
Abstract
Background:
Early diagnosis and accurate prediction of treatment response in esophageal squamous cell carcinoma (ESCC) remain major clinical challenges due to the lack of reliable and noninvasive biomarkers. Recently, artificial intelligence-driven endoscopic ultrasound image analysis has shown great promise in revealing genomic features associated with imaging phenotypes.
Methods:
A prospective study of 115 patients with ESCC was conducted. Deep features were extracted from endoscopic ultrasound using a ResNet50 convolutional neural network. Important features shared across three machine learning models (NN, GLM, DT) were used to construct an image-derived signature. Plasma levels of leukotriene B4 (LTB4) and other inflammatory markers were measured using enzyme-linked immunosorbent assay. Correlations between signature and inflammation markers were analyzed, followed by logistic regression and subgroup analyses.
Results:
The endoscopic ultrasound image-derived signature, generated using deep learning algorithms, effectively distinguished esophageal cancer from normal esophageal tissue. Among all inflammatory markers, LTB4 exhibited the strongest negative correlation with the image signature and showed significantly higher expression in the healthy control group. Multivariate logistic regression analysis identified LTB4 as an independent risk factor for ESCC (odds ratio = 1.74, p = 0.037). Furthermore, LTB4 expression was significantly associated with patient sex, age, and chemotherapy response. Notably, higher LTB4 levels were linked to an increased likelihood of achieving a favorable therapeutic response.
Conclusions:
This study demonstrates that deep learning-derived endoscopic ultrasound image features can effectively distinguish ESCC from normal esophageal tissue. By integrating image features with serological data, the authors identified LTB4 as a key inflammation-related biomarker with significant diagnostic and therapeutic predictive value.
Introduction
Esophageal squamous cell carcinoma (ESCC) is the predominant histological subtype of esophageal cancer worldwide, particularly affecting regions with high incidence rates of esophageal cancer such as East Asia and Africa. 1 China alone reported 224,012 new cases and 187,467 deaths, representing approximately 44% of the global burden. 2 Moreover, the global burden of esophageal cancer is projected to increase substantially, with an estimated 957,000 new cases and 880,000 deaths by 2040. 1 Despite advancements in multimodal treatment approaches, including surgery, chemotherapy, radiotherapy, and immunotherapy, late-stage diagnosis remains common in esophageal cancer, particularly ESCC. Surgery remains the cornerstone of curative treatment for localized disease. However, as most patients are diagnosed at an advanced or metastatic stage, platinum- and fluoropyrimidine-based chemotherapy regimens, such as cisplatin plus 5-fluorouracil, remain the mainstay of treatment for unresectable or metastatic cases. Besides, ESCC exhibits limited responsiveness to conventional cytotoxic chemotherapy. Objective response rates with standard regimens are modest, generally ranging from 30% to 40%, and primary chemoresistance occurs in a significant proportion of patients. 3 Moreover, up to 50% of patients experience disease progression within 6 months after initiating first-line chemotherapy, highlighting the aggressive nature of chemotherapy-resistant tumors. 4 Poor response to chemotherapy is strongly associated with rapid disease progression, early recurrence, and dismal overall survival, with 5-year survival rates remaining below 20% worldwide. 1 These challenges contribute to substantial health care burdens and emphasize the urgent need for novel therapeutic strategies to overcome chemoresistance and improve patient outcomes. These challenges contribute to substantial health care burdens and highlight the urgent need to identify reliable biomarkers for predicting disease occurrence and chemotherapy response in ESCC, which could facilitate personalized treatment strategies and improve patient outcomes.
The relationship between chronic inflammation and cancer development has been extensively explored, with numerous studies indicating that inflammatory mediators play crucial roles in tumorigenesis. 5 Leukotrienes, particularly leukotriene B4 (LTB4), have emerged as significant inflammatory mediators implicated in various cancers, including lung cancer, 6 breast cancer, colorectal cancer, pancreatic cancer, 7 and ESCC. 8 LTB4 is synthesized from arachidonic acid through a two-step enzymatic process involving 5-lipoxygenase (5-LOX) and 5-lipoxygenase-activating protein (FLAP), which first convert arachidonic acid to leukotriene A4 (LTA4), and LTA4 is then hydrolyzed by leukotriene A4 hydrolase (LTA4H) to produce LTB4. A study revealed that chronic crystalline silica exposure promotes lung cancer progression by inducing sterile inflammation mediated through the LTB4/BLT1 axis. Genetic deletion of BLT1 reduces CS-induced neutrophilic inflammation and tumor burden, highlighting LTB4/BLT1 as a potential immunotherapeutic target. 9 Kim et al. 7 showed that LTB4 can promote epithelial–mesenchymal transition and upregulate vimentin expression in PANC-1 pancreatic cancer cells via activation of the BLT2/ERK2 signaling pathway, and that inhibition or silencing of BLT2 or ERK2 significantly suppresses LTB4-induced vimentin expression, highlighting a potential mechanism linking inflammation to pancreatic cancer progression. However, the specific role of LTB4 in the context of ESCC and its potential as a predictive biomarker for chemotherapy response remain under investigation. This research gap underlines the necessity for studies that delve deeper into LTB4 levels in patients with ESCC and its correlation with inflammation and chemotherapy response.
In this context, the authors integrated artificial intelligence (AI)-based analysis of endoscopic ultrasound imaging to extract quantitative features, enabling the construction of a deep learning-derived image signature. By combining image-based biomarkers with serological data, this study evaluates the utility of plasma LTB4 as a predictive biomarker for treatment outcomes and provides new insights into how inflammation-related mediators and imaging phenotypes jointly contribute to ESCC progression and therapeutic response.
Materials and Methods
Data preparation and preprocessing
A total of 115 patients diagnosed with esophageal cancer at this center between May 2018 and May 2022 were included in this study (Ethical Approval No. 2022.20). All patients provided written informed consent before participation. At the time of diagnosis, all patients underwent routine clinical examinations, including complete blood counts and measurement of LTB4 levels and other inflammation-related factors.
In addition to serological data, high-resolution esophagogastroduodenoscopy images were obtained for each patient. During the same period, 115 healthy individuals without any history of malignancy or major systemic disease were randomly selected from the physical examination center to serve as the control group. Basic demographic information, as well as results from routine blood and urine tests, was collected for all controls to match the data obtained from the patient group. Thus, each patient with esophageal cancer had paired endoscopic ultrasound imaging data and corresponding serological test results. All image data underwent standardized quality control procedures to ensure completeness, consistency, and diagnostic clarity. Images with motion blur, poor illumination, or incomplete anatomical coverage were excluded. Preprocessing steps included image resizing, pixel normalization, and denoising where necessary, to optimize image quality for subsequent analysis. Laboratory data were also preprocessed, including handling of missing values, standardization of measurement units, and exclusion of outliers based on predefined clinical thresholds. The final dataset consisted of matched endoscopic ultrasound and serological data for each cancer patient, along with demographically matched and quality-controlled clinical examination data from healthy controls. A schematic illustration of the study design and data processing workflow is shown in Figure 1.
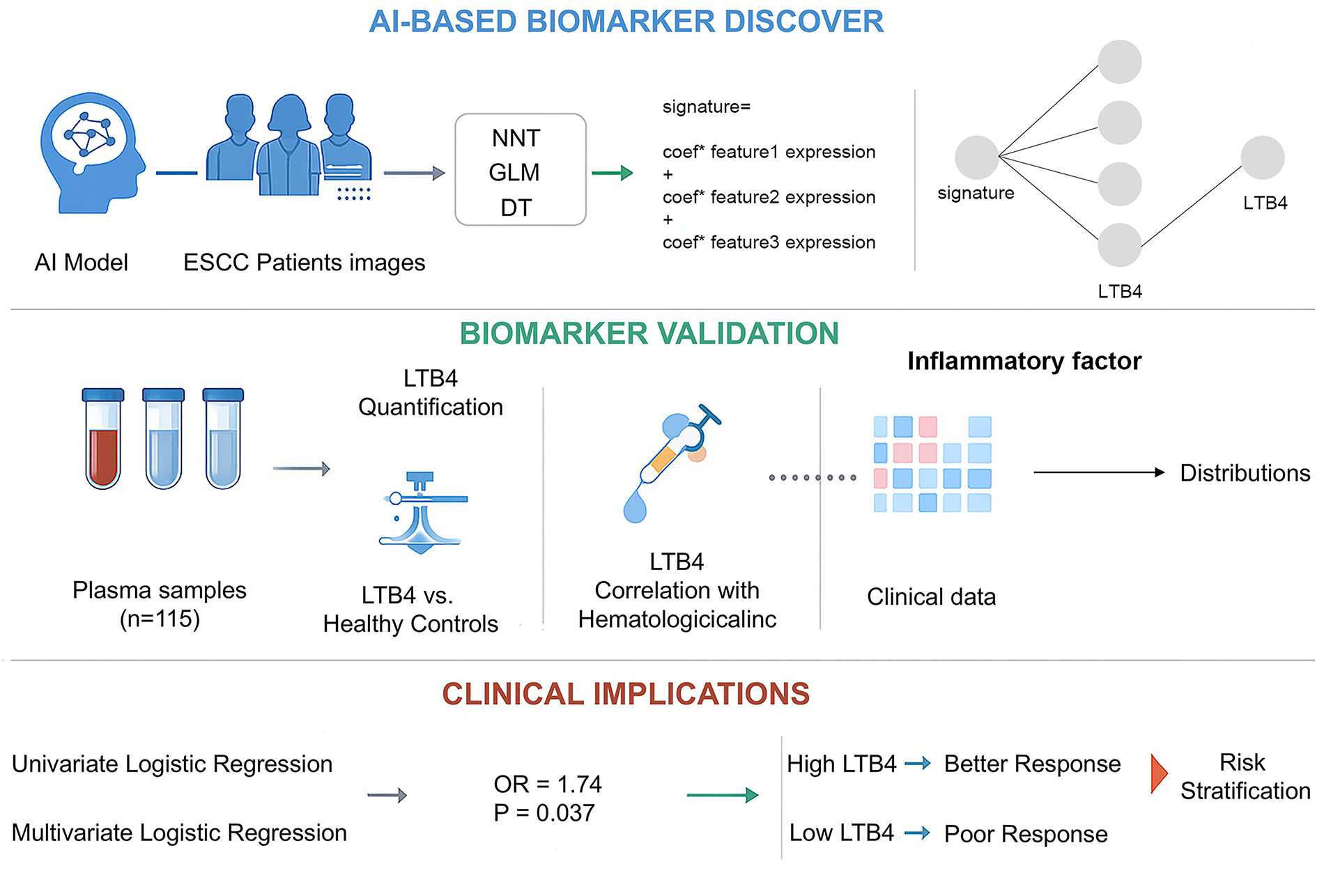
Workflow of study.
Deep learning-based feature extraction
In this study, a ResNet50 convolutional neural network model was used for automated recognition and feature extraction from endoscopic ultrasound. The model was pretrained on the ImageNet dataset and subsequently fine-tuned using annotated esophageal cancer images to improve its performance in the medical imaging domain. The model was applied to identify regions of interest indicative of potential lesions, and intermediate feature maps were extracted from the final convolutional layers. These were then transformed into high-dimensional feature vectors that represent the structural and textural characteristics of local image regions for subsequent statistical analysis and modeling.
Machine learning-assisted selection of important features and build the signature
To further evaluate the clinical relevance of image features and their discriminatory power for disease status, three supervised learning models were constructed: a feedforward neural network (NN), a generalized linear model (GLM), and a decision tree (DT) classifier. Each model was trained on the extracted image feature vectors, using the binary outcome of esophageal cancer diagnosis as the target variable. Feature importance was assessed using model-specific approaches: the NN used weight sensitivity analysis to determine the influence of each feature on the output; the GLM used standardized regression coefficients and corresponding p-values to quantify feature significance and effect size; and the DT measured the mean decrease in Gini impurity to reflect each feature’s contribution to classification accuracy. Based on the selected important features, the authors constructed a feature-related signature capable of accurately predicting image-based diagnosis. The dataset, comprising 115 patients and 115 controls, was randomly divided into separate subsets for model development and evaluation. A stratified split was applied to maintain balanced case–control ratios in each subset. All splits were performed at the patient level to prevent data leakage, and a fixed random seed was used to ensure reproducibility.
Serological indicator collection and analysis
Each participant provided 2 mL of fasting venous blood, which was collected in EDTA anticoagulant tubes. All blood samples were processed using a Sysmex XN-1000i automatic hematology analyzer for routine blood parameters. Serum concentrations of leukotriene E4 (LTE4) and LTB4 were quantified using competitive enzyme-linked immunosorbent assay (ELISA) kits, following the instructions. In addition to LTB4 and LTE4, serum levels of multiple inflammatory cytokines and mediators were measured using multiplex ELISA or chemiluminescent immunoassays, depending on the availability and sensitivity requirements. Subsequently, the expression levels of LTB4 and other inflammatory markers were compared between healthy controls and patients with ESCC. Furthermore, correlations between LTB4 levels and other inflammatory indicators were assessed using Pearson or Spearman correlation coefficients, as appropriate. These serological markers were also incorporated into multivariate models to predict the expression status of key inflammatory mediators based on endoscopic ultrasound image-derived features, to explore potential image–serology correlations and identify imaging biomarkers indicative of systemic inflammation.
Correlation and regression analysis of signature and inflammatory markers
To investigate the relationship between image-derived signatures and systemic inflammation, correlation analyses were conducted between the extracted signature scores and serum levels of inflammatory markers. Pearson or Spearman correlation coefficients were calculated depending on the data distribution. Inflammatory markers that showed a significant correlation with the signature were selected for further analysis. Subsequently, logistic regression models were constructed to evaluate whether these signature-associated inflammatory markers could contribute to disease diagnosis. The presence of ESCC was used as the dependent variable, while the selected inflammatory markers and relevant clinical variables (e.g., age, sex, laboratory values) were included as independent variables. Odds ratios with 95% confidence intervals were reported to quantify the strength of association. In addition, the expression levels of the identified inflammatory markers were compared across different clinical subgroups of patients with ESCC (e.g., by tumor stage, lymph node involvement, or histological grade). This subgroup analysis explored the potential stratification value of the marker and its applicability in different clinical contexts.
Results
Demographic and clinical characteristics
A total of 115 patients were enrolled in this study, including 69 of Han ethnicity and 46 of Mongolian ethnicity. The average age of the patients was 52.89 ± 8.08 years. Among the enrolled patients, 33 exhibited elevated serum carcinoembryonic antigen levels, 22 had elevated cytokeratin-19 fragment levels, and 40 patients showed increased squamous cell carcinoma antigen levels. The detailed demographic and serological profiles of the patients are summarized in Figure 2.
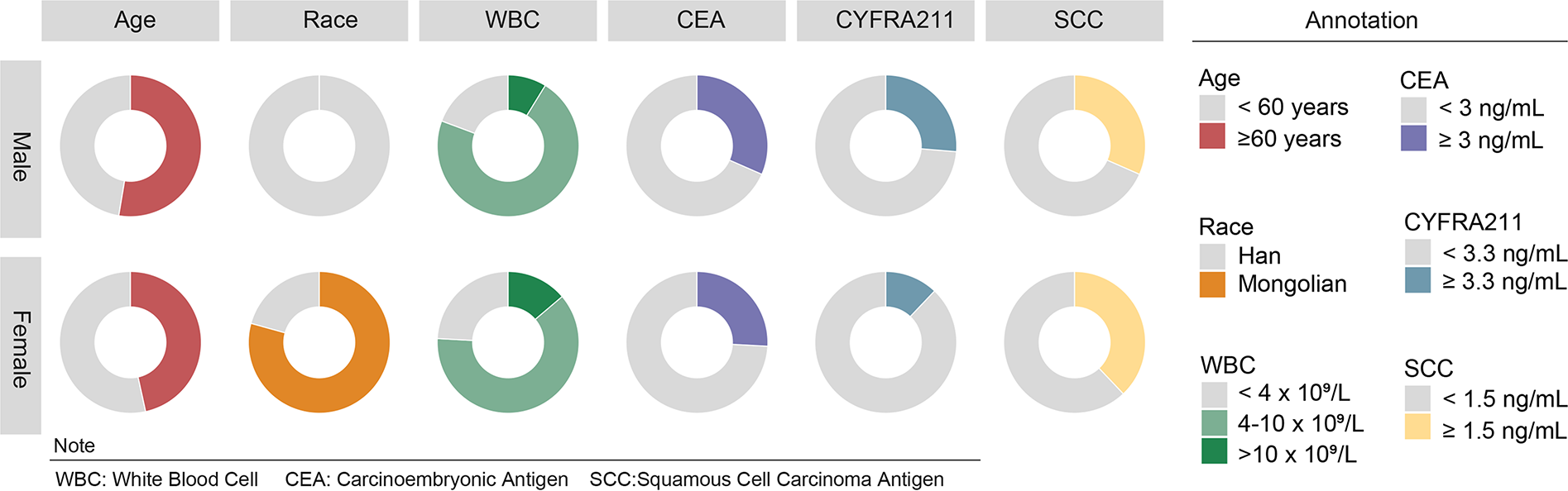
Demographic and serological characteristics of enrolled patients.
Image feature extraction and differential feature identification
Before analysis the image was used to normalize and use CAM heatmap to show the disease area (Fig. 3A–C). Image features were extracted using the previously described ResNet50-based deep learning approach, generating high-dimensional representations of endoscopic ultrasound for each patient. In addition, the features were also normalized by R software (Fig. 3D, E). To identify features with discriminative power, differential analysis was performed using the limma package in R. Features with a p-value of <0.1 were considered statistically significant and retained as differential features between esophageal cancer patients and healthy controls for further analysis (Fig. 3F).
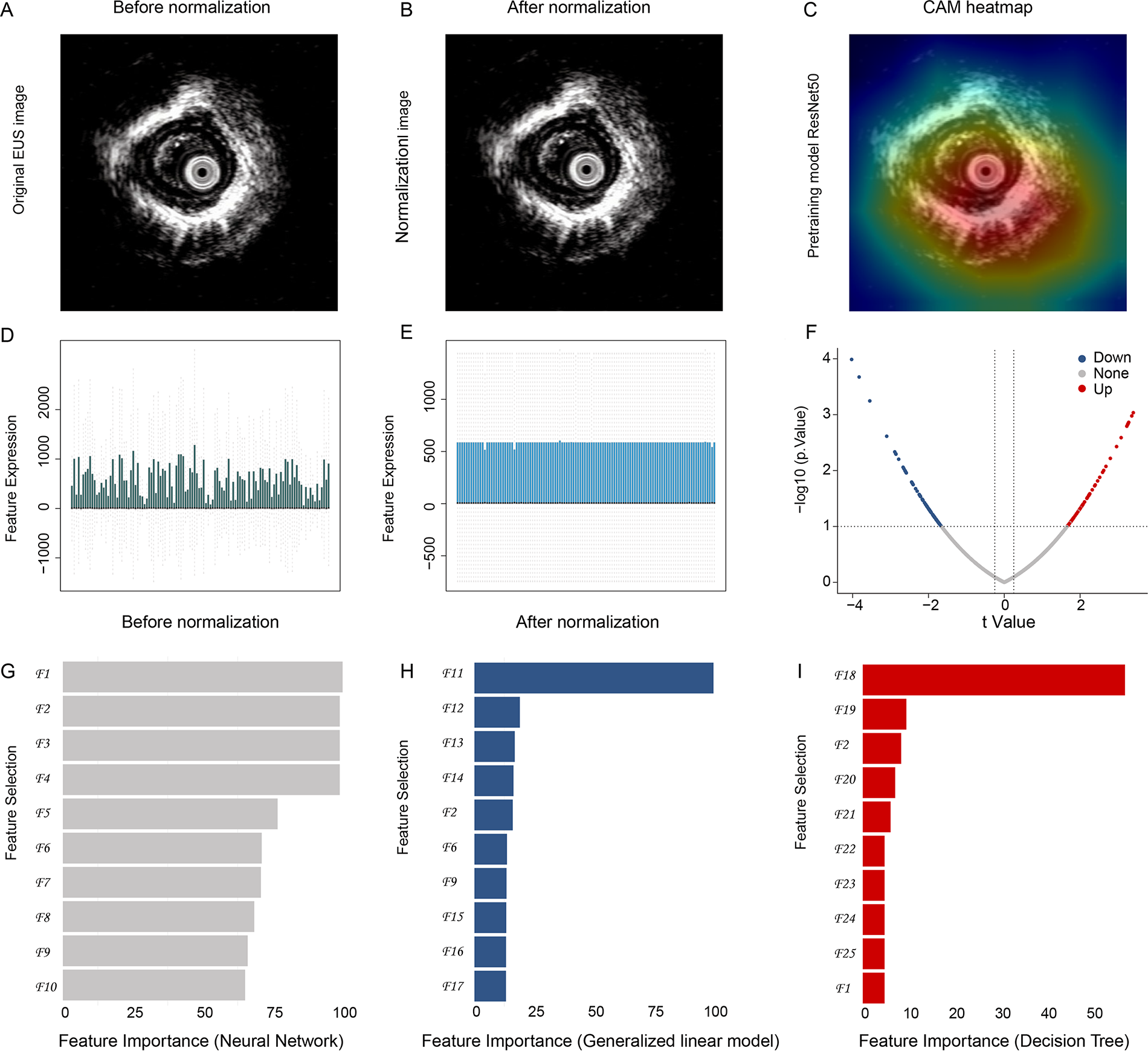
Image feature extraction, differential analysis, and construction of diagnostic signature.
Select key image features and signature construction
To identify the most important features, three supervised machine learning models were developed: feedforward NN, GLM, and DT classifier. Features consistently ranked as important across all three models—denoted as F2, F3, F6, F7, and F9, were selected as core image features. The top 10 features of each model are shown in Figure 3G–I (Supplementary Table S1). The model index evaluation is shown in Supplementary Figure S1. A regression-based signature score was then constructed by multiplying each feature by its corresponding model coefficient and summing the results. This image-derived signature served as a composite score reflecting disease-relevant imaging phenotypes.
Identification of inflammation marker LTB4 associated with the feature signature
To explore the association between imaging features and systemic inflammation, Pearson correlation analysis was performed between the image signature and serum inflammatory markers. LTB4 showed the strongest and most significant negative correlation with the signature score, suggesting its potential role in disease development and image phenotype expression in esophageal cancer (Supplementary Table S2).
LTB4 as an independent risk factor for chemoresistance in esophageal cancer
This part workflow is shown in Figure 4A. Multivariate logistic regression analysis revealed that low LTB4 expression was an independent risk factor for chemotherapy resistance in esophageal cancer patients (Fig. 4B). Subgroup analyses further indicated significant differences in LTB4 expression levels across different genders and age groups, with a strong correlation between LTB4 expression and chemotherapy response. These findings suggest that LTB4 not only reflects the systemic inflammatory state of esophageal cancer patients but may also serve as a predictive biomarker for chemotherapy sensitivity, highlighting its potential clinical utility (Fig. 4C–E).
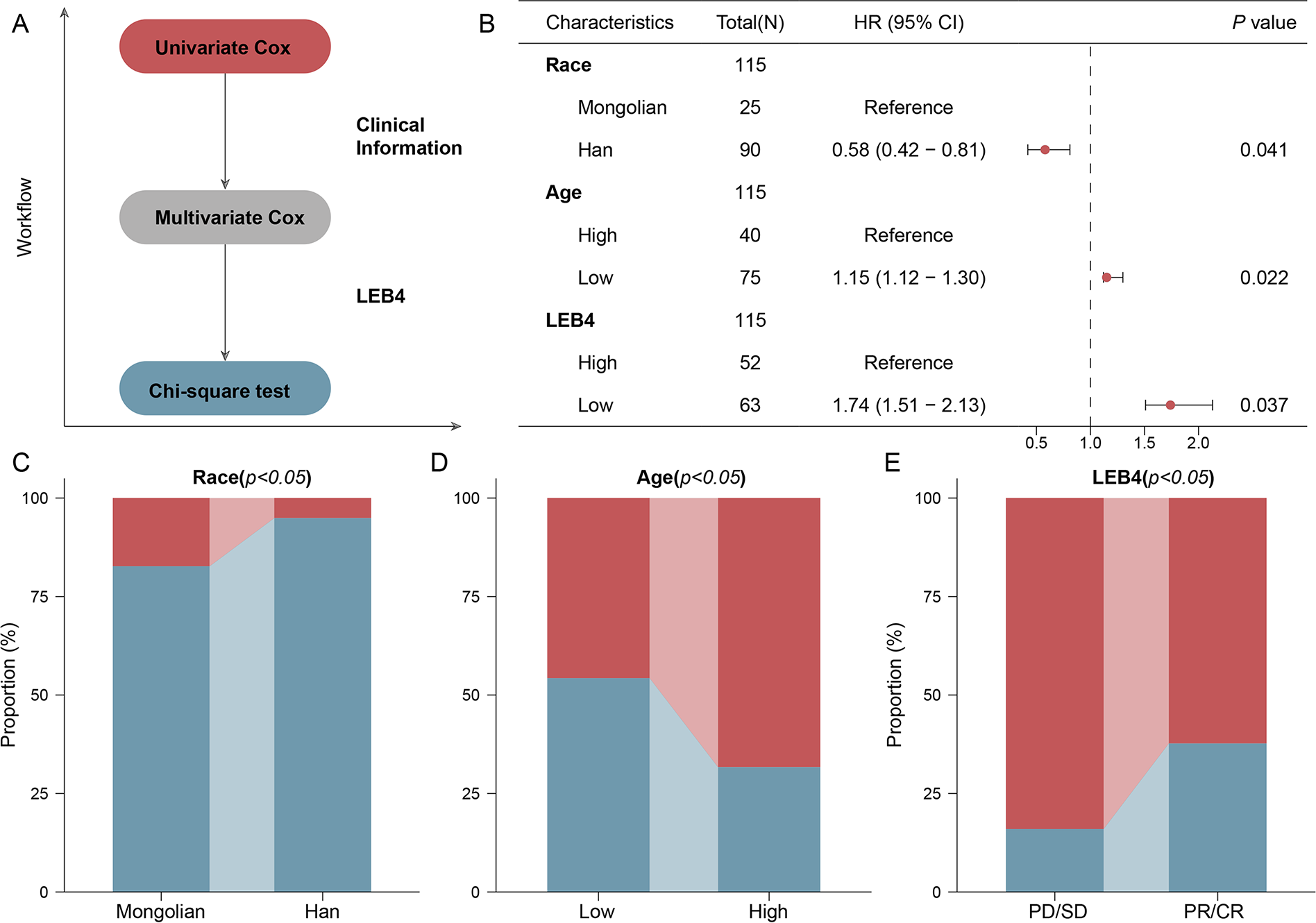
Association between image-derived signature and leukotriene B4 (LTB4) levels, and predictive value of LTB4 for chemoresistance.
LTB4 is downregulated in patients with ESCC and associated with other inflammation markers
LTB4 levels were significantly lower in esophageal cancer patients compared with healthy controls. The mean LTB4 level in the patient group was 47.92 ± 26.55 pg/mL, significantly lower than the 68.19 ± 36.46 pg/mL observed in the control group (p < 0.001, Fig. 5A). Compared with the control group, esophageal cancer patients showed significant decreases in red blood cell count, hemoglobin, hematocrit, platelet count, lymphocyte percentage, and absolute lymphocyte count (p < 0.0001). Conversely, neutrophil percentage (Neu%) and monocyte percentage (Mono%) were elevated in the patient group, with a more prominent increase in Mono% (p < 0.001) and a moderate increase in Neu% (p < 0.05) (Fig. 5B–H). Although total white blood cell count (WBC), absolute neutrophil count (Neu), and absolute monocyte count (Mono) did not differ significantly between groups (p > 0.05), both the neutrophil-to-lymphocyte ratio (NLR) and monocyte-to-lymphocyte ratio (MLR) were significantly elevated in the patient group (p < 0.001). The platelet-to-lymphocyte ratio (PLR) was significantly reduced, decreasing from 113.69 ± 29.54 in the control group (p < 0.0001) (Fig. 6A–L).
Downregulation of leukotriene B4 (LTB4) and associated hematological changes in esophageal squamous cell carcinoma (ESCC) patients.
Systemic inflammatory markers in esophageal squamous cell carcinoma (ESCC) patients.
Discussion
Leukotrienes, a group of bioactive lipid mediators derived from arachidonic acid through the 5-LOX pathway, have been increasingly recognized for their roles beyond classical inflammation. 10 Emerging evidence suggests that leukotrienes, particularly LTB4, contribute to tumorigenesis and cancer progression through multiple mechanisms. First, 5-LOX and leukotriene signaling is critical in shaping the tumor microenvironment (TME) by mediating interactions among epithelial, stromal, and immune cells. 11 LTB4 can cooperate with cytokines such as TNF-α to promote tumor cell growth, survival, invasion, and metastasis, with inhibition of 5-LOX or LTA4H significantly reducing tumor burden in various cancer models.12,13 Second, leukotrienes have been shown to enhance tumor cell proliferation, survival, migration, and invasion through activation of downstream signaling pathways such as PI3K/Akt and NF-κB.14,15 Moreover, elevated leukotriene signaling may contribute to therapy resistance by protecting cancer cells from apoptosis and promoting an immunosuppressive microenvironment.11,16 A previous study has shown that LTB4 receptors (LTB4R and LTB4R2) are upregulated in ESCC tissues compared with the adjacent nontumorous epithelium and healthy esophageal mucosa. 17 However, in the present study cohort, the authors observed that plasma LTB4 levels in patients with ESCC were significantly lower than those in healthy individuals. This finding appears to contradict previous reports focusing on tumor tissues. One possible explanation for this discrepancy is that the systemic circulation of LTB4 may not directly reflect its localized production within the TME. Moreover, advanced cancer stages are often associated with systemic immunosuppression and altered leukotriene metabolism, which could lead to decreased circulating LTB4 levels. In addition, differences in sample types (plasma vs. tumor tissue), disease stage, prior treatments, or patient-specific factors such as nutritional status and systemic inflammation might also contribute to the observed variations.
Addressing the research gap regarding plasma LTB4 levels and chemotherapy response in ESCC, this study further demonstrates that LTB4 can serve as an independent predictive factor for chemotherapy efficacy. Notably, patients with lower plasma LTB4 levels exhibited poorer responses to chemotherapy. This association was further confirmed in the subgroup of patients older than 60 years. Previous studies have demonstrated that elevated expression of LTB4 receptors (BLT1 and BLT2) promotes tumor progression and chemoresistance in various cancers, including ovarian, breast, and pancreatic cancers. 18 In addition, it has been shown that chemotherapy-induced apoptosis in hepatocellular carcinoma cells can activate the LOX pathway, leading to increased LTB4 production, which enhances the adhesion and migration of residual tumor cells and potentially facilitates metastasis. 19 Although these previous findings appear to contradict these results, this apparent discrepancy may be explained by differences between systemic and local TME dynamics. While receptor overexpression indicates enhanced leukotriene signaling activity within tumor tissues, decreased circulating LTB4 levels could result from rapid local consumption, receptor-mediated uptake, or altered systemic inflammatory status, ultimately contributing to immune suppression and therapy resistance.
In addition, this analysis reveals that plasma LTB4 levels are negatively correlated with the percentage of lymphocyte and absolute lymphocyte counts, while positively correlated with the NLR, an established marker of systemic inflammation. 20 Previous studies have shown that an elevated NLR is associated with poor prognosis and reduced chemotherapy efficacy in various cancers, including ESCC.21,22 These findings suggest that lower circulating LTB4 levels may reflect an impaired lymphocyte-mediated immune response and a shift toward a proinflammatory, immunosuppressive systemic environment. Therefore, reduced LTB4 levels in plasma could indicate a compromised antitumor immune state, thereby contributing to suboptimal chemotherapy responses in patients with ESCC. Further mechanistic studies are warranted to clarify the role of LTB4 in regulating immune balance during cancer progression and treatment.
Through the prospective analysis, the authors identified that plasma LTB4 levels are reduced in patients with ESCC and that lower LTB4 levels are associated with poorer chemotherapy response. By focusing on LTB4, they propose a novel inflammatory biomarker candidate for predicting chemotherapy efficacy in ESCC. Unlike previous research emphasizing genetic mutations or classical inflammatory markers, these findings highlight the potential clinical significance of systemic LTB4 levels in patient stratification and personalized therapy. The observed associations between LTB4 levels and various hematological parameters suggest a complex interplay between inflammation and tumor biology. By further elucidating the clinical applications of LTB4, the authors may enhance early detection and intervention strategies for esophageal cancer, ultimately improving patient outcomes. Nevertheless, several limitations still need to be considered. The relatively small sample size and single-center design may limit the generalizability of the findings. Although significant associations were observed, the underlying biological mechanisms remain speculative and require experimental validation. Furthermore, most existing studies have focused on leukotriene signaling within tumor tissues, while the systemic role of circulating LTB4 remains largely unexplored. This highlights the need for future studies involving larger, multicenter cohorts and mechanistic investigations to fully establish the clinical utility of plasma LTB4 as a biomarker and therapeutic target in ESCC.
The limitation of this study lies in the demographic composition of the dataset. The relatively small sample size and limited ethnic diversity may restrict the generalizability of the findings across different populations. This imbalance was not intentional but rather reflects the demographic characteristics of the available data sources. As a result, the model’s performance in underrepresented populations remains to be validated. Future studies involving larger, multicenter, and ethnically diverse cohorts are essential to confirm the robustness and clinical utility of the proposed approach.
Conclusions
In conclusion, these findings demonstrate that combining deep learning-based analysis of endoscopic ultrasound with serological profiling offers a novel and effective approach for improving the diagnosis and treatment prediction of ESCC. The identification of LTB4 as a signature-associated inflammatory biomarker highlights its potential role not only in disease classification but also in reflecting tumor–host interactions and chemotherapy sensitivity. This integrative radiogenomic strategy underscores the value of AI in uncovering biologically meaningful patterns from routine clinical data and paves the way for more personalized, non-invasive diagnostic tools in ESCC management. Moreover, by leveraging widely available imaging modalities and cost-effective blood-based assays, this approach holds particular promise for deployment in low-income countries, where access to advanced diagnostic infrastructure is limited but the burden of ESCC remains high.
Authors’ Contributions
Y.W. (Yang Wang) and C.B. contributed to the design of the work. S.H., W.Z., and Y.W. (Yingnan Wang) contributed to the acquisition, analysis, and/or interpretation of data. S.H., W.Z., J.Q., and Y.W. (Yang Wang) have drafted the work and/or substantively revised it.
Footnotes
Ethics Statement
This study was approved by the Ethics Committee of The Chifeng Cancer Hospital (No. 2022.20).
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Disclosure Statement
The authors declare that they have no competing interests.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.