
Abstract
Background:
Although timely communication between visiting nurses and primary care physicians is a key component of care coordination in home healthcare, few studies have examined how communication methods contribute to the timeliness of information-sharing. This study examined the association between the communication methods used by these professionals and physicians’ perceived timeliness of information-sharing in Japanese home healthcare.
Methods:
We conducted a multicenter cross-sectional study in 2024 involving patients receiving home visits from physicians. Patient-related data were collected using questionnaires completed by physicians. The outcome was physician-reported perceived timeliness of information-sharing for each patient, measured on a seven-point Likert scale (1 = not at all timely, 7 = extremely timely). Because communication methods were not mutually exclusive, they were entered simultaneously into a multivariable linear mixed-effects model with facility- and physician-level random intercepts.
Results:
Overall, 363 patients were included in the analysis. The mean timeliness score was 5.4 (standard deviation 1.2). In multivariable linear mixed-effects models, using an information and communication technology (ICT)-based system was significantly associated with higher timeliness scores compared with non-use (adjusted mean difference 0.95, 95% confidence interval [CI]: 0.69-1.20). Face-to-face interaction and telephone communication were also independently associated with significantly higher scores (0.61 [95% CI: 0.39-0.83] and 0.49 [95% CI: 0.28-0.71], respectively).
Conclusions:
Physicians reported higher timeliness of information-sharing when ICT-based systems, face-to-face interaction, or telephone communication were used, compared with non-use. Although confidence intervals overlapped, ICT-based systems showed the largest point estimate, highlighting their potential contribution to timely collaboration alongside traditional communication methods.
Keywords
Introduction
With global population aging and the growing prevalence of chronic diseases, the number of frail older adults with functional impairment continues to rise. The demand for home healthcare services has therefore grown, particularly among individuals who are unable or find it hard to leave their homes independently.1,2 Visiting nurses play an important role in providing care at home. 3 In countries such as the United States and Japan, the number of home visits by physicians, including primary care physicians and geriatricians, has also been rising.4,5
In home healthcare settings, where multiple professionals often provide care asynchronously, effective care coordination is vital. Communication between visiting nurses and primary care physicians is especially critical for this. 6 Failures in communication between these professionals have been linked to negative outcomes, such as increased hospital readmissions among patients with chronic heart failure 7 and more frequent emergency department visits for people living at home. 8 However, there are challenges in ensuring effective communication between visiting nurses and primary care physicians.6,9
One factor that may influence communication between these 2 groups is the method of communication used, such as telephone calls, face-to-face interactions, or information and communication technology (ICT) systems. 6 For instance, telephone contact is considered essential for effective communication, but ICT is expected to make information-sharing easier and more efficient. 6 However, few studies have examined how each communication method contributes to the timeliness of information-sharing. A quantitative study published in 2014 reported no significant association between the use of ICT and timeliness. 10 To the best of our knowledge, no similar research has been published since. Similarly, no studies have examined the relationship between more traditional communication methods, such as face-to-face contact and telephone use, and the timeliness of information-sharing. Meanwhile, the environment surrounding home healthcare has changed substantially over the past decade. The coronavirus disease 2019 (COVID-19) pandemic changed the needs for home healthcare services, increasing the demand for these services and altering how they are delivered.4,11 It also shifted communication among home healthcare professionals from face-to-face interactions to digital or telephone-based communication. 12 These system-level and technological changes may have influenced the relationship between communication methods and the timeliness of information-sharing, necessitating a re-examination of this issue. This study therefore examined the association between the communication methods used by visiting nurses and primary care physicians, and physicians’ perceived timeliness of information-sharing in home healthcare in Japan.
Methods
We conducted a multicenter cross-sectional study in 2024 involving patients receiving home visits and their primary care physicians.
Setting
In Japan, home healthcare is primarily provided by visiting nurses, home care physicians (including primary care physicians and other physicians involved in geriatric care), rehabilitation therapists, and pharmacists. A small number of visiting nurses are affiliated with hospitals or clinics, whereas the majority work at small-scale, community-based independent agencies. 13 Visiting nurses, including registered and licensed practical nurses, provide services such as home care guidance, family support, assistance with daily activities, medication management, and wound care. 13
Home care physicians provide medical care and prescribe treatments during home visits for patients who have difficulty accessing their facilities. It is common for each physician to collaborate with multiple visiting nurses across different nursing agencies. Patient care is delivered by nurses in response to written medical orders issued by the relevant physician for each patient. 13 Visiting nurses are then legally required to report back to the physician, through written care reports. 13 The reporting frequency is not strictly regulated, but it is customary for reports to be submitted once a month. Both medical orders and care reports are paper-based, and communication beyond this formal documentation is at the discretion of the professionals involved.
In most cases, home care physicians’ offices or hospitals are organizationally independent from nursing agencies, and electronic health record systems are not shared. Day-to-day communication between physicians and visiting nurses may occur through telephone, face-to-face interaction, or ICT, depending on local practice patterns and individual professional relationships. ICT platforms are not nationally standardized, and various systems are available from several private companies. These systems allow users to exchange electronic messages in a format similar to common social networking services, and share information such as images of skin lesions.
For this study, we conducted a questionnaire survey at 7 medical facilities that provide home visits by primary care physicians in Tokyo and Ibaraki Prefecture. These facilities were independent institutions and were not part of a single healthcare organization. Five of the participating facilities were community-based offices, and 2 were small and medium-sized local hospitals. Tokyo is a highly urbanized area with a high density of healthcare providers, and Ibaraki Prefecture includes suburban and rural areas with fewer medical resources.
Participants and Data Collection
The participants in this study were patients who received home visits from physicians at 7 medical facilities between February and March 2024, and their physicians. Inclusion criteria for patients were: (1) aged 18 years or older, and (2) living at home and not a residential care facility. Exclusion criteria included: (1) the initiation of home visits after February 2024, and (2) having unstable physical symptoms or a limited prognosis that meant that study participation could impose an undue burden. This judgment was made by the patient’s attending physician based on routine clinical assessment. Patients who were not receiving visiting nursing services were also excluded.
Physicians completed structured questionnaires by extracting patient information from medical records as part of the study; participation by physicians was voluntary. This study was conducted as part of a broader research project involving both physician- and patient-reported data collection, although the present analysis used only physician-reported data. Written informed consent was obtained from patients who received and returned questionnaires as part of the overall project, while an opt-out approach was applied for patients whose data were obtained solely from medical records, as approved by the institutional review board.
Measures
Outcome Variable: Physicians’ Perceived Timeliness of Patient-Level Information Sharing Between Visiting Nurses and Primary Care Physicians
We found no validated scale specifically assessing physicians’ perceived timeliness of information-sharing between visiting nurses and primary care physicians; therefore, we developed a single-item measure. The conceptual focus of the item was informed by the “Communication and Information Exchange” domain of the Collaborative Practice Assessment Tool. 14 The specific phrasing, “Relevant information relating to changes in patient status or care plan is shared in a timely manner between myself and the visiting nurse,” was designed to enhance face validity and contextual relevance for physicians. Responses were recorded using a seven-point Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). Although internal consistency reliability cannot be assessed for a single-item measure, measurement theory indicates that single-item instruments may be psychometrically defensible when the target construct is conceptually narrow, unidimensional, and clearly defined. 15 Under such conditions, single-item measures have been proposed as a pragmatic approach that can adequately represent the construct while minimizing respondent burden. 15
Independent Variable: Methods Used to Communicate About Patients Between Visiting Nurses and Primary Care Physicians
For each patient included in the study, participating physicians were asked whether they exchanged information with visiting nurses about that patient through any means other than those legally mandated (generally written care instructions or monthly care reports). If they answered yes, physicians were asked to indicate which communication methods they used. Multiple responses were allowed. The options included face-to-face interaction, telephone communication, fax, email, and ICT-based information-sharing systems (hereafter, ICT-based systems). An open field was also provided for respondents to specify any other methods used. We treated secure, multifunctional smartphone applications, such as those allowing encrypted messaging and image sharing, as ICT-based systems.
Covariates
Given the limited research on the relationship between communication methods used by visiting nurses and physicians and the timeliness of information-sharing, we selected the following patient-level variables as covariates based on expert consensus among the research team: age, gender, frailty severity, primary disease, and the number of home medical procedures. Frailty severity was assessed using the Clinical Frailty Scale, which ranges from 1 (very fit) to 9 (terminally ill).16,17 Scores of 7 or higher were classified as severe frailty or worse. Patients were categorized by primary disease into malignancy and non-malignancy. This dichotomization was employed to account for the distinct clinical trajectories associated with terminal cancer, characterized by rapid functional decline and a high demand for urgent communication (e.g., frequent emergency home visits 18 ), compared with the more stable or gradually progressive trajectories of other chronic conditions, including dementia or post-stroke sequelae. Although multimorbidity and cognitive function are also important clinical indicators, we used the Clinical Frailty Scale as a comprehensive measure of clinical complexity and physiological reserve, as it integrates the overall functional impact of multiple coexisting conditions, including cognitive impairment. Home medical procedures included interventions such as tracheostomy care, enteral feeding, home oxygen therapy, pressure ulcer management, intravenous therapy, and indwelling urinary catheterization. The number of home medical procedures was counted and categorized as none, 1, or 2 or more.
Statistical Analysis
We calculated descriptive statistics for patient characteristics and physicians’ perceived timeliness of information-sharing. Bivariable linear regression analysis was used to examine the association between communication methods and the timeliness of information-sharing. Based on Norman’s assertion that Likert-type scales can be robustly analyzed using parametric statistics, 19 the timeliness score was treated as a continuous variable. Each communication method—ICT-based information-sharing system, face-to-face interaction, telephone, and fax or handwritten notes—was included as a binary variable (0 = not used, 1 = used). Email use was reported for only 2 patients, and was therefore excluded from the analysis to avoid compromising statistical reliability.
To further examine the associations, we performed a multivariable analysis using linear mixed-effects models with random intercepts. A 2-level random intercept model was applied to account for clustering at both the facility and physician levels. Because communication methods were not mutually exclusive, they were entered simultaneously into the same multivariable model. This mutual adjustment allowed us to account for co-use and substitution patterns among modalities and to estimate the association of each method independent of the others. All covariates (patient age, gender, frailty severity, malignancy as primary disease, and number of home medical procedures) were treated as categorical variables.
For each analysis, we used a 2-sided significance level of P = .05. All statistical analyses were performed on complete cases, excluding patients with missing data and using SPSS Statistics version 29 (IBM Corp, Armonk, NY, USA).
Results
Participant Characteristics and Timeliness of Information-Sharing Scores
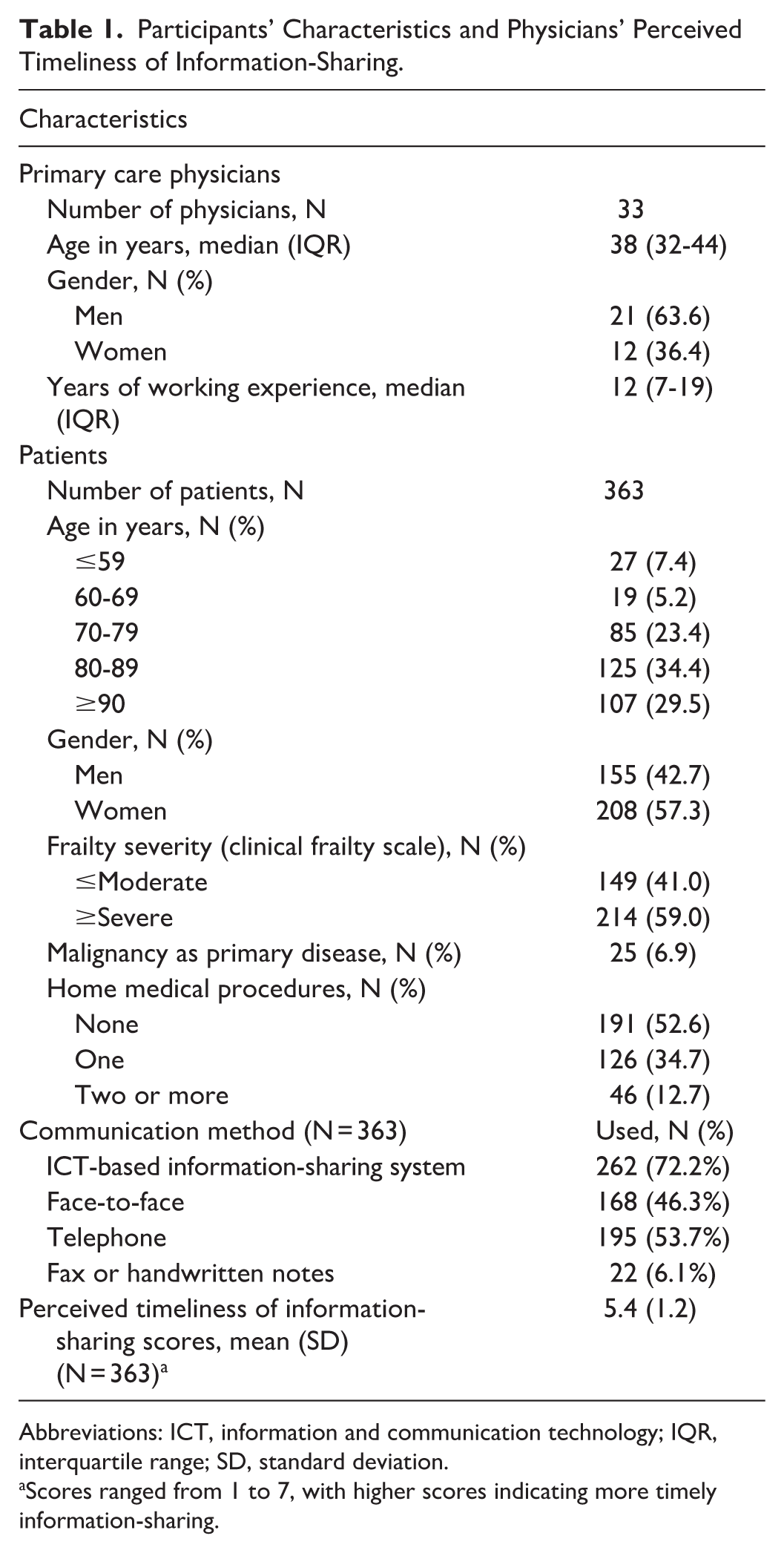
Thirty-three primary care physicians from 7 medical institutions participated in the study. Their median number of years since graduation was 12 years (interquartile range: 7-19; Table 1). Data were collected for 506 patients under the care of participating physicians. After excluding 140 patients who were not receiving visiting nursing services and 3 patients with missing data on the Clinical Frailty Scale, 363 patients were included in the analysis.
Participants’ Characteristics and Physicians’ Perceived Timeliness of Information-Sharing.
Abbreviations: ICT, information and communication technology; IQR, interquartile range; SD, standard deviation.
Scores ranged from 1 to 7, with higher scores indicating more timely information-sharing.
Table 1 shows that nearly 60% of patients were classified as having severe or greater frailty, and almost half had received at least 1 home medical procedure. Nurses and physicians communicated about patients using an ICT-based information-sharing system for 72.2% of patients, face-to-face interaction for 46.3%, telephone for 53.7%, and fax or handwritten notes for 6.1% (see Supplemental Table S1 for the frequency of combinations of communication methods). The mean score for the timeliness of information-sharing was 5.4 (standard deviation 1.2). The distribution showed no marked floor or ceiling effects.
Timeliness of Information-Sharing by Communication Method
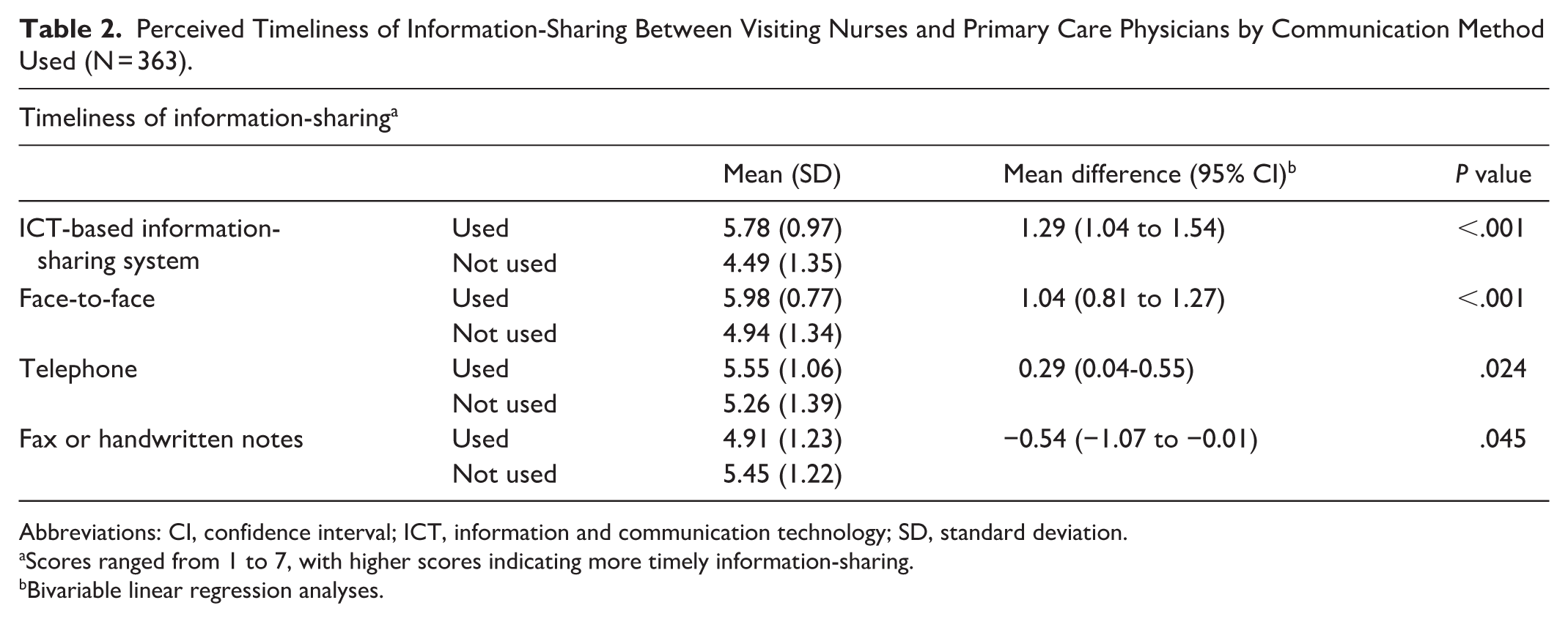
Table 2 shows descriptive statistics and results from the bivariable linear regression analyses examining differences in timeliness of information-sharing by the presence or absence of each communication method. Timeliness scores were significantly higher when ICT-based systems, face-to-face interaction, or telephone communication were used.
Perceived Timeliness of Information-Sharing Between Visiting Nurses and Primary Care Physicians by Communication Method Used (N = 363).
Abbreviations: CI, confidence interval; ICT, information and communication technology; SD, standard deviation.
Scores ranged from 1 to 7, with higher scores indicating more timely information-sharing.
Bivariable linear regression analyses.
Multivariable Analysis Using Linear Mixed-Effects Models
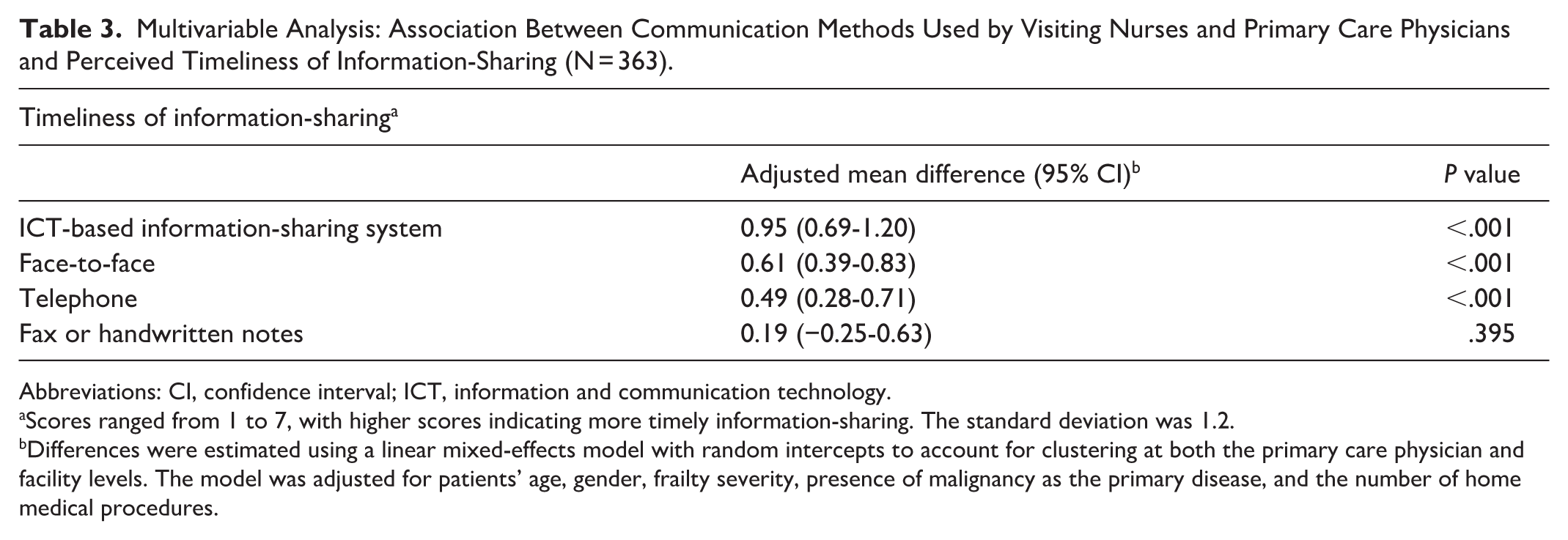
Table 3 shows the results of the multivariable analysis. The use of an ICT-based information-sharing system was associated with significantly higher timeliness of information-sharing than non-use (adjusted mean difference 0.95, 95% confidence interval [CI]: 0.69-1.20). Face-to-face interaction and telephone communication were also independently associated with significantly higher timeliness scores (0.61 [95% CI: 0.39-0.83] and 0.49 [95% CI: 0.28-0.71], respectively).
Multivariable Analysis: Association Between Communication Methods Used by Visiting Nurses and Primary Care Physicians and Perceived Timeliness of Information-Sharing (N = 363).
Abbreviations: CI, confidence interval; ICT, information and communication technology.
Scores ranged from 1 to 7, with higher scores indicating more timely information-sharing. The standard deviation was 1.2.
Differences were estimated using a linear mixed-effects model with random intercepts to account for clustering at both the primary care physician and facility levels. The model was adjusted for patients’ age, gender, frailty severity, presence of malignancy as the primary disease, and the number of home medical procedures.
Discussion
Our study examined the association between communication methods used by visiting nurses and primary care physicians, and physicians’ perceived timeliness of information-sharing in home healthcare. Physicians reported higher timeliness of information-sharing when ICT-based systems, face-to-face interaction, or telephone communication were used, compared with non-use. While the confidence intervals for these 3 methods overlapped, ICT-based systems demonstrated the largest point estimate, which is noteworthy and may indicate a relatively stronger association with timely information-sharing. Although this study relies solely on physicians’ reports, our findings can be interpreted alongside previous studies that incorporated visiting nurses’ perspectives.
In line with the nursing perspectives reported elsewhere, we found that traditional communication methods, particularly telephone and face-to-face interaction, were positively associated with perceived timeliness. Prior studies from the Netherlands and the U.S. indicate that face-to-face contact or telephone facilitate timely communication,6,20 which visiting nurses in particular tend to prefer. 6 The Media Richness Theory states that face-to-face communication is a medium rich in immediate interaction and has the advantage of facilitating rapid mutual understanding. 21 However, in practice, the feasibility of face-to-face interaction is affected by structural factors, including geographical proximity between visiting nursing agencies and physicians’ clinics.
Earlier studies on visiting nurses have reported mixed results regarding ICT use and timeliness of information-sharing.10,22 Qualitative studies suggested that ICT systems offer advantages such as asynchronous communication 23 and clinical image sharing, which are particularly valued by visiting nurses. 22 In contrast, a 2014 quantitative study in the Netherlands found no significant difference in perceived timeliness between e-messaging users and non-users. 10 Lyngstad et al suggested this may reflect the time needed to adapt to new workflows. 10 Our findings, showing a positive association from the physicians’ perspective, may reflect a decade of advancements in ICT infrastructure and system-level changes.4,11,12 Asynchronous communication is ideal for “conveyance-type” tasks, 24 allowing clinicians to process complex information at their own pace despite busy workflows. In this sense, ICT-based systems may enhance timeliness not by accelerating responses per se, but by enabling more efficient information handling in time-constrained settings.
Our findings, suggesting a potential role for ICT-based systems in improving the timeliness of communication, may have implications for policy, practice, and education. In Japan, a new reimbursement policy that incentivizes the use of ICT-based systems in home healthcare was implemented in June 2024. Our findings align with and reinforce the policy’s intent. From a practice perspective, both individual practitioners and organizations may benefit from actively adopting ICT tools. However, their effective use will require appropriate implementation strategies, including training and user support tailored to varying levels of experience.25,26
At the same time, our findings indicate that no single communication method is universally optimal; rather, maintaining a diverse media repertoire may best support timely and context-appropriate information-sharing. From this perspective, the concept of a “media repertoire” 27 suggests that practitioners benefit from flexibly selecting communication methods according to situational demands rather than relying on a single modality. For example, practitioners may use the telephone for urgent changes or ethically complex decisions, and ICT-based systems for accurate record-keeping or efficiency, ideally guided by shared team-based agreements. Further research is needed to understand how practitioners select communication methods in practice. Such insights could be gained through qualitative studies involving visiting nurses and physicians.
The organizational independence of visiting nursing agencies and physicians in Japan, together with the absence of nationally standardized ICT platforms, may be distinctive in an international context. However, accumulating evidence on communication methods may help improve information-sharing between visiting nurses and physicians in other healthcare systems. This includes settings with greater electronic health record integration or different organizational structures, where similar coordination challenges may arise.8,28
Limitations
This study had several limitations. First, the outcome measure was not formally validated. Because it was assessed using a single-item instrument, internal consistency reliability could not be evaluated, and the measure may not fully capture a complex or multidimensional construct. However, measurement theory suggests that single-item instruments can be acceptable when the target construct is conceptually narrow and clearly defined. 15 Empirical studies have shown that single-item measures can demonstrate validity comparable to multi-item scales for specific and concrete constructs in psychology, 29 and similar findings have been reported in epidemiologic research. 30 In the present study, the outcome focused on a specific aspect of perceived timeliness in information-sharing to minimize respondent burden. Nonetheless, the use of a single-item may have introduced measurement error and limited sensitivity, potentially underestimating effect sizes.
Second, because data were collected solely from physicians, visiting nurses’ perspectives were not captured, potentially biasing the observed associations. Additionally, potential clustering or confounding effects related to visiting nurses or their agencies could not be accounted for. The association with face-to-face interaction may partly reflect geographical proximity. Although each patient usually has a primary nurse, some agencies may use a team-based approach; in such cases, physicians’ evaluations are considered to reflect the functional timeliness of communication with the nursing team as a whole.
Third, unmeasured patient-level and contextual factors—including living situation, clinical urgency, physician workload, and familiarity with ICT—may have influenced communication method selection and perceived timeliness, even after accounting for physician-level clustering. Fourth, because multiple communication methods were frequently used together (see Supplemental Table S1), the observed associations should be interpreted as reflecting the relative contribution of each method within a multimodal communication context, rather than the isolated effect of any single method. Finally, the study was conducted in a limited geographical area of Japan, which may restrict the generalizability of the findings to other regions.
Conclusions
In the context of home healthcare, physicians reported higher perceived timeliness of information-sharing when ICT-based systems, face-to-face interaction, or telephone communication were used between visiting nurses and primary care physicians. Although confidence intervals overlapped, ICT-based systems showed the largest point estimate, highlighting their potential contribution to timely collaboration alongside traditional communication methods. Whether communication method selection constitutes a modifiable health process associated with system-level performance in home healthcare warrants further investigation.
Supplemental Material
sj-doc-1-hhc-10.1177_10848223261445864 – Supplemental material for Communication Methods and Perceived Timeliness of Information-Sharing Between Visiting Nurses and Primary Care Physicians in Japanese Home Healthcare
Supplemental material, sj-doc-1-hhc-10.1177_10848223261445864 for Communication Methods and Perceived Timeliness of Information-Sharing Between Visiting Nurses and Primary Care Physicians in Japanese Home Healthcare by Gen Nakayama, Shoichi Masumoto, Yu Sun, Mitsuaki Ishii, Sayaka Nin, Takashi Inaba, Natsuki Kajikawa, Shuhei Hamada, Noriyuki Kimura and Jun Hamano in Home Health Care Management & Practice
Footnotes
Acknowledgements
The authors thank the participating physicians for their cooperation with the survey. We are also grateful to Dr. Atsushi Ueda, Director of Kizuna Home Care Clinic, for his cooperation in this study. We thank Melissa Leffler, MBA, from Edanz (![]() ) for editing a draft of this manuscript.
) for editing a draft of this manuscript.
During the preparation of this manuscript, ChatGPT (OpenAI) was used in order to refine language. The tool was not used to generate scientific content, data, analyses, or conclusions. The authors reviewed and edited the content as needed and take full responsibility for the accuracy and originality of the work.
Ethical Considerations
Ethics Committee of the Institute of Medicine, University of Tsukuba (approval no. 1951-1).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS Grant-in-Aid for Scientific Research Grant Number 21K15658.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request*.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.