
Abstract
Ocular malignancies provide a unique therapeutic challenge because of their anatomical intricacy, limited accessibility, and vision-critical nature. Recent developments in radiopharmaceutical design have been paired with ultrasound-mediated medicine administration to create highly targeted, less invasive therapies for intraocular cancers. This research looks at the emerging topic of ultrasound-responsive radiopharmaceutical devices built specifically for ocular oncology. These methods enhance tumor selectivity, decrease off-target effects, and enable real-time imaging-guided therapy by utilizing targeted ultrasound to induce localized medication release or radiotherapeutic agent activation. Microbubble-assisted delivery, thermosensitive liposomes, and phase-transition nanodroplets carrying radionuclides have all been designed to optimize ocular pharmacokinetics and tissue penetration. Preclinical studies reveal promising results in increasing radiotherapeutic efficacy against retinoblastoma and uveal melanoma while sparing healthy ocular tissues.
Keywords
Introduction
Ocular malignancies, such as uveal melanoma, retinoblastoma, and conjunctival squamous cell carcinoma, provide considerable therapeutic problems due to their anatomical complexity, resistance to systemic treatment, and propensity to impair vision or metastasis.1,2 Despite breakthroughs in targeted therapies such as plaque brachytherapy, enucleation, and photocoagulation, ensuring tumor-specific delivery while protecting the surrounding healthy ocular structures remains a significant challenge. Conventional radiotherapeutic techniques are frequently hampered by nonspecific tissue exposure, poor penetration across ocular barriers, and the intrinsic vulnerability of intraocular tissues to ionizing radiation. 3
Radiopharmaceuticals—molecular constructions containing a radionuclide coupled to a tumor-targeting ligand—provide a potential path for precision, systemic, or localized radiotherapy. 4 Their rising use in oncology has shown that they may deliver lethal radiation directly to malignant cells while causing minimal harm to surrounding tissues. However, in ocular cancer, their therapeutic efficiency is restricted due to issues with medication transport, biodistribution, and control over radiation release dynamics within the eye’s confined and compartmentalized environment. 5 Ultrasound penetrates deeper ocular tissues than light-based solutions, eliminating the need for intrusive optics. Unlike magnetic field delivery, ultrasonography provides real-time imaging feedback and targeted energy deposition. These features make ultrasonography an ideal choice for ocular oncology, where accuracy and noninvasiveness are crucial. Radiation-induced retinopathy remains a serious long-term problem, especially for long-lived isotopes. Pathological findings include vascular blockage, macular edema, and neovascularization. To reduce these dangers, ongoing research focuses on dosage reduction and fractionated exposure. 6
Recent advances in stimulus-responsive drug delivery systems have presented the idea of ultrasound-triggered release as a way to overcome these constraints. Focused ultrasound (FUS) has evolved as a noninvasive tool for spatially and temporally controlling drug release through thermal, mechanical, or cavitation effects. 7 Phase-change nanodroplets are nanoscale carriers made up of a perfluorocarbon liquid core surrounded by a lipid or polymer shell. When exposed to FUS, these droplets undergo acoustic droplet vaporization (ADV), which converts the liquid into a gas phase and produces microbubbles in situ. This transition improves both imaging contrast and therapeutic administration because the resulting bubbles increase cavitation and tissue permeability. Nanodroplets (<300 nm) may extravasate into ocular tissues and activate on demand, unlike traditional microbubbles that are limited by their size (∼1–10 μm) and circulation restrictions. This allows for spatiotemporal control of treatment. Recent imaging advancements in ocular oncology include optical coherence tomography (OCT) angiography for vascular monitoring, adaptive optics for single-cell resolution, and PET/US hybrid systems for functional–structural integration. These methods supplement ultrasound-triggered nanocarrier systems. Researchers have created multifunctional systems that may be externally activated to release therapeutic drugs at specific ocular regions by combining radiopharmaceuticals into ultrasound-sensitive carriers such as thermosensitive liposomes, microbubbles, or phase-change nanodroplets.8–10 This method not only enhances intratumoral drug accumulation, but it also allows for real-time imaging guidance and post-treatment monitoring.
Despite significant advances in systemic tumors, the integration of ultrasound-responsive radiopharmaceutical devices into ocular applications is still underexplored. The anatomical accessibility of the eye, together with its immune-privileged position and the necessity for organ-sparing therapy, makes it a suitable venue for the use of this technique. Furthermore, new preclinical data indicate that ultrasound-mediated administration might temporarily breach the blood–retinal barrier, increase drug permeability, and improve radiopharmaceutical absorption in ocular malignancies without causing irreparable tissue damage.11,12 Unlike earlier evaluations that focused solely on nanomedicine or ocular imaging, this work combines the function of ultrasound-triggered nanocarriers with radiopharmaceutical techniques. This integration focuses on theranostic synergies that are yet to be explored in ocular oncology.
In this study, the author reviews recent advancements in ultrasound-responsive radiopharmaceutical platforms with a particular focus on their translational potential in ocular oncology. The author analyzes the design and performance of various ultrasound-sensitive nanocarriers, evaluates their therapeutic efficacy in ocular models, and explores the challenges associated with clinical adoption. By bridging the domains of molecular radiotherapy and ultrasound-mediated delivery, this work provides a comprehensive framework for next-generation strategies in the treatment of ocular malignancies.
Design Strategies for Ultrasound-Responsive Radiopharmaceutical Nanocarriers
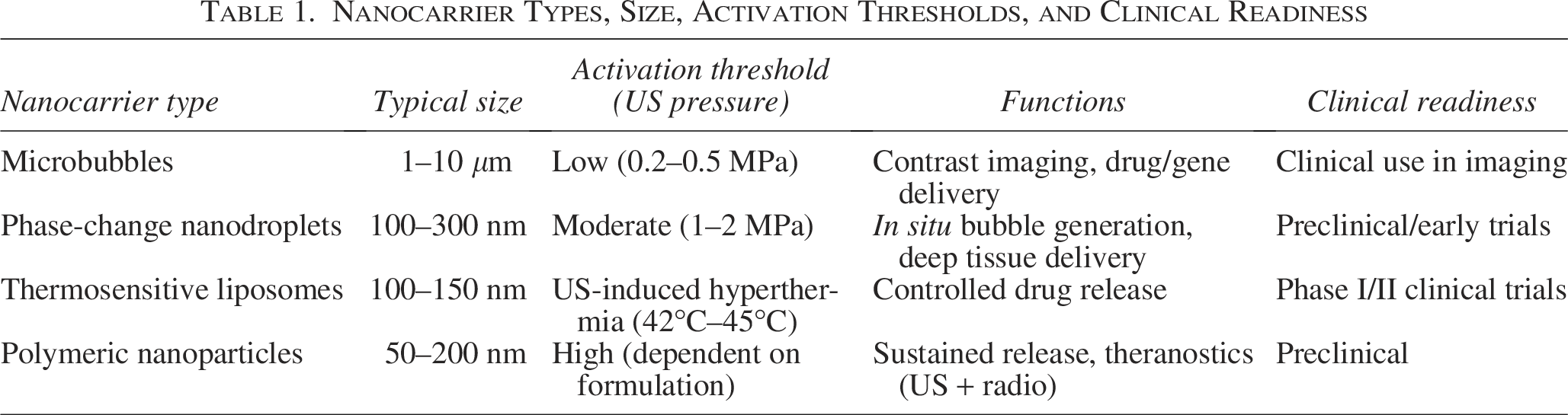
Ultrasound-responsive radiopharmaceutical systems necessitate precisely developed nanocarriers that can respond to sonic stimuli while retaining radiolabel integrity and targeting specificity. Figure 1 shows the mechanistic process of ultrasound-triggered delivery in ocular tissues, which includes nanocarrier injection, ultrasound-mediated activation, transitory barrier modification, and drug release. As shown in Figure 1, these nanocarriers must strike a compromise between physiological stability and the ability to rapidly activate and release drugs upon ultrasonic exposure. Several types of ultrasound-sensitive carriers have emerged as viable platforms for targeted radiotherapy delivery in solid tumors, including ocular cancers. The advantages of ultrasound include precise control of nanocarrier activation, less systemic exposure, and an improved therapeutic index. Risks include cavitation-induced vascular injury, retinal heating, and off-target administration. Mitigation options include optimizing acoustic settings (0.5–2 MHz, <1.5 MPa) and real-time cavitation monitoring. Table 1 represents detailed nanocarrier types, size, activation thresholds, and clinical readiness.
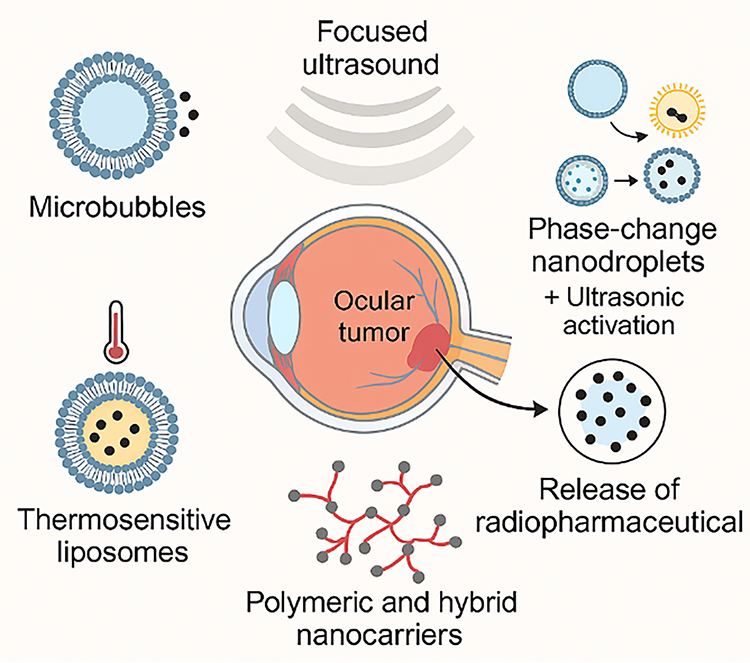
Design strategies for ultrasound-responsive radiopharmaceutical nanocarrier delivery system.
Nanocarrier Types, Size, Activation Thresholds, and Clinical Readiness
Microbubbles
Microbubbles are gas-filled vesicles with lipid or polymer shells that were created for ultrasonic imaging. Because of their strong echogenicity and sensitivity to sonic pressure, they have been used as drug carriers in ultrasound-mediated therapies. Under concentrated ultrasound, microbubbles oscillate or collapse (cavitation), resulting in transitory permeability of adjacent cell membranes or mechanical rupture of the bubble structure. This enables the regulated release of radiopharmaceutical payloads conjugated to their shells or coencapsulated inside the structure. Their micron-scale size restricts their penetration into solid tumor parenchyma, but it makes them extremely effective in vascular-targeted treatments. Despite their established contrast imaging capacity, microbubbles confront translational hurdles such as a limited circulation half-life, the possibility of embolism, and the need for high acoustic pressures, which can damage the sensitive retinal vasculature. Furthermore, ocular administration necessitates smaller scale carriers to accomplish intraocular penetration, limiting the usage of typical clinical microbubbles.
Phase-change nanodroplets
Phase-change nanodroplets are nanometer-sized emulsions made of low boiling-point perfluorocarbons enclosed in a stabilizing shell. When subjected to ultrasound at high enough acoustic pressure, these droplets evaporate and form microbubbles, a process known as ADV. This conversion improves ultrasonography contrast and enables targeted medication or radionuclide release. Their nanoscale size promotes tumor penetration, and their ultrasound-triggered expansion can be used to mechanically destroy tumor vasculature or tissue.
Thermosensitive liposomes
Thermosensitive liposomes are lipid-based vesicles that release their contents during moderate hyperthermia (usually 40°C–42°C). When heated with ultrasound (∼42°C), thermosensitive liposomes release contained medicines. Repeated ultrasonic exposures can disrupt the bilayer, resulting in cumulative leaking. Studies show that stability is formulation-dependent, with cholesterol-enriched liposomes being more resilient after repeated cycles. FUS can cause localized tissue heating, allowing liposomes to release their payloads more precisely. They can be designed to encapsulate radiotherapeutics inside their aqueous core while also providing adjustable features such as PEGylation for longer circulation or pH-sensitive coatings for increased tumor selectivity. The combination of thermal sensitivity and ultrasound-induced heating enables spatiotemporal control over radionuclide administration.
Polymeric and hybrid nanocarriers
Polymeric nanocarriers, including those made from biocompatible materials such as poly(lactic-co-glycolic) acid, chitosan, or dendrimers, offer robust architecture for controlled drug loading and release. These systems can be formulated to respond to ultrasonic cavitation, temperature, or mechanical disruption. Hybrid carriers, which integrate inorganic components (e.g., gold, silica, iron oxide) with polymers, allow for additional functionalities such as magnetic targeting, photoacoustic imaging, or multimodal activation. Their modularity enables precise tuning of release kinetics and biodistribution profiles.
Radiolabel incorporation and carrier stability
When developing ultrasound-responsive radiopharmaceuticals, the radionuclide and chelation method must be carefully considered. The carrier system must keep the radiolabel in circulation and only allow its release or activation at the intended spot. Chelator strength, radiometal selection, and the carrier’s structural integrity under ultrasonic stress all have an impact on the system’s efficacy. Stable radionuclide integration reduces off-target radiation exposure while increasing tumor-specific cytotoxicity.
Preclinical Evaluation in Ocular Malignancy Models
The effective translation of ultrasound-responsive radiopharmaceutical devices into clinical settings is dependent on comprehensive preclinical validation in relevant eye cancer models. Animal studies, particularly those using orthotopic or xenografted ocular malignancies in mice or rabbits, provide essential information on the biodistribution, tumor uptake, therapeutic effectiveness, and safety of these innovative delivery methods.
Model selection and relevance
Intraocular injection of human or mouse retinoblastoma or uveal melanoma cells is commonly used to produce preclinical ocular malignancy models. These models mimic the essential aspects of human ocular malignancies, including intraocular growth dynamics, vascular anatomy, and immunological microenvironment. The model selection (xenograft vs. syngeneic, anterior vs. posterior section) has a direct impact on imaging depth, delivery route, and ultrasound accessibility. While rabbit and mouse models have proven extremely useful in ocular oncology, their limits must be recognized. Rabbit eyes are similar to human eyes in size but differ in vitreous viscosity and immunological response, whereas mouse eyes are much smaller, restricting translation of pharmacokinetics and ultrasonography thresholds. Furthermore, tumor induction models in rodents frequently fail to reproduce the spontaneous heterogeneity of human ocular malignancies. Therefore, preclinical data should be viewed with caution when extending to clinical circumstances. Rabbit models are very suitable for ultrasonic experiments because of their bigger ocular capacity and similar acoustic qualities to humans.
Biodistribution and tumor targeting
Radiopharmaceutical biodistribution after systemic or local injection is often assessed by SPECT/CT or PET imaging. Ultrasound activation promotes intratumoral deposition of radiolabeled carriers by increasing vascular permeability and enabling extravasation via sonoporation. Studies utilizing phase-change nanodroplets or thermosensitive liposomes have demonstrated considerable increases in tumor-to-background ratios when paired with FUS, particularly in animals with intact blood–ocular barriers.
Therapeutic efficacy
Ultrasound-activated administration of β- or α-emitting radiopharmaceuticals significantly improves tumor regression and survival compared with nonactivated controls. These effects are frequently associated by lower systemic toxicity, as ultrasonography allows for targeted release at the tumor location. Repeated treatments with ultrasound-enhanced radiotherapy have been shown to delay tumor progression while causing no structural damage to the surrounding ocular tissues, according to histological and fundoscopic analyses.
Safety and ocular toxicity
Because of the eye’s sensitivity, it is necessary to thoroughly assess off-target radiation exposure, retinal integrity, and immunological response following treatment. Histopathology of the retina, optic nerve, and choroid; electroretinography (ERG) to assess visual function; and ocular imaging to monitor inflammation or bleeding are all part of the safety evaluation process. When high-dose radiopharmaceuticals were paired with ultrasound, preclinical experiments in rabbits and mice revealed localized retinal edema, inflammatory infiltration, and radiation-induced retinopathy. However, these effects were dose-dependent and mostly reversible with optimal ultrasound conditions. Long-term surveillance is necessary to adequately determine eye toxicity. Thermosensitive devices have shown low retinal toxicity, but cavitation-based microbubbles must be precisely adjusted to minimize mechanical damage.
Imaging-guided delivery and monitoring
Real-time ultrasound imaging is frequently utilized to guide and monitor therapy, providing information on carrier localization, cavitation events, and treatment zones. In multimodal systems, PET/ultrasound or SPECT/ultrasound fusion imaging improves spatiotemporal monitoring of radiolabeled drugs, allowing for dynamic pharmacokinetic evaluation and treatment planning.
Challenges and Translational Considerations
While ultrasound-responsive radiopharmaceutical devices show great promise in preclinical research, various biological, technological, regulatory, and clinical challenges must be overcome before general implementation in ocular cancer. Case studies such as the FDA’s clearance of 125I plaque brachytherapy for uveal melanoma show how regulatory routes might influence the translation of radiopharmaceutical nanocarriers. These examples highlight the significance of stability, dosimetry, and patient safety validation. These difficulties originate from the eye’s unique physiological restrictions, the difficulty of nanocarrier design, and the stringent requirements of clinical translation in radiopharmaceutical therapy. While rabbit models show that ultrasound can penetrate the blood–retinal barrier, early human case reports highlight practicality but underscore safety concerns.
Anatomical and physiological constraints
The eye is a highly segmented organ with several barriers preventing drug entry and retention. The blood–retinal barrier and strict intraocular pressure management can impede the systemic and local distribution of nanoparticle-based systems. Patient-specific variability has a substantial influence on delivery results in ocular cancer. Pediatric eyes have lower ocular volumes and thinner scleral walls, which affects ultrasound penetration and medication distribution. Tumor heterogeneity, such as the vascular variations found in uveal melanoma and retinoblastoma, influences carrier accumulation and therapy response. Furthermore, changes in ocular anatomy, such as vitreous density, choroidal thickness, and retinal integrity, must be addressed when optimizing nanocarrier design and ultrasonic settings. FUS provides a technique to temporarily release these barriers, but the settings must be carefully adjusted to avoid retinal detachment, hemorrhage, or inflammation. Furthermore, ocular tissues have different acoustic characteristics, demanding highly specialized and personalized ultrasonic targeting techniques.
Nanocarrier manufacturing and scalability
The clinical translation of ultrasound-responsive nanocarriers depends on reproducible, scalable, synthesis processes that comply with good manufacturing practice (GMP). This includes strict control over particle size, surface chemistry, payload loading, and responsiveness to ultrasound. Thermosensitive liposomes and phase-change droplets, in particular, are highly sensitive to formulation variables such as lipid composition, emulsifier concentration, and radionuclide binding efficiency. In addition, ensuring radiolabel stability during storage and transport remains a critical hurdle for clinical use. Radiopharmaceutical nanocarriers are subject to two sets of regulations: pharmaceuticals and devices. Radiopharmaceuticals must fulfill severe purity, sterility, stability, and dosimetry standards under FDA regulations (21 CFR Part 212), but EMA nanomedicine guidelines emphasize quality-by-design and nanoscale characterization. Translating ultrasound-activated radiopharmaceutical carriers necessitates overcoming obstacles such as dual categorization, limited shelf life of radiolabeled formulations, and repeatability of activation thresholds. Learn from case studies of previously authorized ocular medicines, such as radiolabeled antibodies, to aid regulatory navigation.
Ultrasound equipment standardization
Therapeutic ultrasound must be integrated with diagnostic and delivery systems before it can be used widely in clinical settings. Current FUS platforms have varying acoustic strength, frequency, and beam shaping capabilities. These variations impede consistency between investigations and hinder regulatory approvals. Smaller, precision-guided ultrasound probes are required for ocular applications to reduce off-target effects and allow imaging-assisted delivery within the eye’s limited structure.
Regulatory and safety considerations
Radiopharmaceuticals already face tight regulatory procedures owing to their radioactive nature, and combining them with externally triggered nanocarriers adds to the complexity. Regulatory authorities will demand detailed information on pharmacokinetics, dosimetry, and long-term safety. Ocular toxicity, off-target radiation, immunological response, and carrier system biocompatibility all require careful consideration. Clinical studies must contain ophthalmological objectives such visual acuity, retinal function, and intraocular inflammation.
Clinical trial design and patient selection
Early-phase clinical trials in ocular cancer must overcome recruiting obstacles caused by the rarity of rare intraocular malignancies, as well as the necessity for highly specialized hospitals with nuclear medicine and ocular ultrasonography expertise. Patient selection criteria will be based on tumor location, size, accessibility, and treatment history. Outcome metrics must go beyond tumor reduction to include eyesight preservation, quality of life, and cost–effectiveness when compared with traditional therapy.
Discussion
Ultrasound-responsive radiopharmaceutical devices provide a game-changing strategy in precision oncology, particularly in difficult anatomical situations such as eye cancer. The capacity to modify medication delivery geographically and temporally by ultrasound has a demonstrable benefit in reducing overall toxicity while increasing tumor localization. In ocular cancer, this might allow for a noninvasive, vision-preserving alternative to standard therapies such as enucleation and plaque brachytherapy. 13 Ultrasound-responsive carriers can be used with other imaging modalities to provide multimodal theranostics. For example, PET/US hybrids provide molecular imaging and acoustic activation at the same time, whereas MRI/US systems provide complementing soft-tissue contrast with real-time monitoring. When paired with ultrasonography, OCT improves the vision of small ocular structures as well as therapy response. Such multimodal platforms not only increase diagnostic precision but also speed up the clinical translation of theranostic nanocarriers in ocular cancer. New approaches combine MRI’s high-resolution tissue contrast with OCT’s micron-scale structure imaging. When combined with ultrasound-mediated activation, these modalities give additional anatomical and functional information for ocular tumors, directing precise therapy.
Among the nanocarrier classes investigated, thermosensitive liposomes, phase-change nanodroplets, and polymeric hybrids have shown the most promise for merging radiotherapeutic drugs with ultrasound-triggered release mechanisms.14,15 The choice of isotope for radiolabel incorporation is crucial in terms of half-life compatibility with ocular pharmacokinetics and imaging time frames. Short-lived isotopes, such as 68Ga (t½ = 68 min), can be used for same-day imaging but have limited longitudinal monitoring capabilities. Intermediate isotopes, such as 64Cu (t½ = 12.7 h), provide a compromise between imaging window and patient radiation exposure. Long-lived isotopes, such as 89Zr (t½ = 78 h), allow for multiday theranostic assessment but require stringent dosimetry to avoid radiation-induced ocular damage. Thus, isotope selection must strike a compromise between logistical practicality, safety, and the desired diagnostic or therapeutic use. Their selection was based on their customizable physical qualities, large payload capacity, and biocompatibility. Shin et al. created 64Cu-labeled perfluoropentane nanodroplets for dual PET/ultrasound imaging and targeted activation, displaying real-time theranostic capabilities. 16
Preclinical studies indicate that when combined with targeted ultrasound, these technologies dramatically enhance intratumoral radiopharmaceutical accumulation. In tumor-bearing mice, using ultrasound to activate phase-transition carriers resulted in tumor-to-background ratios more than 5:1, highlighting the improved delivery accuracy.17,18 Furthermore, Bhardwaj et al. found that a triresponsive nanocarrier (ultrasound, redox, and pH-sensitive) enhanced radiosensitization and tumor regression in a mouse model. 19
Despite these breakthroughs, translation into ocular oncology is still in its early stages. While the eye’s anatomical accessibility makes it an excellent option for localized treatments, the fragility of intraocular tissues imposes severe safety limits. Ultrasound disruption of the blood–retinal barrier has been proven to be reversible and nondestructive under carefully regulated acoustic settings,20,21 although the possibility of causing retinal detachment, hemorrhage, or inflammation needs careful optimization.
Carrier stability and radiolabel retention are critical for preserving effectiveness while decreasing off-target radiation. Dual-chelation systems have been studied to increase stability during sonication and circulation. 22 Velikyan et al. found that DOTA-based and mixed-ligand chelators improved in vivo retention of 68Ga and 177Lu during ultrasound-triggered release. 23 Radiolabel integrity is especially important for α- and β-emitting isotopes due to their high cytotoxicity.
On a technological level, clinical implementation of FUS devices for eye treatment presents engineering obstacles. Eye-specific transducers, visual guiding, and real-time feedback systems must be designed and verified. 24 Current technologies built for brain or prostate applications are inadequate for the tiny, curving anatomy of the eye. Nonetheless, advances in high-frequency, low-power transducers provide hope for safer, more targeted activation in ocular tissues. 25
The intricacy of regulations further hinders development. Radiopharmaceuticals must fulfill stringent requirements for isotope purity, half-life validation, and dosimetry. Including a stimulus-responsive feature demands more safety data, especially for long-term ophthalmological results. Agencies will most certainly require extensive preclinical research, including ERG, histopathology, and inflammatory marker analysis. 26
There is also a logistical challenge in expanding nanocarrier manufacturing. Liposomes and nanodroplets exhibit batch-to-batch variation in size, radiolabel incorporation, and release threshold. Before significant clinical studies can begin, large-scale repeatability under GMP conditions must be proven.27,28
The rarity of ocular tumors limits patient pools in clinical trial design, and outcome measures must incorporate more than just tumor reduction, such as vision preservation, ocular toxicity, and patient-reported quality of life. Studies should also investigate using hybrid imaging procedures (PET/ultrasound) to improve treatment planning and monitoring.29,30
Finally, while no clinical trials have yet been conducted to investigate the use of ultrasound-responsive radiopharmaceuticals in ocular malignancies, their use in glioblastoma 31 and breast cancer provides strong proof-of-concept for potential extension into ophthalmic applications.
Conclusion
The combination of ultrasound-responsive devices with radiopharmaceutical drugs marks a significant shift in the targeted treatment of ocular cancers. By utilizing the spatiotemporal precision of FUS, these systems enable controlled activation and targeted radiotherapeutic administration, overcoming significant hurdles provided by the eye’s delicate architecture and physiological constraints.
Preclinical investigations have shown promising results in terms of tumor selectivity, increased radiopharmaceutical absorption, and lower systemic toxicity. Several carrier systems—microbubbles, thermosensitive liposomes, and phase-change nanodroplets—have been tuned for ultrasonic activation and show promise in adapting to intraocular malignancies. Furthermore, developing multimodal techniques that combine imaging and treatment provides new options for real-time monitoring and dosage tailoring.
Despite these advancements, major translational hurdles must yet be overcome. These include the necessity for scalable and repeatable carrier production, accurate ultrasound targeting inside ocular tissues, radiolabel stability under sonic stress, and extensive safety testing. In parallel, regulatory frameworks must change to accommodate the novel mix of radioactive agents and externally triggered delivery methods.
Future directions in this field include creating personalized nanocarriers based on ocular anatomy and tumor phenotype, incorporating AI-assisted ultrasound imaging for precise treatment guidance, and developing next-generation theranostic platforms that combine molecular imaging and targeted therapy. Furthermore, multicenter clinical studies with coordinated regulatory strategies are required to close the gap between preclinical success and clinical acceptance in ocular cancer.
Footnotes
Funding Information
This work was supported by the Talent Research Start-up Project of Eye Hospital of Wenzhou Medical University [grant number KYQD20250402].
Author’s Contributions
Y.Y.: Conceptualization, data curation, visualization, methodology, validation, investigation, formal analysis, and writing and editing the article.