
Abstract
Background:
Homecare rehabilitation providers serve clients at home and in the community. Like homecare providers of other disciplines, they were required to use facial protective equipment (FPE) during the SARS-CoV-2 pandemic. Increased FPE usage may also be required during future respiratory disease outbreaks, epidemics, and pandemics. With no known studies exploring homecare rehabilitation providers’ FPE adherence, this pilot study explored factors influencing their adherence to respiratory and eye protection.
Methods:
Cross-sectional online surveys were completed by rehabilitation providers from 2 large not-for-profit homecare agencies in Ontario, Canada, in January 2023. Factors influencing respiratory and eye protection adherence were examined separately using descriptive, bivariate, and logistic regression techniques. Conventional content analysis was used to explore open-text responses.
Results:
Rehabilitation providers (n = 124) reported adherence rates of 77% and 53% to respiratory and eye protection, respectively. Higher respiratory protection adherence was associated with previous exposure while lower adherence was associated with negative mental health effects due to past exposure. Eye protection adherence varied by provider occupation. Higher adherence to eye protection was associated with working 35 hours or less and with using face shields. Qualitative findings emphasized training and FPE accessibility to support adherence.
Discussion:
This pilot study revealed initial opportunities to support homecare rehabilitation providers’ adherence to FPE. Early insights suggest mental health support, easy FPE availability, and training opportunities may increase adherence. Hours worked, eye protection choice, and occupation may also be important factors. Future research is needed to deepen our understanding of the insights observed in this pilot study.
Keywords
Introduction
Healthcare workers’ (HCWs) use of facial protective equipment (FPE), including respiratory and eye protection, can prevent the transmission of infectious diseases, including SARS-CoV-2 (COVID-19 1 ), protecting HCWs and their patients/clients.2-5 During the recent SARS-CoV-2 pandemic, the use of FPE was required by many HCWs who had not previously used it on a regular basis. Heightened use may again be required during future outbreaks, epidemics and pandemics. While factors influencing HCWs’ use of FPE and adherence to usage guidelines have been studied extensively in institutional settings, 6 there has been minimal work focused on the homecare setting. Existing studies in home care have examined FPE adherence by nurses and personal support workers (PSWs),7-9 but none have yet explored the FPE-related experiences of rehabilitation providers. Even beyond home care, only 1 SARS-CoV-2 pandemic-era study has characterized rehabilitation providers’ use of FPE. This study of physiotherapists across all care settings found that 92% and 24% of respondents used face masks and goggles, respectively, 10 but did not separate usage rates by sector, nor did they specifically explore factors influencing FPE adherence.
Rehabilitation providers play a crucial role in home care that is distinct from nursing and personal support work. This provider group can include occupational therapists, physiotherapists, occupational and/or physical therapy assistants, dietitians, speech-language pathologists, and social workers. They provide care in clients’ homes and community locations (e.g., clinics, schools), promoting rehabilitation following injury or illness and supporting clients’ functioning in activities of daily living. Some characteristics unique to the homecare environment which may impact how FPE is used and managed include daily travel between community-based clients, the need to collect and travel with any necessary equipment, and navigating the complex physical and social conditions associated with working within clients’ homes. 11
To promote homecare rehabilitation providers’ safety, the objective of this pilot study was to gain initial insight into the individual, environmental, and organizational factors that influenced their self-reported adherence to FPE use during the SARS-CoV-2 pandemic. This pilot study may also be used to inform future studies exploring FPE adherence among a larger population of homecare providers. With no known studies exploring FPE adherence among this population, this study begins to address an important literature gap.
Methods
Design and Participants
A cross-sectional, electronic survey was distributed to rehabilitation providers at 2 large, not-for-profit homecare agencies in Ontario, Canada. Eligible participants included occupational therapists, physiotherapists, dietitians, speech-language pathologists, social workers, occupational and/or physiotherapy assistants, and communications disorders assistants. Based on a prior study using a similar survey, 8 a sample size of 160 participants (80 per agency) was targeted to detect large differences between populations. The Univeristy of Toronto’s Research Ethics Board reviewed and approved this study (REB#: 43647).
Rehabilitation providers were invited by email to participate in a confidential, online survey via REDCap,12,13 between January 11 and 24, 2023. They were provided a digital study information letter which included the study team’s contact information; individuals could participate in the survey after selecting “I consent to participate.” Participants received a $20 gift card honorarium if they chose to share their email address for this purpose.
Survey Tool
The study used an adapted homecare version of the Facial Protection Questionnaire (FPQ) originally developed by Nichol et al.14,15 The original survey drew on the PRECEDE (Predisposing, Reinforcing and Enabling Constructs in Educational Diagnosis and Evaluation) model for health behavior to identify individual, organizational, and environmental influences on acute-care nurses’ adherence to FPE.14,15 The FPQ was adapted for use in home care during the SARS-CoV-2 pandemic by King et al through a pilot then large-scale study.8,9 They modified the tool to account for homecare-specific contextual conditions and terminology8,9; the inclusion of PSWs in addition to nurses8,9; gender and ethnicity 9 ; and SARS-CoV-2-specific factors (e.g., contemporaneous public health guidelines regarding transmission at each timepoint).8,9 For the present study, the FPQ for home care was further updated for use with rehabilitation providers and existing items were updated for clarity. Additional items included proportion of virtual care, preferred eye protection type, combined respiratory (surgical mask or respirator) protection adherence, and an open-text item to gather suggestions for promoting future FPE adherence. Participants were asked to respond based on their practices as of May 2022; governmental FPE use guidelines had been updated on June 11, 2022. 16 The 154-item FPQ for homecare rehabilitation providers is included as a Supplemental File.
Survey Scales
Like previous questionnaire versions, the survey used 4 response types. 9 Most survey items used a frequency scale (always/mostly/sometimes/rarely/never or daily/weekly/monthly/rarely/never) or an agreement scale (strongly agree/agree/neutral/disagree/strongly disagree). Knowledge-based items included a “don’t know” option while an “N/A, I don’t use this” option was added to the barriers-related items. Categorical items allowed respondents to select 1 or multiple, responses.
Definitions
Outcomes
Respiratory protection adherence (3 items) was defined as always using a mask or respirator when within 2 m of clients. Eye protection adherence (3 items) was defined as always using a face shield or goggles when within 2 m of a client.
Individual Factors
Gender, age, ethnicity, primary employer, highest education, occupation, length of employment, hours, proportion of virtual care, method of travel, and eye protection choice were measured using single items. Participants could select multiple gender and ethnic identity response options. Individuals could also indicate whether they held any formal leadership roles or worked with multiple employers.
Frequent pre-pandemic use of respiratory protection was defined by choosing daily, weekly, or monthly for mask and respirator usage (2 items). Pre-pandemic eye protection adherence (3 items) was defined as choosing always/mostly across all related items.
High knowledge of transmission (7 items), perceived efficacy of FPE (4 items), knowledge of FPE (6 items), and perception of risk (3 items) were defined by agreeing/strongly agreeing (or disagreeing/strongly disagreeing) to all included items.
Respondents indicated whether they were exposed to a workplace respiratory infectious disease; became sick due to workplace exposure; experienced negative physical effects from workplace exposure; and/or experienced negative mental health effects from workplace exposure by selecting agree/strongly agree to each item. Individuals reported whether they knew someone who had been exposed to a workplace respiratory infectious disease, with an opportunity to specify their relationship. The number of barriers reported was the sum of barriers to use identified across each FPE type (29 items). Individuals could specify if they sought out solutions (on their own or via supervisors, healthcare, or other means) to address identified barriers (16 items).
Environmental Factors
Client location (where participants most often provided care) was dichotomized as private homes/apartments versus other settings (clinics, congregate care, hospitals, or other). Availability of FPE (6 items) and convenience of access to FPE (2 items) were defined as high if the participant agreed/strongly agreed to all related items. Media influence (2 items) was considered high if participants agreed/strongly agreed to either related item.
Organizational Factors
Training related to COVD-19, its transmission, and FPE were measured using 7 items; full training was defined as responding yes to all. Individuals could indicate whether they received a fit test. Organizational support (6 items), absence of job hindrances (3 items), and team communication and support (7 items) were categorized as high if the participant agreed/strongly agreed to all related items.
Statistical Analysis
Surveys with missing data were excluded from quantitative analyses; exceptions included items where a non-response was equivalent to “prefer not to say,” “N/A,” or “No.” Descriptive and bivariate comparisons were conducted to assess the relationship of each variable with respiratory and/or eye protection adherence. T-tests and Fisher’s Exact tests were used for continuous and categorical data, respectively. Unadjusted odds ratios were calculated, with Haldane’s correction applied for cell counts of 0. Logistic regression models were created for respiratory and eye protection adherence with predictors included based on their bivariate significance, cell size, and model impact. Adjusted odds ratios were calculated for each predictor. A significance level of P < .05 was used. Sensitivity analysis included removing each variable individually to check model robustness. Quantitative analysis was performed using RStudio (Version 2022.07.1+554, Posit Software, PBC, Boston, MA, USA); R version 4.3.2, The R Foundation for Statistical Computing, Vienna, Austria).
Qualitative Analysis
Conventional content analysis 17 was conducted on responses to the free-text item asking for recommendations to support future FPE adherence. Responses were uploaded into Excel® for Microsoft 365 (Microsoft Corporation, Redmond, WA, USA). Line-by-line, inductive coding was conducted by a single coder to identify the initial coding scheme, and codes were subsequently categorized based on related emergent codes. The resulting categories and example quotations were discussed with the study team for interpretation and comparison to quantitative findings.
Results
Sample
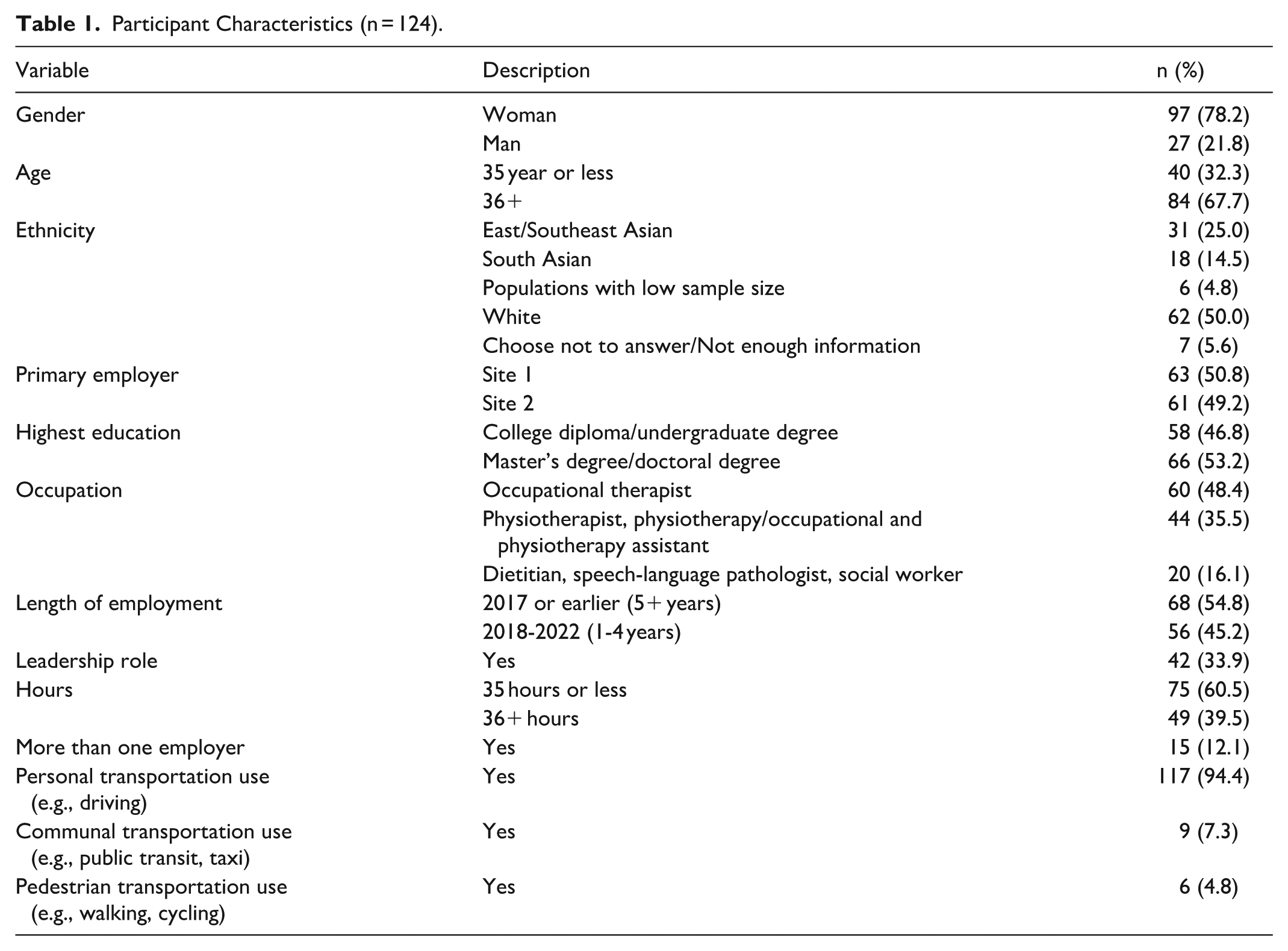
There were 124 complete surveys for quantitative analysis. There were 194 individuals who consented to participate, of which 32 did not finish the survey. Of the remaining 162 responses, 8 respondents did not answer the outcome item; an additional 30 respondents did not provide answers for one or more constructs, leaving 124 surveys with sufficiently complete data for inclusion in the analysis. These participants were equally divided between sites (site 1: 50.8%, site 2: 49.2%; Table 1). Individuals were primarily occupational therapists (48.4%); physiotherapists and physiotherapy/occupational and physiotherapy assistants (35.5%) with the remainder (16.1%) comprising dietitians, speech-language pathologists, and social workers. Participants were 78.2% women and 21.8% men, with no respondents identifying as gender-diverse. Two thirds were over 35 years of age. Most individuals identified as White (50.0%), followed by East/Southeast Asian (25.0%), and South Asian (14.5%).
Participant Characteristics (n = 124).
Adherence
Participants reported being more adherent to respiratory protection (77.4%, n = 96) than eye protection (53.2%, n = 66). Notably, some individuals (18.2%, n = 12) who were always adherent to eye protection were not always adherent to respiratory protection.
Respiratory Protection
No factors showed bivariate associations with respiratory protection adherence (Table 2), however, 2 factors were significant in the regression model (Table 3). Those with workplace exposure to respiratory infectious disease had more than 3 times the odds of reporting adherence (adjusted Odds Ratio [aOR]: 3.47, 95% Confidence interval [CI] 1.14-10.57). However, those who experienced negative mental health effects due to a work-related exposure had 83% lower odds of reporting adherence (aOR: 0.17, 95% CI: 0.04-0.68).
Relationship Between Respiratory Protection and Eye Protection Adherence With Individual, Environmental, and Organizational Factors.
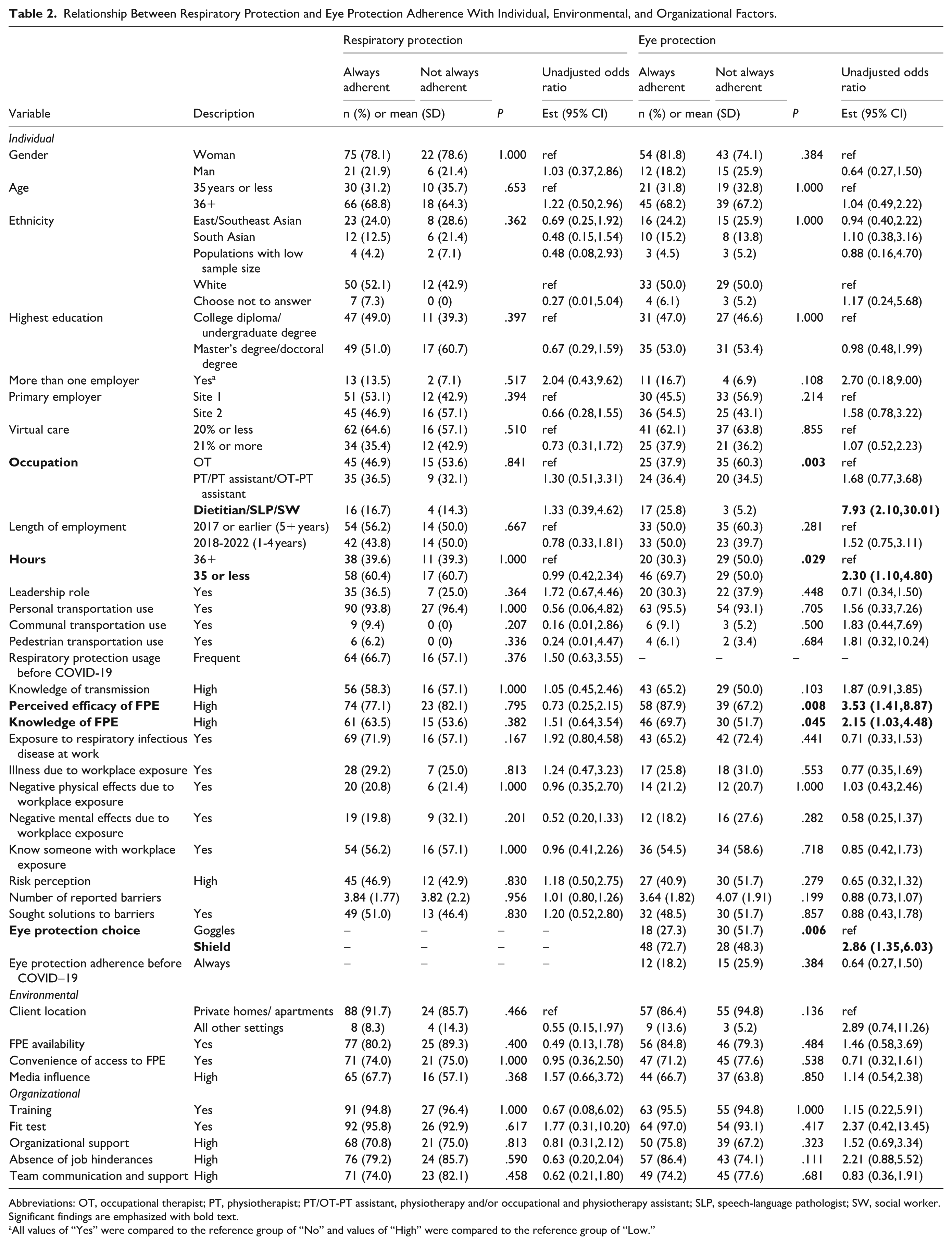
Abbreviations: OT, occupational therapist; PT, physiotherapist; PT/OT-PT assistant, physiotherapy and/or occupational and physiotherapy assistant; SLP, speech-language pathologist; SW, social worker. Significant findings are emphasized with bold text.
All values of “Yes” were compared to the reference group of “No” and values of “High” were compared to the reference group of “Low.”
Logistic Regression Assessing Factors Associated With Respiratory Protection Adherence.
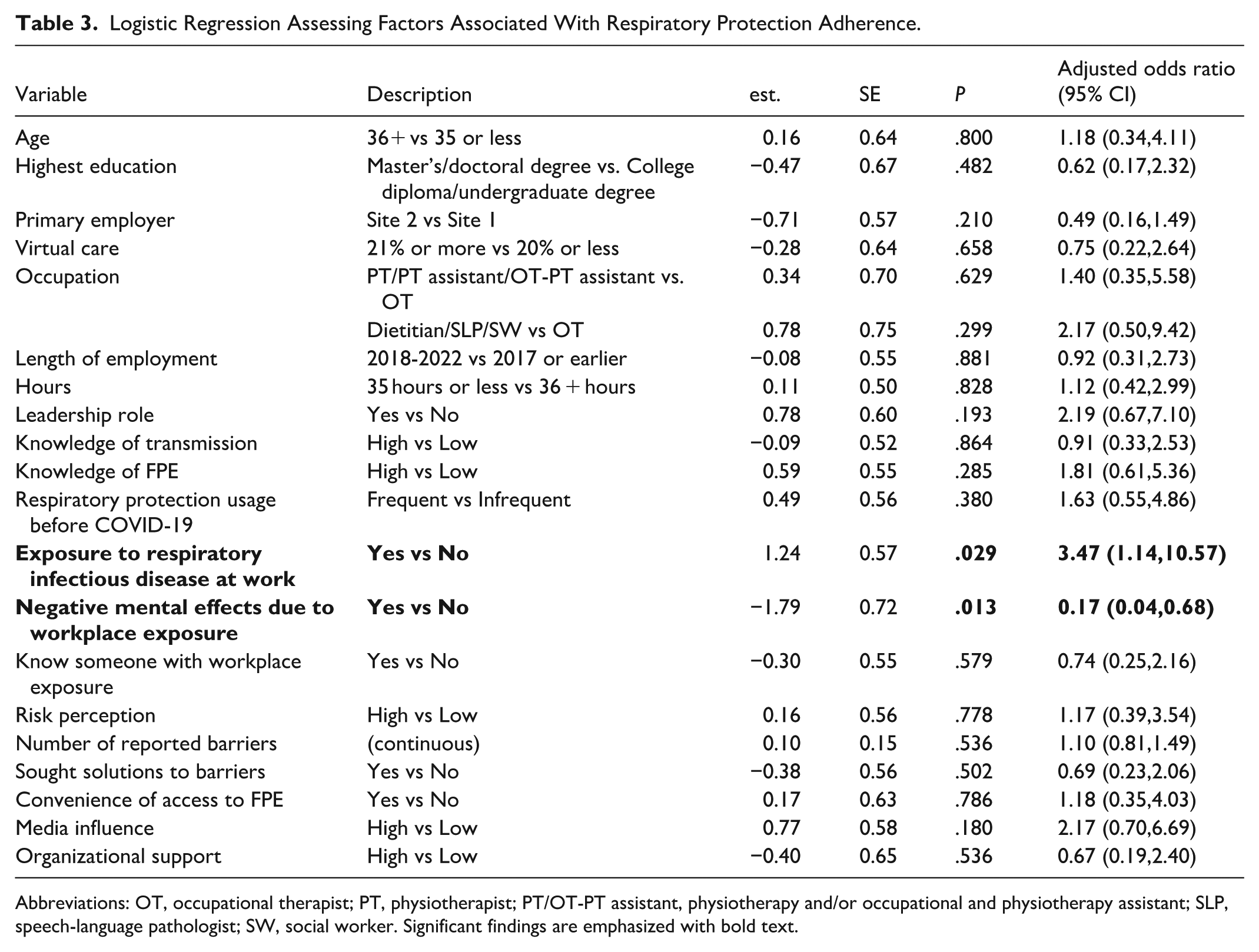
Abbreviations: OT, occupational therapist; PT, physiotherapist; PT/OT-PT assistant, physiotherapy and/or occupational and physiotherapy assistant; SLP, speech-language pathologist; SW, social worker. Significant findings are emphasized with bold text.
Eye Protection
Five factors showed significant bivariate associations with eye protection adherence (Table 2), of which occupation, hours worked, and eye protection choice remained significant in the regression model (Table 4). Dietitians, speech-language pathologists and social workers had almost 14 times the odds of reporting adherence compared to occupational therapists (aOR: 13.66 95% CI: 2.30-81.05). Individuals who worked 35 hours or less per week had nearly 4 times the odds of reporting adherence compared to those who worked more hours (aOR: 3.98, 95% CI: 1.39-11.41). Finally, those who used face shields had 3.4 times the odds of reporting adherence compared to those who used goggles (aOR: 3.43, 95% CI: 1.21-9.67).
Logistic Regression Assessing Factors Associated With Eye Protection Adherence.
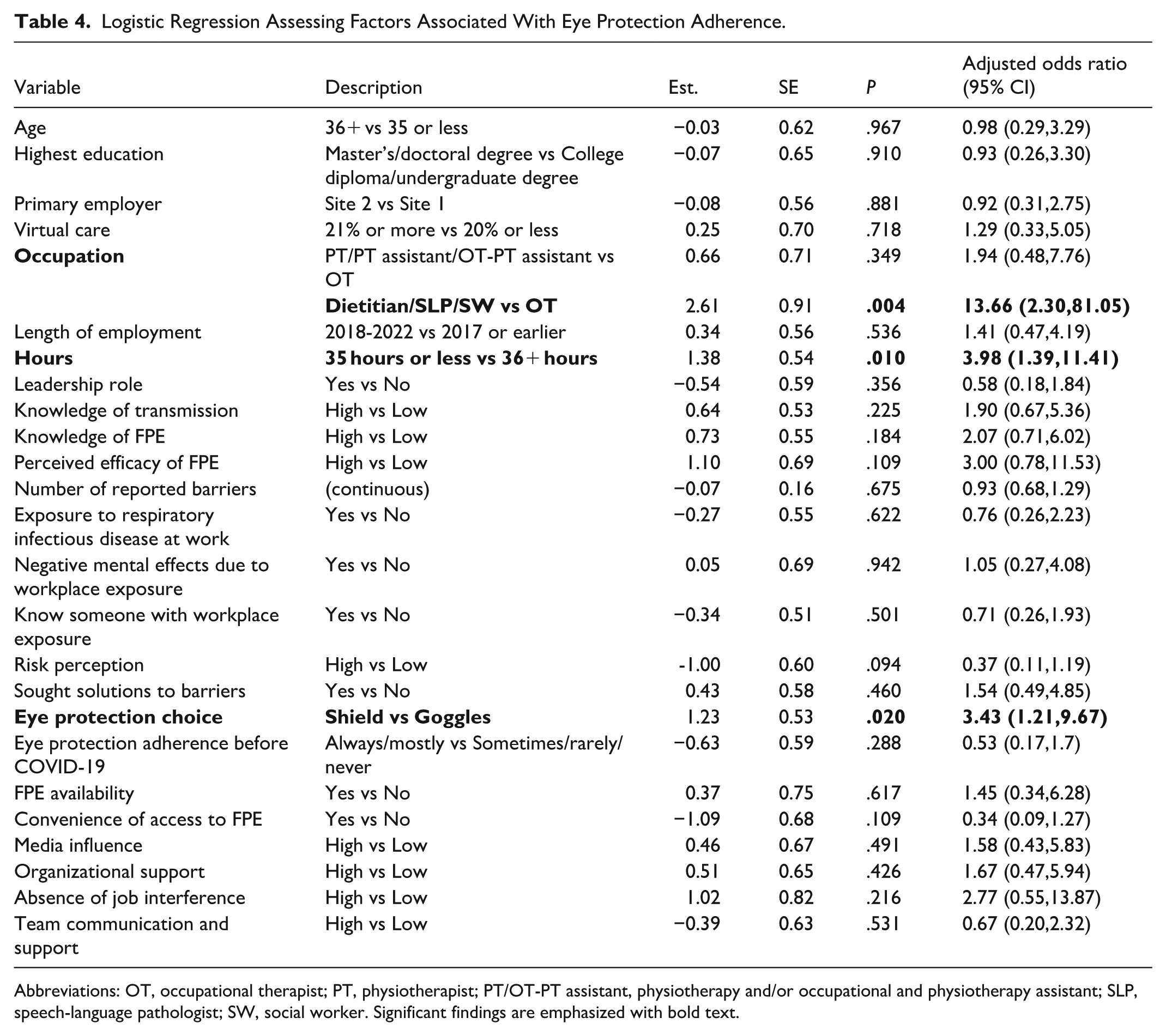
Abbreviations: OT, occupational therapist; PT, physiotherapist; PT/OT-PT assistant, physiotherapy and/or occupational and physiotherapy assistant; SLP, speech-language pathologist; SW, social worker. Significant findings are emphasized with bold text.
Qualitative Analysis
Of the 194 individuals who consented to participate, 70 responded to the free-text item which asked for recommendations to support future FPE adherence. Responses were brief, ranging from a few words to a few sentences.
The most common recommendations pertained to ease of FPE access. Multiple participants recommended that FPE be provided at convenient community pick-up points or mailed to providers’ homes. Suggestions also referenced the early days of the pandemic, when, like healthcare providers across all care sectors, homecare rehabilitation providers faced FPE shortages.
Initial shortages in availability were an issue. There needs to [be] a large supply available and staff need to be able to take a large enough supply at one time so it is not necessary to travel to the pick-up location or office more than necessary as that travel time takes a significant amount of time from front line staff life and is not compensated for.
Some further suggested that providers receive compensation for their time spent picking up supplies: “If you don’t pay staff extra time for time lost picking up, donning & doffing PPE, some will opt to avoid PPE or cut [client] visits short instead.”
Several participants provided recommendations to improve training and communication clarity to support FPE adherence. Recommendations included various forms of education on the infection risk associated with a new pathogen and the proper use of FPE to protect against exposure during onboarding and through automated reminders/emails to reinforce these messages. Participants commented on the importance of clarity and accessibility in organizational policies and guidelines. Additionally, a few participants suggested client-facing education, such as one comment calling for a “client education brochure outlining [the] importance of PPE for both client and service provider.” These participants believed that information provision could both encourage clients to use FPE and increase client awareness of expectations for FPE use by providers.
Beyond the pandemic context, some participants highlighted strategies for continued use, such as: [Agencies] should have a good emergency stock of PPE on hand at all times, and promote regular use of PPE even during non-pandemic times to ensure staff are comfortable and used to using it.
Finally, participants identified diverse needs and preferences which should be considered when selecting FPE. In addition to the general need for sufficient FPE supplies, some participants specifically suggested greater respirator access: “provide better access to N95 [respirators].” Respondents also highlighted the need to consider compatibility with eyeglasses and masks that can fit different face shapes and sizes: “[agencies] should ensure that they have a variety of different options for facial protective equipment (different models and sizes of goggles and face shields) to accommodate all providers.”
Discussion
This pilot study is the first to specifically explore factors influencing FPE adherence among homecare rehabilitation providers. Rehabilitation providers’ adherence to respiratory protection (77%) and eye protection (53%) were lower than the range of adherence rates previously reported for homecare nurses and PSWs (respiratory: 89%-96%8,9; eye: 64%-73%7-9). Compared to one study of physiotherapists across care sectors, homecare rehabilitation providers reported lower adherence to respiratory protection (77% vs 92%), however, eye protection rates were twice as high (53% vs 24%). 10
Although respiratory protection adherence was higher for providers who reported workplace infectious disease exposures, negative mental health effects related to workplace exposures were significantly associated with lower respiratory protection adherence. This is important given the prevalence of adverse mental health impacts experienced by HCWs throughout the pandemic.18-21 These results align with findings among homecare nurses and PSWs. 9 They also align with previous findings related to “pandemic fatigue” (a reduction in motivation to follow COVID-19-related precautions 22 ) among the general population; individuals with greater pandemic fatigue were more likely to report a history of SARS-CoV-2 infection, greater stress related to SARS-CoV-2, more strenuous efforts to cope, 23 and lower adherence to mask use.24,25 Literature suggests that both emotional states (transient experiences) and traits (stable patterns) influence HCWs’ risk-related decision-making,26,27 with different aversive emotions associated with different behaviors.26,28 Heyhoe et al 26 note that anxiety increases risk aversion in clinical decision-making, while anger increases risk-taking. Future research should explore, with greater specificity, the mental health impacts of infectious disease exposures to improve understanding of how these influence FPE adherence. This may reveal opportunities for homecare agencies to support FPE adherence by prioritizing rehabilitation providers’ mental health through employee assistance programs for those with immediate concerns as well as comprehensive workplace programming which extends beyond immediate assistance and seeks to create an environment that supports workers’ mental health. 29
Eye protection adherence was associated with different individual factors than respiratory protection. The group of dietitians, speech-language pathologists, and social workers was more adherent than occupational therapists. This may be partially explained by differences in their job tasks; these providers likely perform their work in closer face-to-face proximity to the client, where increased awareness of respiratory droplet transmission may promote adherence. The association between working 35 hours or less and reporting higher eye protection adherence has not previously been observed among homecare nurses and PSWs.8,9 Providers who used face shields instead of goggles were more adherent to eye protection; additional work is required to understand whether this is an individual choice or influenced by organizational and environmental factors. These findings suggest that occupation-specific training and ensuring that face shields are available may promote adherence.
Although neither environmental nor organizational factors were significant in the quantitative results, qualitative findings highlighted participants’ requests for easy access to appropriate FPE and related information and training. This is consistent with previous homecare literature where available and accessible FPE were significantly associated with higher adherence among PSWs and nurses, 9 while availability of related supplies was associated with higher adherence to infection prevention and control (IPAC) protocols by nurses.7,30 Training has not been previously associated with adherence in home care.7-9 However, in a study among acute-care nurses which used a similar questionnaire, training was significantly associated with adherence 15 ; another study found that the recency of training was associated with IPAC adherence during the SARS-CoV-1 epidemic. 31 Further research can explore how training and information provision might support FPE adherence among homecare rehabilitation providers.
This pilot study is the first to focus on homecare rehabilitation providers, however, its cross-sectional nature and comparatively small sample size should be considered when interpreting the initial insights observed in this pilot study. The survey was voluntary and reflects self-reported behaviors. Individuals with pre-existing interests or beliefs related to FPE may have been more likely to take part. Social desirability and recall effects may have resulted in an overestimation of adherence rates. The survey was conducted within 2 large homecare agencies in Ontario, Canada; rehabilitation providers working in smaller agencies, through self-employment/other arrangements, or in other jurisdictions within and outside of Canada, may face different influences on their FPE adherence. This may limit the generalizability of findings to those working in other jurisdictions and employment frameworks.
Conclusion
This pilot study addressed a gap in research related to homecare rehabilitation providers’ FPE adherence. The association between poorer adherence and negative mental health effects of past exposures was similar to findings among other homecare providers and suggests that there may be opportunities to support adherence through the provision of effective mental health promotion and supports. Associations between eye protection adherence and occupation may suggest opportunities for occupation-specific interventions. Further study is required to understand the reasons underlying higher adherence by face shield users than goggles users and higher adherence by those working 35 hours or less per week. Qualitative insights highlighted the importance of FPE accessibility and training. Differences in factors influencing FPE adherence in this pilot study, compared to those among homecare nurses and PSWs, suggest that homecare rehabilitation providers may have unique needs, motivations, and considerations that influence their adherence to respiratory and eye protection. These findings provide a valuable starting point for exploring how targeted interventions could support higher FPE adherence by homecare rehabilitation providers.
Supplemental Material
sj-pdf-1-hhc-10.1177_10848223261459610 – Supplemental material for Factors Affecting Self-Reported Facial Protective Equipment Adherence by Rehabilitation Providers in Home Care During the SARS-CoV-2 Pandemic: A Cross-Sectional Pilot Study
Supplemental material, sj-pdf-1-hhc-10.1177_10848223261459610 for Factors Affecting Self-Reported Facial Protective Equipment Adherence by Rehabilitation Providers in Home Care During the SARS-CoV-2 Pandemic: A Cross-Sectional Pilot Study by Travis A. Van Belle, Cara Evans, Emily C. King, Justine Giosa, Katherine A. P. Zagrodney, Sandra M. McKay, Kathryn A. Nichol and D. Linn Holness in Home Health Care Management & Practice
Supplemental Material
sj-pdf-2-hhc-10.1177_10848223261459610 – Supplemental material for Factors Affecting Self-Reported Facial Protective Equipment Adherence by Rehabilitation Providers in Home Care During the SARS-CoV-2 Pandemic: A Cross-Sectional Pilot Study
Supplemental material, sj-pdf-2-hhc-10.1177_10848223261459610 for Factors Affecting Self-Reported Facial Protective Equipment Adherence by Rehabilitation Providers in Home Care During the SARS-CoV-2 Pandemic: A Cross-Sectional Pilot Study by Travis A. Van Belle, Cara Evans, Emily C. King, Justine Giosa, Katherine A. P. Zagrodney, Sandra M. McKay, Kathryn A. Nichol and D. Linn Holness in Home Health Care Management & Practice
Footnotes
ORCID iDs
Ethical Considerations
This study was performed at VHA Home HealthCare and SE Health. The study was reviewed and approved by the Research Ethics Board at the University of Toronto (REB# 43647).
Consent to Participate
Written, informed consent was collected. Individuals were provided with study information and had to select “I consent to participate” before beginning the survey.
Author Contributions
King, McKay, Giosa, Nichol, and Holness contributed to the conception and design of the study. King and Giosa were responsible for data acquisition. All authors contributed to analysis and interpretation. Van Belle, Evans, King, and Giosa were responsible for drafting the manuscript; Zagrodney, McKay, Nichol, and Holness revised it critically for important intellectual content. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centre for Research Expertise in Occupational Disease, which is funded by the Ontario Ministry of Labour, Immigration, Training and Skills Development [grant numbers 512389-Subgrant 9, 512389-Subgrant 10]. The views expressed are those of the authors and do not necessarily reflect the views of the Province.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Van Belle, Evans, King, Giosa, Zagrodney, McKay, and Nichol were each employed by organizations that hosted this study. Holness is Director of the Centre for Research Expertise in Occupational Disease which provided funding for this study. The Centre for Research Expertise in Occupational Disease is funded by the Ontario Ministry of Labour, Immigration, Training and Skills Development. The views expressed are those of the authors and do not necessarily reflect the views of the Province.
Data Availability Statement
In accordance with REB approval, to ensure participant confidentiality, data is not available for sharing.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.