
Abstract
Background:
Effective hypertension management among older adults increasingly depends on engagement in health-promoting behaviors (HPBs) within home and community settings. Health literacy is a key determinant of self-management capacity; however, limited evidence exists regarding sex differences in the relationship between health literacy and HPBs among community-dwelling older adults with hypertension, particularly in the post–COVID-19 context where home-based care has become more prominent.
Methods:
A cross-sectional study was conducted among 164 community-dwelling older adults aged 60 years and older with diagnosed hypertension in urban and rural communities in Thailand. Participants completed validated self-report questionnaires. Sex differences were examined using chi-square and Fisher’s exact tests. Multiple regression analyses were performed separately for men and women to identify sex-specific predictors of health-promoting behaviors.
Results:
Both men and women demonstrated relatively high levels of health literacy and overall health-promoting behaviors. Health literacy was a significant predictor of health-promoting behaviors for both men (β = .34, P < .001) and women (β = .32, P < .001). Women reported significantly higher engagement in smoking and alcohol avoidance behaviors than men, while physical activity levels were low across both groups. Among women, older age was positively associated with engagement in health-promoting behaviors (β = .14, P = .001); this association was not observed among men.
Conclusion:
Health literacy plays a critical role in supporting health-promoting behaviors among older adults with hypertension, with notable sex-specific patterns. These findings highlight the importance of integrating health literacy assessment and sex-responsive education strategies into home health nursing practice.
Introduction
Hypertension is 1 of the most prevalent chronic conditions among older adults and a leading contributor to cardiovascular morbidity and mortality worldwide. 1 As populations age, hypertension management increasingly occurs in home and community settings, placing greater responsibility on older adults to engage in effective self-care and health-promoting behaviors. 2 Supporting sustained lifestyle modification in these settings is therefore a central concern for home health care management and nursing practice.
Health-promoting behaviors (HPBs)—such as maintaining a healthy diet, engaging in regular physical activity, avoiding tobacco and excessive alcohol use, adhering to prescribed medications, and participating in preventive care—are essential for controlling blood pressure and preventing complications.3,4 However, many community-dwelling older adults struggle to adopt and maintain these behaviors, particularly those with long-standing hypertension and multiple health demands. 5 Evidence from Thailand indicates that suboptimal lifestyle practices and delayed behavior change remain common among older adults with hypertension, underscoring the need for targeted, practice-relevant interventions in home-based care settings.6,7
Health literacy is a key determinant of older adults’ capacity to manage chronic conditions at home. Health literacy refers to the ability to access, understand, and apply health information to make appropriate health decisions.8,9 Adequate health literacy supports medication adherence, lifestyle modification, and effective navigation of healthcare services, while limited health literacy is associated with poorer self-management and worse health outcomes in chronic disease populations.10,11 In hypertension, higher health literacy has been linked to improved self-care behaviors and better blood pressure control. 12 Nevertheless, a substantial proportion of older adults experience difficulty understanding health information, which may limit their engagement in these behaviors within home and community contexts. 13
Sex differences may further influence the relationship between health literacy and HPBs among older adults. Sex functions as a social determinant of health, shaping health beliefs, behaviors, and use of healthcare services. 14 Prior research suggests that women are generally more likely to engage in preventive health behaviors, whereas men more frequently report risk behaviors and delayed care seeking. 12 However, evidence regarding sex differences in health literacy and its association with HPBs remains limited, particularly in the post–COVID-19 era, when disruptions to healthcare access and daily routines heightened reliance on home-based self-management.15,16 Addressing this gap, the present study examined sex differences in health literacy and health-promoting behaviors among community-dwelling older adults with hypertension in the post–COVID-19 context, with the goal of informing sex-responsive, home health nursing interventions.
Methods
Study Design
This was a cross-sectional design study to determine gender differences in the association between health literacy and health-promoting behaviors among community-dwelling older adults with hypertension during the new normal post-COVID-19 Era.
Sample and Settings
We utilized data from a prior study 17 that recruited older adults with NCDs from both urban and rural areas in Thailand. Recruitment took place between September 10th and November 10th, 2022, during the new normal post-COVID-19 pandemic. The original study examined health-promoting behaviors among older adults with noncommunicable diseases using structural equation modeling. In contrast, the present analysis focuses specifically on the hypertension subgroup and examines sex differences in health literacy and health-promoting behaviors to generate implications for home health nursing practice. Participants completed a one-time self-reported questionnaire. Eligible participants were selected using a combination of multistage stratified sampling and simple random sampling. The inclusion criteria specified that participants had to be older adults aged 60 years and above, diagnosed with hypertension, and capable of understanding Thai. Those who were unwilling to participate or unable to complete the questionnaire were excluded from the study. This research specifically targeted older adults with hypertension, and a comprehensive description of the methods, sample size, and data collection procedures has been documented separately. Initially, 250 participants were recruited; however, 86 were excluded for not meeting the hypertension diagnosis criteria. As a result, the final sample size for this study comprised 164 participants.
Measures
The research questionnaires consisted of 3 parts:
Part I: The Health Literacy Scale was originally developed in Thai by the Health Education Division 18 and is utilized to assess health literacy among older adults with hypertension. This scale consists of 10 items, each rated on a four-point scale ranging from “1 = strongly disagree” to “5 = strongly agree.” Higher scores indicate a greater level of health literacy. The levels of health literacy are categorized into 4 distinct ranges: “poor level (10-20), fair level (20-29), good level (30-39), and very good level (40-50).” The scale demonstrates a high reliability, with a Cronbach’s alpha of .90.
Part II: The Health-Promoting Behaviors Scale was originally developed in Thai by the Health Education Division 18 and consists of a 19-item questionnaire divided into 7 subscales: (1) nutrition, (2) exercise, (3) smoking, (4) alcohol consumption, (5) stress management, (6) rational drug use, and (7) preventive measures against COVID-19 infection. Respondents use a five-point rating scale ranging from “1 = not at all” to “5 = completely,” with higher scores indicative of stronger HPBs. The levels of HPBs, both overall and across subdomains, are categorized into 4 tiers: bad level (<60%), fair level (60%-70%), good level (71%-80%), and very good level (>80%). The scale demonstrates good reliability, with a Cronbach’s alpha of .75, and each subdomain ranging from .73 to .83.
Part III: Sociodemographic data, which consists of sex, age, education, income, comorbidity, health care coverage, perceived smoking, perceived alcohol drinking, perceived physical health, perceived mental health status, perceived sleep quality, and perceived exercise.
Data Analyses
Descriptive statistics were employed to analyze the sociodemographic data of participants, detailing frequency, percentages (%), mean scores, and standard deviation (SD). Chi-squared and Fisher’s exact tests were utilized to compare health literacy and HPBs between male and female participants. Furthermore, multiple regression analysis was conducted to explore predictive factors influencing health-promoting behaviors among older adults with hypertension. All assumptions regarding normality, linearity, multicollinearity, and autocorrelation were satisfied. A significance level of P < .05 was established for all analyses. The statistical analyses were performed using IBM SPSS 25.0 software (IBM Corp., Armonk, NY, USA).
Results
Among the 164 participants in the study, Table 1 presents detailed sociodemographic information, along with levels of perceived smoking, alcohol consumption, sleep quality, exercise, physical health, and mental health status. The majority of participants were female (62.19%), with a mean age of 70.30 years (SD = 7.77). Furthermore, 69.5% had a primary school education or lower. The average income was USD 102.34 (SD = 144.75), and most participants relied on universal health coverage (84.1%). Additionally, 81.7% reported having comorbid conditions. In terms of smoking, 91.5% did not smoke, while only 6.1% were current smokers at the same level as before the COVID-19 pandemic; moreover, 86.60% did not consume alcohol. Most participants reported their levels of perceived exercise and sleep remained consistent with pre-pandemic conditions, at 82.3% and 90.9% respectively. Furthermore, a majority rated their physical health and mental health status positively, with 38.4% and 42.1% reporting good levels, respectively. When comparing demographic data between male and female participants, perceived exercise and sleep scored significantly higher among females.
Participants’ Demographic Data.
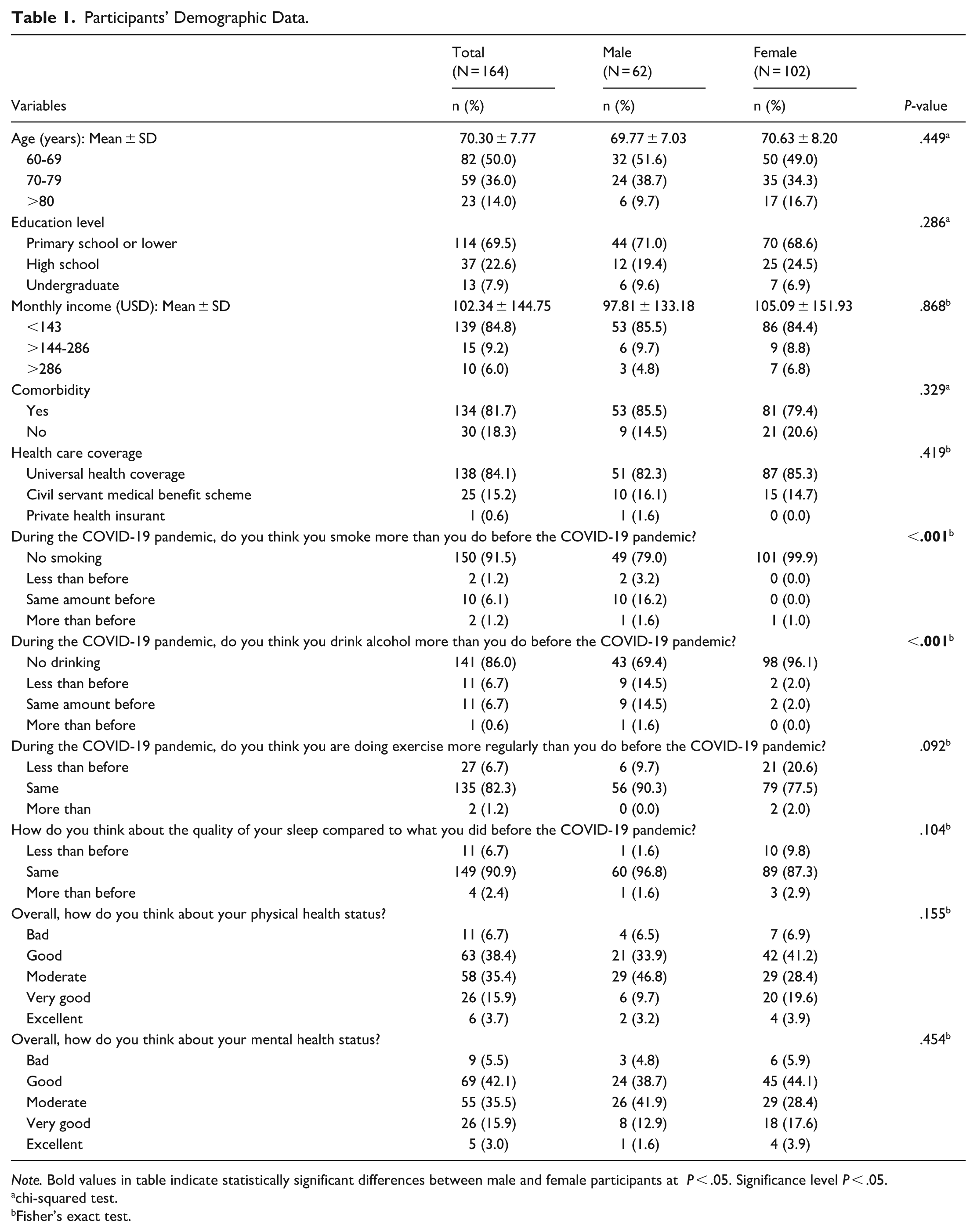
Note. Bold values in table indicate statistically significant differences between male and female participants at P < .05. Significance level P < .05.
chi-squared test.
Fisher’s exact test.
As illustrated in Table 2, participants exhibited high levels of health literacy (mean = 37.50, SD = 6.33) and healthy behavioral practices (mean = 68.02, SD = 7.05). Breaking down the healthy behavioral practices by subdomain, smoking (mean = 9.12, SD = 1.62), alcohol consumption (mean = 4.66, SD = 0.85), rational drug use (mean = 4.66, SD = 0.85), and preventive behaviors against COVID-19 (mean = 14.06, SD = 1.52) were found to be at very good levels. In contrast, the exercise domain was rated poorly, with a mean score of 5.96 (SD = 2.04). Furthermore, scores in the smoking and alcohol subdomains were significantly higher among female participants compared to their male counterparts.
Levels of Health Literacy and Health-Promoting Behaviors.
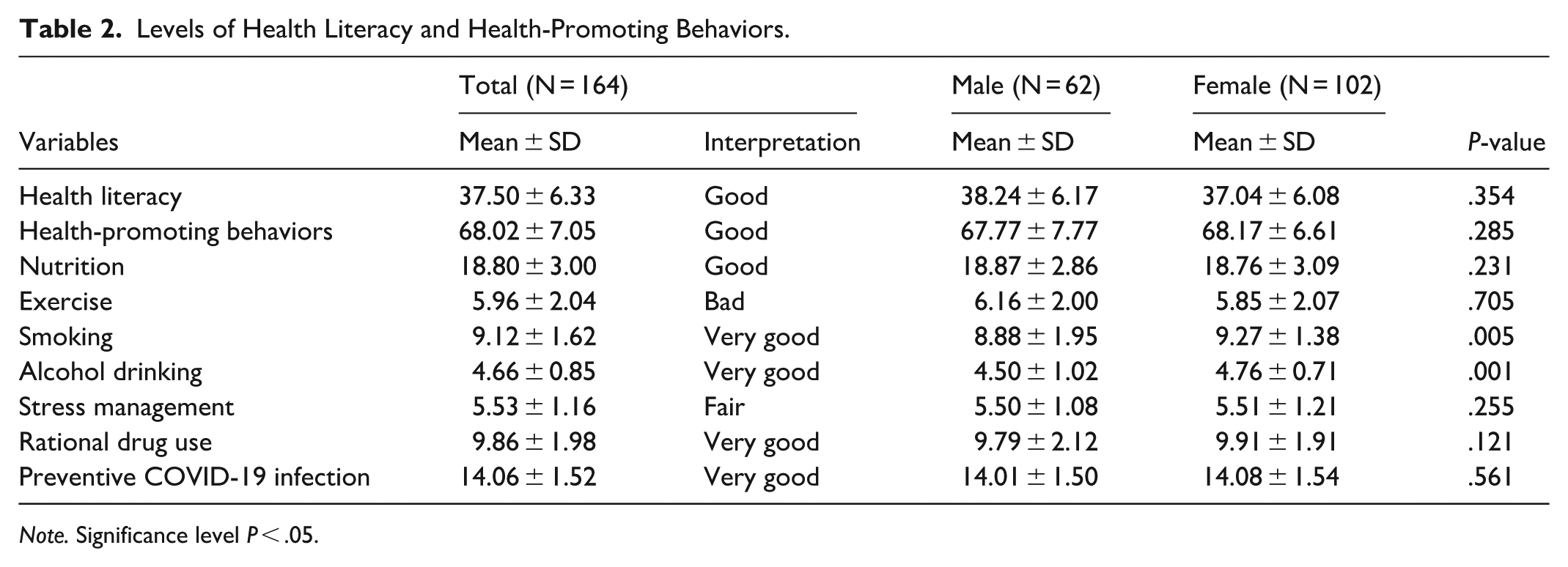
Note. Significance level P < .05.
In Table 3, which outlines the factors influencing HPBs among the male group, it is noted that health literacy (β = .342, P < .001) and perceived smoking (β = .196, P = .024) serve as significant predictors of health-promoting behaviors in older adults with hypertension, explaining approximately 26.7% of the variance. Similarly, for the female group, health literacy (β = .342, P < .001), perceived smoking (β = .296, P = .043), and age (β = .136, P < .001) were found to be predictive of HPBs in older adults with hypertension, accounting for roughly 40.9% of the variance.
Factors Predicting Health-Promoting Behaviors Among Older Adults with Hypertension.
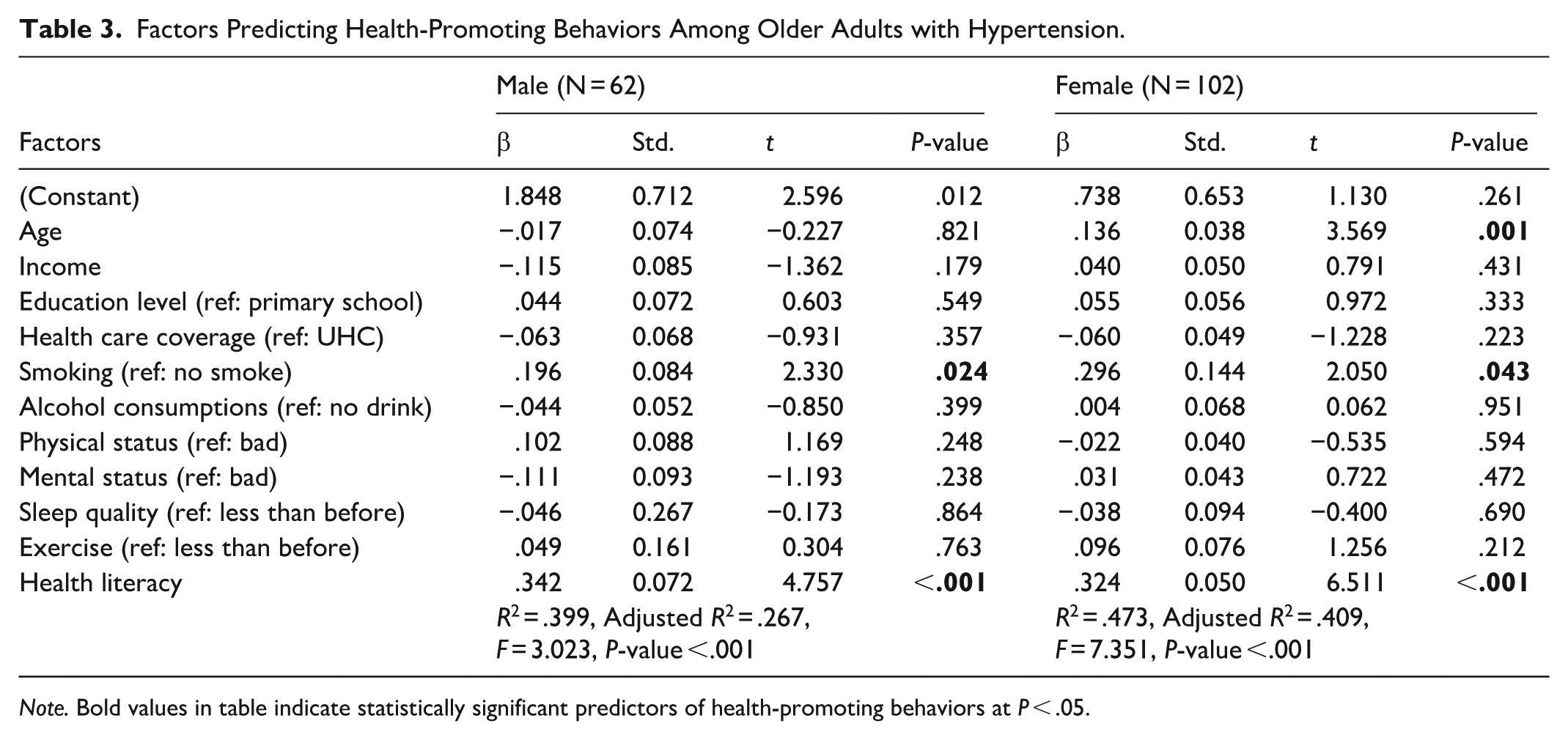
Note. Bold values in table indicate statistically significant predictors of health-promoting behaviors at P < .05.
Discussion
This study contributes to the growing evidence that health literacy is a critical determinant of health-promoting behaviors among older adults with chronic conditions. Consistent with previous research, higher health literacy was associated with greater engagement in these behaviors, supporting its role in effective chronic disease self-management among community-dwelling older adults. 19 Our findings reinforce that older adults with adequate health literacy are better equipped to adopt recommended lifestyle behaviors, including medication adherence and dietary modification, which are essential for hypertension control.
In contrast, limited health literacy has been linked to unhealthy lifestyle patterns, such as insufficient physical activity and poor dietary practices, which may compromise chronic disease management. 20 The present findings align with evidence indicating that hypertensive patients with higher health literacy demonstrate improved disease knowledge and blood pressure management, whereas those with lower health literacy experience greater challenges in maintaining recommended self-care behaviors. 21 These results underscore the importance of addressing health literacy as a modifiable factor in home-based hypertension management.
Notably, health literacy levels did not differ significantly between men and women in this study. While previous research has reported potential sex disparities in health literacy related to educational and social factors, 22 the comparable health literacy observed here may reflect the impact of public health education initiatives and community-based support in reducing literacy gaps among older adults. This finding suggests that equitable access to health information may mitigate traditional sex-based disparities in health literacy within this population.
Sex differences were, however, evident in specific health-promoting behaviors. Women demonstrated higher engagement in smoking and alcohol avoidance behaviors, consistent with established evidence that older men are more likely to engage in health-risk behaviors such as tobacco and alcohol use. 23 Conversely, physical activity levels were low across both sexes, highlighting a persistent challenge in promoting regular exercise among older adults regardless of sex. 23 These patterns suggest that while some behaviors may benefit from sex-specific strategies, others—such as physical activity—require universal, accessible approaches tailored to older adults’ functional abilities.
The post–COVID-19 context provides important insight into health behavior adaptation among older adults. High adherence to preventive behaviors observed in this study likely reflects effective health communication and sustained awareness during the pandemic, as reported in prior studies.15,22 These findings indicate that older adults can successfully adopt and maintain health behaviors when provided with clear, accessible information and community support—an important consideration for ongoing home health care delivery.
Practical Implications
The findings have direct implications for home health care management and nursing practice. Routine assessment of health literacy during home visits may help identify older adults who require tailored education and support. Home health nurses are well positioned to deliver health literacy–sensitive interventions, including simplified communication, visual aids, and reinforcement of key self-management behaviors related to hypertension. 24
Sex-responsive strategies may further enhance intervention effectiveness. For example, older men may benefit from targeted counseling focused on smoking cessation and alcohol reduction, while both men and women may require structured, home-based physical activity guidance to address consistently low exercise levels. Integrating health literacy-focused education into routine home care may strengthen self-management capacity, improve blood pressure control, and reduce preventable complications. 25
At the systems level, incorporating health literacy into home health protocols and community-based aging services may support more equitable and effective chronic disease management. Community partnerships, caregiver involvement, and accessible educational resources can further reinforce health-promoting behaviors among older adults living at home. Together, these approaches highlight the importance of health literacy—informed, practice-oriented strategies in improving outcomes for older adults with hypertension.
To translate these findings into practice, home health nurses should incorporate routine health literacy screening using brief validated tools during home visits. For patients with limited health literacy, nurses can apply strategies such as the teach-back method, simplified written materials, and visual aids to improve understanding and adherence. Additionally, structured home-based interventions—such as personalized exercise plans, medication management support, and behavioral counseling—should be tailored according to sex-specific needs. For example, targeted smoking cessation and alcohol reduction counseling may be prioritized for older men, while both men and women may benefit from guided physical activity programs adapted to functional capacity. Engaging family caregivers and community health volunteers may further enhance adherence and sustainability of health-promoting behaviors among homebound older adults.
Study Limitations
Several limitations should be considered when interpreting the findings. First, the cross-sectional design precludes causal inference between health literacy and HPBs. Second, the modest sample size (N = 164), drawn from specific urban and rural communities in Thailand, and the smaller proportion of male participants may limit generalizability. Third, reliance on self-reported measures may introduce recall and social desirability bias, potentially overestimating positive health behaviors. Fourth, health literacy was assessed using a Thai-language scale focused primarily on basic health understanding, which may not capture more complex or digital dimensions of health literacy. Finally, unmeasured factors such as hypertension-specific knowledge, self-efficacy, and pandemic-related stressors may have influenced behaviors, as reflected in the moderate variance explained by the regression models. Future studies using longitudinal designs, objective behavioral measures, and broader health literacy assessments are warranted.
Conclusion
This study highlights the central role of health literacy and health-promoting behaviors among community-dwelling older adults with hypertension. Although overall health literacy levels did not differ by sex, meaningful sex-specific differences were observed in certain behaviors, particularly smoking and alcohol avoidance, and in age-related patterns of engagement in health-promoting behaviors among women. These findings underscore the importance of integrating health literacy assessment and sex-responsive education into home health nursing practice. Tailored, health literacy-sensitive interventions may strengthen chronic disease self-management and promote healthier aging among older adults in the post–COVID-19 context.
Footnotes
Ethical Considerations
The study was carried out in accordance with the Declaration of Helsinki and received approval from the Institutional Review Board of Krirk University (protocol code 0204/001, dated July 1, 2022) as well as the Institutional Review Board of Ubon Ratchathani Provincial Health Office (protocol code SSJ.UB 2565-115, dated September 9, 2022).
Author Contributions
Conceptualization, W.S., S.T., and J.S.; methodology, W.S. and S.T.; software, W.S. and J.S.; validation, W.S., S.T., and J.S.; formal analysis, W.S.; investigation, W.S. and S.T.; writing—original draft preparation, W.S.; writing—review and editing, S.T. and J.S; supervision, S.T. and J.S. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.