
Abstract
Aim:
This study aims to evaluate the utility of 68Ga-FAPI PET/CT in combination with MAMMI PET for assessing pathological complete response (pCR) to neoadjuvant chemotherapy (NACT) in patients with breast cancer.
Materials and Methods:
This study retrospectively reviewed patients with breast cancer who underwent NACT and had pre/post-therapy imaging with 18F-FDG PET/CT, 68Ga-FAPI PET/CT, and 68Ga-FAPI MAMMI PET. Radiological and histopathological findings before and after treatment were documented. Quantitative PET parameters were calculated, and the post-therapy diagnostic performance of PET imaging was assessed using ROC analysis. Threshold values for detecting residual tumor were calculated, and univariate and multivariate analyses were performed for the breast and axilla.
Results:
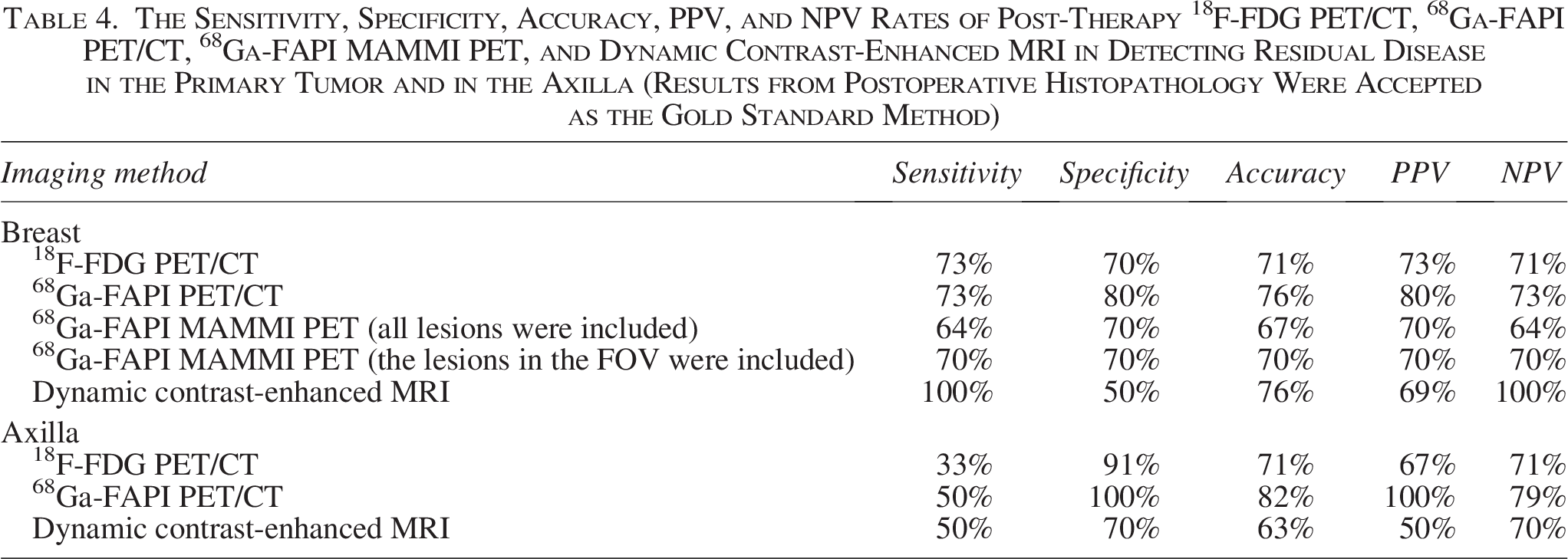
Twenty female patients were included. In visual assessment of residual tumor detection in the breast, the sensitivity, specificity, and accuracy were as follows: 73%, 70%, and 71% for 18F-FDG PET/CT; 73%, 80%, and 76% for 68Ga-FAPI PET/CT; and 64%, 70%, and 67% for 68Ga-FAPI MAMMI PET (all lesions); for detecting residual disease in the axilla, the metrics were: 33%, 91%, and 71% for 18F-FDG PET/CT; 50%, 100%, and 82% for 68Ga-FAPI PET/CT; and 50%, 70%, and 63% for MRI. In quantitative analysis, post-therapy 68Ga-FAPI MAMMI PET tumor background rate (TBR) SUVmax was the only significant parameter in multivariate analysis, demonstrating 91% sensitivity, 80% specificity, and 86% accuracy at a threshold value of 1.35 for detecting residual tumor (p = 0.002; AUC: 0.900; 95% CI: 0.765–1.000).
Conclusions:
The diagnostic performance of quantitative parameters derived from 68Ga-FAPI PET/CT combined with MAMMI PET was superior to current diagnostic methods for determining pCR in the breast; however, the sensitivity in the axilla remains limited. Further research in larger patient groups should be conducted.
Introduction
Neoadjuvant chemotherapy (NACT) is the primary treatment for locally advanced or inoperable breast cancer (BC), as it facilitates breast-conserving surgery by reducing tumor size and may prevent axillary lymph node dissection (ALND). Recently, NACT has also been adopted for early-stage BC.1,2 Previous studies have shown that patients achieving pathological complete response (pCR) after NACT have better survival rates.3,4 Therefore, an accurate assessment of therapy response is crucial, especially for patients who do not achieve pCR, as it impacts prognosis prediction and further treatment planning. 5
Therapy response to NACT in BC is evaluated using both anatomical and molecular imaging methods. It is shown that dynamic contrast-enhanced (dCE) MRI has lower specificity compared to 18F-FDG PET/CT (69% vs. 78%), while its accuracy for determining pathological response is higher (AUC: 0.88 vs. 0.84). 6 Other imaging methods, such as dedicated breast PET (dB PET), have shown promise in improving pCR prediction. Tokuda et al. reported that dB PET had a sensitivity of 85.7% and specificity of 72.7% (AUC: 0.82) compared to 71.4% and 77.3% (AUC: 0.73) for 18F-FDG PET/CT and 100% and 50% (AUC: 0.773) for dynamic contrast-enhanced MRI, suggesting superior diagnostic accuracy of dB PET. 7
Recently, the fibroblast activating protein inhibitor (FAPI) molecule, which targets fibroblast activating protein expressed in cancer-associated fibroblasts, has been reported with promising results in many cancers as an alternative imaging tool to 18F-FDG PET/CT.8,9 68Ga-FAPI PET/CT has been reported to have similar sensitivity but higher specificity and accuracy compared to 18F-FDG PET/CT in detecting primary lesions during BC staging. 10 Limited studies have explored the effectiveness of 68Ga-FAPI PET/CT in evaluating therapy response to NACT. Backhaus et al. demonstrated that therapy response in the breast and axilla could be better assessed with 68Ga-FAPI PET/MR compared to MRI alone, although further studies are warranted. 11
This study explores a concept analogous to the Schrödinger’s cat paradox in quantum physics. This paradox describes a cat in a box that is simultaneously both alive and dead until the box is opened and the cat’s state is observed. Similarly, in this study, the true pathological response to neoadjuvant chemotherapy (pCR or residual disease) can only be definitively determined through postoperative pathological evaluation.
This study aims to evaluate the clinical contribution of 68Ga-FAPI PET/CT in BC patients receiving NACT before the surgery. The primary objective is to evaluate the utility of 68Ga-FAPI PET/CT combined with Mammography with Molecular Imaging PET (MAMMI PET) in the assessment of pCR to NACT in BC patients, with the goal of assessing tumor response without surgery—analogous to determining the state of Schrödinger’s cat without opening the box.
Material and Methods
Patient selection
This study retrospectively reviewed patients diagnosed with local, locally advanced, or oligometastatic BC who received NACT and underwent surgery shortly after therapy. All patients had pre- and post-therapy imaging with 18F-FDG PET/CT, 68Ga-FAPI PET/CT, and 68Ga-FAPI MAMMI PET. Luminal B patients with a Ki-67 value of ≥35%, HER2 positive and triple negative breast cancer patients were included, while. Luminal A and Luminal B patients with a Ki-67 value below 35% were excluded, as pCR rates to NACT are expected to be higher in more aggressive subgroups with greater Ki-67 values, which tend to have a better therapy response. 12 Patients with multimorbidity, a history of radiotherapy on the breast, or concurrent malignancies were also excluded. Written informed consent was obtained from all participants. The study was approved by the Istanbul Faculty of Medicine Ethics Committee on December 1, 2023 (File Number: 2023/2077).
Imaging protocols
Pretherapy PET/CT, MAMMI PET, and MRI acquisitions were performed before the first cycle of chemotherapy. Post-therapy 18F-FDG PET/CT acquisitions were performed at least 2 weeks after the last cycle of chemotherapy (median time interval: 15 days, range: 14–18 days). Post-therapy 68Ga-FAPI PET/CT and MAMMI PET acquisitions were performed at least 1 week after the last cycle (median time interval: 9 days, range: 7–12 days), and post-therapy MRI acquisitions were performed within 1 month after the last cycle (median time interval: 14 days, range: 10–30 days). Surgery was scheduled within a month after PET/CT acquisitions (median interval: 22 days for 18F FDG PET/CT; 28 days for 68Ga FAPI PET/CT).
18F-FDG PET/CT
After fasting for at least 6 h, patients received 3.7–7.4 MBq/kg (0.1–0.2 mCi/kg) of 18F-FDG intravenously. Imaging was performed approximately 1 h post-injection using a GE Healthcare IQ Discovery PET/CT device, with low-dose CT (140 kV, 50 mAs) and PET images acquired from vertex to knee (6–8 beds, 2 min/bed).
68Ga-FAPI PET/CT
68Ga-FAPI PET/CT was performed using 68Ga-FAPI-04 radiopharmaceutical according to established protocols. 13 Patients received 1.85–3.7 MBq/kg (0.05–0.1 mCi/kg) of 68Ga-FAPI intravenously. Imaging was conducted 25–45 min post-injection with the same device, using low-dose CT (140 kV, 50 mAs) and PET images (6–8 beds, 4 min/bed).
MAMMI PET
MAMMI PET (Oncovision, Spain) images were acquired approximately 60 min after 68Ga-FAPI injections and following the completion of the 68Ga-FAPI PET/CT scan. Imaging was performed for 3–7 beds, 3.5 min/bed, with the patient in a prone position and the breast within the ring detector. Contralateral breast imaging was performed when clinically necessary.
Dynamic contrast-enhanced MRI
The dynamic contrast-enhanced (dCE) MRI examination of both breasts was performed using FLASH 3D axial and sagittal sequences following the intravenous injection of 20 mL of contrast agent.
Analysis of the images
Images from 18F-FDG PET/CT, 68Ga-FAPI PET/CT, and MAMMI PET were reviewed by two experienced nuclear medicine specialists and a radiology specialist. Images from dCE MRI were reviewed by an experienced radiology specialist. Clinical data including age, clinical stage, lesion localization, solitary or multifocal tumors, and axillary lymph node (ALN) involvement were documented.
All PET images underwent visual and quantitative assessment. TBR was calculated from contralateral breast parenchyma in PET/CT images and from the point furthest from the lesion in MAMMI PET images. Metabolic tumor volume (MTV) and tumor lesion glycolysis (TLG) values were calculated based on the 41% threshold per EANM guidelines. 14 For 68Ga-FAPI PET/CT and 68Ga-FAPI MAMMI PET, FAPI-TV and FAPI-TL values were calculated similarly.
The response evaluation criteria were as follows: no detectable FDG or FAPI uptake defined as a complete response (CR); a decrease in uptake by greater than 30% considered a partial response; changes in uptake within ±30% were classified as stable disease; and an increase in uptake by greater than 30% termed progressive disease. These findings were compared with radiological and histopathological results.
Pathological assessment
Post-NACT breast surgeries of the patients were performed within a month after the last cycle of chemotherapy. Breast excision or mastectomy specimens were thoroughly sampled and microscopically evaluated, focusing on the tumor bed area. The pathological complete response (pCR) was defined as the absence of invasive cancer in both the breast and ALNs, regardless of the presence of residual ductal carcinoma in situ (DCIS) in the breast or isolated tumor cells in the axilla. 15
Statistical analysis
The diagnostic performance of quantitative parameters such as SUVmax-mean, TBR SUVmax-mean, MTV/FAPI-TV, TLG/FAPI-TL, and delta SUVmax-mean derived from pre/post-treatment 18F-FDG PET/CT, 68Ga-FAPI PET/CT, and 68Ga-FAPI MAMMI PET, and noncategoric parameters such as tumor size and Ki-67% for detecting pathologically proven residual tumors was evaluated using ROC analysis. Sensitivity and specificity for the detection of residual tumor in the breast and axilla were calculated by determining threshold values. Univariate analysis using a logistic regression model was performed, and multivariate analysis was applied for statistically significant parameters. Statistical analyses were conducted with IBM SPSS version 24.0, considering a p-value below 0.05 as significant.
Results
Twenty female patients were enrolled in the study. Nineteen patients had unilateral BC, and one patient had bilateral BC. Clinical, histopathological, and molecular characteristics at the time of initial diagnosis are shown in Table 1.
Clinical, Histopathological, and Molecular Characteristics of the Patients
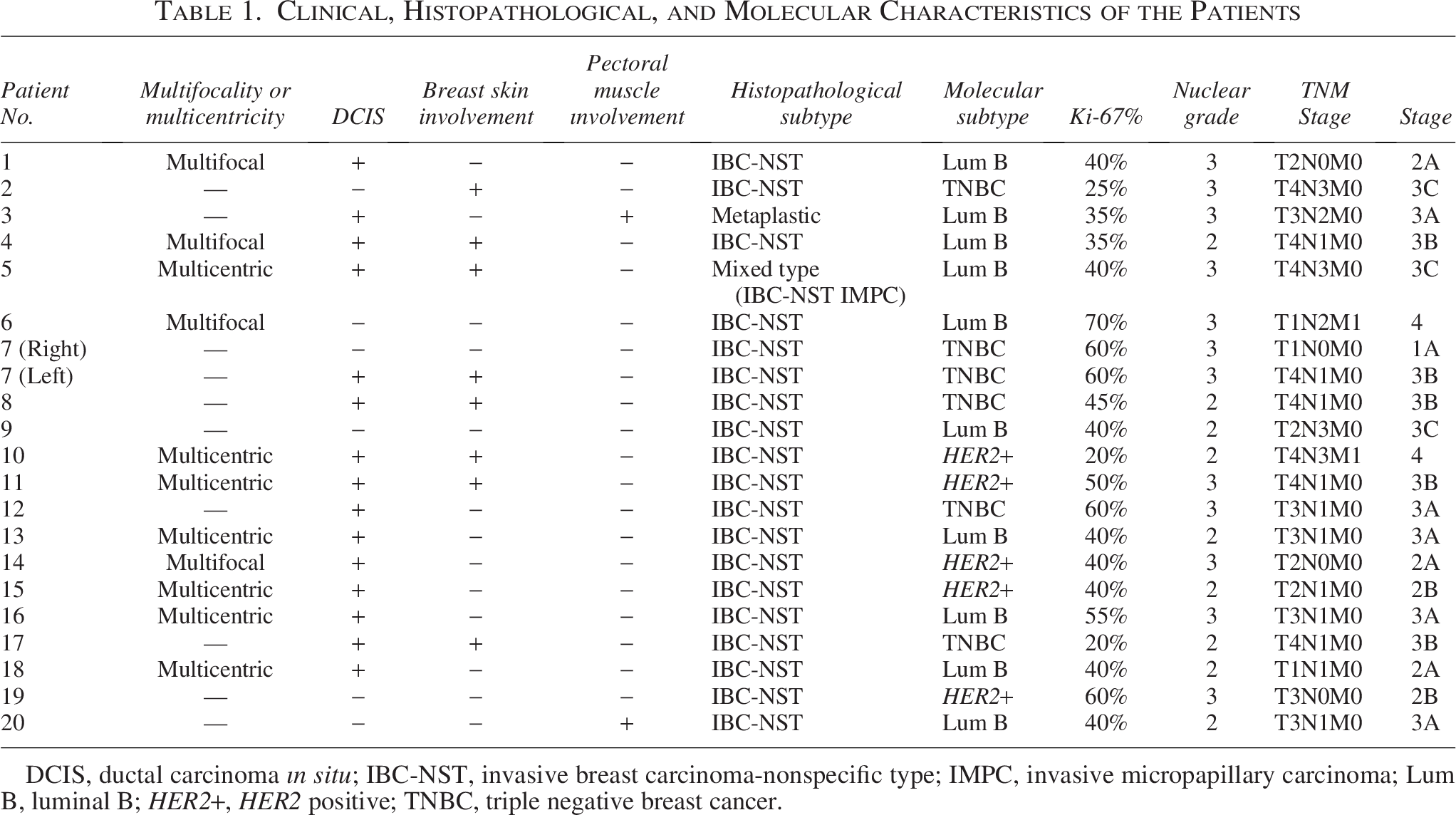
DCIS, ductal carcinoma ın situ; IBC-NST, invasive breast carcinoma-nonspecific type; IMPC, invasive micropapillary carcinoma; Lum B, luminal B; HER2+, HER2 positive; TNBC, triple negative breast cancer.
Final staging results
The final diagnosis identified 35 malign invasive lesions, 15 DCIS lesions, and 7 benign lesions in 20 patients. Skin or nipple involvement (SNI) was determined in eight patients. Seventeen patients (85%) had at least one ipsilateral axillary lymph node (ALN) metastasis. Thirteen of them had only ipsilateral ALN metastases and conglomerated in six of them. Additionally, two patients had supraclavicular lymph node (LN) metastasis, and two patients had ipsilateral ipsilateral internal mammary (IMA) lymph node metastasis.
Two patients (10%) were classified as M1 stage. One patient had a sternal bone metastasis and a mediastinal LN metastasis, and the other patient had a contralateral ALN metastasis, which was revealed as oligometastatic disease.
Assessment of Therapy Response to NACT
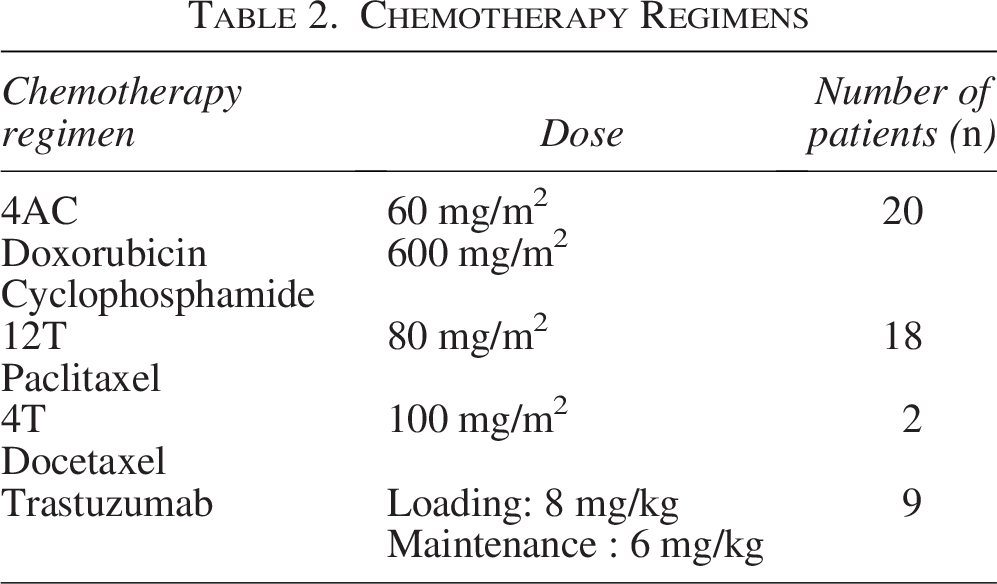
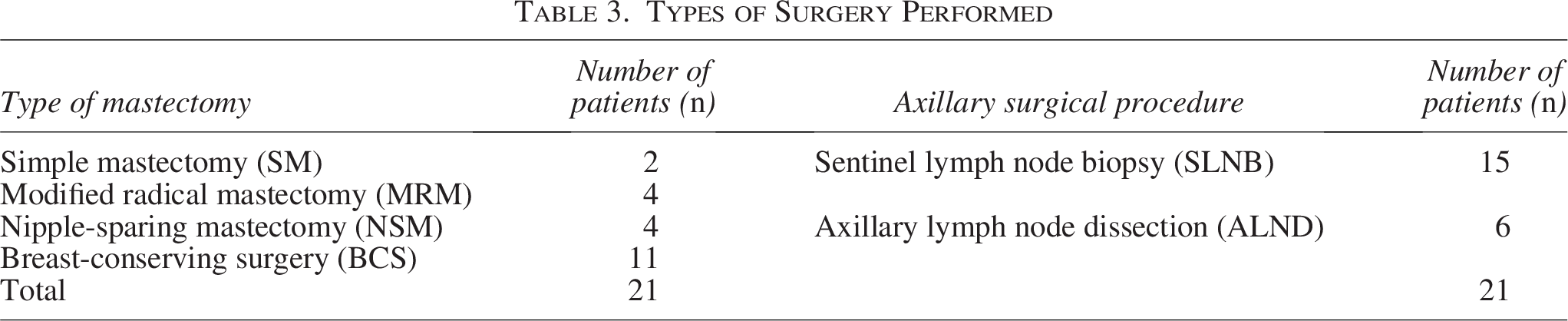
The administered chemotherapy regimens are detailed in Table 2, while the types of breast and axillary surgeries performed are summarized in Table 3. All 20 patients received 4 cycles of AC (doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2). Of these, 18 patients received 12 cycles of paclitaxel (80 mg/m2), and 2 patients received 4 cycles of docetaxel (100 mg/m2). In addition, nine patients with HER2 positivity on immunohistochemical analysis received trastuzumab (loading dose 8 mg/kg, maintenance dose 6 mg/kg).
Chemotherapy Regimens
Types of Surgery Performed
Pathological findings in breast and ipsilateral ALN
Postoperative histopathology showed pCR in 10 breasts (47.6%) and pathological partial response (pPR) in 11 breasts (52.4%). Residual DCIS was found in four of the pCR cases. Residual SNI persisted in two of eight patients with SNI.
Among 17 patients with ipsilateral ALN metastases, 11 patients achieved pCR, while 6 patients had pPR. Isolated tumor cells were present in one pCR case.
Final findings for extraaxillary metastasis
Residual tumors were defined in two of four patients with supraclavicular and ipsilateral IMA LN metastases. In patients with bone metastasis in the sternum and contralateral ALN metastases, CR was defined in the sternum, based on imaging findings of post-therapy PET/CT and MRI, and pCR was determined in contralateral ALN metastasis by histopathological findings.
18F-FDG PET/CT therapy response visual assessment
18F-FDG PET/CT identified pCR in 7/10 breasts and residual tumors in 8/11 cases. A false positive occurred in three pCR patients, and one of them had only residual DCIS.
18F-FDG PET/CT defined pCR in the ipsilateral ALN in 10/11 cases and residual tumor in 2/6 cases. A false positive occurred in one pCR patient, while the NACT responses were correctly identified in four patients with extraaxillary LN metastases. 18F-FDG PET/CT revealed CR in the bone metastasis in the sternum and contralateral ALN metastases after NACT.
68Ga-FAPI PET/CT therapy response visual assessment
68Ga-FAPI PET/CT identified pCR in 8/10 breasts and residual tumors in 8/11 patients. False positive occurred in two pCR patients, and one of them had only residual DCIS.
68Ga-FAPI PET/CT defined pCR in the ipsilateral ALN in 11/11 cases and residual tumor in 3/6 cases. 68Ga-FAPI PET/CT correctly determined the NACT response in four patients with extraaxillary LN metastases and revealed CR in the bone metastasis in the sternum and contralateral ALN metastases.
68Ga-FAPI MAMMI PET therapy response visual assessment
68Ga-FAPI MAMMI PET identified pCR in 7/10 breasts and residual tumors in 7/11 patients (Fig. 1). False negatives occurred in four pPR patients, and in one of them residual tumor was out of the field of view. False positives occurred in three pCR patients, and two of them had only residual DCIS.
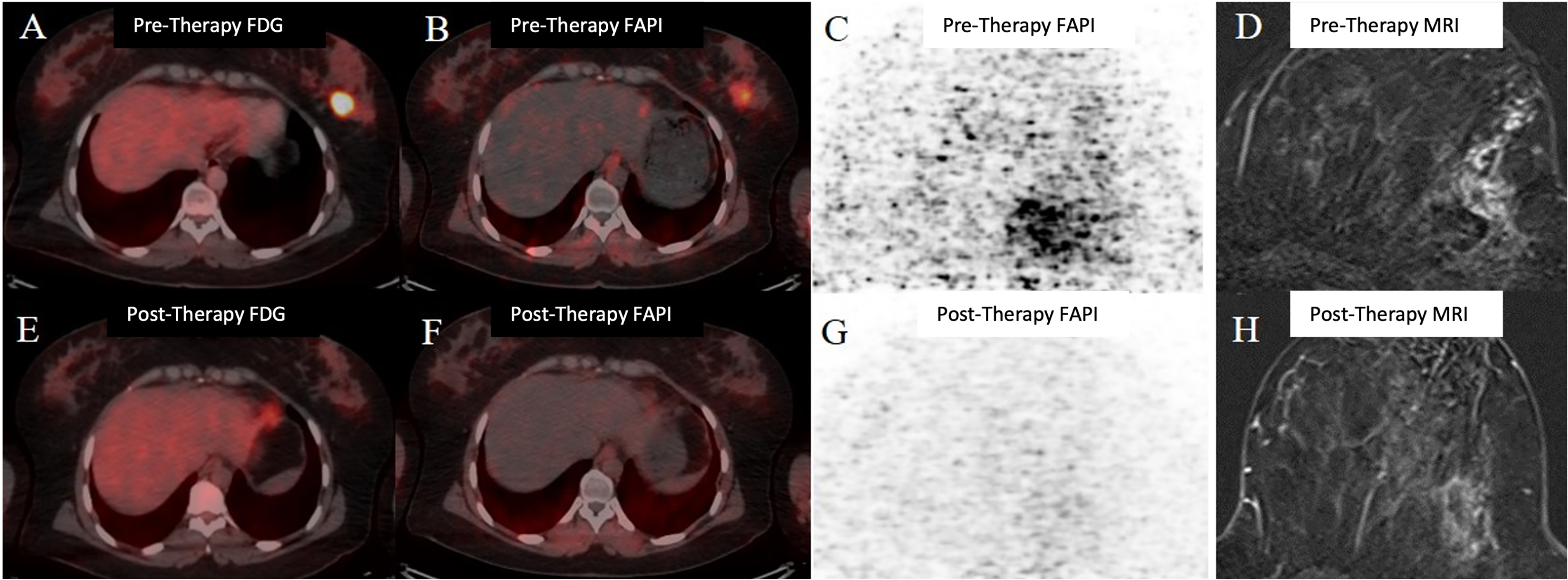
A 39-year-old female patient with T2N0M0 breast cancer in the left breast had the primary tumor shown in pretherapy 18F-FDG PET/CT
MRI therapy response visual assessment
MRI identified pCR in 5/10 breasts and residual tumor in 11/11 patients. False positives occurred in half of the pCR patients (Figs. 1 and 2), and three of them had only residual DCIS.
MRI defined pCR in ipsilateral ALN in 7/11 patients, and the response could not be evaluated in one patient since the LN was out of the field. False positives occurred in three pCR patients, and false negatives occurred in three pPR patients.
The sensitivity, specificity, PPV, NPV, and accuracy rates of post-therapy 18F-FDG PET/CT, 68Ga-FAPI PET/CT, 68Ga-FAPI MAMMI PET, and MRI in detecting residual metastases in breast, as well as those of post-therapy 18F-FDG PET/CT, 68Ga-FAPI PET/CT, and MRI in ALN were given in Table 4.
The Sensitivity, Specificity, Accuracy, PPV, and NPV Rates of Post-Therapy 18F-FDG PET/CT, 68Ga-FAPI PET/CT, 68Ga-FAPI MAMMI PET, and Dynamic Contrast-Enhanced MRI in Detecting Residual Disease in the Primary Tumor and in the Axilla (Results from Postoperative Histopathology Were Accepted as the Gold Standard Method)
Semi-quantitative findings of PET imaging in therapy response assessment
ROC analysis revealed that TBR SUVmean derived from pretherapy 68Ga-FAPI MAMMI PET, and TBR SUVmean, TBR SUVmax, and primary tumor SUVmean derived from post-therapy 68Ga-FAPI MAMMI PET, and TBR SUVmax value derived from post-therapy 68Ga-FAPI PET/CT were significant parameters to determine residual tumor in breast. Among them, the most significant parameter was TBR SUVmax of post-therapy 68Ga-FAPI MAMMI PET; the sensitivity was 91%, and the specificity was 80% considering the threshold value of 1.35 (p = 0.002; AUC: 0.900; 95% CI: 0.765–1.000) (Fig. 1 and Fig. 2). However, other PET parameter including MTV/FAPI-TV, TLG/FAPI-TL, delta SUVmax, delta SUVmean of primary tumor, and none of the PET parameters of ALN were found statistically significant in detecting residual tumor in ALN metastasis.

A 57-year-old female patient with left breast cancer. In staging 18F-FDG PET/CT
The statistically significant parameters in the assessment of therapy response in breast were evaluated with logistic regression analysis. TBR SUVmax, value derived from post-therapy 68Ga-FAPI PET/CT was not significant in univariate analysis (p > 0.05), while other parameters derived from 68Ga-FAPI MAMMI PET were found as statistically significant (p = 0.005–0.024). Among them, only the TBR SUVmax value derived from post-therapy 68Ga-FAPI MAMMI PET was statistically significant in the multivariate analysis (p = 0.015, Exp(ß): 32.7). The result of semi-quantitative parameters in the assessment of therapy response after NACT is given in detail in Table 5.
Receiver Operating Characteristics, Univariate and Multivariate Analysis of Quantitative PET Parameters in Detecting Residual Disease in the Primary Tumor (Results from Postoperative Histopathology Were Accepted as the Gold Standard Method)
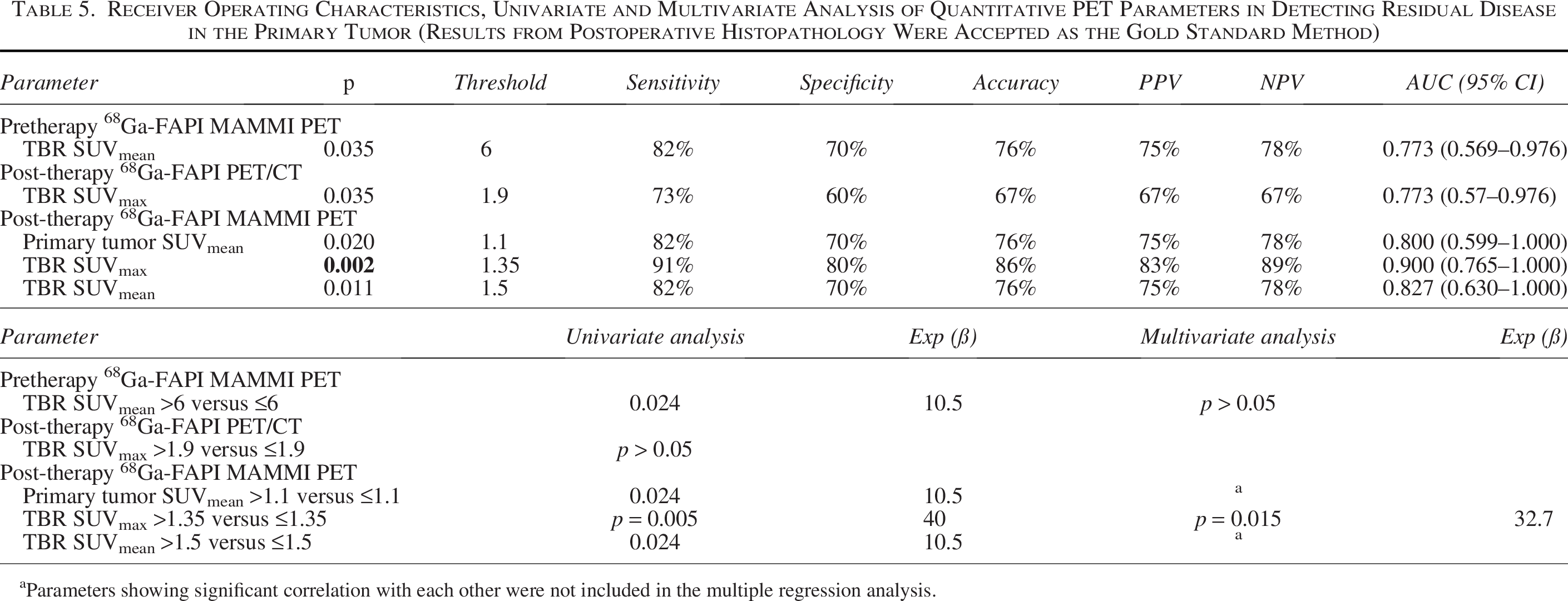
Parameters showing significant correlation with each other were not included in the multiple regression analysis.
Discussion
Surgery remains the standard approach following NACT in BC if no progression/recurrence is detected. However, the necessity of surgery in patients achieving pCR is still under debated. Ozkurt et al. reported no significant difference in 5-year survival rates between patients who underwent surgery and those followed up without surgery after achieving pCR (96.8% vs. 92.5%; p = 0.15). 16 Similarly, the OPTIMIST trial showed that patients with pCR confirmed by vacuum biopsy and MRI, who underwent only radiotherapy, hormone therapy, and targeted therapies, achieved a 5-year disease-free survival rate of 88% without surgery. 17 These findings support the monitoring of pCR patients with only radiotherapy and systemic treatments, instead of surgery, which may help avoid surgical complications as well as negative cosmetic and psychological effects. However, current diagnostic methods are considered insufficient for accurate evaluation of the pathological response, 18 highlighting the need for alternative imaging methods with higher diagnostic accuracy for assessment of therapy response after NACT in breast cancer patients.
Previous studies have demonstrated that 68Ga-FAPI PET/CT exhibits higher specificity and accuracy compared to 18F-FDG PET/CT in staging BC.10,19 However, limited research has indicated the efficacy of 68Ga-FAPI PET/CT in the assessment of therapy response to NACT.20,21 This work investigated the utility of 68Ga-FAPI PET/CT combined with MAMMI PET in the assessment of pCR following NACT in BC patients. Based on visual assessment, the sensitivity, specificity, and accuracy of 68Ga-FAPI PET/CT for the detection of residual disease in the breast after NACT were 73%, 80%, and 76%, respectively. Combination of 68Ga-FAPI PET/CT and MAMMI PET reduced false positives to one patient with DCIS following NACT but missed 3 of 10 patients with residual disease in the visual interpretation. The visual assessment findings of 68Ga-FAPI PET/CT ± MAMMI PET were not satisfactory, since undetermined residual tumors can increase the risk of recurrence if patients are followed up without surgery. In contrast, the semi-quantitative results appeared promising for defining residual disease in breast, particularly when 68Ga-FAPI PET/CT was combined with MAMMI PET. The sensitivity, specificity, and accuracy for TBR SUVmax value of 68Ga-FAPI MAMMI PET (threshold: 1.35) were satisfying: 91%, 80%, and 86%, respectively (p = 0.002; AUC: 0.900; 95% CI: 0.765–1.000). Using this threshold, only one patient with a residual tumor was missed. So far, only a limited number of studies have investigated the role of 68Ga-FAPI PET/CT or PET/MRI in determining NACT response in BC.11,20,21 Backhaus et al. reported that the sensitivity for detecting pCR using visual assessment with 68Ga-FAPI PET/MRI and MRI was 100% for both, while the specificity was 71% and 61%, respectively. 11 Furthermore, they indicated that the TBR SUVmax values of the patients with pCR were significantly lower than those of patients with non-pCR (p = 0.001), with 100% sensitivity and specificity for the detection of pCR using TBR SUVmax values. Moreover, Chen et al. evaluated pretherapy, interim, and post-therapy 68Ga-FAPI PET/CT scans of 21 BC patients receiving NACT and revealed that the highest diagnostic efficiency for detecting pCR in the breast was achieved using TBR SUVmax values, yielding 100% sensitivity, 93.3% specificity, 85.7% PPV, and 100% NPV. 20 Moreover, Zheng et al. indicated the clinical relevance of quantitative PET parameters in detecting pCR in interim and post-NACT images and showed the existence of statistically significant differences in ΔSUVmax, ΔSUVmean, ΔFTV (FAPI-TV), and ΔTLF (FAPI-TL) between pCR and non-pCR patient groups. 21 The semi-quantitative findings of this study agree with these studies, supporting the clinical utility of combined 68Ga-FAPI MAMMI PET as a potential alternative imaging modality for detecting pCR in breast.
Our findings suggest that semi-quantitative assessment using 68Ga-FAPI MAMMI PET TBR SUVmax values may diminish this false-positive interpretation. Backhaus et al. also mentioned DCIS as a limitation for 68Ga-FAPI PET/MRI for accurate assessment of pCR, 11 considering the previous studies declared that approximately 12% of patients may have DCIS after NACT.22,23 Based on the authors’ knowledge, this is the first study utilizing MAMMI PET, which can cause false positivity in the presence of DCIS due to the higher spatial resolution.24,25 Regressive fibrosis following NACT may contribute to the false positivity in 68Ga-FAPI PET/CT, as FAP expression in the fibrosis areas has been well described in the literature. 26
In the study’s cohort, the sensitivity, specificity, and accuracy for 18F-FDG PET/CT based on visual assessments were 73%, 70%, and 71%, while for MRI, they were 100%, 50%, and 76%, respectively, for defining residual disease in the breast. Semi-quantitative findings of 18F-FDG PET/CT were not significant. Several studies have investigated the efficacy of 18F-FDG PET/CT and MRI in determining pCR after NACT in BC.27,28 Meta-analyses reported pooled sensitivity and specificity of MRI for detection of pathological response in the breast as 88% and 55–69%, respectively, while for 18F-FDG PET/CT, they were 71–77% and 77–84%.6,29 In the present study, 18F-FDG PET/CT findings were consistent with the literature, whereas MRI demonstrated higher sensitivity in determining pathological responses in small patient cohort. Although MRI demonstrated all residual tumors in the breast, it yielded false positives in 5/10 patients who achieved pCR. On the other hand, TBR SUVmax value of 68Ga-FAPI MAMMI PET demonstrated acceptable sensitivity and superior specificity and accuracy compared to MRI.
Sentinel lymph node biopsy (SLNB) is routinely performed to evaluate the pathological response to NACT in patients with ALN metastasis. 30 Although few LNs are excised in SLNB, complications such as lymphedema, nerve damage, infection, and bleeding can occur in 5% of patients. 31 Therefore, accurate diagnosis of pCR in ALNs is valuable to avoid unnecessary SLNB. A meta-analysis reported the pooled sensitivity and specificity of MRI for detecting residual tumor in ALNs as 63% and 75%, respectively (AUC: 0.76), 32 while for 18F-FDG PET/CT, the sensitivity and specificity were 38% and 86%. 33 Another study defined the sensitivity, specificity, PPV, and NPV of axillary ultrasonography in predicting pCR as 29%, 77.5%, 69%, and 38.5%, respectively. 34 Current imaging methods are insufficient to replace SLNB in determining the pathological response in ALN metastasis. In this study, neither visual nor semi-quantitative assessments of 68Ga-FAPI PET/CT were efficient to detect residual metastasis in ALNs. 68Ga-FAPI PET/CT yielded false negatives in half of the patients with residual disease in ALN, as well as MRI. On the other hand, 68Ga-FAPI PET/CT had no false positive results in ALNs, unlike MRI, which was falsely positive in 3/10 pCR patients. Backhaus et al. also noted that 68Ga-FAPI PET/MRI could miss residual disease in ALNs but reported no false-positive ALN. 11 It seems that 68Ga-FAPI PET/CT is not capable of replacing SLNB; however, its high PPV for ALNs may still be useful in post-NACT therapy management.
Our study has several limitations, primarily due to its retrospective design. 18F-FDG MAMMI PET was available for only a limited number of cases and could not be included in the study. Nonetheless, the primary objective was to determine the clinical contribution of 68Ga-FAPI PET/CT and its combination with MAMMI PET, as previous studies have already addressed 18F-FDG MAMMI PET findings. 24 Due to the technical characteristics of the MAMMI PET device, deeply located lesions (close to the pectoral muscle) may remain outside the MAMMI PET field of view, which can lead to a reduction in the sensitivity of the MAMMI PET. The small patient population was another limitation, like previous studies.11,20,21 Post-therapy 18F-FDG PET/CT acquisitions were performed at least 2 weeks after the last chemotherapy cycle to reduce the risk of false-positive findings related to treatment-induced inflammation. In contrast, to the best of the authors’ knowledge, no standardized imaging interval has been established for 68Ga-FAPI PET/CT or MRI following NACT. Therefore, these scans were conducted within a time frame of 1 week to 1 month after the final chemotherapy cycle.
Furthermore, only patients with aggressive histopathological subtypes were included, as they were expected to achieve a pCR after NACT. The role of 68Ga-FAPI PET/CT in patients who had received NACT for Luminal A, low Ki-67%, or invasive lobular breast carcinoma should be investigated with further studies. Additionally, ethical considerations prevented histopathological verification of all lesions, particularly for distant metastases.
Conclusions
Our findings indicate that the semi-quantitative analysis of post-NACT TBR SUVmax derived from 68Ga-FAPI PET/CT combined with MAMMI PET is a promising method for determining pCR in the breast after NACT, offering high sensitivity and specificity. However, despite the notable specificity of 68Ga-FAPI PET/CT for response assessment in the axilla, its sensitivity is limited in post-NACT imaging, and it cannot replace SLNB. Future research should investigate larger populations, including patients with less aggressive histology, to further validate the findings of this study.
Authors’ Contributions
M.O.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software supervision, validation, visualization, writing—original draft, and writing—review and editing. D.H.S.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing—original draft, and writing—review and editing. R.Y.: Conceptualization, data curation, formal analysis, methodology, resources, software, supervision, and visualization. N.C.: Conceptualization, data curation, methodology, resources, and supervision. S.O.: Conceptualization, data curation, formal analysis, investigation, resources, supervision, and writing—original draft. E.G.I.: Conceptualization, data curation, investigation, methodology, resources, software, supervision, and writing—original draft. Z.G.O.: Conceptualization, data curation, funding acquisition, investigation, project administration, resources, software, supervision, writing—original draft, and writing—review and editing. A.A.: Conceptualization, data curation, investigation, methodology, project administration, resources, and supervision. Y.S.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, writing—original draft, and writing—review and editing. S.K.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing—original draft, and writing—review and editing.
Footnotes
Author Disclosure Statement
All authors declare no conflicts of interest.
Funding Information
No funding was received for this article.
Ethical Approval
All procedures performed in studies involving human participants were by the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.