
Abstract
Introduction:
Identifying factors associated with job satisfaction among home health care workers can help identify high-risk health professionals and provide evidence-based data for interventions to improve working conditions.
Objective:
To investigate professional group differences in job satisfaction, burnout, and depression, and to identify factors associated with job satisfaction among healthcare workers in home health care services.
Methods:
In Turkey, the Istanbul Provincial Health Directorate, which has 200 healthcare workers, conducted the study with 177 people from its home health services unit. Maslach Burnout Inventory, the Beck Depression Inventory, and the Job Satisfaction Scale were used. In this cross-sectional study, data were collected online.
Results:
There was a significant difference between professions in terms of emotional burnout, depression, and job satisfaction scores, with nurses being the most disadvantaged group in all 3 categories. According to the regression model, job satisfaction decreased as the depression score (β = −.020, P = .008) and emotional burnout (β = −.024, P = .006) increased, while it increased as the personal accomplishment score increased (β = .019, P = .016). Job satisfaction was also higher among those who were more likely to recommend their profession to others (β = .124, P = .031).
Conclusion:
The fact that nurses are the most disadvantaged group regarding burnout and depression, as well as job satisfaction, should be taken into consideration in workforce and work planning for home health care services. The inverse relationship between depression and burnout with job satisfaction reveals the connection between healthcare professionals’ mental health and their working life.
Introductıon
Home health care services are intended not only to support patients’ health status in their home environment but also to help alleviate the caregiving burden on family members and support caregivers’ quality of life.1,2 The multidimensional nature of home health care services makes the role of healthcare professionals critical in ensuring the quality and effectiveness of these services. Healthcare professionals working in home health care services often face substantial job demands, including heavy workload, time pressure, emotionally demanding care, and challenging or fragmented working conditions.3,4 Such working conditions may adversely affect healthcare professionals’ mental well-being and contribute to burnout and depressive symptoms.3,5
Burnout is a work-related syndrome that arises from chronic workplace stress that has not been successfully managed. 6 Importantly, evidence from home care settings suggests that burnout is also a substantial problem in this workforce. An integrative review reported that burnout among home care nurses ranged from 13% to 36%, with work overload, time pressure, fragmented care, role conflict, and emotional demands identified as recurrent contributors. 7 Depressive symptoms are prevalent among healthcare professionals and represent an important occupational mental health concern.8,9 Depressive symptoms and broader mental health strain also appear to be relevant in home-based care work.10,11 Identifying levels of burnout and depression among home healthcare workers and related factors, developing strategies to address these issues, and implementing measures to enhance job satisfaction are of great importance for effectively addressing the challenges faced in the health sector.
Job satisfaction is an important workforce outcome in healthcare because it is closely linked to employee well-being and broader organizational functioning. This issue is also highly relevant in home care, where job satisfaction has been linked to work organization and daily working conditions. 12 Higher job satisfaction has been associated with better quality of life and lower absenteeism, and may also contribute to improved quality and safety of care.13-15 Among home care workers, job satisfaction appears to be shaped particularly by time pressure, interruptions, role conflicts, autonomy, care continuity, and management and teamwork practices. 12 Development of strategies by healthcare institutions to enhance job satisfaction can positively impact both the well-being of employees and the quality of patient care.
Although burnout, depression, and job satisfaction have been widely studied among healthcare professionals in a variety of healthcare settings, evidence from home health care remains comparatively limited and has often focused on specific professional groups or selected outcomes rather than examining these issues together.3,16 This gap is important because population aging and the growing need for long-term, integrated care are increasing the relevance of home- and community-based services; therefore, identifying the factors associated with job satisfaction in this workforce is essential for informing strategies to improve service quality and effectiveness.17,18
In Türkiye, the population aged 65 and over was 10.6% in 2024, while in the WHO European region it was 18.1%, indicating the potential for this rate to almost double over time. The fact that the prevalence of diabetes in the 20 to 79 age group is 7.8% in the WHO European region, while it is 16.5% in Türkiye, indicates that Türkiye has an increased disease burden in terms of some chronic diseases. On the other hand, Türkiye ranks second to last among OECD countries in terms of the number of physicians and last in terms of the number of nurses. 19 Factors such as an aging population, an increasing burden of chronic diseases, and a shortage of healthcare personnel are creating an environment where home healthcare services face limited resources but high demand. Research in home healthcare services can help develop solutions to this issue in Türkiye.
This study aimed to investigate professional group differences in burnout, depression, and job satisfaction, and to identify factors associated with job satisfaction, among healthcare workers in home health care services affiliated with the Istanbul Provincial Health Directorate.
Methods
Compliance With Ethical Standards
Ethical approval for the study was obtained from the Ethics Committee of Gazi University on February 7, 2023 (Research Code No: 2023-276). Permission was also granted by the Istanbul Provincial Health Directorate on June 20, 2023 (Decision No: 2023/11). The Declaration of Helsinki’s guiding principles were followed when conducting the study.
Study Design
This study is a cross-sectional study. The study was conducted with the participation of healthcare professionals working in home health care service units affiliated with the Public Hospitals Directorates under the Istanbul Provincial Health Directorate. In Istanbul, there are 6 home health care units operating under Tuzla State Hospital, Üsküdar State Hospital, Bahçelievler State Hospital, Prof. Dr. Cemil Taşcıoğlu City Hospital, Haseki Training and Research Hospital, and Beylikdüzü State Hospital. The inclusion criterion for this study is being a healthcare professional working in home health care. The study population included healthcare professionals such as physicians, nurses, physiotherapists, health technicians, dietitians, and psychologists employed in these units. Personnel such as security officers, drivers, secretaries, and staff from administrative, financial, and support services were excluded from the study as they are not classified as healthcare professionals. 200 healthcare professionals met the inclusion criteria. 177 individuals participated in the study (88.5%).
Data Collection
The research data were collected between July 20, 2023, and March 1, 2024. Prior to administering the questionnaire, participants were informed about the study, and their consent was obtained. The data was collected online; a link to the questionnaire was shared with the participants.
The questionnaire consisted of a total of 93 questions organized into 5 sections. The first included basic demographic characteristics of the participants including age, gender, profession; the second focused on work-related features; the third contained the Maslach Burnout Inventory; the fourth included the Beck Depression Inventory; and the fifth comprised the Job Satisfaction Scale. The primary dependent variable in this study is job satisfaction.
Scales
The Maslach Burnout Inventory was adapted into Turkish, and its validity and reliability were established.20,21 The scale consists of 3 dimensions: emotional burnout (9 items), depersonalization (5 items), and personal accomplishment (8 items). Items are scored on a 5-point Likert scale from 0 (never) to 4 (always), yielding possible score ranges of 0 to 36 for emotional exhaustion, 0 to 20 for depersonalization, and 0 to 32 for personal accomplishment. High scores on the emotional burnout and depersonalization subscales and low scores on the personal accomplishment subscale are considered indicative of burnout.20,21 The emotional burnout subscale reflects feelings of being emotionally overextended and exhausted by one’s work or profession. The depersonalization subscale describes an unfeeling and impersonal response toward the recipients of care or service, characterized by treating them in a dehumanizing or indifferent manner without recognizing them as unique individuals. The personal accomplishment subscale assesses a sense of competence and successful achievement in one’s work with people, particularly in face-to-face interactions. 21
The Beck Depression Inventory is one of the most widely used scales for assessing depression. The Beck Depression Inventory consists of 21 items scored on a 4-point scale (0-3), with total scores ranging from 0 to 63. Higher total scores indicate greater severity of depressive symptoms. It has been translated into Turkish, and studies have confirmed that it is a valid and reliable instrument for measuring depression. 22
The Job Satisfaction Scale was developed through a validity and reliability study. Exploratory factor analysis revealed that the scale comprises 34 items across 5 factors, and the overall Cronbach’s alpha coefficient of the scale was found to be .963. 23 A 5-point Likert scale ranging from “strongly disagree” to “strongly agree” was used to measure the items.
Variables and Statistical Analysis
Considering that the study variables exhibited a normal distribution, parametric analysis techniques such as the Student’s t-test and ANOVA (Analysis of Variance) were employed. When ANOVA results were found to be statistically significant, the Post-Hoc Bonferroni test was applied to identify which specific group differences were significant.
Pearson correlation analysis was used to determine the relationships between variables. To construct a multivariable model related to job satisfaction, linear regression analysis was performed using the variables that were found to be significantly associated with job satisfaction in the correlation analysis. The categorical independent variables in the regression model included perceived health status (reference: very poor), level of willingly choosing the profession (reference: not at all), willingness to recommend the profession to others (reference: definitely would not recommend), and preference for going abroad to work (reference: would never prefer). The continuous independent variables in the model were emotional burnout score, depersonalization score, personal accomplishment score, and depression score. The “Backward Selection” method was used in the linear regression analysis. A P-value of <.05 was considered statistically significant. IBM SPSS version 28 was used for data analysis.
Results
Demographic and Professional Characteristics of Participants
Women constituted 61% of the participants. Regarding perceived health status, 0.6% of the participants reported it as very poor, 3.4% as poor, 24.9% as neither good nor poor, 49.7% as good, and 21.5% as very good. Additionally, 14.1% stated that they had a chronic illness. Participants’ ages ranged from 20 to 59 years, with a mean age of 30.9.
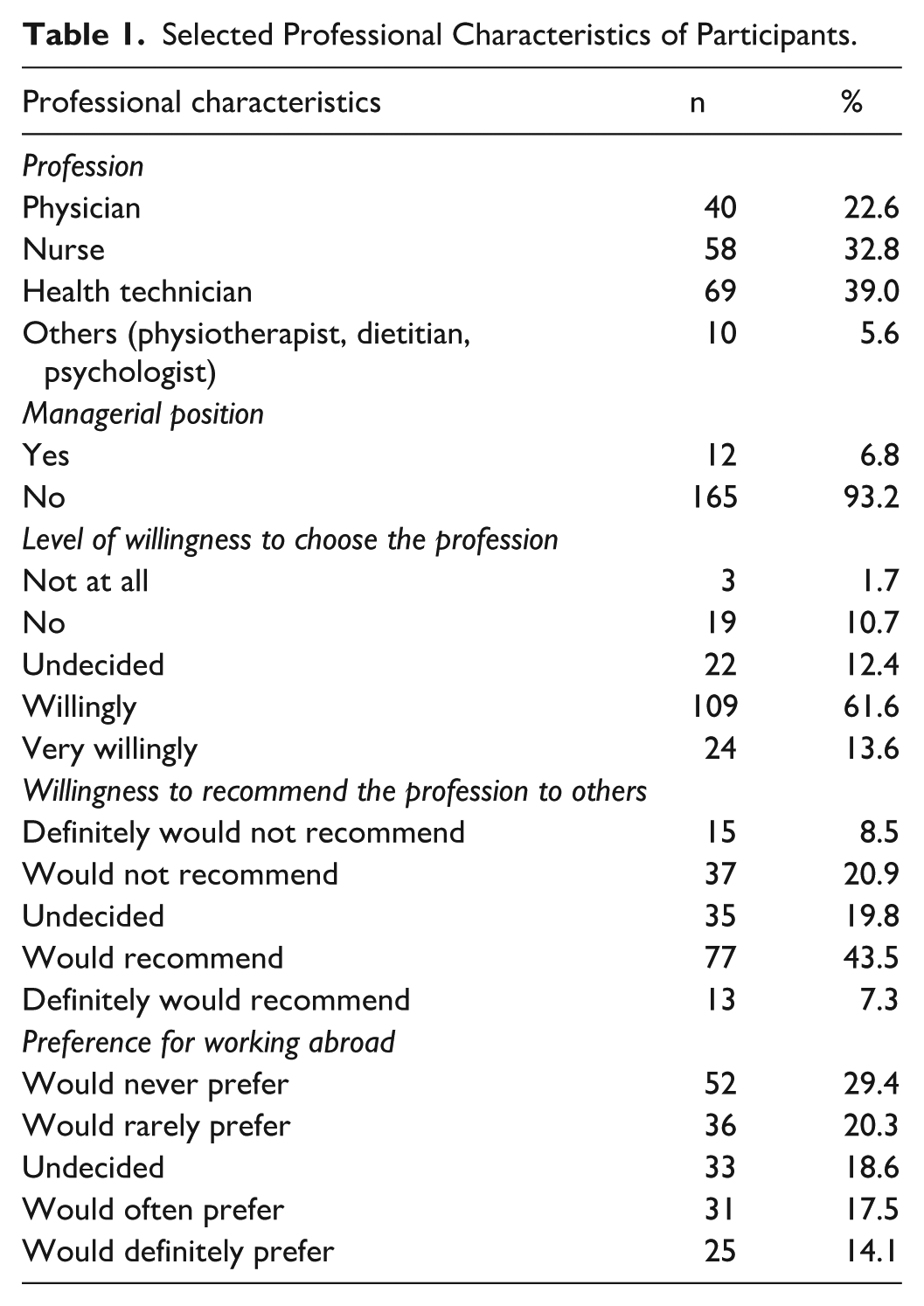
Table 1 presents selected professional characteristics of the participants. 5.6% were categorized as other healthcare professionals (n = 10). These are including physiotherapists (n = 8), a dietitian (n = 1), and a psychologist (n = 1).
Selected Professional Characteristics of Participants.
Maslach Burnout, Beck Depression, and Job Satisfaction Scores
Table 2 shows the changes in burnout scores by profession. A statistically significant difference was observed among professions in terms of emotional burnout scores (P = .005). This difference was primarily due to the disparity between nurses and health technicians (P = .009). A statistically significant difference was found in depression scores across professions (P = .018), which was again attributable to the difference between nurses and health technicians (P = .016). Similarly, job satisfaction scores differed significantly by profession (P = .018), with the difference arising from the comparison between nurses and health technicians (P = .020).
Changes in Maslach Burnout, Beck Depression, and Job Satisfaction Scores by Profession.
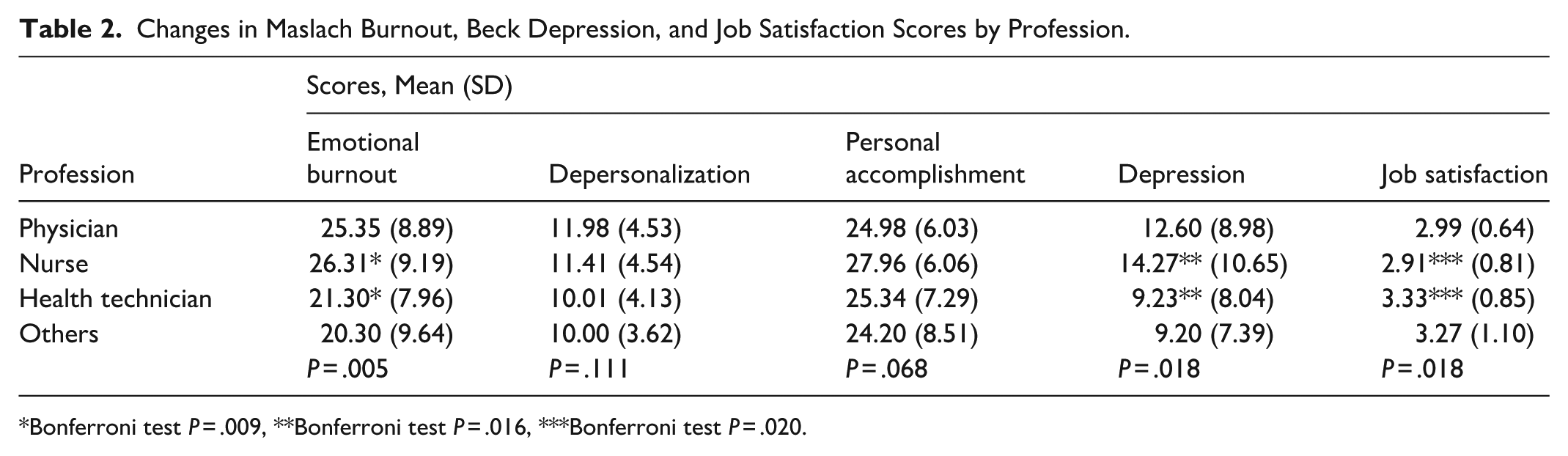
Bonferroni test P = .009, **Bonferroni test P = .016, ***Bonferroni test P = .020.
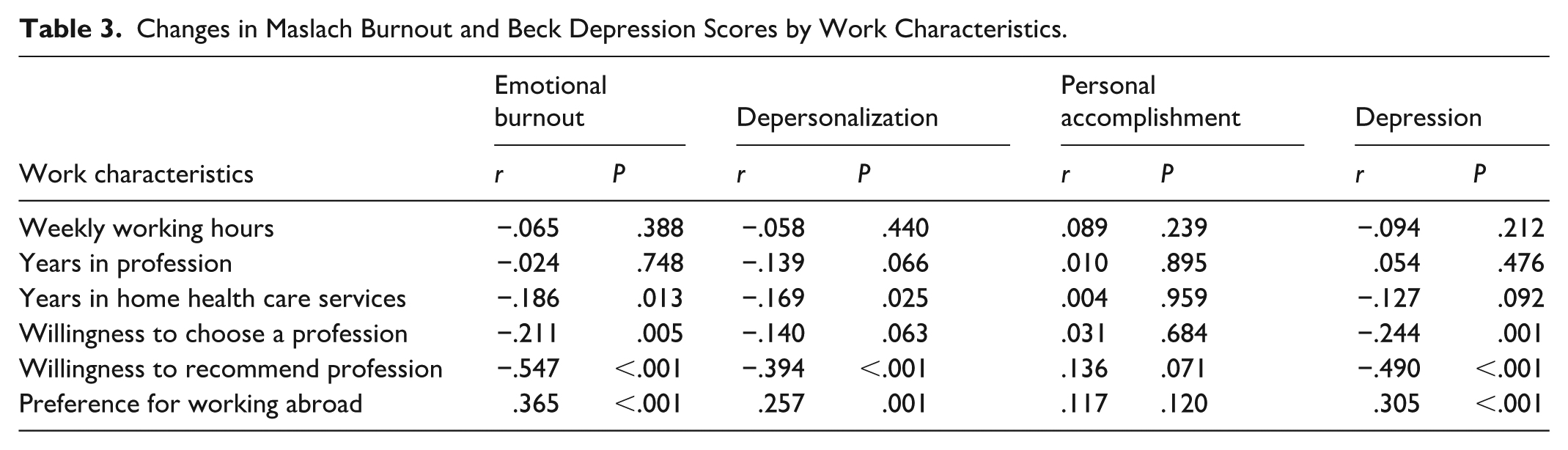
Table 3 presents the changes in Maslach Burnout and Beck Depression scores according to certain work-related characteristics. Years in home health care services were found to be correlated with emotional burnout (r = −.186, P = .013), depersonalization (r = −.169, P = .025). Willingness to choose a profession was found to be correlated with emotional burnout (r = −.211, P = .005) and depression (r = −.244, P < .001). Willingness to recommend profession was found to be correlated with emotional burnout (r = −.547, P < .001), depersonalization (r = −.394, P < .001), and depression (r = −.490, P < .001). A preference for working abroad was found to be correlated with emotional burnout (r = .365, P < .001), depersonalization (r = .257, P < .001), and depression (r = .305, P < .001).
Changes in Maslach Burnout and Beck Depression Scores by Work Characteristics.
Factors Associated With Job Satisfaction
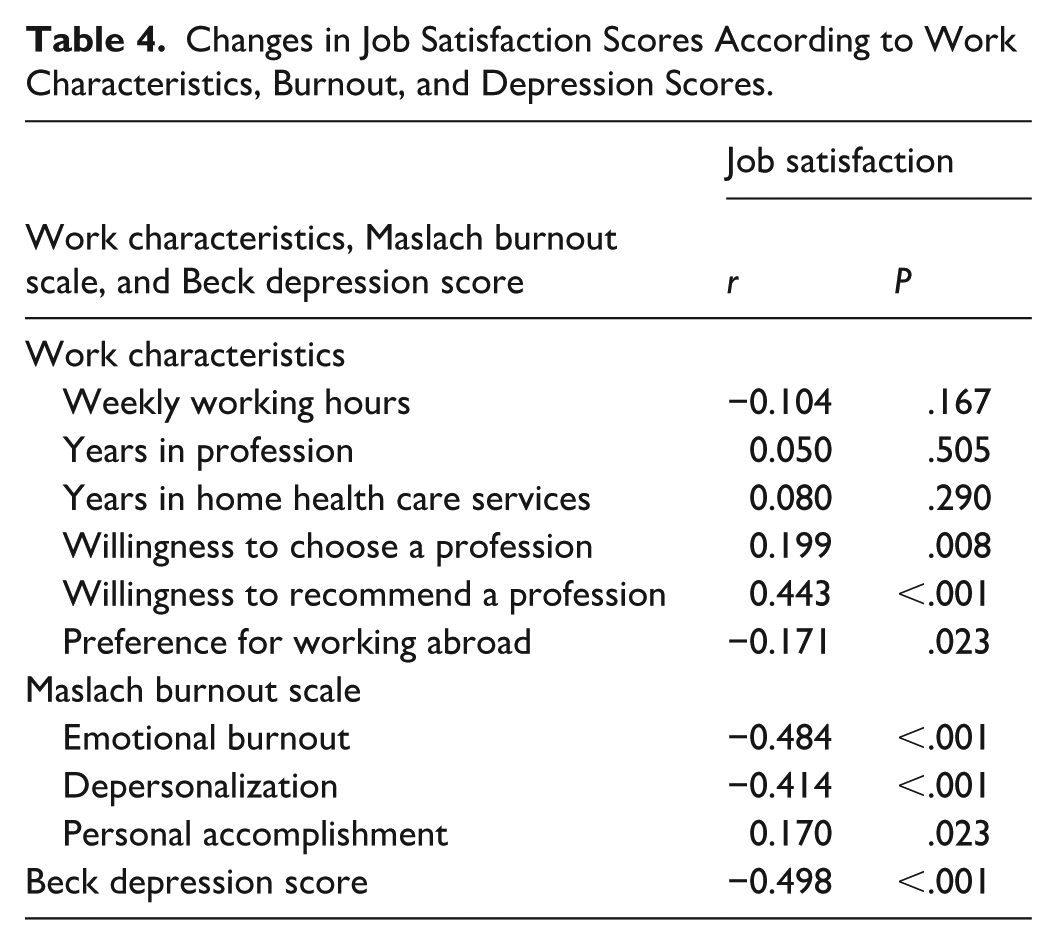
Table 4 shows the changes in job satisfaction scores according to certain work-related characteristics as well as burnout and depression scale scores. Job satisfaction score was found to be correlated with the level of willingly choosing the profession (r = .199, P = .008), willingness to recommend the profession to others (r = .443, P < .001), and preference for working abroad (r = −.171, P = .023). Job satisfaction was also correlated with emotional burnout score (r = −.484, P < .001), depersonalization score (r = −.414, P < .001), personal accomplishment score (r = .170, P = .023), and Beck Depression Inventory score (r = −.498, P < .001).
Changes in Job Satisfaction Scores According to Work Characteristics, Burnout, and Depression Scores.
No statistically significant differences were found in job satisfaction scores between genders (P = .826), marital status groups (P = .387), or between those with and without chronic illnesses (P = .585). Additionally, no correlation was observed between age and job satisfaction score (P = .212). However, a positive correlation was identified between perceived health status and job satisfaction score (r = .341, P < .001).
Table 5 presents the linear regression model of factors associated with job satisfaction. According to the multivariable model, depression score (standardized β = −.231, P = .008) and emotional burnout score (standardized β = −.258, P = .006) had a negative effect on job satisfaction score. In contrast, personal accomplishment score (standardized β = .159, P = .016) and willingness to recommend one’s profession to others (standardized β = .169, P = .031) were positively associated with job satisfaction score (Model P < .001).
Linear Regression Model of Factors Associated With Job Satisfaction.
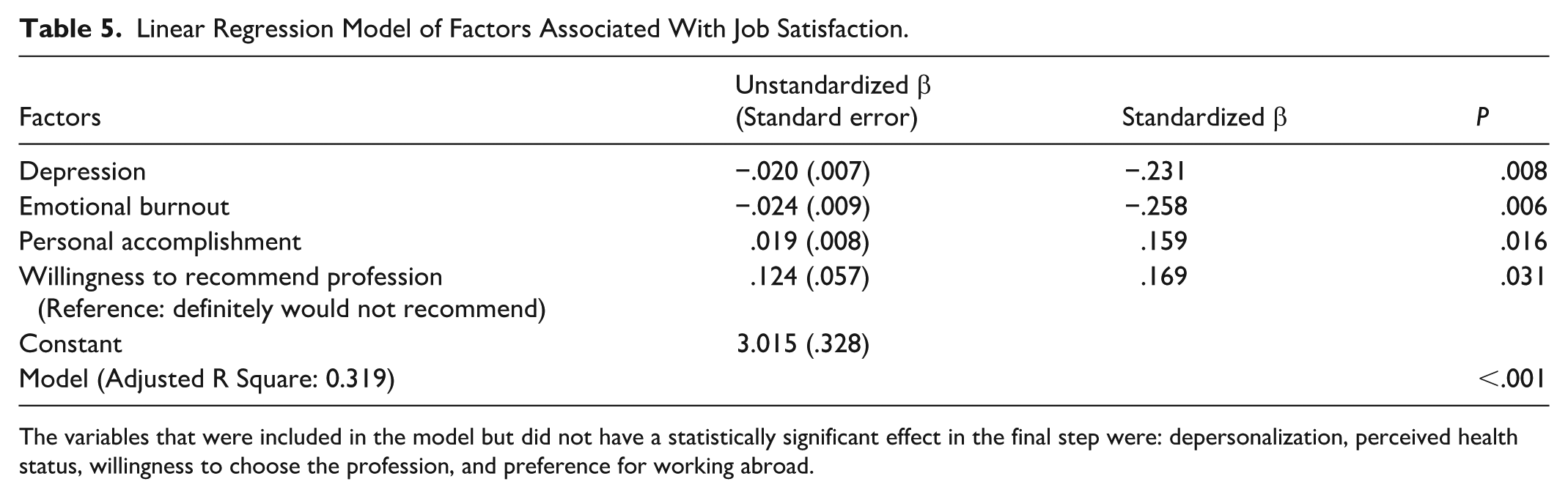
The variables that were included in the model but did not have a statistically significant effect in the final step were: depersonalization, perceived health status, willingness to choose the profession, and preference for working abroad.
Discussion
Home health care services are ideally delivered through a multidisciplinary team composed of various healthcare professionals, including physicians, nurses, health officers, physiotherapists, psychologists, dietitians, social workers, and drivers. In this study as well, the majority of participants (77.4%) were non-physician healthcare professionals from different disciplines.
In our study, emotional burnout differed significantly across professions, and nurses had the highest mean score. Studies conducted in hospitals in the US and Greece have shown that nurses are among the occupational groups at the highest risk of burnout.24,25 In a recent Turkish study conducted among healthcare workers in public home health care units, professional category was significantly associated with burnout, and nurses had significantly higher emotional exhaustion scores than technicians. 26 Taken together, these findings suggest that although the magnitude of burnout may vary by service setting, nurses appear to be particularly vulnerable across different areas of healthcare. The finding that nurses are a high-risk group for burnout in home health care services should be taken into account in workforce planning and work organization for these services.
Among the participants, 50.3% were at a minimal level of depression, 23.7% at a mild level, 18.6% at a moderate level, and 7.3% at a severe level. These findings indicate that a significant proportion of healthcare personnel working in home health care services are at risk for depression. A significant difference was found in depression scores across professions, with nurses having the highest mean score. Some studies, outside of home health care settings, have found that nurses are at higher risk for depression.26-28 In contrast, studies conducted in a university hospital and among operating room staff found no significant differences in depression scores between professions.29,30 While there are studies examining mental health among home health care workers, these studies tend to focus on a specific occupational group and do not include comparative results between different professions.10,12 According to our study, nurses working in home health care units are also a high-risk group in terms of depression highlights their disadvantaged position regarding mental health in this particular field of practice.
A significant difference in job satisfaction was observed between professions, with nurses having the lowest mean score. In a 2026 Turkish study of healthcare workers in public home health care units, job satisfaction differed significantly across occupations, with nurses appearing more disadvantaged than health technicians. 26 Similar profession-based differences have also been reported in public primary care, where job satisfaction was found to be low especially among general practitioners and nurses, although the most disadvantaged group may differ across settings. 31 In our study, nurses had the highest scores in terms of emotional burnout and depression, and also had the lowest scores in job satisfaction. This indicates that, among home health care professionals, nurses represent the most disadvantaged group across multiple dimensions.
The finding that nurses were the most disadvantaged group in terms of burnout, depressive symptoms, and job satisfaction may be related to the distinctive organization of home health care nursing.3,10,32 In this setting, nurses often work more independently and with less immediate peer support than in hospital-based environments, while also facing time pressure, fragmented care processes, interruptions, and emotionally demanding patient contact.3,10 Qualitative evidence from home health aides also suggests that workers want support that reduces isolation and helps them manage mood and stress. 10 Accordingly, the disadvantages observed among nurses in our study point to the need for more than staffing expansion alone; strengthening real-time clinical backup, peer support, continuity of assignments, protected break time, and nurses’ influence over scheduling and daily work organization may help reduce burnout and depressive strain while improving job satisfaction.
Although our study did not find a significant relationship between overall years of professional experience and burnout, a negative correlation was observed between the length of time working in a home health care unit and both emotional burnout and depersonalization scores. This pattern may reflect either a selection effect, whereby workers who cope less well with demanding work leave earlier, or the gradual development of setting-specific coping strategies over time.33,34 This finding underscores the need to develop orientation and adaptation training programs for healthcare professionals who are newly assigned to home health care units.
Correlation analyses indicate that as the level of preference for working abroad increases, emotional burnout, depersonalization, and depression scores also rise, while job satisfaction scores decline. These findings suggest that interventions aimed at reducing burnout and enhancing job satisfaction among healthcare professionals may help mitigate the growing loss of health workforce capacity due to international migration. Because of the cross-sectional design, we cannot determine whether migration intention is driven primarily by burnout and depressive strain or by declining job satisfaction; however, recent evidence from Türkiye suggests that these processes are likely interrelated rather than mutually exclusive, as brain drain attitudes among nurses were found to be negatively associated with job satisfaction and positively associated with burnout. 35 Similarly, workload has been shown to increase nurses’ intention to leave, with work satisfaction acting as an important mediator of this relationship. 36 From a broader health-system perspective, these findings are important because recent Turkish literature identifies heavy workload, low pay, insufficient staffing, workplace violence, limited career opportunities, and poor working conditions as major push factors for migration among nurses and physicians.37,38
According to the correlation analysis, higher levels of willingly choosing one’s profession are associated with lower emotional burnout and depression scores, and higher job satisfaction scores. These findings highlight the importance of providing counseling during the career selection process that includes information about the working conditions in the healthcare field, as such guidance can play a crucial role in fostering long-term job satisfaction throughout one’s professional life.
Higher levels of job satisfaction among those who were more likely to recommend their profession to others were observed both in bivariate comparisons and in the multivariable model. This finding suggests that willingness to recommend one’s profession is a stronger predictor of job satisfaction compared to other variables examined. Therefore, the tendency to recommend one’s profession to close contacts may serve as a practical indicator in the rapid assessment of job satisfaction.
In our study, the multivariable model showed that higher depression scores were associated with lower levels of job satisfaction. Although recent studies directly evaluating the association between depressive symptoms and job satisfaction in home health care workers are limited, available evidence from home health aides indicates that job-related organizational factors influence mood and stress in this workforce. 10 In other healthcare settings, this relationship has been demonstrated more directly; depression was significantly negatively correlated with nurses’ job satisfaction in a 2024 meta-analysis, and healthcare workers with mental disorders were shown to report lower job satisfaction than healthy colleagues in a 2024 occupational health study. 39 The persistence of this effect in our multivariable model indicates that depression continues to negatively influence job satisfaction even when other potentially related factors are accounted for. This relationship highlights the connection between mental health and job satisfaction.
In our study, the multivariable model revealed that job satisfaction decreased as emotional burnout increased and increased as personal accomplishment scores rose. Similarly, studies are in the Germany and USA conducted among nurses reported a negative relationship between burnout and job satisfaction.40,41 Identifying factors that may contribute to increased burnout and implementing interventions to improve these factors may lead to enhanced job satisfaction among healthcare workers.
Study Limitations
Since this study was conducted in only 1 province, its results cannot be generalized to the country level. Since it is a cross-sectional study, its capacity to show cause and effect relationships is quite low compared to other types of studies. Another limitation of this study is that it used scales containing self-reported responses as measurement tools. While factors related to job satisfaction, including burnout and depression, were examined, a possible limitation of this study may be the insufficient consideration of potential confounding variables.
Conclusions
The identification of significant differences between professions in terms of emotional burnout, depression, and job satisfaction—with nurses emerging as the most disadvantaged group across all 3 variables—highlights the need to prioritize improving the working conditions of nurses employed in home health care services.
As this is a cross-sectional study, it does not allow for conclusions about the direction of causality; therefore, the relationships observed may be bidirectional. Nonetheless, the multivariable analysis results reveal the associations of depression and burnout with job satisfaction, underscoring the strong link between work life and mental health. Efforts aimed at improving job satisfaction may also function as preventive mental health interventions.
Willingness to recommend one’s profession to others was identified as a factor that increases job satisfaction in a multivariate model. Therefore, a question regarding willingness to recommend one’s profession to others could be functional in a rapid assessment of job satisfaction.
Footnotes
Author Note
This article was prepared based on Alituran’s doctoral thesis in public health, which was conducted under Tüzün’s supervision.
Ethical Considerations
Ethical approval for the study was obtained from the Ethics Committee of Gazi University on February 7, 2023 (Research Code No: 2023-276).
Consent to Participate
Participants were informed about the study beforehand, and their consent was obtained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset is not being shared because permission has not been obtained from the provincial health directorate, which is the senior management of the healthcare institutions from which the study data was collected.