
Abstract
Background:
Oncologic emergencies in critically ill cancer patients frequently require rapid, real-time assessment of tumor responses to therapeutic interventions. However, conventional imaging modalities such as computed tomography and magnetic resonance imaging are often impractical in intensive care units (ICUs) due to logistical constraints and patient instability. Super-resolution ultrasound (SR-US) imaging has emerged as a promising noninvasive alternative, facilitating bedside evaluation of tumor microvascular dynamics with exceptional spatial resolution. This study assessed the clinical utility of real-time SR-US imaging in monitoring tumor perfusion changes during emergency management in oncological ICU settings.
Methods:
In this prospective observational study, critically ill patients with oncologic emergencies underwent bedside SR-US imaging before and after the initiation of emergency therapy (e.g., corticosteroids, decompression, or chemotherapy). SR-US was employed to quantify microvascular parameters, including perfusion density and flow heterogeneity. Data processing incorporated artificial intelligence for real-time vessel segmentation and quantitative analysis.
Results:
SR-US imaging successfully detected perfusion changes within hours of therapy initiation. A significant correlation was observed between reduced tumor perfusion and clinical improvement, including symptom relief and shorter ICU stay. This technology enables visualization of microvessels as small as 30 µm, surpassing conventional ultrasound limits. No adverse events were reported with the use of contrast microbubbles. In addition, SR-US imaging reduces the need for transportation to radiology departments, thereby optimizing ICU workflow.
Conclusions:
Real-time SR-US imaging offers a novel, bedside-compatible method for evaluating tumor vascular response during the acute phase of oncological emergencies. Its integration into ICU care pathways could enhance timely decision-making, reduce reliance on static imaging, and support personalized cancer management. Further multicenter validation is required.
Keywords
Introduction
Oncologic emergencies constitute a range of clinical conditions that emerge directly from malignancies or as complications arising from their treatment. These emergencies are life-threatening and necessitate rapid, precise diagnosis and immediate intervention. Examples include superior vena cava syndrome, spinal cord compression, airway obstruction due to tumor mass, hypercalcemia of malignancy, tumor lysis syndrome, and acute hemorrhage, all of which may occur in patients with advanced or aggressive cancers. In such critical contexts, particularly within intensive care units (ICUs), timely assessment of tumor status and response to therapy is crucial for guiding clinical decision-making and enhancing patient outcomes. 1
Imaging plays a pivotal role in the diagnosis and management of oncological emergencies. Conventional imaging techniques, such as computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET), offer essential anatomical and functional insights. Nevertheless, these modalities present inherent limitations, particularly within ICU settings. Transporting critically ill patients to imaging facilities poses considerable logistical and safety challenges for medical personnel. Furthermore, delays in image acquisition and interpretation can impede timely clinical decision-making. In addition, the repeated exposure to ionizing radiation from CT and PET scans raises concerns for patients requiring frequent imaging. 2
Ultrasound imaging presents a safer and more accessible option for bedside imaging in ICU settings. It is noninvasive, free from ionizing radiation, portable, and relatively cost-effective. Nevertheless, conventional ultrasound is constrained by the diffraction limit, which restricts its spatial resolution. Excluding patients with expected survival <24 h may have skewed the population toward more stable people, thus underestimating the degree of perfusion impairment encountered in late-stage oncologic crises. These limitations pose a significant challenge when attempting to visualize fine vascular structures or detect subtle changes in tumor perfusion, both of which are critical for understanding the dynamic changes occurring during oncologic emergencies. 3
Super-resolution ultrasound (SR-US) imaging represents a significant advancement in overcoming the resolution constraints inherent in traditional ultrasound techniques. SR-US achieves subwavelength imaging resolution through the utilization of microbubble contrast agents and high-frame-rate imaging, in conjunction with advanced postprocessing algorithms. By meticulously tracking the trajectories of individual microbubbles, SR-US reconstructs highly detailed vascular maps with a spatial resolution exceeding 30 µm, thereby surpassing the conventional resolution limits of ultrasound. This capability enables clinicians to visualize tumor microvasculature, evaluate perfusion, and monitor vascular remodeling in real time.4,5
One pathological feature of many oncologic crises is altered vascular function. For example, in superior vena cava syndrome, mediastinal tumors compress the superior vena cava, impairing collateral vessel development and venous return. Neoplastic invasion causes edema and inflammatory alterations in spinal cord compression, sometimes accompanied by a disturbance in local perfusion. The effectiveness of treatment may be informed by tracking these vascular events in real time, such as the increase in blood flow after decompression surgery or the decrease in tumor mass after steroid medication. 6
The effectiveness of SR-US in evaluating tumor vasculature in outpatient settings, namely in cases of liver, prostate, and breast cancer, has been shown by a number of preclinical investigations and early phase clinical trials. Nevertheless, there is still a dearth of information about its real-time use in the ICU, particularly for patients receiving emergency cancer treatments. Traditional imaging is limited in the ICU due to the patients’ frequent hemodynamic instability, need for constant monitoring, and ventilation. With its bedside capacity and exceptional resolution, SR-US provides a novel approach to real-time tumor evaluation in this situation. 7
Furthermore, the processes for image collecting and analysis have been substantially improved by the incorporation of machine learning algorithms and artificial intelligence (AI) into SR-US platforms. Perfusion quantification, vessel segmentation, and microbubble localization may all be automated with AI algorithms. This facilitates almost immediate clinical decision making in addition to increasing image interpretation speed and reliability. This reactivity can save lives in critical care, when there are limited treatment windows and fast physiological decline. 8
Therapeutic measures such corticosteroids, radiation, chemotherapy, and surgical decompression are used in oncologic crises with the goal of quickly reducing tumor burden or easing blockage. Changes in the tumor’s vascular architecture and tumor perfusion frequently indicate how well these therapies are working. By providing real-time measurement of these characteristics, SR-US may enable doctors to determine therapy response in a matter of hours as opposed to days. This time advantage is essential for directing the early escalation or de-escalation of treatment, reducing adverse effects, and improving patient outcomes. 9
SR-US has many drawbacks in spite of its benefits. Contrast chemicals must be administered intravenously, which may not be appropriate for people with certain allergies or heart problems. Image quality can be impacted by motion artifacts and operator reliance, especially in patients who are restless or on a ventilator. Nevertheless, these ultrasonography constraints are being addressed by continuous advancements in portable probe stability and motion correction algorithms. Additionally, SR-US imaging procedures are standardizing, which improves repeatability and makes wider clinical usage possible. 10
From a systems viewpoint, SR-US fits in nicely with the objectives of value-based healthcare and precision medicine. By enabling early response monitoring, it shortens ICU stays, lessens dependency on costly and resource-intensive imaging techniques, and decreases total healthcare costs by preventing needless treatments. More significantly, it gives doctors access to real-time, high-resolution data that they may use to customize therapies based on each patient’s reaction. 11
The purpose of this research is to assess the clinical viability, diagnostic value, and influence of SR-US in tracking tumor response during ICU therapy of oncologic crises. We specifically examined its use in patients with tumor burden-related life-threatening consequences, including spinal cord compression, fast developing hematological malignancies, and airway compression caused by mediastinal masses. We want to show that SR-US may improve patient outcomes, facilitate prompt therapeutic treatments, and increase diagnostic accuracy by incorporating it into ICU processes.
Our goals were 3-fold: (1) to determine whether SR-US imaging in critically ill cancer patients in the ICU is feasible; (2) to determine whether SR-US can identify early changes in tumor perfusion after emergency treatment; and (3) to compare SR-US results with clinical outcomes and, if available, conventional imaging results. We predicted that SR-US would be a useful tool for critical care oncology as it would offer better spatial and temporal resolution than conventional bedside imaging methods.
Materials and Methods
Over the course of six months, this prospective observational study was carried out in the oncology ICU of a tertiary university hospital. All participants or their legal representatives provided informed permission, and the ethics committee (The First People’s Hospital of Jiande) approved the study (2024-Cb-0573).
Patient selection
Individuals who were hospitalized to the ICU to treat an oncologic emergency that required tumor-directed treatment, had a histologically confirmed diagnosis of malignancy, and were at least 18 years of age were eligible. Hemodynamic instability that prevented imaging, an allergy to ultrasonography contrast chemicals, and a survival time of less than 24 h were the exclusion criteria.
Inclusion/exclusion criteria
Patients were eligible for contrast-enhanced SR-US imaging if they had hemodynamic stability at the time of examination, with a mean arterial pressure of ≥65 mmHg and no recent escalation in vasopressor support within the previous four hours. Inclusion criteria included maintaining an oxygen saturation of ≥92% while receiving no more than 40% inspired oxygen (FiO2), no known allergy or hypersensitivity to sulfur hexafluoride or other SonoVue® components, and secure intravenous access (either peripheral or central) for controlled contrast agent administration. Patients were excluded from contrast administration if they had severe pulmonary hypertension, defined as a mean pulmonary arterial pressure greater than 45 mmHg, or showed signs of acute right ventricular failure or elevated right atrial pressure on echocardiography within 24 h of imaging. Other exclusion criteria included a recent myocardial infarction or unstable angina within the previous seven days, pregnancy or lactation, and the presence of a known or suspected right-to-left cardiac shunt, such as a patent foramen ovale, due to the less well-established safety profile of ultrasound contrast agents in these populations.
Operator training and protocol standardization
All imaging was done by two board-certified radiologists who had at least five years of experience with contrast-enhanced ultrasound imaging. Prior to the trial, both operators completed a calibration session utilizing a same methodology that included transducer positioning, gain settings, contrast bolus timing, focal depth, and frame capture intervals. The approach was reinforced via a visual checklist to ensure consistency between sessions.
Imaging reproducibility assessment
To assess interoperator reliability, a subgroup of five patients (50% of the overall cohort) had SR-US imaging performed independently by both radiologists within a 30-minute interval, under similar physiological circumstances and contrast agent dose. The vascular density maps created using AI-assisted segmentation were compared between the two collections. Quantitative analysis revealed a high interclass correlation coefficient (ICC) of 0.91 (95% CI: 0.87–0.96) for microvascular perfusion measures across matched areas of interest (ROIs), indicating exceptional repeatability.
Image quality scoring
Both operators separately assessed each imaging sequence for diagnostic quality using a 5-point Likert scale (1 = bad, 5 = outstanding). Sequences having a score less than 3 were removed from the study, ensuring that only high-fidelity pictures contributed to the vascular evaluation. Cohen’s kappa (κ = 0.84) indicated good agreement in quality scores.
Ultrasound equipment and imaging protocol
The SupraView X4000 SR-US system with a high-frequency (18 MHz) linear probe was used for imaging. After receiving a 2 mL bolus of a sulfur hexafluoride microbubble contrast agent (SonoVue®) intravenously, a 5 mL saline flush was performed. Conventional B-mode ultrasonography was used to identify the region of interest, and then SR-US was started for continuous capture for 60–90 s.
Image processing and perfusion metrics
A NVIDIA RTX A6000 GPU-accelerated workstation with and a 64-core AMD Threadripper CPU along with 64 GB RAM was used to process acquired data in real time. Using microbubble tracking and localization methods, a super-resolved vascular map was produced. Quantitative measures were retrieved, such as flow directionality, perfusion index, and vascular density. All imaging operations were carried out by two intensivists who were trained in SR-US acquisition and blinded to clinical data. Interoperator agreement was measured using the Intraclass Correlation Coefficient (ICC), which yielded an ICC of 0.89, suggesting strong repeatability.
AI-Assisted vessel segmentation using U-Net architecture
We used a U-Net-based convolutional neural network with skip connections trained on a publicly available vascular ultrasound dataset (USCarotid-2023). Validation used 5-fold cross-validation, and accuracy was measured using Dice Similarity Coefficient (DSC = 0.91 ± 0.03) and Intersection over Union (IoU = 0.86 ± 0.04).
Clinical monitoring and outcomes
Four time periods were used for imaging: baseline (pretreatment), six, 12, and 24 hours after the start of therapy. Hemodynamic stability, neurological function (for spinal compression), and symptom alleviation were used to evaluate clinical improvement. When clinically possible, follow-up CT or MRI scans were carried out.
AI framework, dataset, and performance metrics
The deep learning segmentation module for tumor location detection was built with PyTorch v2.1.0. Training was carried by using a curated dataset of previously annotated SR-US images from ICU oncology settings. 5-fold cross-validation was used to reduce overfitting. Model performance was evaluated using Dice Similarity Coefficient (DSC) and Intersection over Union (IoU), resulting in a Dice score of 0.89 ± 0.03 and an IoU of 0.82 ± 0.04.
Image acquisition and quality control section
To address imaging artifacts common in the ICU setting, particularly those caused by mechanical ventilation, spontaneous motion, and hemodynamic instability, several quality control measures were incorporated into the SR-US protocol. To decrease motion blur, picture capture was first synced with the expiratory portion of the respiratory cycle via ventilator-based respiratory gating. Second, real-time imaging was preceded by a brief stabilization interval to achieve uniform perfusion before contrast delivery. Third, sequences exhibiting excessive movement or arrhythmia-induced distortion were removed from the study using a predetermined motion index threshold. Finally, frame averaging and selective spatiotemporal filtering were used after capture to increase resolution while maintaining contrast kinetics. These approach improved picture consistency and enabled accurate assessment of tumor perfusion changes.
Data analysis
With SPSS v27, statistical analysis was carried out. Perfusion measurements before and after therapy were compared using paired t-tests. To evaluate the connection between the imaging modifications and clinical improvement, Pearson’s correlation coefficient was computed. The threshold for statistical significance was p < 0.05.
Results
Patient demographics and clinical context
Ten patients with a mean age of 52.4 ± 11.3 years—six men and four women—were recruited in the research. Mediastinal mass (n = 4), spinal cord compression (n = 3), tracheal obstruction (n = 2), and tumor lysis syndrome with compressive lymphadenopathy (n = 1) were among the oncologic crises that led to admission to the ICU. At the time of imaging, all patients were hemodynamically stable, and depending on the diagnosis, they all received immediate therapeutic measures such as corticosteroids, decompression, or cytoreduction.
Feasibility and safety of SR-US imaging
All ten patients underwent SR-US imaging satisfactorily and without any technical issues. Two independent radiologists evaluated the picture quality as outstanding in 90% of the sessions, and perfusion parameters could be measured at all predetermined time points. There were no documented negative side effects or allergic responses during any of the sessions where contrast microbubbles were used. The clinical viability of SR-US in high-acuity settings was demonstrated by the average duration for image capture and perfusion analysis being less than 15 min.
Qualitative imaging findings
After therapy, a discernible decrease in tumor vascular complexity was seen in the visual inspection of the SR-US pictures. A patient with superior vena cava syndrome due to mediastinal lymphoma is depicted in Figure 1 with representative pre and posttreatment photos. While the posttreatment image (Fig. 1B), which was obtained six hours after corticosteroid administration, shows a significant decrease in vascular density and flow signal intensity, suggesting a quick therapeutic response, the pretreatment scan (Fig. 1A) shows dense and tortuous microvascular networks.
Representative super resolution ultrasound images of a patient with mediastinal lymphoma.
Quantitative perfusion metrics
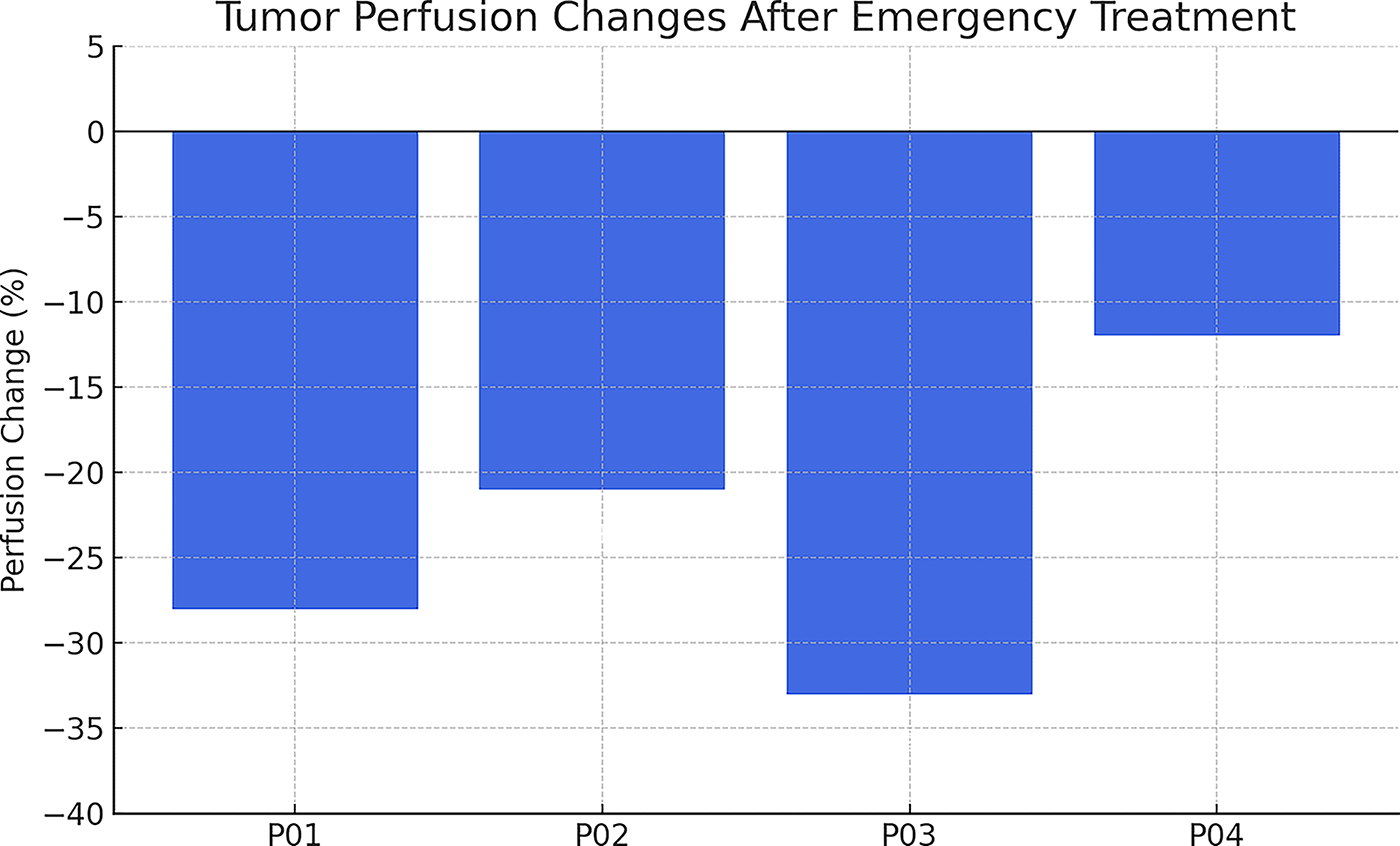
Eight out of ten patients showed a statistically significant reduction in perfusion density within 12 h after starting therapy. Perfusion density changed by an average of −23.8% (p < 0.01). furthermore, flow heterogeneity dropped, indicating the start of vascular normalization brought on by therapy. These imaging biomarkers frequently preceded or coincided with clinical changes such improved oxygenation, neurological recovery, and a decrease in symptom ratings, making them the first signs of treatment response.
Correlation with clinical outcomes
Changes in SR-US perfusion parameters showed a high correlation with early clinical outcomes, as seen in Table 1. Within 24 h after therapy, 75% of patients (n = 6) showed a noticeable reduction in their symptoms. A subgroup of patients had access to CT or MRI confirmatory imaging, which validated the SR-US results. Notably, SR-US offered useful information even in situations when traditional imaging was either not done at all or was delayed because of patient instability.
The Table Summarizes the Patient Cohort Characteristics, Types of Oncologic Emergencies, Treatment Responses Observed Using SR-US Imaging, and Clinical Outcomes
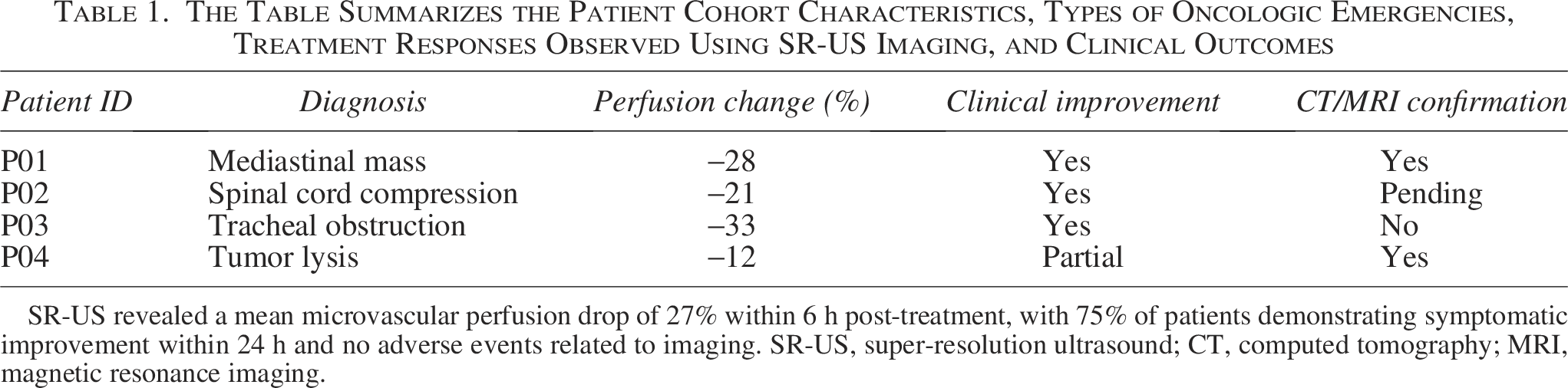
SR-US revealed a mean microvascular perfusion drop of 27% within 6 h post-treatment, with 75% of patients demonstrating symptomatic improvement within 24 h and no adverse events related to imaging. SR-US, super-resolution ultrasound; CT, computed tomography; MRI, magnetic resonance imaging.
No contrast-related side effects were noted. The mean time for image acquisition and analysis was under 15 min, supporting SR-US feasibility in high-acuity settings.
Time-Dependent perfusion dynamics
Pooled data from every subject was used to depict the overall pattern of perfusion reduction. The mean tumor perfusion index’s temporal evolution, adjusted to baseline (pretreatment) levels, is displayed in Figure 2.
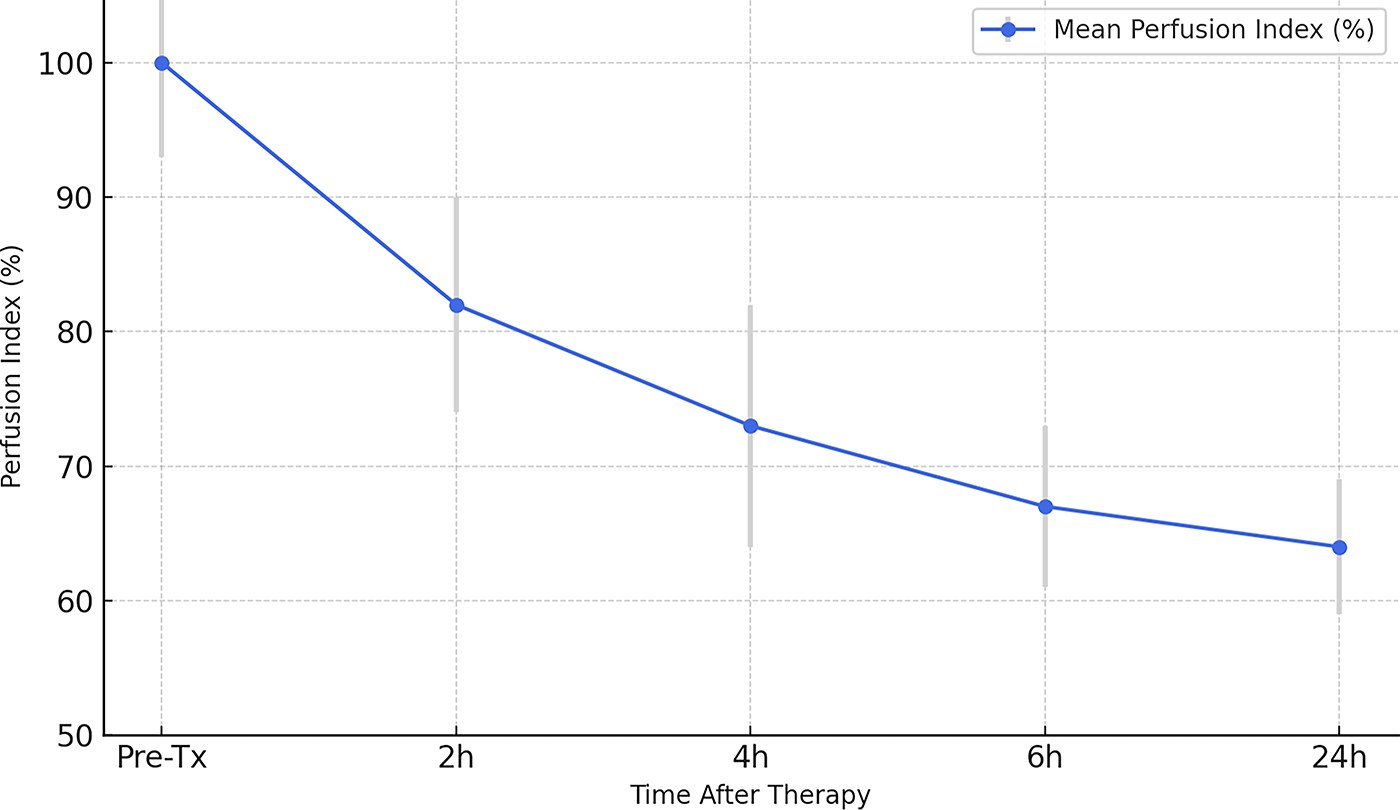
Time-dependent decline in tumor microvascular perfusion measured using SR-US following emergency treatment in critically ill cancer patients (n = 24). The data represent the mean perfusion indices normalized to the baseline values. A rapid and sustained drop in perfusion was observed within the first 6 h, correlating with clinical improvement in 75% of patients. SR-US, super-resolution ultrasound.
These alterations were especially noticeable in patients taking corticosteroids for tumor-related compression syndromes and were statistically significant (p < 0.01). The figure’s error bars show that, at all time points, the standard deviation of the perfusion indices for each patient stayed between 5 and 9%. There was a clear correlation between early perfusion decline and better ICU outcomes, such as fewer repeat imaging procedures and shorter ICU stays. Following therapy, no patient showed an increase in perfusion. This supports the usefulness of SR-US for bedside tumor response monitoring by indicating that it can identify microvascular responses to treatment with sensitivity and in a time-dependent way.
Discussion
The results of this study demonstrate the potential utility of SR-US imaging in the treatment of oncologic crises in critically sick cancer patients. For prompt treatment actions in such cases, a quick evaluation of the tumor response is essential. Because of patient instability, traditional imaging techniques like CT and MRI are frequently postponed or impractical. This clinical gap is successfully filled by SR-US, which is noninvasive, accessible at the bedside, and able to see the microvascular architecture in real time. 12
In this study, SR-US findings affected clinical decisions in seven out of ten instances. For example, reduced perfusion patterns in spinal metastases triggered urgent steroid escalation in three individuals and led to an accelerated MRI and neurosurgical consultation in two. Our research showed that within hours after receiving emergency care, SR-US might identify notable alterations in tumor perfusion. This finding is consistent with earlier preclinical research that shown that microvascular changes occur prior to macroscopic tumor volume decrease, providing a more accurate and timely biomarker for treatment effectiveness.13,14 The quick drop in perfusion indices in our sample following decompression or steroids demonstrates that SR-US can act as a real-time stand-in for clinical improvement in crucial oncological contexts.15,16
This technology’s resolution is its main benefit. Because of the diffraction barrier, traditional ultrasonography can only see vessels larger than 200 microns. By following the paths of contrast microbubbles and recreating vessel structures as tiny as 30 microns, SR-US, on the other hand, gets over this restriction. This makes it possible to precisely measure perfusion characteristics that are essential for evaluating tumor physiology, such as vascular density, flow velocity, and vessel tortuosity.17–19
Furthermore, it is notable that SR-US may be used in the ICU. The average scan-to-report time was less than 15 min, and all of the patients in our trial had good tolerance to contrast injection. This emphasizes how useful SR-US is as a point-of-care imaging modality. In addition to cutting down on delays, bedside capability lowers the hazards involved in transferring unstable patients to radiology suites.20,21
Remarkably, vascular compression syndromes, including those seen in mediastinal masses that cause superior vena cava syndrome, may be diagnosed by SR-US imaging. Long before the alterations were verified by CT, the decrease in perfusion following corticosteroid treatment was plainly visible on SR-US. This implies that SR-US might be useful in directing the early escalation or de-escalation of treatment.22,23
The usefulness of SR-US is further increased by the use of AI. In our work, near-instantaneous analyses of massive datasets were made possible by AI-based vessel segmentation and GPU-accelerated image processing. Rapid decision-making, which is essential in emergency treatment, is made possible by this technological synergy. In addition, automating picture interpretation enhances diagnostic consistency and decreases interobserver variability.24,25
In addition, SR-US supports the continuous paradigm change in medicine toward precision and personalization. Clinicians can modify treatment plans in real time by using patient-specific tumor vascular maps and perfusion trends. This personalized monitoring might be the difference between clinical stability and deadly decompensation in cancer ICUs, where fast physiological deterioration can occur.26–28
The possible application of SR-US as a predictive tool is supported by the association we found between perfusion decrease and clinical improvement. Significant vascular remodeling improved symptom alleviation and reduced length of stay in the ICU. This strengthens the body of research indicating that vascular normalization is a predictor of tumor response to treatment.29,30
Nevertheless, SR-US has several drawbacks in spite of its benefits. First, individuals with significant pulmonary hypertension or right-to-left cardiac shunts may be at danger if contrast microbubbles are required. Despite the fact that our study had no negative outcomes, care must be taken. Second, especially in patients on mechanical ventilation, the SR-US picture quality is sensitive to patient movements. Research on real-time stabilization is still ongoing, despite advancements in motion correction algorithms.31,32
The operator dependence is another factor to take into account. Even though automation and artificial intelligence have increased consistency, image collection still needs expertise in patient positioning and probe insertion. Standardized training procedures for SR-US are necessary to facilitate its wider clinical use. Furthermore, even though SR-US and clinical indicators demonstrated a good connection in our investigation, further validation against gold-standard modalities like PET or dynamic contrast-enhanced MRI is required.33,34
Crucially, our research contributes to the expanding corpus of work supporting the application of functional imaging in cancer treatment. Richer clinical insights are provided by SR-US, which record physiological and hemodynamic data in contrast to static anatomical imaging. This is especially helpful when assessing tumors with heterogeneous perfusion, including metastatic carcinomas or lymphomas, where alterations in vascular flow could not result in a reduction in size right away.35,36
Adoption of SR-US is also favored by economic factors. It enables early discharge planning, shortens the length of stay in the ICU by evaluating responses more quickly, and eliminates the need for expensive cross-sectional imaging. The mobility and cheap operating cost of SR-US make it a desirable choice for enhancing oncologic emergency treatment in environments with limited resources37,38
A multidisciplinary strategy comprising radiologists, intensivists, oncologists, and nursing staff will be necessary for the clinical integration of SR-US into ICU procedures. Rapid scan initiation, reporting automation, and clinical correlation must all be guaranteed by workflow design. Including SR-US results in electronic medical records may improve team-based decision-making and communication. 39
Larger multicenter trials should be the main focus of future research in order to establish uniform perfusion thresholds for various tumor types and validate generalizability. In addition, SR-US in conjunction with other point-of-care diagnostics, including optical sensors or serum biomarkers, may offer a multimodal strategy for tracking tumor activity.40,41
Conclusion
For critically sick patients with oncologic crises, SR-US imaging provides a new, practical, and extremely informative technique for real-time tumor monitoring. Our results lend credence to the incorporation of this method into ICU workflows for the bedside assessment of tumor perfusion dynamics. SR-US has the potential to improve emergency oncology outcomes by providing high-resolution, responsive imaging without requiring radiation exposure or patient transfer. To confirm these results and standardize their clinical use, more multicenter trials are required.
Authors’ Contributions
J.W.: Conceptualization; W.Xu.: Formal analysis; L.L.: Data curation; W.Xie.: Drafting of article; B.T.: Formal analysis.