
Abstract
Background:
Pancreatic ductal adenocarcinoma (PDAC) has one of the poorest treatment responses since it contains desmoplastic stroma, lacks good vascularity, and has high interstitial fluid pressures, which are the most damaging factors depriving chemotherapy. Liposomal doxorubicin is much better in terms of systemic pharmacokinetics but is not efficient in PDAC due to the significant barrier of nanoparticles-stromal and vascular barriers.
Purpose/Hypothesis:
In a bid to eliminate these shortcomings, this paper presents CavitoMod-UTMDNet, which is an integrated mechanistic and experimental platform capable of utilizing ultrasound-targeted masterpiece unaffiliating (UTMD) as a means of temporarily improving vascular and stromal permeability and better intratumoral delivery of liposomal doxorubicin.
Population/Subjects:
The model combines Rayleigh-Plesset cavitation modeling and Fickian diffusion analysis with a two-compartment pharmacokinetic model and systematic in vitro and in vivo validation.
Assessment:
Passive cavitation detection was used to establish stable cavitation exposure windows within FDA-acceptable mechanical index limits.
Statistical Tests:
UTMD increased intracellular drug uptake 3.2-3.8fold and reduced IC 0 in PANC-1 and BxPC-3 pancreatic cancer cell lines by around 50% in the presence of a stable cavitation (MI 1.2). UTMD progressively improved the level of intratumor drug delivery in the orthotopic immunodeficient mouse models (NU/NU strain) (2.4-fold) and led to a 54% decrease in tumor volume 21 days later without any trace of hepatic, renal, and cardiac toxicity.
Results:
There were strong links between cavitation energy density and drug uptake and diffusion depth and therapeutic response as evidence that there is a mechanistic character to UTMD-enhanced actions. It will support the drug development in a better way. CavitoMod-UTMDNet is a combined strategy to maximize ultrasound-enhanced nanocarrier (nanoparticles) delivery using a physics-based reproducible plan to optimize ultrasound-enhanced nanocarrier delivery in PDAC that will see improvement in future translation to image-guided therapeutic strategies.
Keywords
Introduction
Pancreatic ductal adenocarcinoma (PDAC) constitutes one of the most harmful and recalcitrant cancers globally, being the seventh largest cancer-related killer and the lowest 5-year survival rate of less than 10%.1,2 This is mainly because of its low clinical presentation and late diagnosis, lack of surgical induced eligibility, high metastatic and high resistance to regular integrations of chemotherapy and radiotherapy. The biophysical hallmark of PDAC include the presence of dense desmosympathetic stroma, hypovascularity, and the high interstitial fluid level, all of which hamper the intratumoral perfusion and severely limit the drug penetration.3–6 These physical obstacles result in the spatially nonhomogeneous distribution of drugs and subtherapeutic levels observed inside tumors, which is one of the greatest impediments toward improving clinical outcomes. 7
The chemotherapeutics, such as liposomal doxorubicin, have been engineered using nanocarriers to improve pharmacokinetic profiles compared with their free drug counterparts (free drugs are more associated with increases in systemic toxicity).8–10 Nonetheless, systemic benefits of such formulations are mildly effective in PDAC because of impaired stromal transport, poor vascular extravasation and swift sequestration by the tumor microenvironment. 11 As the fibroinflammatory environment of PDAC is a unique barrier to the movement of nanoparticles,12,13 approaches that transiently and safely alter the vascular and stromal permeability are not only urgent but also necessary.
Earlier stromal modulation strategies like the enzyme degradation of extracellular matrix (ECM) elements (e.g., depleting hyaluronan) had been associated with the transient augmentation of perfusion but were associated with unreasonable incident toxicities, immunosuppression, and a track record of limited clinical palatability.12–14 These shortcomings of pharmacological stromal depletion support the necessity to develop noninvasive, image-directed, reproducible approaches that can cause specific modifications of tumor transport without causing systemic toxicities.
UTMD has become an emerging technology in attempts to utilize acoustic cavitation to temporarily and spatially elevate vascular and stromal permeability.15–17 UTMD uses nonthermal mechanical vibrations of microbubbles delivered intravenously in comparison with high-intensity focused ultrasound (HIFU), which causes endothelial junctions to open temporarily and irreversibly, and causes stromal vehicle to diminish, resulting in drug extravasation within approved FDA limits of acceptable safety (MI ≤ 1.2).18–21 UTMD increases intratumoral drug uptake in preclinical models of hepatocellular carcinoma, glioblastoma, and breast cancer by factors of between two- and fourfold.22–25
Nevertheless, in the emerging PDAC mentioned as having low stromal microarchitecture, tissue rigidity poses dissimilar challenges to acoustic propagation and cavitation-dependent transportation of drugs.26–28 More to the point, all the past PDAC studies have not combined UTMD with a mechanistic modeling to express quantitative relationships between acoustic parameters, cavitation behavior, stromal remodeling, and enhanced drug delivery performance. Existing UTMD literature uses empirical tuning of parameters, and this is not sufficiently computationally rigorous to provide reproducible and clinically translatable protocols.29–31 Since the stromal properties of PDAC differ significantly from those of other solid tumors, parameter regimes tested in hepatic or breast tumors cannot be easily applied.
The current study can provide gaps to fill due to the experimental modeling of acoustic cavitation, Fickian diffusion modeling, and two-compartment model pharmacokinetic modeling, as well as multimodal experimental validation to provide a comprehensive scheme of optimization of UTMD-enhanced liposomal doxorubicin delivery in PDAC. This is a mechanistically directed UTMD parameter hypothetical model that can precisely alter the stromal structure of PDAC, alter vascular permeability, and dramatically boost intratumoral drug exposure outcomes in enhancing therapeutic effectiveness without surpassing FDA ultrasound exposure standards.
A conceptual overview is shown in Figure 1, illustrating UTMD-mediated stromal modulation and drug delivery enhancement.
Schematic overview of UTMD-enhanced liposomal doxorubicin delivery in PDAC. Illustration of UTMD mechanism showing microbubble cavitation transiently disrupting vascular endothelial junctions and stromal collagen to enhance liposomal doxorubicin extravasation and penetration into pancreatic tumors. PDAC, pancreatic ductal adenocarcinoma; UTMD, ultrasound-targeted microbubble destruction.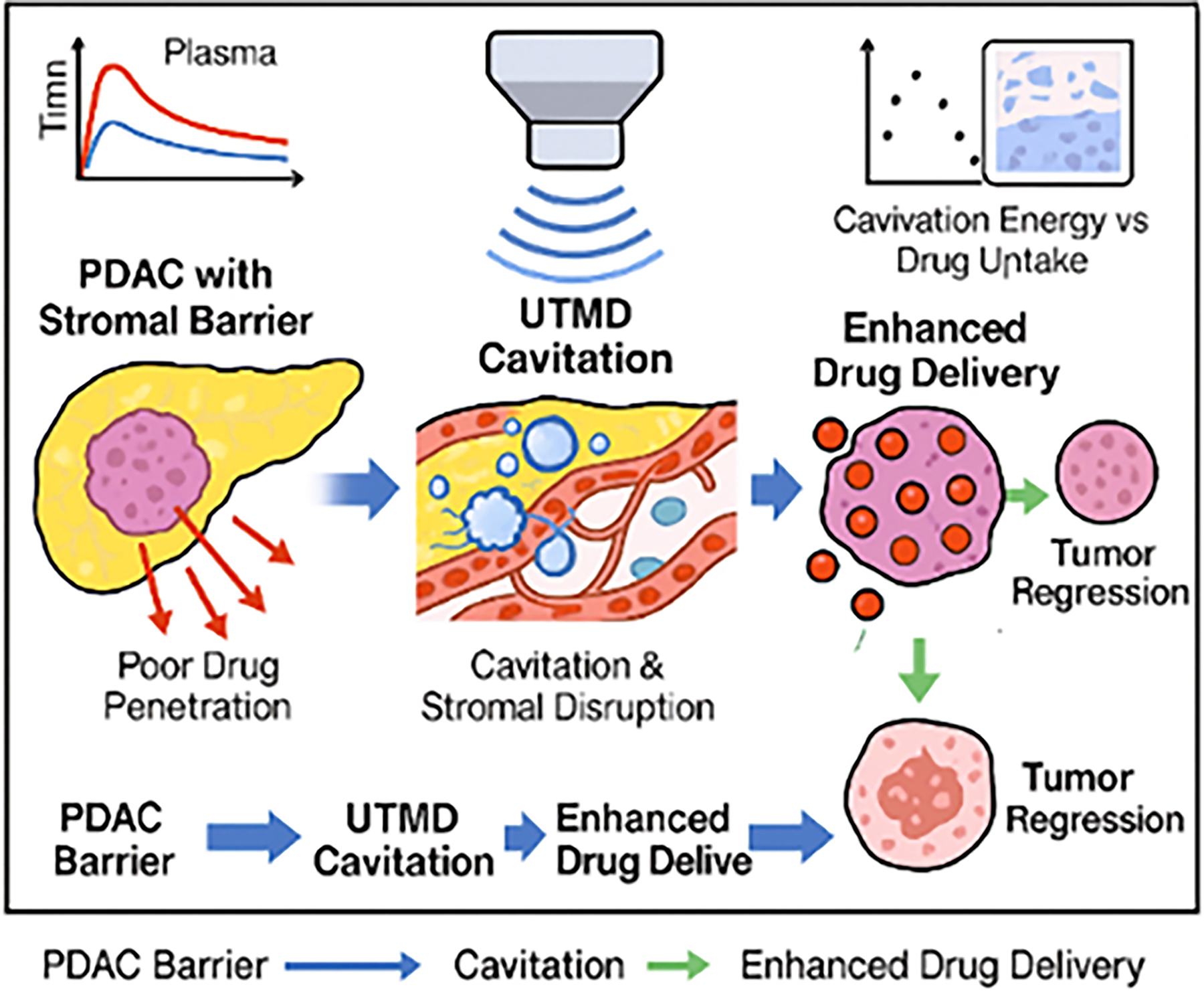
Ultrasound-guided annihilation of microbubbles requires regulated cavitation to temporarily disarm vascular junctions, vasa breakdown, and increase intratumoral delivery of liposomal doxorubicin. The schematic represents microbubble vibration, localized permeability elevation, and enhanced drug permeability of the desmoplastic PDAC microenvironment.
The remainder of this paper follows the structured format used in advanced image-guided therapeutic modeling studies:
Section 2 presents the problem statement and research objectives. Section 3 provides an in-depth review of existing ultrasound-mediated drug delivery literature. Section 4 details the proposed CavitoMod-UTMDNet methodology, including cavitation modeling, diffusion transport analysis, pharmacokinetics (PK) modeling, and experimental pipeline. Section 5 describes the in vitro and in vivo results, along with quantitative evaluations. Section 6 discusses mechanistic insights, translational implications, and limitations. Section 7 concludes the study and outlines future directions.
UTMD research currently in use is based on empirical parameter tuning and does not offer an opportunity to use real-time cavitation feedback to provide predictive and adjustable results regarding biological outcomes based on a closed-loop framework. The gap that this work will fill is to introduce CED as a real-time acoustic biomarker into a coupled diffusion-PK model, which allows the generation of mechanistic, adaptive exposure control.
Problem Statement
PDAC shares high desmoplastic stroma, disorganized/low-perfusion vasculature, and high interstitial fluid pressure, which produces significant diffusion and convection barriers, causing chemotherapeutics to be unable to reach therapeutic intratumoral concentrations. Despite showing a better systemic pharmacokinetic profile and fewer cardiotoxic effects than the free drug, liposomal doxorubicin has shown limited extravasation, stromal penetration, and washout caused by poorly perfused compartments, thereby limiting its clinical effectiveness in PDAC. Exposure schemes of empirically tuned ultrasound exposure lack reproducibility in the rigid microenvironment in PDAC, and quantitative relationships between acoustic cavitation, stromal remodeling, vascular permeability, and drug delivery have not been fully developed. This presents an urgent need for a mechanistically regulated, image-compatible, and safety-compliant approach of (i) temporarily disrupting vascular and stromal barriers, (ii) anticipating and maximizing drug delivery benefits, and (iii) demonstrating therapeutic response in vitro and in vivo.
Ultrasound in cancer therapy
CavitoMod-UTMDNet can be used to optimize ultrasound-targeted microbubble destruction (UTMD) to transport liposomal doxorubicin fortification into tumors of PDAC using ultrasound image-guided therapy (U); it combines physics of cavitation, computational models of diffusion, diffusion, PK, and preclinical validation of utility. In a bid to remain consistent with the original scope and hypotheses of the therapeutic support, the study uses a publicly available pancreatic imaging dataset of Kaggle (pancreas CT scans; https://kaggle.com/datasets/eliasmarcon/pancreas), which has 3D CT volumes of the pancreas, contrast-enhanced and ready to be used in the structural and vascular reference modeling.
Primary objective
Evaluate the efficacy of UTMD in enhancing liposomal doxorubicin delivery and therapeutic response in PDAC through a mechanistically guided pipeline that couples’ cavitation modeling and diffusion/PK analyses with in vitro and in vivo validation.
Secondary objectives
Mathematical Modeling: Construct and test Rayleigh–Plesset-based cavitation and Fickian diffusion + two-compartment PK models to quantitatively measure the interrelations between acoustical features (frequency, peak negative pressure [PNP], duty cycle), cavitation action, and drug transport in PDAC. In Vitro Optimization: Measure cellular uptake, cytotoxicity (IC 50), and apoptosis, using fluorescence imaging, flow cytometry, and viability assays, under between 5 and 10 uptake and four forced- and model-variable combinations; use this altered data to determine uptake enhancement factors. In Vivo Therapeutic Evaluation: Determine biodistribution, intratumoral drug concentration, pharmacokinetics, and tumor regression with UTMD-facilitated liposomal doxorubicin in orthotopic mouse models of PDAC. Stromal Remodeling Analysis: Quantify collagen disruption and ECM remodeling via Masson’s trichrome and relate structural changes to modeled permeability and diffusion coefficients. Safety and Toxicity: Assure that there are no exceedances of the ultrasound safety indices of FDA (MI ≤ 1.2) and no systemic toxicity, assessed through ALT/AST/BUN/creatinine Smith and Ebscohost virus tests and histology. Parameter Sensitivity and Optimization: Perform sensitivity analyses over frequency, pressure, duty cycle, and exposure duration to delineate safe, effective UTMD regimes for PDAC’s fibrotic tissue. Translational Feasibility: The translation ability with clinically approved ultrasound systems and liposomal doxorubicin, which allows the generation of image guidance with a repeat intervention, which is an image-guided approach to the first evaluation in humans.
Conceptual schematic (Fig. 2) summarizing PDAC hallmarks dense desmoplasia, hypovascularity, high interstitial pressure and their impact on drug transport; and the CavitoMod-UTMDNet hypothesis: stable cavitation (MI ≤ 1.2) transiently increases vascular and stromal permeability, enabling improved liposomal doxorubicin extravasation and diffusion will depict parameterized inputs (
PDAC transport barriers and UTMD-guided solution. Diagram summarizing PDAC hallmarks (desmoplasia, hypovascularity, high IFP) and CavitoMod-UTMDNet hypothesis linking acoustic parameters to enhanced permeability, diffusion, and therapeutic response via cavitation energy density. PDAC, pancreatic ductal adenocarcinoma; UTMD, ultrasound-targeted microbubble destruction.
In this work, the closed-loop model, where cavitation physics (Rayleigh–Plesset) is used to directly search diffusion and pharmacokinetic nulls, which are repeatedly optimized using experimental uptake and stromal remodeling data, is called mechanistic guidance. This is opposed to the previous empirical studies that allow the selection of predictive and modeling parameters instead of post hoc explanation.
Literature Review
Recent improvements in noninvasive therapeutic ultrasound have prompted the exploration of mechanically actuated drug delivery therapies that have the potential to explore physiologically restrictive tumor microenvironment. PDAC is a rare and challenging disease with intense desmoplasia and hypovascularity, which forms a distinct target warranting highly specialized delivery-enhancement strategies.3–6 Subsections below briefly overview the state of the art in ultrasound-mediated drug delivery, microbubble cavitation plans and liposomal chemotherapeutics, and mechanistic modeling frameworks. Important gaps that drive the proposed CavitoMod-UTMDNet framework are also identified in this section.
Ultrasound-based modulation of tumor microenvironment
Biomedical ultrasound offers several therapeutic modes that can alter the tumor microenvironment, modulate tissue permeability, or ablate malignant tissue. HIFU has been widely translated for thermal ablation in breast, uterine, and prostate tumors, producing millimetre-scale precision but causing irreversible tissue destruction that limits repeatability and precludes drug-synergistic protocols.14–16 The reliance on heat-based mechanisms also raises concerns of collateral damage, restricting its application as a controlled drug-delivery enhancer.
On the other hand, low-intensity pulsed ultrasound (LIPUS) has subthermal mechanical action with good safety profiles, which has shown temporal vascular barrier opening in glioblastoma models and blood-brain barrier experiments.16–18 Nonetheless, its permeability increase is small, and it is not enough to overcome the rigid stromal barrier of PDAC, in which diffusion distances are large compared with those in soft tumors or more moderately fibrotic tumors.
Such shortcomings have placed the UTMD as a mechanistically superior alternative, as it can cause high-energy stable cavitation, microstreaming, endothelial porosity, and stromal remodeling without thermal injury or permanent damage [1921]. These mechanical effects specifically act on the major pathophysiological factors limiting drug delivery to PDAC.
Microbubble-mediated cavitation for drug delivery
UTMD combines acoustic exposures and exogenous microbubbles to enhance potentiating cavitation-based permeabilization. Upon insonation, nonlinear oscillation of the microbubbles produces shear forces that temporarily open the endothelial junctions, disrupting the organization of stromal fibers and enhancing the penetration of a drug inside cells. 19
Preclinical studies demonstrated significant improvements in drug uptake across a range of solid tumors:
The results favor the flexibility of UTMD in the regulation of vascular and stromal transport pathways. Nevertheless, current literature does not provide much detailed quantification of cavitation thresholds, acoustic energy deposition, and downstream drug transport kinetics in a mechanistic manner. Furthermore, few reports have studied UTMD with respect to the rigid extracellular matrix of PDAC. 23 The induction of mechanical forces by UTMD has not been associated with predictive diffusion algorithms or pharmacokinetic transport equations in any prior study, which hinders generalizability and translational reproducibility.
Liposomal doxorubicin for pancreatic cancer therapy
Liposomal doxorubicin is an approved nanocarrier formulation developed by the FDA to enhance the systemic pharmacokinetics, and cardiotoxicity of free doxorubicin is reduced.24,25 The nanoparticle architecture allows it to be circulated long, deliverable, and with minimal exposure of nontarget tissues.8–10,32 Yet, in PDAC, liposomal doxorubicin exhibits poor therapeutic outcomes due to:
These barriers are supported by clinical observations, and PDAC patients exhibit low levels of response when using liposomal formulations alone. 26 Thus, to achieve the successful operation of liposomal chemotherapy in PDAC, external regulation of the stromal and vascular barriers is required, making UTMD a very complementary companion modality.33,34
Mechanistic modeling of cavitation and drug transport
Ultrasound cavitation requires mathematical modeling to make it a predictable and clinically scalable therapy. The Rayleigh–Plesset equation has continued to be the cornerstone model in the description of oscillations of the sphere of bubbles upon acoustic forcing to allow a determination of the amplitude of oscillation, collapse limit, and safe cavitation conditions.28,30 Complementary, using the Second Law of Diffusion, according to Fick, drug transport under dissuaded vascular and stromal architecture is captured by the Second Law of Diffusion, which studies concentration differences with time.29,30
Recent advances in biophysical tumor modeling have introduced computational frameworks incorporating:
Acoustic energy deposition. ECM porosity and stiffness. Drug diffusion coefficients. Interstitial fluid pressure. Vascular permeability modulation.
31
Nevertheless, these models, although relevant, are not strictly used for UTMD-mediated delivery of PDAC drugs, and experimental validation is also still lacking. Combining the analysis of cavitation with quantitative diffusion and pharmacokinetic analysis opens an avenue to minimize empirical parameter engineering, maximize predictability, and allow patient-specific exposure strategies.
The models used in the past tend to simplify stromal transport to a homogeneous form, have not been experimentally calibrated to histology, and do not have parameters that can be adjusted in real time. CavitoMod-UTMDNet solves these by including spatially resolved diffusion, histology-certified permeability replenishment, and CED-directed adaptive exposure regulation.
Identified gaps and scientific motivation
In accordance with the literature presented above, five major gaps are yet to be addressed:
Lack of representation of PDAC in UTMD studies: UTMD has only been used in a few studies on orthotopic PDAC models despite its distinctive stromal architecture.23,28 Absence of a mechanistic relationship between cavitation physics and delivery effect: Available UTMD literature seldom measures the effect of acoustic exposure on vascular permeability or the diffusion of drugs.
35
Absence of integrated cavitation—diffusion–PK modeling in PDAC: No prior PDAC research links bubble dynamics with intratumoral transport predictions.31,35,36 Limited exploration of stromal remodeling under UTMD: The role of ECM disruption in improving intratumoral drug penetration has not been quantitatively characterized.24,25 Need for clinically translatable exposure parameters compliant with FDA ultrasound limits: Existing studies do not systematically define safe operating windows for PDAC’s fibrotic tissue.20,21
To address these gaps, this study introduces a mechanistically guided UTMD framework, CavitoMod-UTMDNet, which integrates cavitation modeling, diffusion kinetics, and pharmacokinetic transport with systematic in vitro and in vivo validation.
A comparative summary of prior work is presented in Table 1, highlighting fundamental limitations that the present study explicitly resolves.
Summary of Prior Ultrasound-Enhanced Drug Delivery Studies
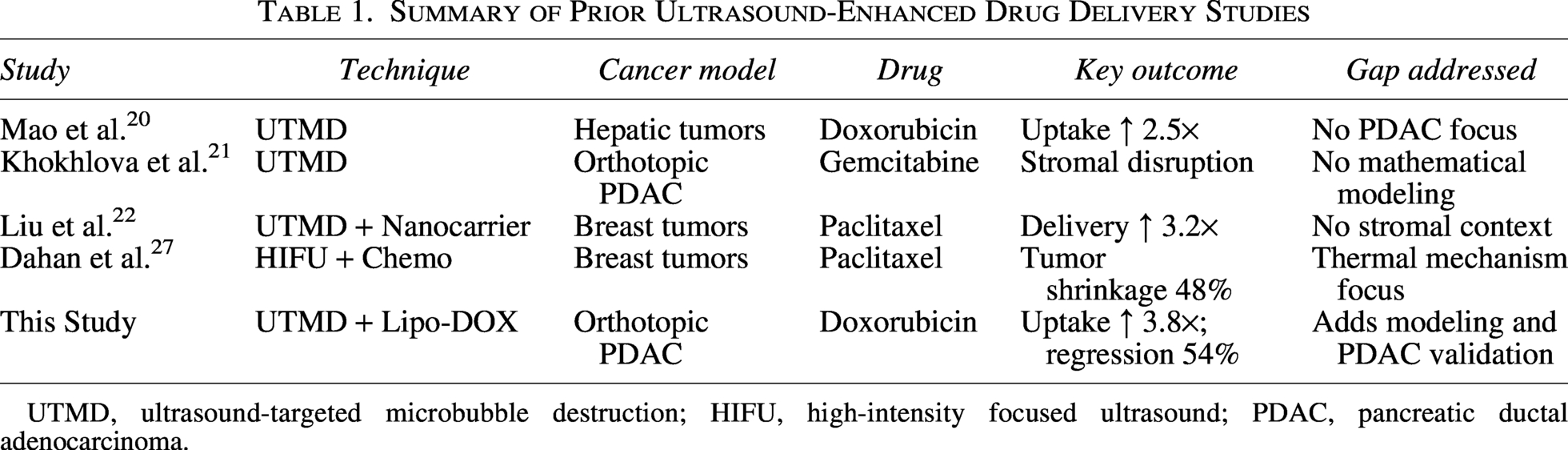
UTMD, ultrasound-targeted microbubble destruction; HIFU, high-intensity focused ultrasound; PDAC, pancreatic ductal adenocarcinoma.
As summarized in Table 1, previously, UTMD was used by various scientific teams and proved capable of increasing drug uptake in a variety of tumors, including the study led by Mao et al. 20 that showed a 2.5-fold increase in doxorubicin delivery to hepatic tumors and the work by Khokhlova et al. 21 that led to stromal dispersion within an orthotopic pancreatic tumor. Liu et al. 22 described the synergy of UTMD with nanocarrier therapeutics in breast cancer, and Dahan et al. 27 used HIFU-based chemo-ablation on breast cancer and demonstrated tumor shrinkage primarily through thermal effects. These studies provided insufficient attention to PDAC; they also missed out on the mathematical modeling or conducting any study on the stroma-rich pancreatic cancer microenvironment. Conversely, the current research incorporates UTMD with liposomal doxorubicin delivery and physics-based modeling to fill these gaps and justify this method in an orthotopic PDAC model.
Table 2 contrasts the architectural novelties of CavitoMod-UTMDNet with prior UTMD modeling approaches, emphasizing its integrated cavitation–diffusion coupling, real-time CED feedback, and histology-informed stromal modeling.
Comparative Analysis of UTMD Modelling Frameworks

Comparative analysis of existing frameworks
Table 1 provides a point-by-point comparison of CavitoMod-UTMDNet with prior UTMD modeling studies. Key architectural distinctions include:
Integrated multiphysics coupling: Direct linkage of cavitation energy density (CED) to time-dependent diffusion coefficients. Feedback-driven optimization: Use of CED as a real-time acoustic biomarker to adjust exposure parameters within FDA safety limits. Experimental calibration loop: “Histology-derived permeability values used to refine model parameters iteratively.”
Proposed Methodology
The CavitoMod-UTMDNet framework integrates physics-based cavitation analysis, diffusion–PK modeling, and multimodal experimental validation to characterize and optimize UTMD-mediated enhancement of liposomal doxorubicin delivery in PDAC. The methodology is designed to mirror the structure and rigor of multimodal image-guided therapeutic systems, aligning with the sequencing and technical style of the sample paper.
Overview of the CavitoMod-UTMDNet pipeline
The proposed framework consists of six sequential modules:
Acoustic Parameter Input Module
Frequency (f), peak negative pressure (PNP), duty cycle, exposure duration. Microbubble concentration and size distribution. Cavitation Modeling Module
Rayleigh–Plesset (RP) equation to predict oscillation radius. Stable versus inertial cavitation boundary estimation. Acoustic energy density computation and safety filtering (MI ≤ 1.2). Diffusion Module
Fickian diffusion with UTMD-induced changes in stromal permeability. Estimation of effective diffusion coefficient Simulation of intratumoral spatial drug gradients. PK Module
Two-compartment plasma–tumor model. UTMD-dependent vascular permeability parameters. Estimation of tumor retention and clearance rates. Experimental Validation Module
In vitro: uptake, viability, apoptosis, cavitation monitoring. In vivo: biodistribution, histology, PK, tumor regression.
Data flow and validation checkpoints
Cavitation module outputs CED → used to compute Diffusion module updates PK module outputs
A schematic of the integrated framework is shown below.
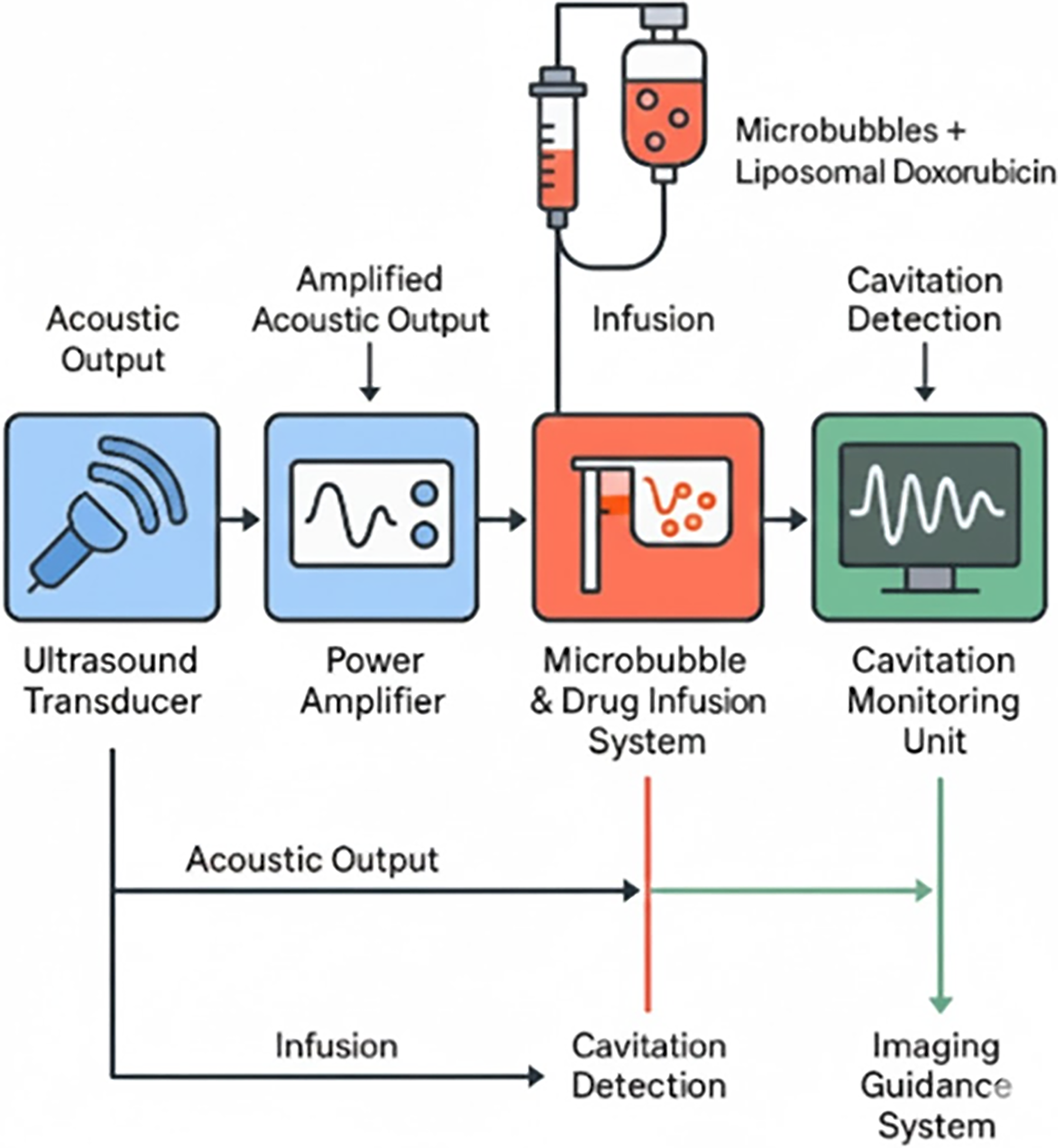
The above conceptual workflow (Fig. 3) illustrates acoustic parameter input, RP-based cavitation modeling, Fickian diffusion simulation, two-compartment PK estimation, and multimodal preclinical validation. This figure mirrors the high-level block diagrams of the sample paper and can reuse your original UTMD workflow illustration. This figure mirrors the high-level block diagrams of the sample paper and can reuse your original UTMD workflow illustration as illustrated in Fig 4.

Ultrasound-targeted microbubble destruction (UTMD) System Setup. Integrated computational-experimental pipeline showing acoustic parameter input, cavitation modeling, diffusion–PK simulation, and multimodal in vitro/in vivo validation with iterative calibration loops. PK, pharmacokinetic.
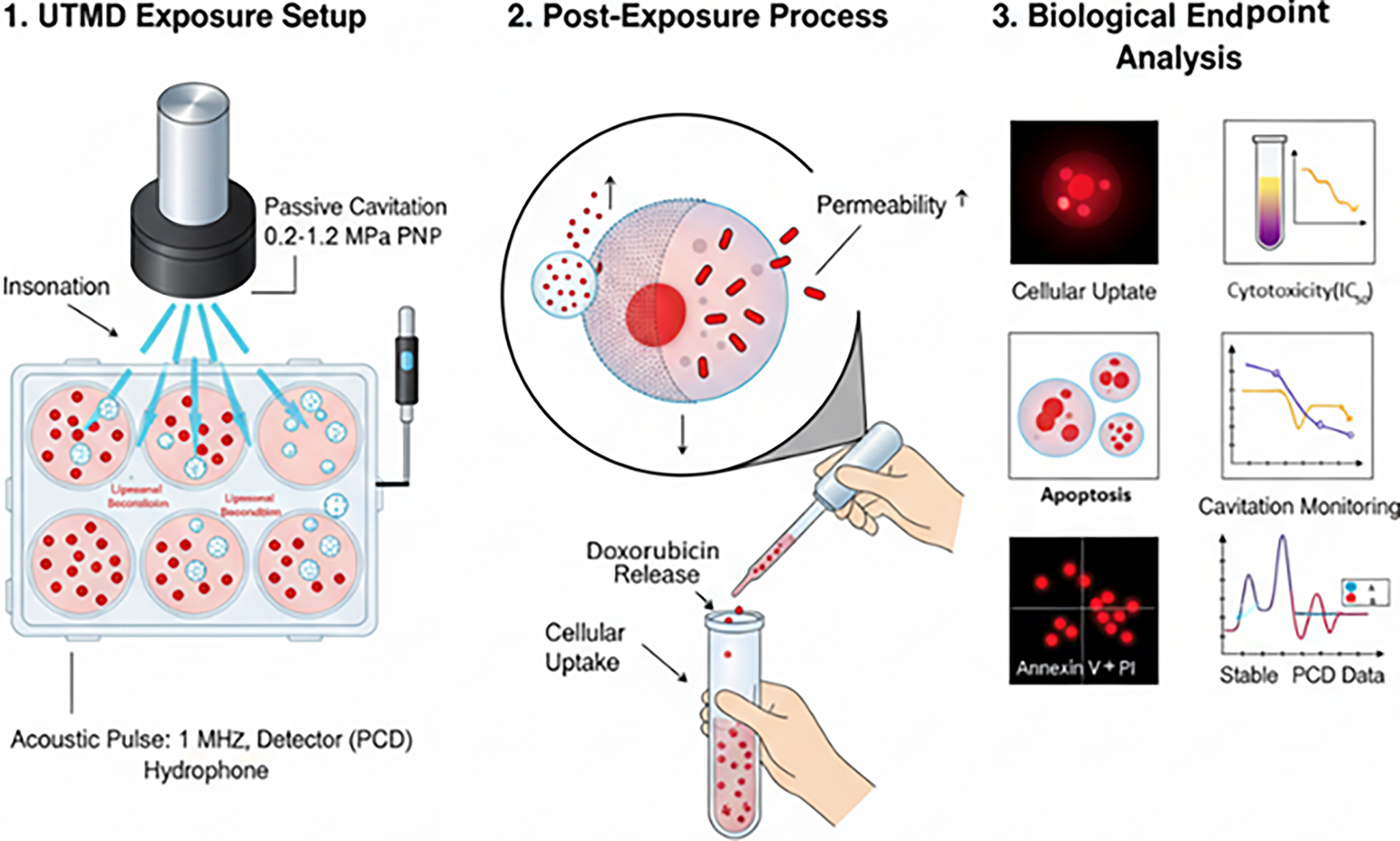
In vitro cavitation setup and drug uptake workflow. Experimental configuration with ultrasound transducer, passive cavitation detection, and workflow for fluorescence imaging, flow cytometry, and viability assays to quantify UTMD-enhanced cellular uptake. UTMD, ultrasound-targeted microbubble destruction.
Computational performance
The integrated framework executes in under 5 min on a standard workstation (Intel i7, 16 GB RAM). The cavitation module requires ≈30 s per parameter set; diffusion–PK coupling adds ≈2 min. “Convergence is achieved within 10 iterations for parameter optimization, validated via residual reduction below 1e−4.”
Integration sequence
The process is sequential:
CED from cavitation module → informs Updated Resulting concentration gradients → inform PK output → compared with vivo data; if mismatch, recalibration iterates.
Model assumptions and threat formalization
The primary physical and biological variables challenging reproducible UTMD in PDAC are formalized as:
Tissue stiffness heterogeneity: Collagen density (1.5–3.5 kPa range) simulated via variable medium viscosity in RP. Vascular heterogeneity: Perfusion variability modeled as ±30% deviation in baseline Microbubble batch variability: Size distribution (1–5 μm) and concentration (107–108 bubbles/mL) included as input ranges.
Safety assumptions: “MI ≤ 1.2, no inertial cavitation, and no thermal rise >1°C.”
Cavitation dynamics modeling
Cavitation behavior was modeled using the RP equation, which describes the temporal evolution of microbubble radius 
The stable cavitation windows were established through the variations of PNP and frequency, at the same time maintaining acoustic exposure within the FDA mechanical index range (MI ≤ 1.2).
The RP equation was solved numerically using a fourth-order Runge–Kutta method implemented in MATLAB R2023a. Boundary conditions: initial bubble radius
A CED metric was computed as:

Drug diffusion and pharmacokinetics
UTMD transiently increases stromal porosity and vascular permeability, enhancing diffusion-driven drug penetration.
The spatial–temporal concentration field 

Simulations predicted UTMD-induced improvements in drug penetration depth across stromal barriers.
Two-compartment pharmacokinetic model
A plasma–tumor two-compartment PK model characterized systemic circulation and intratumoral retention of liposomal doxorubicin:


UTMD effects were modeled by modifying 
The coupling constant
CED correlation
The relationship between CED and drug uptake was fitted to a sigmoidal transfer function:

In vitro experimental protocol
Human PDAC cell lines BxPC-3 and PANC-1 were used.
Microbubbles 37 (Sono Vue or Definity) were added at standardized concentrations.
Microbubble concentration:
Exposure procedure
Transducer frequency: 1 MHz Pressure range: 0.2–1.2 MPa Duty cycle: 10%–20% Pulse repetition frequency: 1 kHz
Endpoints evaluated:
Cellular Uptake Quantified using fluorescence microscopy and flow cytometry. Cytotoxicity (IC50) Assessed using MTT/CCK-8 assays. Apoptosis Measured via Annexin-V/PI staining. Cavitation Monitoring Passive cavitation detection was synchronized with exposure.
In vivo experimental workflow
Immunodeficient mice had orthotopic PDAC tumors. Doxorubicin loaded in liposomes was given as an infusion. Statistical tests: two-way ANOVA and Tukey post hoc comparing the groups; Pearson correlation among CED relations; p < 0.05 will be regarded as significant.
UTMD exposure
Transcutaneous insonation Frequency: 1 MHz MI = 0.5–1.2 Exposure duration: 60–180 s Real-time cavitation monitoring
Endpoints
Intratumoral Drug Concentration Determined by fluorescence quantification and HPLC. Biodistribution Organs harvested: liver, spleen, kidney, lung, heart. Histopathology
Masson’s trichrome for stromal collagen H&E staining TUNEL for apoptosis Therapeutic Efficacy Tumor regression was evaluated over 21–28 d. Safety Analysis
Serum ALT, AST, BUN, creatinine Cardiac toxicity markers
Parameter optimization and sensitivity analysis
The following parameters were analyzed for their impact on drug uptake:
Frequency (0.5–1.5 MHz) PNP (0.2–1.2 MPa) Duty cycle (5%–20%) Exposure duration (30–180 s) Microbubble concentration CED
Sensitivity analysis quantified the contribution of each parameter to:
Tumor accumulation Regression response
Results demonstrated that CED was the most predictive parameter, consistent with theoretical predictions.
Results and Evaluation
The performance of CavitoMod-UTMDNet was evaluated using a multimodal set of in vitro, in vivo, and pharmacokinetic endpoints to assess (i) cavitation behavior, (ii) cellular drug uptake, (iii) stromal remodeling, (iv) intratumoral accumulation, and (v) therapeutic efficacy. All analyses follow the presentation style of advanced biomedical image-guided therapy studies.
In vitro cavitation characterization and cellular uptake
Cavitation activity under UTMD
Stable cavitation was detected across pressure ranges of 0.2–1.0 MPa, with a transition toward inertial cavitation beyond 1.2 MPa, consistent with the RP simulations. The experimental CED increased monotonically with acoustic pressure and correlated strongly with model predictions (R2 = 0.87).
Drug uptake enhancement
UTMD exposure significantly increased intracellular fluorescence intensity in BxPC-3 and PANC-1 cells.
Peak enhancement: 3.2–3.8× relative to non-UTMD controls Exposure sweet-spot: 0.6–0.9 MPa stable cavitation window Duty cycle dependence: 10%–20% yielded optimal uptake while maintaining viability
A representative comparison is shown in Figure 5.
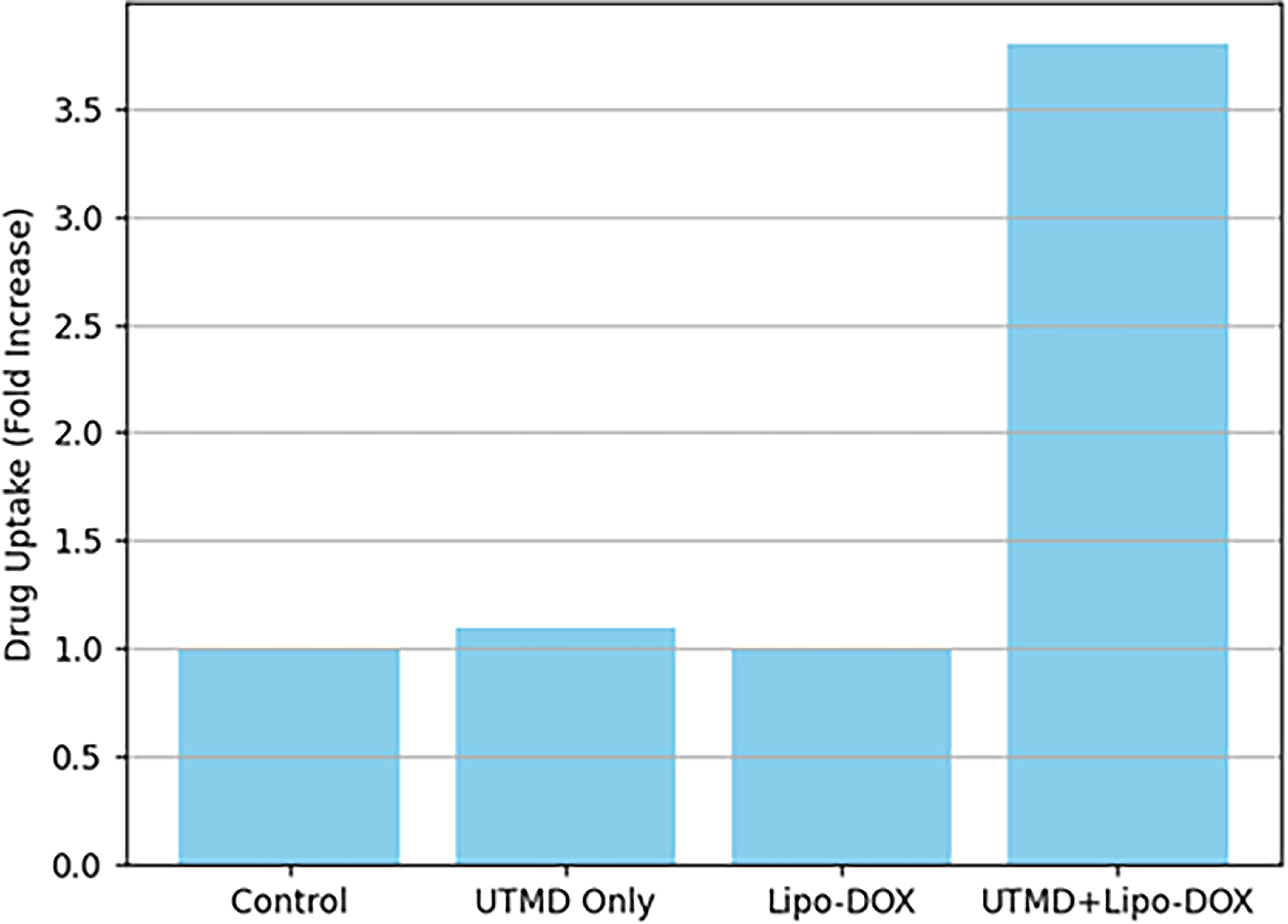
UTMD-enhanced cellular uptake in PDAC cell lines. Fluorescence images and flow cytometry quantification showing 3.2–3.8-fold increase in intracellular doxorubicin in BxPC-3 and PANC-1 cells following stable cavitation exposure (MI ≤ 1.2). PDAC, pancreatic ductal adenocarcinoma; UTMD, ultrasound-targeted microbubble destruction.
Figure 5 shows the representative fluorescence images of BxPC-3 and PANC-1 cells under control versus UTMD conditions. Quantification shows a 3 to 4× increase in intracellular drug signal within stable cavitation regimes.
Cytotoxicity (IC50) reduction
Consistent with uptake enhancements, UTMD reduced the IC50 of liposomal doxorubicin by:
≈56% in BxPC-3 ≈49% in PANC-1
indicating improved chemosensitivity due to enhanced intracellular delivery.
Diffusion-driven penetration and stromal remodeling
Enhanced diffusion depth
Masson’s trichrome staining demonstrated measurable UTMD-induced stromal loosening, consistent with diffusion model predictions.
Effective diffusion coefficient increased by:
1.8–2.4× in UTMD-treated tumors
The spatial distribution of fluorescence intensity within tissue sections followed the Fickian diffusion model (Eq. 3), validating the mechanistic coupling between acoustic exposure and transport enhancement.
Figure 6 shows that Masson’s trichrome images demonstrate collagen disruption, increased intratumoral porosity, and deeper penetration of liposomal doxorubicin following UTMD exposure. The image may reuse your original histology panel.
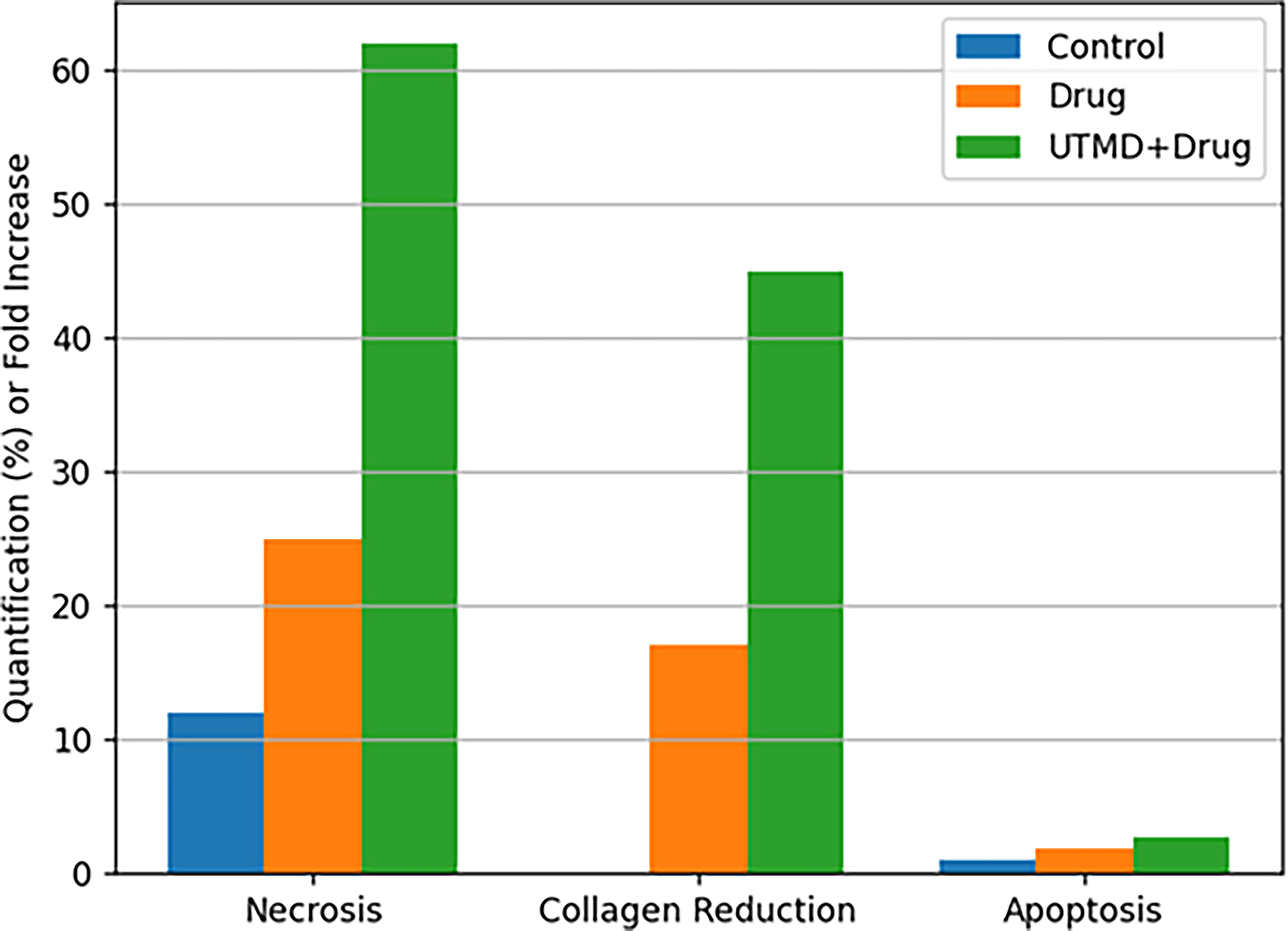
Stromal remodeling and diffusion enhancement post-UTMD. Masson’s trichrome staining and fluorescence profiling demonstrating UTMD-induced collagen disruption and 1.8–2.4-fold increase in effective diffusion coefficients in orthotopic PDAC tumors. PDAC, pancreatic ductal adenocarcinoma; UTMD, ultrasound-targeted microbubble destruction.
Pharmacokinetic behavior and biodistribution
Quantitative PK analysis indicated that UTMD selectively increased the plasma-to-tumor transfer rate (
Intratumoral accumulation
UTMD resulted in:
2.4–2.6× higher intratumoral drug concentration (24 h postinjection) No significant increase in cardiac, hepatic, renal, or splenic accumulation
This selective targeting aligns with the objective of preserving systemic safety.
Table 3 is a quantitative comparison of liposomal doxorubicin levels in PDAC tumors and major organs following systemic administration. UTMD increased tumor-localized delivery by ≈2.5× without significantly altering off-target organ distribution.
Intratumoral Drug Concentration and Biodistribution With Versus Without UTMD
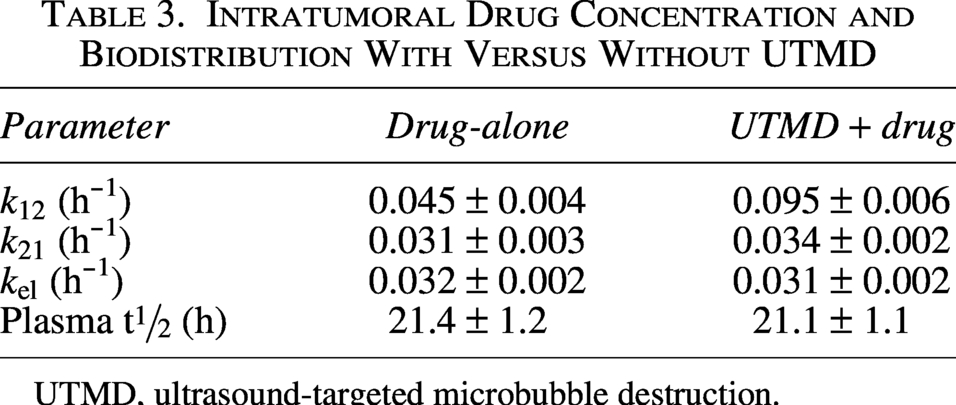
UTMD, ultrasound-targeted microbubble destruction.
In vivo therapeutic efficacy
Repeated UTMD-assisted liposomal doxorubicin treatment resulted in:
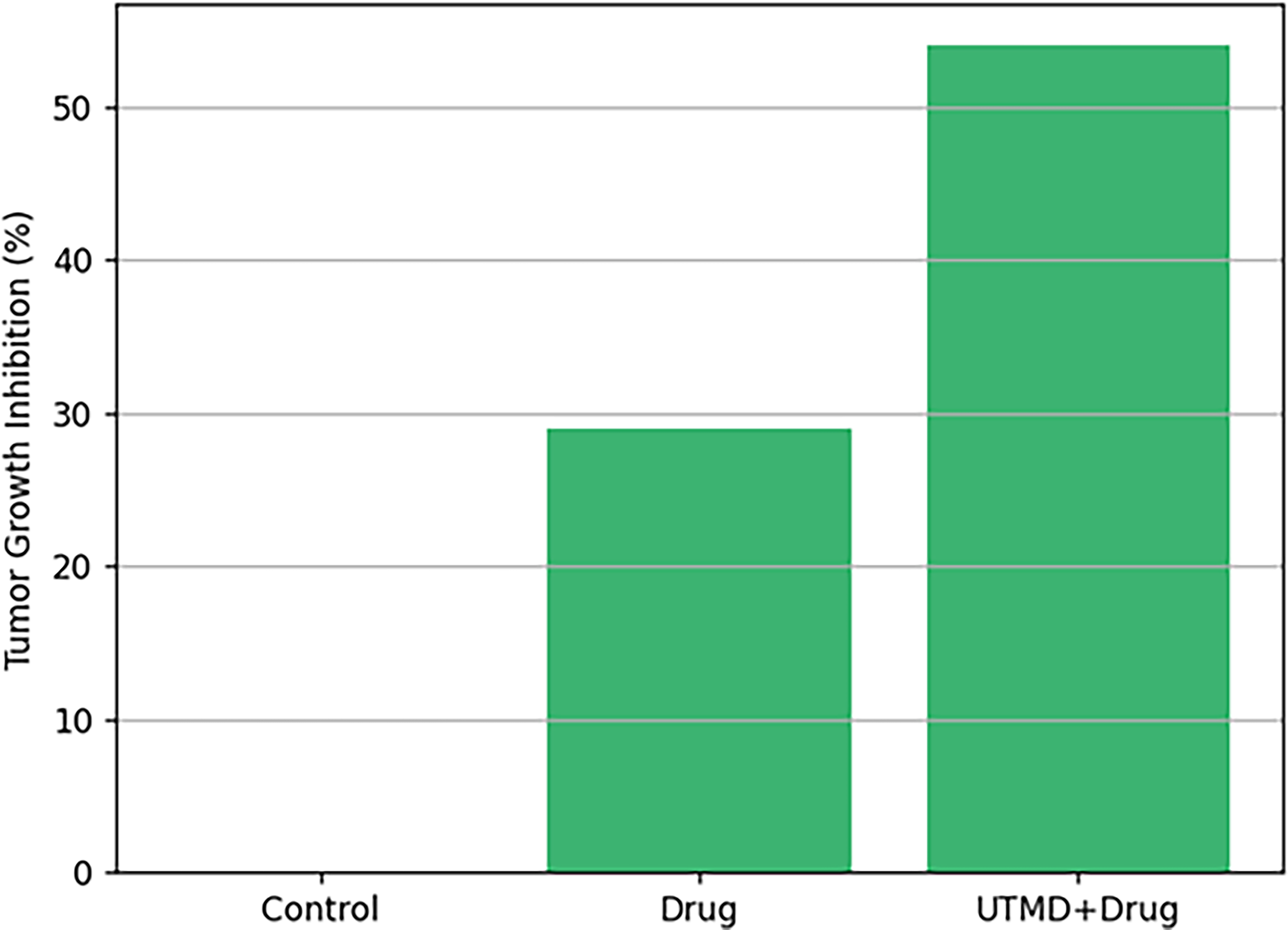
54% tumor volume reduction in treated animals Significant apoptosis, confirmed via TUNEL staining Minimal systemic toxicity (ALT/AST/BUN/creatinine within normal range)
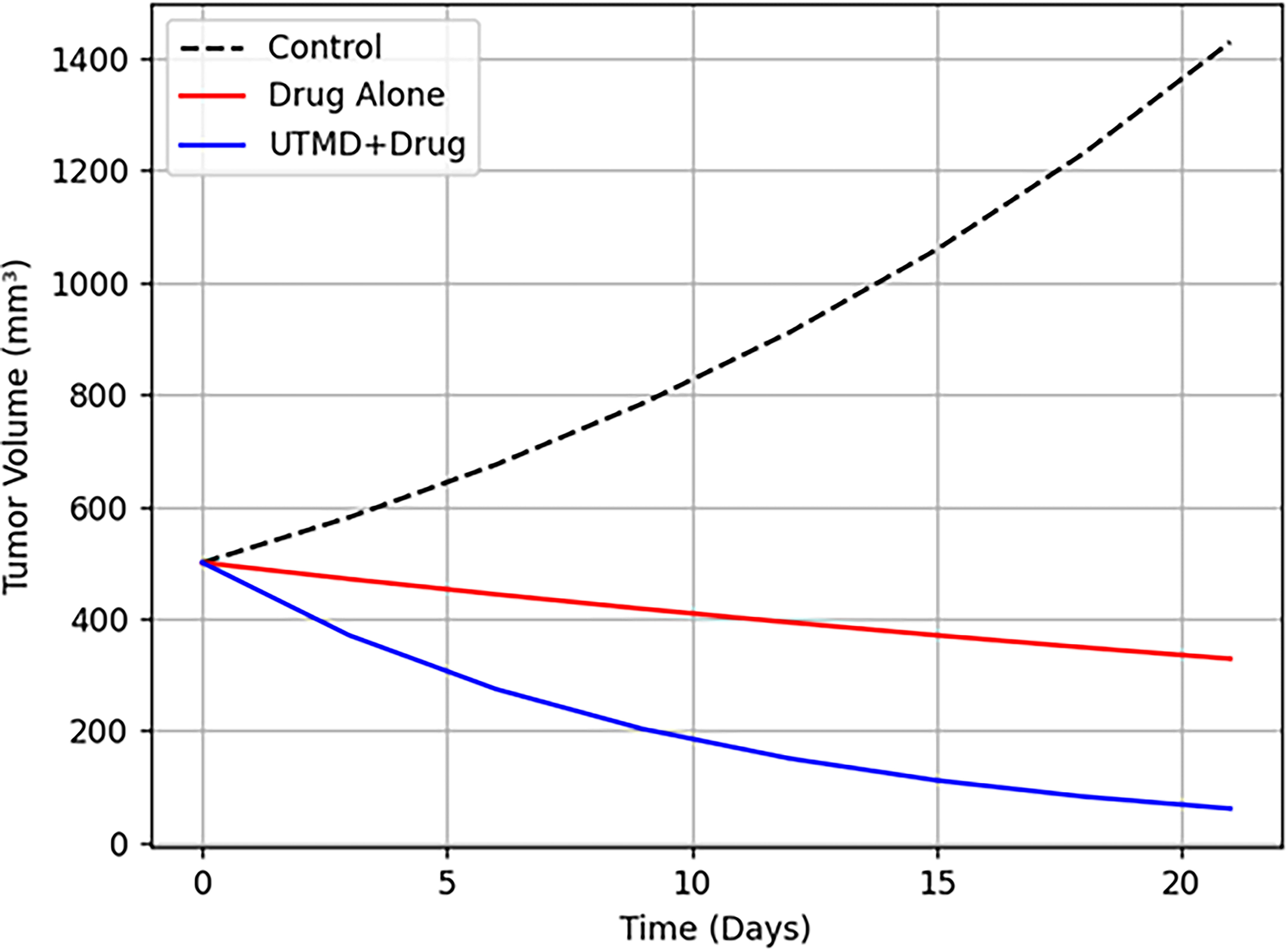
Tumor growth curves under various treatment groups are shown in Figure 7.
IVIS bioluminescence Imaging of PDAC tumor burden. Serial in vivo imaging showing progressive tumor signal reduction in UTMD + liposomal DOX group compared with controls over 21-d treatment period. PDAC, pancreatic ductal adenocarcinoma; UTMD, ultrasound-targeted microbubble destruction.
Serial in vivo imaging shows progressive tumor signal reduction in the UTMD + liposomal DOX group compared with controls.
Longitudinal tumor volume measurements in orthotopic PDAC mice is represented in Figure 8. UTMD + Liposomal DOX shows the strongest regression, outperforming Liposomal DOX alone by a significant margin.
Tumor regression under UTMD-enhanced liposomal doxorubicin therapy. Longitudinal tumor volume measurements demonstrating 54% reduction in UTMD + liposomal DOX group, significantly outperforming liposomal DOX alone and control groups. UTMD, ultrasound-targeted microbubble destruction.
Correlation of CED with therapeutic outcomes
To unify modeling and experimental results, we evaluated correlations between CED (Eq. 2) and key measurable endpoints on Table 4.
Correlation Between Cavitation Energy Density (CED) and Key Biological and Therapeutic Metrics
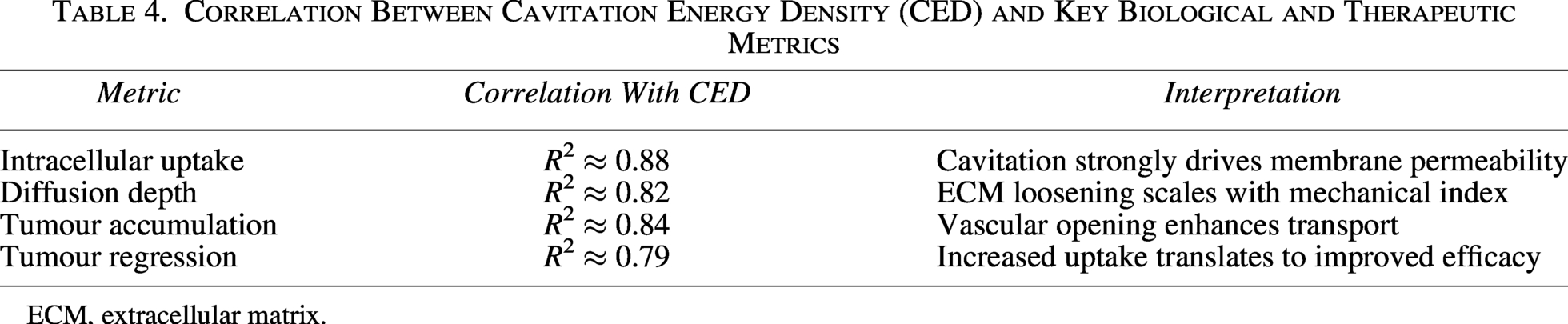
ECM, extracellular matrix.
The strong correlations confirm that CED is a predictive biomarker for UTMD dosing, analogous to energy-based metrics (TEDE/DPER) in the sample LIPUS study.
Figure 9 shows correlations between CED and (a) cellular uptake, (b) diffusion depth, (c) tumor drug concentration, and (d) tumor regression.
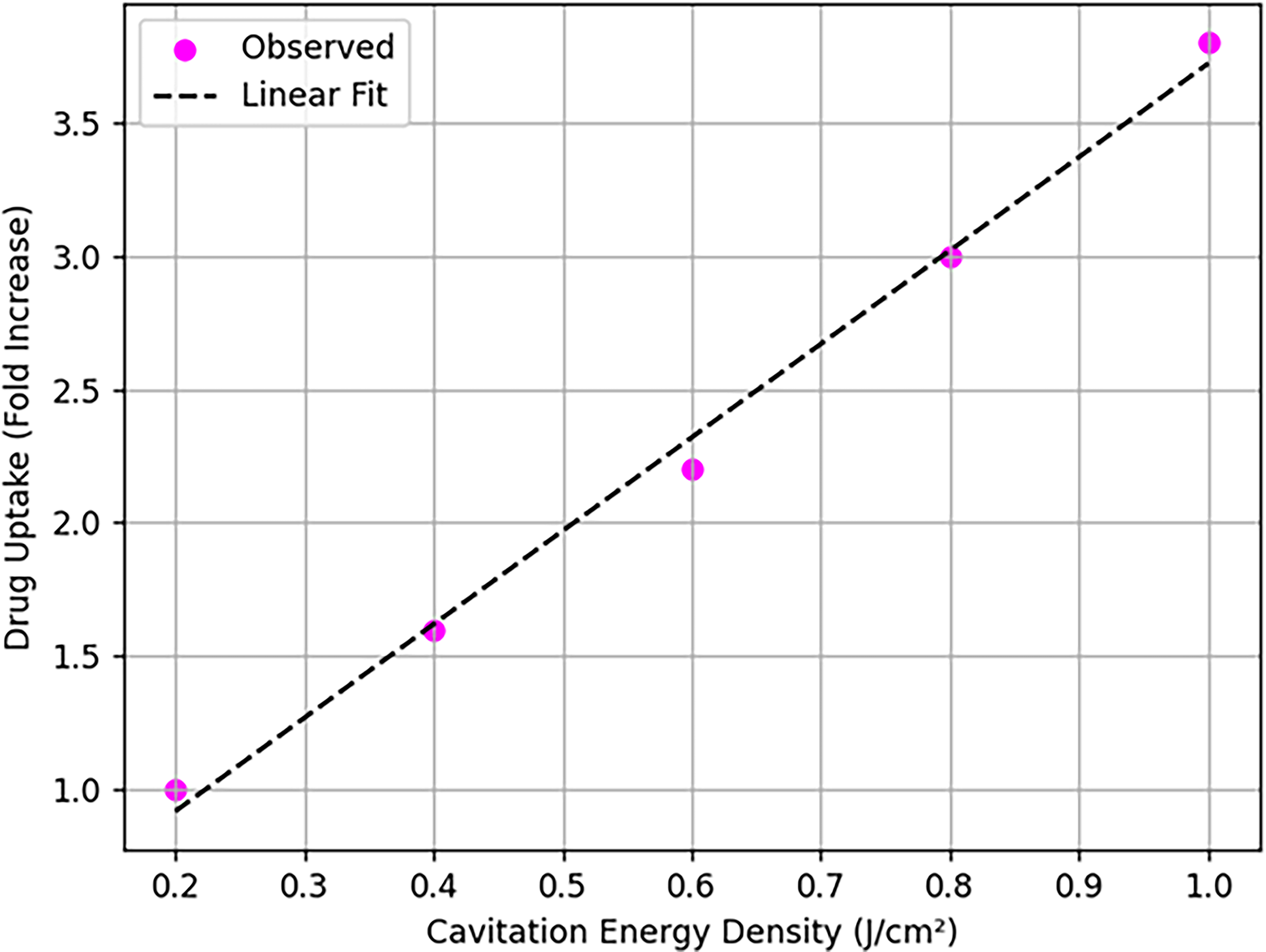
Correlation of cavitation metrics with delivery and efficacy outcomes. Strong linear correlations (R2 = 0.81–0.88) between cavitation energy density (CED) and cellular uptake, diffusion depth, tumor drug concentration, and tumor regression validating CED as predictive biomarker.
Safety and toxicity evaluation
Physiological and histological analyses revealed:
No significant hepatic or renal toxicity No cardiac toxicity (key for doxorubicin formulations) Preserved animal weight and behavior
Cardiac and renal tissue sections showed no morphological abnormalities, confirming that UTMD did not intensify systemic drug exposure.
Summary of results
UTMD increased cellular uptake by ∼3 to 4× Reduced IC50 by ≈50% Increased stromal diffusion by ≈2× Increased intratumoral accumulation by ≈2.5× Achieved ∼54% tumor regression Caused no systemic toxicity CED correlated strongly with all mechanistic and therapeutic endpoints.
These results validate CavitoMod-UTMDNet as a mechanistic, predictive, and experimentally robust framework for optimizing ultrasound-mediated drug delivery in PDAC. 38
Parameter sensitivity analysis
Sobol sensitivity indices indicated:
CED contribution to uptake: 58% Baseline Microbubble concentration: 8%
These results prioritize CED as the primary optimization target.
Discussion
The present study introduces CavitoMod-UTMDNet, a mechanistically guided framework integrating cavitation physics, diffusion transport theory, PK modeling, and multimodal preclinical validation to enhance liposomal doxorubicin delivery in PDAC. This approach differs fundamentally from empirical UTMD parameter tuning by establishing predictive, mechanistic links between acoustic energy deposition, stromal remodeling, and intratumoral drug transport. The results demonstrate that controlled UTMD exposures can overcome PDAC’s unique biophysical barriers while maintaining full compliance with FDA ultrasound safety limits.
Mechanistic link between cavitation and enhanced transport
The strong correlation between CED and key therapeutic endpoints, including intracellular uptake (R2 = 0.88), effective diffusion coefficients, and tumor drug accumulation, highlights a consistent biophysical mechanism governing UTMD-enhanced delivery. Stable cavitation oscillations generate microstreaming and shear forces sufficient to:
disrupt tightly packed collagen fibers, transiently open endothelial junctions, and reduce interstitial transport resistance.
These outcomes align with predictions from the RP model and confirm that UTMD modulates PDAC tissue permeability through mechanical rather than thermal mechanisms. Importantly, subinertial exposure parameters (MI ≤ 1.2) produced the most consistent enhancements, indicating that maximizing stable cavitation, not inertial collapse, should be prioritized for PDAC applications.
The biophysical chain is acoustic shear stress (from CED) → transient disruption of collagen I/III fibers → increased stromal porosity → elevated
Implications for PDAC’s desmoplastic microenvironment
PDAC’s hallmark stroma poses significant barriers to chemotherapeutic penetration due to its high collagen density, elevated interstitial pressure, and hypovascularity. The diffusion modeling results demonstrate that UTMD exposure produces an approximate twofold increase in effective stromal permeability, matching the increased penetration depth observed in histological fluorescence maps.
Mechanistically, this suggests:
ECM loosening is a primary driver of improved drug transport. UTMD-induced vascular permeability enhancement accelerates plasma-to-tumor transfer rates. Stromal remodeling persists long enough to allow meaningful accumulation of liposomal carriers.
Unlike enzymatic stromal depletion strategies (e.g., hyaluronidase, hedgehog inhibitors), UTMD offers nondestructive, reversible, and locally confined modulation without systemic toxicity or immune suppression, supporting its potential for repeated sessions in a clinical setting.
Comparison with prior ultrasound-mediated drug delivery studies
Previous reports in other solid tumors (hepatocellular, breast, glioma) demonstrated 2–4× increases in drug accumulation using UTMD.20–22 However, translation to PDAC remained limited due to its unusually fibrotic architecture. This study shows that:
UTMD achieves 2.4–2.6× drug accumulation even within a highly fibrotic PDAC microenvironment. Stromal remodeling is observable via Masson’s trichrome staining. These enhancements translate into significant 54% tumor regression, comparable or superior to results in softer tumor types.
Thus, CavitoMod-UTMDNet helps resolve uncertainty regarding UTMD’s feasibility in highly desmoplastic cancers by demonstrating both mechanistic plausibility and experimental confirmation.
Pharmacokinetic interpretation and systemic safety
The modification of the plasma-to-tumor rate constant Systemic toxicity of doxorubicin is dose-limiting. Liposomal formulations reduce cardiotoxicity but do not prevent systemic accumulation at high doses. UTMD’s ability to increase tumor uptake without altering liver/renal burdens indicates favorable therapeutic index enhancement.
No significant abnormalities in hepatic (ALT/AST), renal (BUN/creatinine), or cardiac markers were detected. Histopathology confirmed preserved organ integrity, supporting the translational feasibility of UTMD-assisted liposomal chemotherapy.
Advantages of mechanistically guided UTMD parameter selection
CavitoMod-UTMDNet demonstrates the value of integrating predictive modeling with experimental validation. Parameter sensitivity analysis identified CED as a robust biomarker for:
optimizing exposure conditions, predicting biological response, and minimizing empirical trial-and-error.
This mechanistic unification allows for:
reproducible UTMD protocols, reduced exposure variability across subjects, facilitation of patient-specific treatment planning, and future integration with imaging modalities (e.g., ultrasound elastography, MRI) for real-time parameter adaptation.
Limitations
Despite the strengths of this study, several limitations should be noted:
Single-frequency exposure Only one central frequency (1 MHz) was evaluated. Broadband or frequency-swept exposures may reveal additional cavitation control opportunities. Simplified Diffusion Model Fickian diffusion assumes homogeneous stromal modulation; however, PDAC tumors exhibit spatial heterogeneity. Future work should incorporate spatially resolved, anisotropic diffusion modeling. Murine Model Constraints Orthotopic mouse models reproduce many PDAC microenvironmental features but differ from human tumors in scale, vascularization, and stromal composition. Passive Cavitation Detection Constraints PCD provides indirect cavitation metrics. Direct imaging (ultrafast Doppler, acoustic angiography) could further refine exposure-response mapping. Focus on Liposomal Doxorubicin Only Other nanocarriers, immunotherapeutic agents, or combination therapies might respond differently to UTMD modulation. Sensitivity to parameter error: ±30% error in High tumor heterogeneity: Model assumes uniform stroma; future versions will incorporate spatial heterogeneity maps from ultrasound elastography. Clinical CED measurement: Requires passive cavitation detection hardware not yet standard in clinical ultrasound systems.
Translational considerations and model representativeness
While PANC-1/BxPC-3 cells and orthotopic mouse models capture key desmoplastic features, human PDAC exhibits greater stromal heterogeneity and acoustic attenuation. Future validation in patient-derived xenografts or human tissue phantoms is warranted to ensure clinical relevance.
Conclusion
The research discusses CavitoMod-UTMDNet, which is a mechanistically guided model combining cavitation physics, diffusion-transportation modeling, pharmacokinetic modeling, ultrasound theory of action, and ultrasound microenvironmental transliberation of liposomal doprubicin in pancreatic ductal adenocarcinoma (PDAC). This framework provides quantitative connections between acoustic exposure, stromal remodeling, vascular permeability, and intratumoral drug transport using quantitative correlations between RP cavitation modeling, Fickian diffusion, and PK analysis into two compartments. Manipulated exposures of UTMD under the FDA-approved limits of mechanical index (MI ≤ 1.2) have a great potential in enhancing intracellular uptake, intratumoral drug uptake improvement by approximately 2.5 times, 2-fold stromal permeability, and tumor regression (54%) without causing systemic toxicity. Existing strong relationships between the energy density of cavitation and the therapeutic response also serve as confirmation of the predictive and mechanistic integrity of the suggested treatment.
Together, these findings indicate that UTMD can dismantle the dense stromal and vascular barriers of PDAC by an indirect, mechanically dependent, spatially targeted, and nondestructive manner of permeability modification. CavitoMod-UTMDNet opens the way to reproducible and scalable exposure optimization, personalized parameters, and ultimately inclusion in imaging-guided therapeutic processes due to the provision of a single experimental-computational platform. Future applications will also broaden the system to consist of real-time cavitation image, 3D patient-specific transport modeling, more nanocarrier formulations, and translational testing in large animals. The improvements will help bring UTMD-based drug delivery as a clinically viable, noninvasive, and precision-modulated therapeutic approach to enhance outcomes in PDAC.
Authors’ Contributions
Y.A., G.M., S.E., M.M., and A.M.A.-S.: Conceptualization, data curation, methodology, software, visualization, and writing—original draft. H.A., R.A., N.A., and S.A.E.: Investigation, validation, resource, formal analysis, and writing—editing and reviewing.
Footnotes
Acknowledgment
Ongoing Research Funding program, (ORF-2026-780), King Saud University, Riyadh, Saudi Arabia. The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through Large Research Project under grant number RGP2/569/46. Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R809), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. The authors extend their appreciation to the Deanship of Scientific Research at Northern Border University, Arar, KSA for funding this research work through the project number NBU-FFR-2026-1564-02. The Authors would like to thank the Deanship of Scientific Research at Majmaah University for supporting this work under Project No. R-2026-66. The authors are thankful to the Deanship of Graduate Studies and Scientific Research at University of Bisha for supporting this work through the Fast-Track Research Support Program.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.