 sessions, completing 89% of the exercise components each time (Table 2). This group had 109 patients (79%) progress with 59 patients (44%) performing exercises on the floor. The univariate linear regression analysis (Table 3) indicated that for every 2 additional visits, patients in the high intensity group could expect a 0.58-point increase in SPPB, exceeding the small meaningful change of 0.5 points (visits: β = .29, p < .01). Additionally, those completing an extra exercise component per session experienced a further 0.65-point increase in SPPB (β = 3.94, p < .01). Lastly, baseline SPPB performance was significantly associated with changes in SPPB (β = −.23, p < .01).
Linear Regression Results for 60-day Change in SPPB.
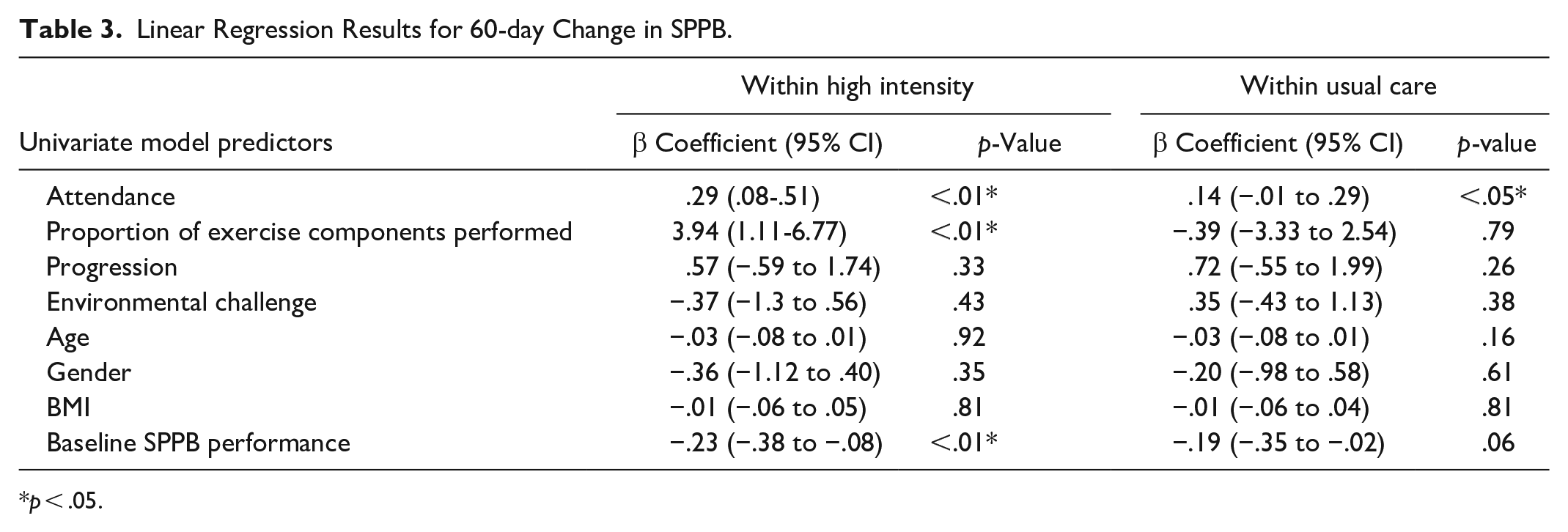
p < .05.
On average, participants in the usual care group participated in 11 sessions, completing 86% of the exercise components for each session (Table 2). A total of 112 usual care participants (80%) progressed during HH care, and 51 (36%) engaged in gait training outside of the sessions. The univariate linear regression analysis (Table 3) indicated that for every 4 additional visits, patients in the usual care group could expect an 0.56-point increase in SPPB (visits: β = .14, p = .046). No other participant characteristics or treatment elements were significantly associated with changes in SPPB (Table 3).
Discussion
This was a secondary analysis of 2 randomized controlled trials that aimed to understand treatment elements associated with improvements in physical function in older adults after hospitalization. We examined patient characteristics and treatment elements for high intensity and usual care to determine their association with change in SPPB scores. In the high intensity groups, a higher proportion of visit components and greater number of visits performed were associated with improved physical function. The high intensity program, delivered twice per week, prioritized muscle strengthening components (3 out of 6 components), and aligned with recommendations for older adults to complete 2 to 3 resistance training visits per week. 28 Findings showed those completing an extra exercise component per high intensity session experienced a further 0.65 point increase, exceeding a small meaningful change on the SPPB.
Study results found achieving the recommended frequency of 2 to 3 visits per week was expectedly linked to greater recovery in physical function. Specifically, for every 2 additional visits, patients in the high intensity group experienced a 0.58-point increase in SPPB. Patients achieving this clinically significant level of improvement are associated with better mobility and independence in daily activities, decreasing their overall risk of adverse events including rehospitalization and mortality. 25 Despite this understanding, a study using nationally representative Medicare hospital and HH claims data revealed that patients hospitalized with critical illness received, on average, only receive 1 HH rehabilitation visit per week, with one-third receiving no rehabilitation visits within the 30-day HH care period. 29 This study’s findings illuminate a potential gap between current practice and the number of visits patients may need for recovery. Specifically, our results suggest that patients receiving high intensity or usual care HH care after hospitalization significantly benefit from participating in a greater number of sessions, up to 12 within 30 to 60 days, to enhance their physical function. The high intensity groups’ stronger association with 60-day SPPB improvement may be due to the association between frequency of high intensity strength training and functional outcomes. 30 This highlights the importance of providing enough rehabilitation visits, where additional visits may incrementally improve physical function outcomes in this population. Future studies may determine the optimal number and duration of HH visits for older adults after hospitalization.
Fidelity elements appeared to be less influential on SPPB improvements in for the usual care group. This may indicate that there is other treatment elements not measured in this study influencing recovery. Possible unmeasured elements shown to impact improvements in outcomes include nutritional supplementation, 31 as well as social support and motivation.32,33 Further research is needed to clarify the relationship between treatment elements and outcomes in usual care practice.
For high intensity, our results found lower baseline SPPB performance was related to improved performance in the SPPB within the 60-day episode of care, aligning with literature that demonstrates individuals with lower baseline physical function may have a greater capacity for improvement.34 -36 Although baseline physical function is a non-modifiable factor, clinicians planning to use high intensity exercise can anticipate patients with lower baseline function may have greater gains and modify their plan of care and goals appropriately. Conversely, those with higher baseline function may show limited measurable gains on the SPPB due to ceiling effects.
We hypothesized that increasing training load or increasing the number of standing exercises (progression) would be associated with improvements in physical function; however, we found that progression was not associated with the SPPB improvements in the 60 days following acute hospitalization for either group. There may be several reasons for this phenomenon. Given the complex nature of rehabilitation interventions, our findings from the high intensity group suggest that progression alone over the 60 days following hospitalization is less impactful on functional improvement than baseline physical function, session participation, and completion of session components. It has been noted using a progressive overload approach can require up to 6 months to observe improvements in functional gains for untrained older adults.20,37 Thus, the 30- to 60-day intervention within this study may have been too short. Additionally, strengthening progress made during the 12 home sessions may not be detectable by the SPPB within this short period.
Modifying the physical environment in which exercise is performed can inherently change the degree of challenge. Environmental challenge in the high intensity groups focused on whether a participant performed an exercise on the floor. Doing an exercise on the floor then included an additional floor transfer in the session. In older adults, ability to rise from the floor predicts all-cause mortality and screens for physical disability, frailty, and functional mobility,38,39 and is potentially modifiable. In a study of older adults receiving home-based exercises after hip fracture, Mangione et al 40 found that those who were able to exercise on the floor (our definition of environmental challenge) had greater changes in 6-min-walk distances than those who did not get on the floor. However, our study did not see a relationship between getting on the floor and SPPB change. The study by Mangione et al involved 32 or 40 home-based visits over 16 weeks—more than 2 and half times the number of visits and up to double the duration performed in the parent trials of this study. Our study’s lower frequency of sessions over a shorter duration may explain the lack of observed association between the environmental challenge and improvement in physical function.
Our study reflects the medical complexity of older adults after hospitalization, with participants also experiencing on average 4 to 5 serious comorbid conditions and a majority experiencing some degree of cognitive impairment. While characteristics, such as age, gender, and BMI, have been linked with lower physical function,41 -43 our results found that these were not associated with the improvements in physical function in the 60 days following hospital discharge.
Strengths and Limitations
A strength of this study is that it includes data from 2 randomized controlled trials. Combining these trial samples is helpful in studying a heterogenous population like those receiving HH care. Another key strength of this study is that it provides valuable information about factors that may be important to consider if providing a high intensity or usual care approach. There were also limitations to this study. First, we combined data from trials that differed in duration of care. Despite the difference in overall duration, both trials prescribed 12 PT visits with a focus on similar components and assessed outcome measures at the same timepoints. Secondly, participating in sessions 2 to 3 times per week might not be enough to distinguish between specific types of exercises being impactful in the absence of adherence to the home program, which was not measured in the parent trials. Lastly, there were variables not measured in this study that may have influenced physical function such as support from providers and transition support from hospital to home, which can affect the success of HH rehabilitation services. 44 Since this was a secondary analysis, data were not available from the parent trials to characterize these additional factors.
The findings indicate that lower baseline SPPB scores are associated with greater recovery for individuals participating in high intensity exercise. Additionally, in the high intensity group, treatment elements of completing more components of a PT session and, participating in more sessions were associated with greater gains in physical function. The number of PT sessions was also found to be significantly associated with recovery in the usual care group; however, considering the lower beta estimate and lack of other treatment elements associated with recovery, there is a need for future research to explore additional factor associated with improvements in physical function. Together, these findings indicate that therapists implementing usual care physical therapy programs with patients after hospitalization should actively educate patients about the importance of consistently participating in all scheduled visits; while therapists implementing a high intensity program should also consider baseline SPPB scores and emphasize completing the full session to maximize improvements.
Footnotes
Acknowledgements
The authors thank the participating home health staff and leadership, especially Berkley Home Health. We also wish to thank Jason Falvey, PT, DPT, Julie Stutzbach, PT, DPT, PhD, Maegan Olivos, PT, DPT, Robert Burke, MD, Ethan Cumbler, MD, Deborah Currier, PTA, Gary Ruvins, JD, MBA, Tanya Budnikova, MBA, and Danielle Derlein, BS for their contributions to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH R01NR016209, VA ORD 5I01RX001978.
Disclaimers
The views expressed in the submitted article are their own and not an official position of the institution or funder.