
Abstract
Background:
Alzheimer’s disease and related dementias (ADRD) represent a growing public health challenge in the United States, with substantial disparities across populations and health systems. However, hospital-level disparities in ADRD burden remain poorly understood, particularly in the Southern United States. This study aimed to examine racial, socioeconomic, and rural–urban disparities in hospital-level ADRD burden across hospitals in the Southern United States.
Methods:
This study conducted a cross-sectional analysis of 1396 hospitals across 17 Southern states. ADRD burden was defined as the proportion of patients diagnosed with ADRD at the hospital level. Racial composition, socioeconomic status (dual eligibility), and rural–urban classification were examined. Quartile-based analyses and multivariable linear regression models were used to assess disparities.
Results:
The mean ADRD burden was 0.24 (SD = 0.11). ADRD burden increased markedly across quartiles of both black patient composition and dual eligibility (both P < .001), with hospitals in the highest quartiles exhibiting nearly double the burden compared to those in the lowest. Rural hospitals had higher ADRD burden than metropolitan hospitals, with micropolitan hospitals showing intermediate levels. In adjusted models, higher proportions of black patients (β = .33, 95% CI 0.292-0.366; P < .001) and dual-eligible patients (β = .32, 95% CI 0.284-0.360; P < .001) were strongly associated with increased ADRD burden. These findings were consistent across analytic approaches.
Conclusion:
Substantial and consistent racial, socioeconomic, and rural disparities in ADRD burden exist across hospitals in the Southern United States. These findings have implications for home health care planning and community-based dementia services.
Keywords
Introduction
Alzheimer’s disease and related dementias (ADRD) continue to pose a growing public health challenge, particularly in aging populations. In the United States, the burden of ADRD has increased steadily over the past decades, with clear differences in risk, diagnosis, and care across population groups. 1 A substantial body of evidence points to persistent racial, socioeconomic, and geographic disparities, reflecting broader structural inequities embedded within the healthcare system.2,3 As dementia care increasingly shifts toward home- and community-based settings, understanding how disparities are distributed across healthcare systems is critical for planning equitable care delivery.
Racial disparities in ADRD are especially well documented. Black populations in the United States consistently experience a higher risk of ADRD compared with White populations. 4 This pattern has been linked to long-standing structural disadvantage, unequal access to healthcare, and a higher burden of cardiometabolic conditions such as hypertension and diabetes.5 -7 Socioeconomic disadvantage further compounds these risks. Individuals with dual eligibility for Medicare and Medicaid often face delays in diagnosis, fragmented care, and limited access to dementia-specific services. 8 Geographic context also plays an important role, as populations in rural areas frequently encounter shortages of specialists and diagnostic resources, contributing to disparities in dementia care and outcomes.9,10
Although these disparities have been extensively described at the individual level, less attention has been given to how they are reflected within healthcare institutions. Hospitals serve populations with differing demographic and socioeconomic profiles, which may translate into substantial variation in disease burden across facilities. This issue is particularly relevant in the Southern United States, a region characterized by higher prevalence of cardiometabolic risk factors, greater socioeconomic disadvantage, and long-standing structural inequalities in health. However, the extent to which these factors shape hospital-level ADRD burden has not been well characterized.
Understanding how ADRD burden is distributed across hospitals is important for identifying where needs are greatest and for informing more equitable allocation of healthcare resources. Examining disparities at the institutional level may also provide insight into structural patterns that are not apparent in individual-level analyses. The present study, therefore, examined racial, socioeconomic, and rural–urban disparities in ADRD burden across hospitals in the Southern United States. It was hypothesized that hospitals serving higher proportions of Black patients and socioeconomically disadvantaged populations, as well as those located in rural areas, would have higher ADRD burden.
Methods
Study Design and Data Source
This study used a cross-sectional design based on secondary analysis of a publicly available hospital-level dataset of fee-for-service Medicare beneficiaries in 2019. 11 The analytic sample was restricted to hospitals located in the Southern United States, defined according to U.S. Census regional classification. Hospitals were included if they had available information on ADRD burden, racial composition, dual eligibility, rural–urban classification, hospital size, number of patients, number of beds, and teaching status. Hospitals were excluded if they were located outside the Southern region, were not classified as hospitals in the dataset, or had missing data on key analytic variables. After applying these inclusion and exclusion criteria, the final analytic sample included 1396 hospitals across 17 Southern states.
Measures
Outcome
The primary outcome was ADRD burden, defined as the proportion of patients diagnosed with ADRD at the hospital level. This variable was used as the dependent variable in all primary regression analyses.
Exposures
The main exposure variables captured hospital-level patient composition and geographic context. Racial composition was measured as the proportion of Black patients within each hospital. Socioeconomic status was operationalized using the proportion of patients dually eligible for Medicare and Medicaid. Geographic classification was based on rural–urban status and categorized as metropolitan, micropolitan, or small town/rural.
Covariates
Hospital characteristics included total number of patients and number of beds (both standardized per 1000 units), as well as hospital size (small, medium, large) and teaching status (teaching vs non-teaching). These variables were included to account for differences in hospital capacity and organizational structure.
Statistical Analysis
Descriptive statistics were used to summarize hospital characteristics. Continuous variables are presented as means with standard deviations, and categorical variables are presented as counts with percentages. To examine unadjusted gradients in ADRD burden, hospitals were categorized into quartiles based on the distribution of Black patient composition and dual eligibility. These quartile variables were used only for descriptive and group-comparison analyses, and differences in ADRD burden across quartiles were assessed using 1-way analysis of variance (ANOVA). Multivariable linear regression models were then used to examine the associations between ADRD burden and key predictors, including racial composition, socioeconomic status, and rural–urban classification, while adjusting for hospital characteristics. In these regression models, Black patient composition and dual eligibility were entered as continuous proportion variables ranging from 0 to 1, rather than as quartile categories. Regression coefficients (β), 95% confidence intervals, and P-values were reported. All statistical tests were 2-sided, and a P-value < .05 was considered statistically significant. Hospitals with missing data on key study variables were excluded from the analysis. The proportion of missing data was minimal (<5%) and did not materially affect the analytic sample. Analyses were conducted using R version 4.5.3 (2026-03-11).
Results
Table 1 summarizes the characteristics of 1396 hospitals in the Southern United States. The mean ADRD burden was 0.24 (SD = 0.11), indicating that approximately 24% of patients were diagnosed with ADRD at the hospital level. ADRD burden is presented as a proportion in Table 1 and as a percentage in the quartile-based comparisons to improve interpretability. On average, Black patients comprised 24% of hospital populations, Hispanic patients comprised 13%, and dual-eligible patients accounted for 48%. Hispanic patient composition was included as a descriptive characteristic of the hospital populations, whereas the primary analytic focus was on Black patient composition, dual eligibility, and rural–urban status. Most hospitals were medium-sized (51.27%) and located in metropolitan areas (66.12%), with the majority being non-teaching institutions (95.20%). The largest proportions of hospitals were in Texas (21.56%) and Florida (11.89%).
Characteristics of Hospitals in the Southern United States (N = 1396).
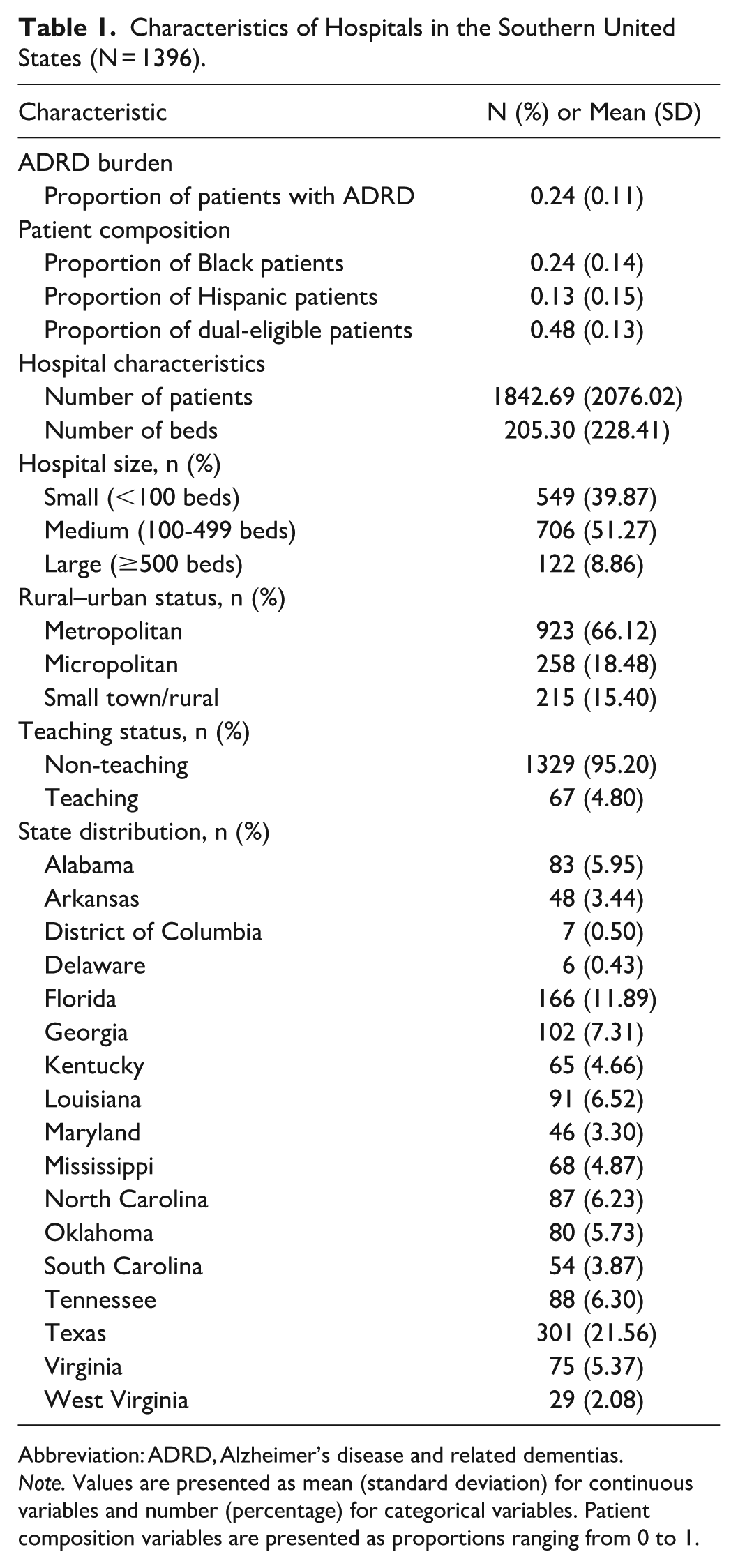
Abbreviation: ADRD, Alzheimer’s disease and related dementias.
Note. Values are presented as mean (standard deviation) for continuous variables and number (percentage) for categorical variables. Patient composition variables are presented as proportions ranging from 0 to 1.
ADRD burden increased progressively across quartiles of both racial composition and socioeconomic status (Table 2). Hospitals in the highest quartile of Black patient composition and dual eligibility had nearly twice the ADRD burden compared to those in the lowest quartile (both P < .001).
ADRD Burden by Racial Composition and Socioeconomic Status Among Hospitals in the Southern United States (N = 1396).
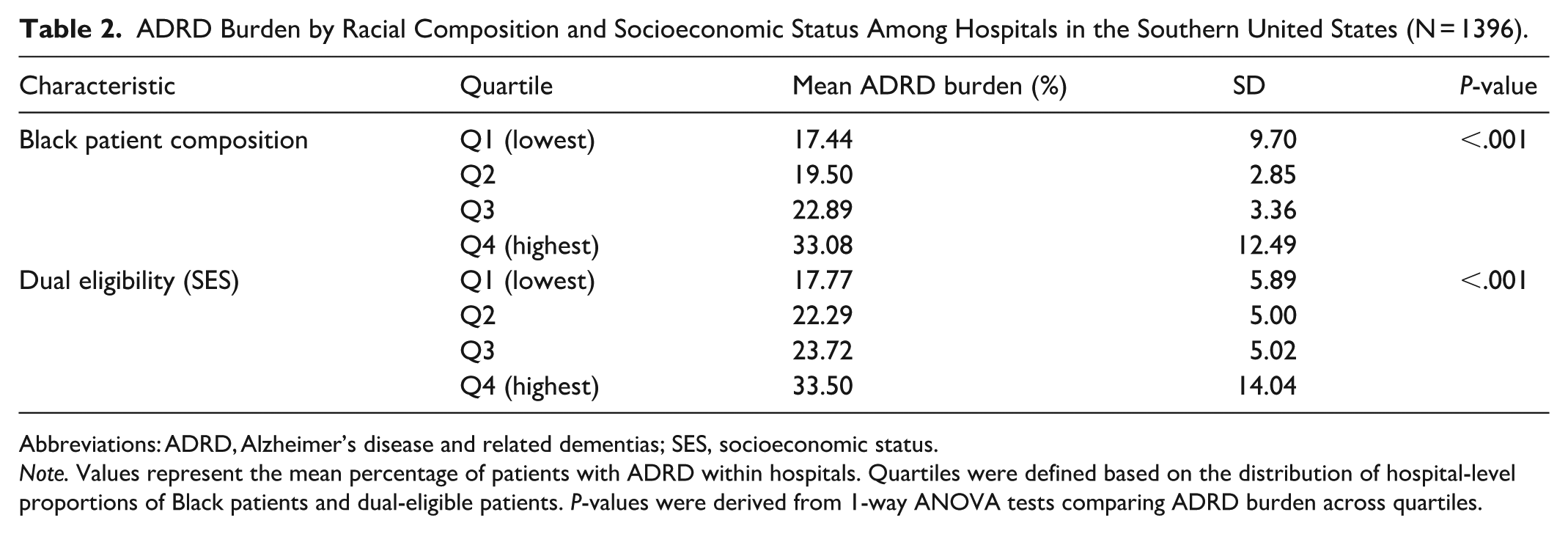
Abbreviations: ADRD, Alzheimer’s disease and related dementias; SES, socioeconomic status.
Note. Values represent the mean percentage of patients with ADRD within hospitals. Quartiles were defined based on the distribution of hospital-level proportions of Black patients and dual-eligible patients. P-values were derived from 1-way ANOVA tests comparing ADRD burden across quartiles.
Figure 1 shows the distribution of hospital-level ADRD burden across rural–urban categories. A clear gradient was observed, with rural hospitals exhibiting the highest ADRD burden, followed by micropolitan and metropolitan hospitals. Median ADRD burden increased progressively across these groups, and rural hospitals demonstrated greater variability compared to metropolitan hospitals. Micropolitan hospitals showed intermediate levels, indicating a consistent rural–urban disparity in ADRD burden.
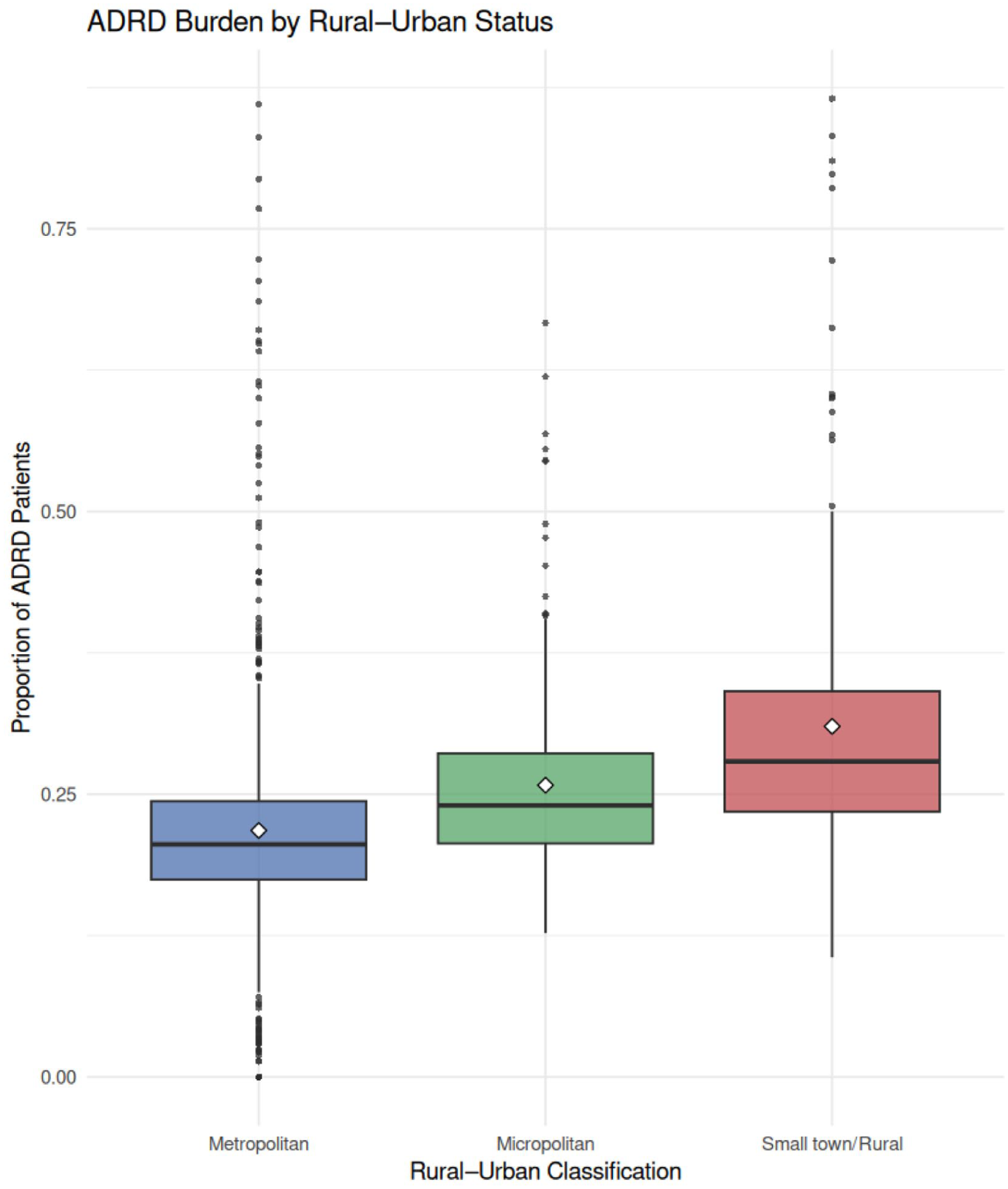
Distribution of ADRD burden by rural–urban status.
Figure 2 shows the distribution of ADRD burden across quartiles of Black patient composition. A clear increasing gradient was observed, with ADRD burden rising progressively from the lowest to the highest quartile. Hospitals in the highest quartile exhibited substantially greater ADRD burden compared to those in the lowest quartile, indicating pronounced racial disparities.
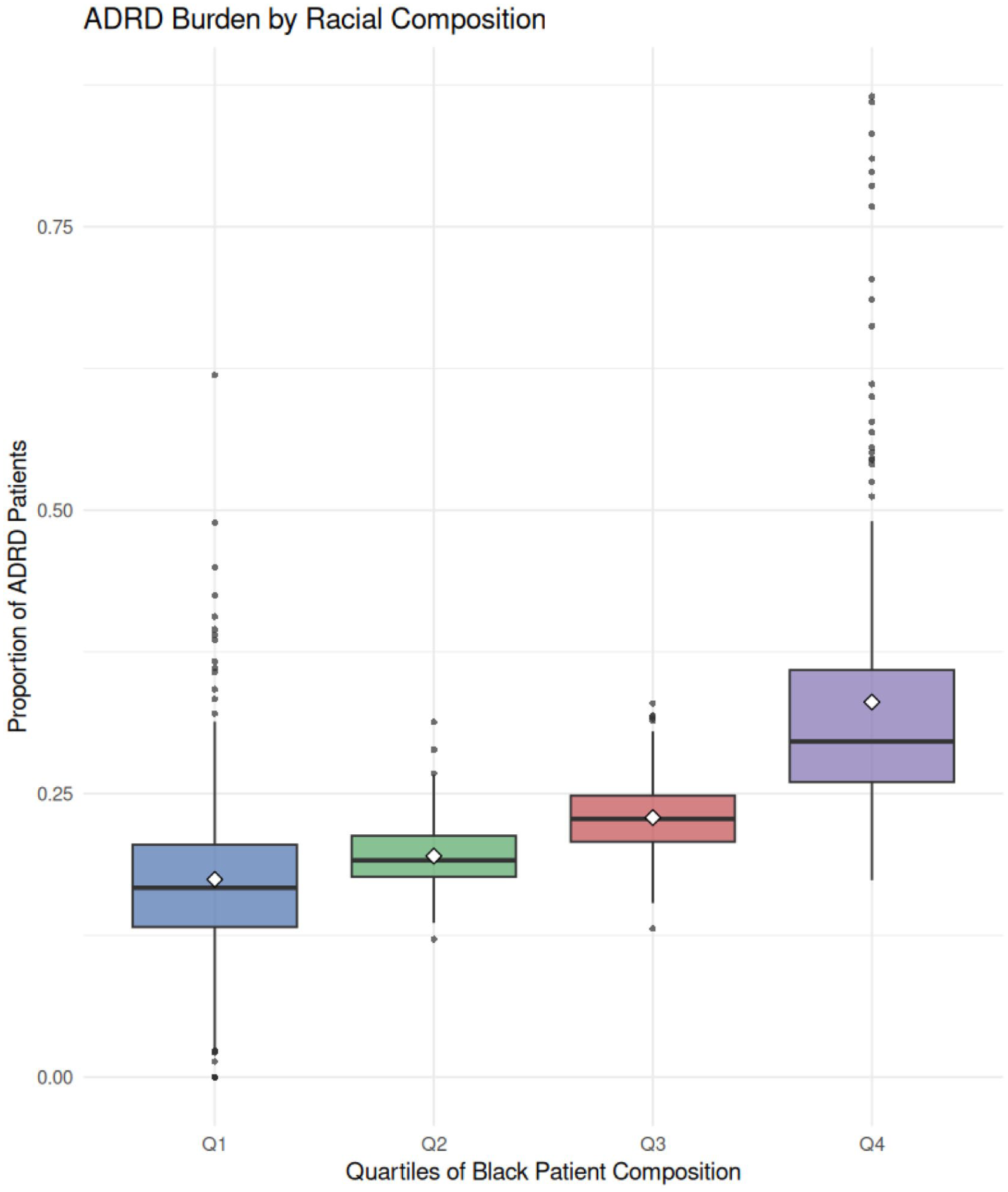
Distribution of ADRD burden by racial composition.
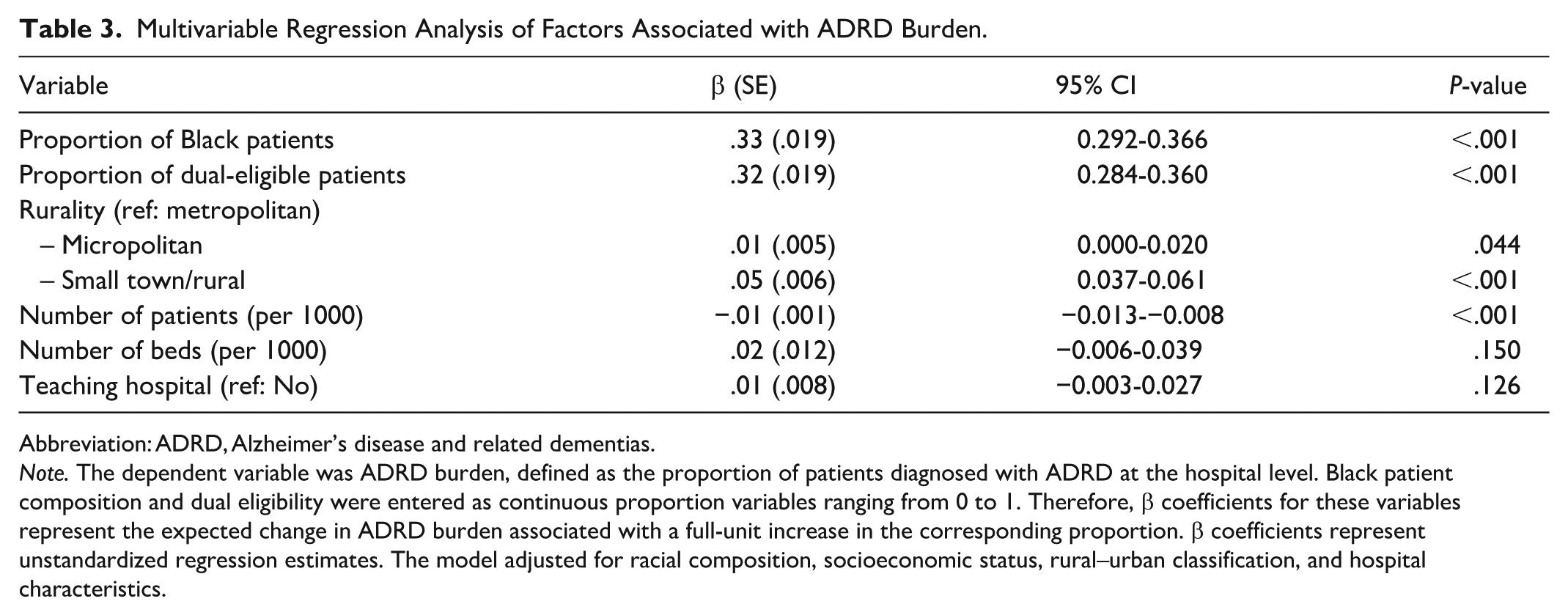
Multivariable regression analysis showed that racial composition and socioeconomic disadvantage were independently associated with ADRD burden, defined as the proportion of patients diagnosed with ADRD at the hospital level (Table 3). Black patient composition and dual eligibility were entered as continuous proportion variables ranging from 0 to 1. A higher proportion of Black patients was associated with greater ADRD burden (β = .33, 95% CI 0.292-0.366; P < .001). Similarly, a higher proportion of dual-eligible patients was associated with greater ADRD burden (β = .32, 95% CI 0.284-0.360; P < .001). Rural–urban differences were also observed. Compared with metropolitan hospitals, micropolitan hospitals had slightly higher ADRD burden (β = .01, 95% CI 0.000-0.020; P = .044), whereas small-town/rural hospitals had substantially higher ADRD burden (β = .05, 95% CI 0.037-0.061; P < .001). Among hospital characteristics, a greater number of patients was associated with lower ADRD burden (β = −.01 per 1000 patients, 95% CI −0.013-−0.008; P < .001). In contrast, number of beds and teaching status were not significantly associated with ADRD burden.
Multivariable Regression Analysis of Factors Associated with ADRD Burden.
Abbreviation: ADRD, Alzheimer’s disease and related dementias.
Note. The dependent variable was ADRD burden, defined as the proportion of patients diagnosed with ADRD at the hospital level. Black patient composition and dual eligibility were entered as continuous proportion variables ranging from 0 to 1. Therefore, β coefficients for these variables represent the expected change in ADRD burden associated with a full-unit increase in the corresponding proportion. β coefficients represent unstandardized regression estimates. The model adjusted for racial composition, socioeconomic status, rural–urban classification, and hospital characteristics.
Discussion
The current study demonstrates substantial and systematic disparities in ADRD burden across hospitals in the Southern United States. In descriptive, stratified, and multivariable analyses, a consistent gradient was apparent, with hospitals with higher proportions of Black patients, dual-eligible patients, and patients from rural areas having significantly greater burdens of ADRD. These disparities were large, with the burden of ADRD almost doubling from the lowest to the highest quartile in both racial composition and socio-economic disadvantage. These findings have direct implications for home health care services, as hospitals serving populations with higher ADRD burden are likely to face greater demand for post-acute care, care coordination, and long-term support in community settings.
Although the present study did not directly measure discharge disposition, rehospitalization, or post-acute care utilization, the concentration of ADRD burden in disadvantaged and rural-serving hospitals may indicate settings where greater home health care and community-based dementia support are likely to be needed. Hospitals serving populations with higher ADRD burden may require stronger discharge planning, caregiver education, cognitive and functional assessment, referral pathways, and coordination with home health agencies and community-based services. These implications should be interpreted as practice and planning considerations rather than direct evidence of post-acute care gaps.
These results align with and extend prior evidence of racial and socioeconomic disparities in dementia risk and care.12,13 In the United States, Black populations have consistently been shown to face a higher risk of ADRD, reflecting the cumulative effects of structural inequities and unequal access to healthcare.14,15 The current findings build on this literature by demonstrating that these disparities are not confined to individual-level risk but are also evident at the institutional level, suggesting that high-risk populations are disproportionately concentrated within specific healthcare systems.
The strong association between dual eligibility and ADRD burden further underscores the role of socioeconomic disadvantage. Individuals who are dually eligible for Medicare and Medicaid often encounter barriers to timely diagnosis, continuity of care, and access to specialized dementia services.8,16 The clear gradient observed across quartiles indicates that socioeconomic disadvantage functions as a structural determinant shaping the distribution of ADRD burden across hospitals.
Geographic disparities were also pronounced. Rural hospitals exhibited a higher ADRD burden and greater variability than metropolitan hospitals, while micropolitan hospitals demonstrated intermediate levels. This pattern is consistent with prior research showing that rural populations face limited access to dementia-related services, including diagnostic resources and specialist care.10,17 Together, these findings support the interpretation of a continuum of geographic disadvantage rather than a simple rural–urban dichotomy.
The disparities arise from multiple underlying mechanisms. Structural inequities, such as historical segregation and unequal resource distribution, may direct disadvantaged populations toward specific healthcare facilities.18 -20 The deficiency of accessible preventive services and management strategies for chronic illnesses may increase the risk of ADRD within socioeconomically disadvantaged groups.9,21 Additionally, populations in vulnerable circumstances often experience diagnostic delays and underdiagnosis of ADRD, potentially accounting for the higher burden observed at the point of care.22,23 Substantial evidence indicates that the consistency of these findings across various approaches is attributable to systemic inequities rather than methodological artifacts.
Implications for Policy and Practice
These findings have important implications for home health care delivery. Hospitals with higher ADRD burden, particularly those serving racially marginalized, socioeconomically disadvantaged, and rural populations, may represent priority settings for strengthening discharge planning and linkage to home- and community-based dementia services.24,25 Home health agencies may need to prepare for greater demand for dementia-informed care, including medication management, fall prevention, behavioral symptom monitoring, caregiver education, and coordination with primary care and specialist providers. In rural and underserved communities, limited availability of dementia specialists and community resources may place additional pressure on family caregivers and home health providers. Therefore, equity-oriented dementia care planning should include stronger referral pathways between hospitals, home health agencies, primary care clinics, caregiver support programs, and community-based organizations. Targeted investment in home health care capacity may help reduce fragmentation of care and support safer transitions for older adults with ADRD. 3
Strengths and Limitations
This study has several important strengths. First, this study used a large, multi-state dataset, enabling a thorough evaluation of hospital-level differences in ADRD burden across the Southern United States. Second, the use of multiple analytic approaches, including descriptive analyses, quartile comparisons, and multivariable regression, provides consistent evidence that enhances the reliability of the results. Third, these findings suggest that disparities in ADRD are not only driven by individual risk factors but are also structurally embedded within healthcare institutions.
Several limitations should also be acknowledged. The cross-sectional design limits causal inference and precludes assessment of temporal relationships. In addition, the use of hospital-level measures may obscure within-hospital heterogeneity and does not capture individual-level clinical and social factors that may influence ADRD risk. Although we adjusted for key hospital characteristics, residual confounding from unmeasured factors cannot be excluded. Finally, the focus on hospitals in the Southern United States may limit generalizability to other regions with different demographic and healthcare system contexts.
Footnotes
Ethical Considerations
This study used publicly available, de-identified data from the Inter-university Consortium for Political and Social Research (ICPSR). As the data do not contain personally identifiable information, this study was considered exempt from institutional review board (IRB) review in accordance with federal regulations.
Author Contributions
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are publicly available from the Inter-university Consortium for Political and Social Research (ICPSR). The dataset is publicly available and can be downloaded without restriction. Data are accessible through the ICPSR repository subject to their terms of use.