
Abstract
Background:
In this single-center retrospective study, the authors evaluated whether real-time ultrasound-guided positioning of an implantable venous access port catheter tip at the superior vena cava-right atrial junction (SVC-RAJ) reduces the risk of catheter-related thrombosis (CRT) in adult patients with cancer and developed a multivariable risk prediction model to support individualized prevention.
Methods:
Clinical data from 600 consecutive patients who underwent port implantation at Zhongshan People’s Hospital were analyzed. Patients were grouped according to final catheter tip position (SVC-RAJ versus non-SVC-RAJ), and CRT incidence was compared between groups.
Results:
The overall incidence of CRT was 30.33% (182/600) and was significantly lower in the SVC-RAJ group than in the non-SVC-RAJ group (22.42% vs. 38.73%, p < 0.001). In multivariable analysis, catheter tip positioning at the SVC-RAJ remained an independent protective factor (odds ratio = 0.517, 95% confidence interval [CI]: 0.353–0.756). Age, body mass index (BMI), tumor stage, neutrophil-to-lymphocyte ratio, D-dimer level, catheterization duration, and prophylactic anticoagulation status were also independently associated with CRT. A nomogram integrating these variables demonstrated good discrimination (area under the curve = 0.866, 95% CI: 0.837–0.895), with a sensitivity of 70.33% and a specificity of 85.89%. Performance across specific age or BMI strata was not separately evaluated in this study, and further stratified validation in larger datasets is needed to assess model consistency across demographic subgroups.
Conclusions:
These findings support ultrasound-guided SVC-RAJ positioning as a clinically relevant strategy for reducing CRT risk and maintaining reliable venous access in contemporary oncology care pathways.
Keywords
Introduction
The use of implantable venous access port (IVAP) has become a favorable venous infusion technique in clinical practice in cancer patients undergoing chemotherapy due to convenience operation, reduced risk of infection, and longer service life. Nevertheless, catheter-related thrombosis (CRT) is among the most prevalent complications of IVAPs, and the reported rates of incidence are between 31.3% and 73.3%, which justly affects the course of treatment and the quality of life of patients. 1 Not only is CRT a potential cause of catheter dysfunction and unintended removal, but also may result in life-threatening events such as pulmonary embolism, raising health care expenses and limiting patients psychologically. 2 Therefore, one of the areas of interest in research within oncology supportive care is the investigation of CRT prevention and the creation of risk prediction models.
CRT pathophysiological processes comprise three main factors, which are vascular endothelial damage, hemodynamic changes, and hypercoagulability. These cells may develop a thrombogenic microenvironment through the release of procoagulant factors (tissue factors), platelet aggregation, and disruption of the integrity of vascular endothelial cells. Chemotherapeutic agents also increase thrombotic risk by impairing the integrity of the vascular endothelial cells and suppressing the production of anticoagulant proteins.3,4 Also, the presence of patient-specific (advanced age, obesity, inflammatory status) and catheter-related (catheter material, tip position, duration of catheterization) variables has been confirmed correlates of CRT occurrence. 2 Of these, the most ideal placement of IVAP tips has been especially controversial with the traditional X-ray guidance placing the tip at the mid-superior vena cava (SVC) position, but more recent research proposes the SVC-right atrial junction (SVC-RAJ) area, with faster blood flow and less turbulence, as more amenable to minimizing thrombus formation. 5
Real-time ultrasound-guided techniques have been progressively implemented in IVAP implantation procedures for vascular puncture and tip positioning due to their visualization advantages. Compared with conventional X-ray localization, ultrasound guidance enables dynamic monitoring of catheter trajectory, prevents vascular damage, and confirms tip positioning through intracavitary electrocardiography or Doppler flow signals. 6 Studies have shown 7 that in ultrasound-guided placement of the SVC-RAJ, the accuracy of tip placement is improved to above 92%, with a major reduction in hemodynamic abnormalities due to poor placement. However, there is no strong clinical evidence with large-sample studies on the preventive action of ultrasound-guided SVC-RAJ positioning on CRT. At the same time, mathematical models are now a critical instrument for risk prediction of the disease. 8 As a visualization model, multivariate regression-based nomograms have the potential to incorporate several independent risk factors to give a personal risk evaluation that could be used to make clinical decisions.
Based on these considerations, the purpose of the present single-center retrospective study is the evidence-based recommendations to prevent IVAP-related CRT with the most precision through the inclusion of real-time ultrasound-guided tip positioning as a modifiable risk factor in the model; integrating both clinical indicators and procedure factors to build a multidimensional risk prediction model; and the systematic assessment of the clinical utility of the model using receiver operating characteristic (ROC) curve analysis and K tests to provide a base for future multicenter research.
Materials and Methods
Patient demographics
The retrospective study involved 600 patients aged older than 18 years, with a cancer diagnosis, who had IVAP implantation at the Department of Medical Oncology, Zhongshan People Hospital. The patients whose data were included in the study were identified based on the hospital electronic medical record system and catheterization procedure database, which included patient demographics, laboratory tests, catheterization procedure documentation, and follow-up information. The Ethics Committee of this hospital signed the study (approval number: 2022-035-K037). The retrospective design predetermined the informed consent waiver, and the use of data was performed according to the privacy protection principles described in the Declaration of Helsinki.
Inclusion criteria
(1) Histopathologically confirmed malignancy requiring intravenous chemotherapy. (2) First-time IVAP implantation (model: Deltec® Port-A-Cath® Low Profile™ polysulfone/titanium venous access system with PolyFlow® polyurethane catheter, 1.9 mm [5.8 Fr] O.D. × 1.0 mm I.D., 6 Fr introducer; REF 21-4083-24). (3) Postprocedural confirmation of IVAP tip position via anteroposterior chest X-ray (Philips DigitalDiagnost C90) and color Doppler ultrasonography (Philips EPIQ 7 C, probe frequency 5–12 MHz). (4) Age ≥18 years with follow-up duration ≥3 months.
Exclusion criteria
(1) Concomitant hematological diseases (e.g., leukemia, lymphoma) or congenital coagulation malfunction. (2) History of violation of deep vein thrombosis or pulmonary embolism. (3) Preimplantation administration of anticoagulants (e.g., warfarin, low-molecular-weight heparin). (4) Incomplete clinical data (e.g., not documented time of catheterization, not completed ultrasound follow-up). (5) Pregnant or lactating women.
Grouping criteria
Patients were categorized into the following two groups based on IVAP tip position:
SVC-RAJ group (n = 223): Catheter tip positioned within the 1–2 cm range of the SVC-RAJ (measured by chest X-ray as the distance from the tip to the upper border of the right atrium, confirmed by ultrasound Doppler flow signals). Non-SVC-RAJ group (n = 377): Catheter tip positioned in the mid-SVC (>2 cm from the upper border of the right atrium) or other locations such as the internal jugular vein.
CRT diagnostic criteria
(1) Clinical manifestations included swelling, pain, infusion dysfunction, or elevated skin temperature in the catheterized limb. 9 (2) Imaging confirmation required Doppler ultrasonography demonstrating solid echoes around or within the catheter lumen, noncompressible venous lumen under pressure, flow signal filling defects, or distal flow velocity <10 cm/s. 10 Types of thrombus were categorized as fibrin sheath thrombosis, mural deep vein thrombosis, and intraluminal catheter thrombosis. 11 The diagnostic algorithm ranked ultrasound screening as the initial step on suspected cases and then the grading opened to symptom-based grading to confirm the suspected cases with a nonexclusive differentiation with conditions such as phlebitis. The ultrasound results were read out by 2 doctors who had 5 years or more experience, and diagnostic consistency was ensured by meeting the K of 0.85, which confirmed the diagnosis.
Data collection and quality control
Demographics and baseline characteristics:
Age and gender: The age is calculated, based on the birth date to the catheterization date, and is derived out of the patient identification information in the hospital information system; gender information based directly on the front pages of the medical record; and the error rate of double-checking the electronic and paper records is less than 0.5%. Body–mass index (BMI): Measured using SECA 813 electronic scales and SECA 213 height meters, calibrated weekly, with fasting weight and height measured precatheterization; calculated as weight (kg)/height (m).
2
Tumor type and staging: Tumor type determined from postoperative pathology reports or biopsy results; tumor staging based on AJCC 8th edition TNM classification,
12
assessed through imaging (CT/MRI) and pathological findings; pathology reports reviewed by two attending physicians, with staging discrepancies submitted to oncology multidisciplinary team consultation.
13
Laboratory parameters
Complete blood count (neutrophil-to-lymphocyte ratio [NLR], platelet-to-lymphocyte ratio [PLR]): 2 mL venous blood collected under fasting conditions within 72 h precatheterization, EDTA-anticoagulated, analyzed using an automated hematology analyzer (Sysmex XN-9000) for neutrophil, lymphocyte, and platelet counts; NLR = neutrophil count/lymphocyte count; PLR = platelet count/lymphocyte count; daily calibration with internal quality control samples, CV <5%; abnormal results verified by blood smear examination.
14
Coagulation profile (D-dimer, fibrinogen): 2 mL venous blood collected under fasting conditions within 72 h precatheterization, sodium citrate-anticoagulated; fibrinogen (FIB) measured by magnetic bead method (Stago STA-R Max), D-dimer by immunoturbidimetry; reference ranges: D-dimer <0.5mg/L, FIB 2–4 g/L; each batch tested with international standards (ISTH standard),
15
interbatch CV <8%. Inflammatory markers (hs-CRP, TNF-α): 3 mL venous blood collected under fasting conditions within 72 h precatheterization, serum separated, and stored at −80°C pending analysis; hs-CRP measured by immunoturbidimetry (Roche Cobas 8000), detection limit 0.02mg/L; TNF-α by ELISA (R&D Systems), detection range 3.12–200 pg/mL; each plate included low-, medium-, and high-concentration quality controls, recovery rate 90%–110%. Catheterization-related factors: Access route, catheterization duration, catheter material (polyurethane/silicone), prophylactic anticoagulation use. IVAP tip position (SVC-RAJ/non-SVC-RAJ):
Vertical distance from the catheter tip to the upper border of the right atrium was measured on standardized anteroposterior chest X-ray images (precision to 1 mm). To reduce the influence of respiratory motion and posture-related variation, measurements were performed on routine supine imaging obtained under standardized radiographical positioning conditions. A distance ≤20 mm within the middle-lower one-third segment of the SVC was classified as SVC-RAJ; otherwise, placement was categorized as non-SVC-RAJ. For measurements within ±2 mm of the 20 mm cutoff, repeat assessment and consensus review were performed to minimize misclassification. Cases with persistent measurement uncertainty after repeat review were conservatively categorized as non-SVC-RAJ to avoid overestimation of the protective effect. Measurements were independently performed by 3 radiologists, demonstrating high reproducibility (intraclass correlation coefficient [ICC] = 0.93; 95% confidence interval [CI] 0.89–0.96). Discrepancies >2 mm triggered repeat assessment and consensus review. To address anatomical variability, including differences in body habitus and age-related vascular changes, positioning assessment relied on fixed anatomical landmarks (upper border of the right atrium) rather than external body surface references. Real-time Doppler flow confirmation was used to verify intravascular location, thereby reducing potential measurement deviation associated with obesity or altered thoracic configuration. CRT diagnosis: Ultrasound examination using Philips EPIQ 7C (5–12 MHz linear array probe), with double-blind interpretation by 2 physicians with >5 years of experience.
Ultrasound-guided IVAP implantation procedures were performed by attending physicians with prior institutional training in ultrasound-guided vascular access and tip localization. All operators had independently performed more than 50 ultrasound-guided central venous procedures before participation in this study, reflecting standard competency requirements at this center.
Statistical analysis
Data were analyzed using SPSS 26.0, MedCalc (V20.0.3), and GraphPad Prism 9 software. The Kolmogorov–Smirnov test was used to verify normal distribution of quantitative data. Normally distributed quantitative data were expressed as mean ± standard deviation (x̄ ± s) and compared between groups using independent t-tests. Categorical data were presented as number (percentage) and analyzed using χ2 tests. Multivariate logistic regression analysis was performed on variables identified in univariate analysis, with regression coefficients (β), standard errors (SEs), odds ratios (ORs), and 95% CIs recorded. Prior to multivariable modeling, collinearity diagnostics were performed by examining variance inflation factors (VIFs) to assess potential correlation among inflammatory and coagulation-related predictors. All included variables demonstrated VIF values below 2.0, indicating the absence of clinically relevant multicollinearity. ROC curves were utilized to assess diagnostic performance, with area under the curve (AUC), Youden index (YI), and 95% CI documented. Assumptions of logistic regression were evaluated prior to final model construction. Linearity of continuous predictors on the log-odds scale was assessed using the Box–Tidwell approach, and no significant deviation from linearity was detected. Model fit was further examined using the Hosmer–Lemeshow goodness-of-fit test.
Results
Comparison of patient baseline characteristics
As shown in Table 1, a total of 600 patients were included in this study, with 223 patients in the SVC-RAJ group and 377 patients in the non-SVC-RAJ group. The two groups were well-balanced in terms of gender, tumor type, and other indicators. However, the non-SVC-RAJ group exhibited significantly higher values in age, BMI, and other parameters compared with the SVC-RAJ group (p < 0.05).
Comparison of Patient Baseline Characteristics [n(%)/(

SVC-RAJ, superior vena cava-right atrial junction; BMI, body–mass index; NLR, neutrophil-to-lymphocyte ratio.
CRT incidence and univariate analysis
As demonstrated in Table 2, among the 600 patients included in this study, 182 developed CRT postoperatively, yielding an overall incidence rate of 30.33%. The CRT incidence in the SVC-RAJ group was 22.42% (49/223), which was significantly lower than the 38.73% (146/377) observed in the non-SVC-RAJ group (χ2 = 23.56, p < 0.001). Univariate analysis revealed that age, BMI, NLR, catheterization duration, tumor stage, D-dimer levels, prophylactic anticoagulation use, and catheter tip position were significantly associated with CRT occurrence (p < 0.05). The remaining parameters demonstrated no statistical significance (p > 0.05).
Demographics and Baseline Characteristics [(
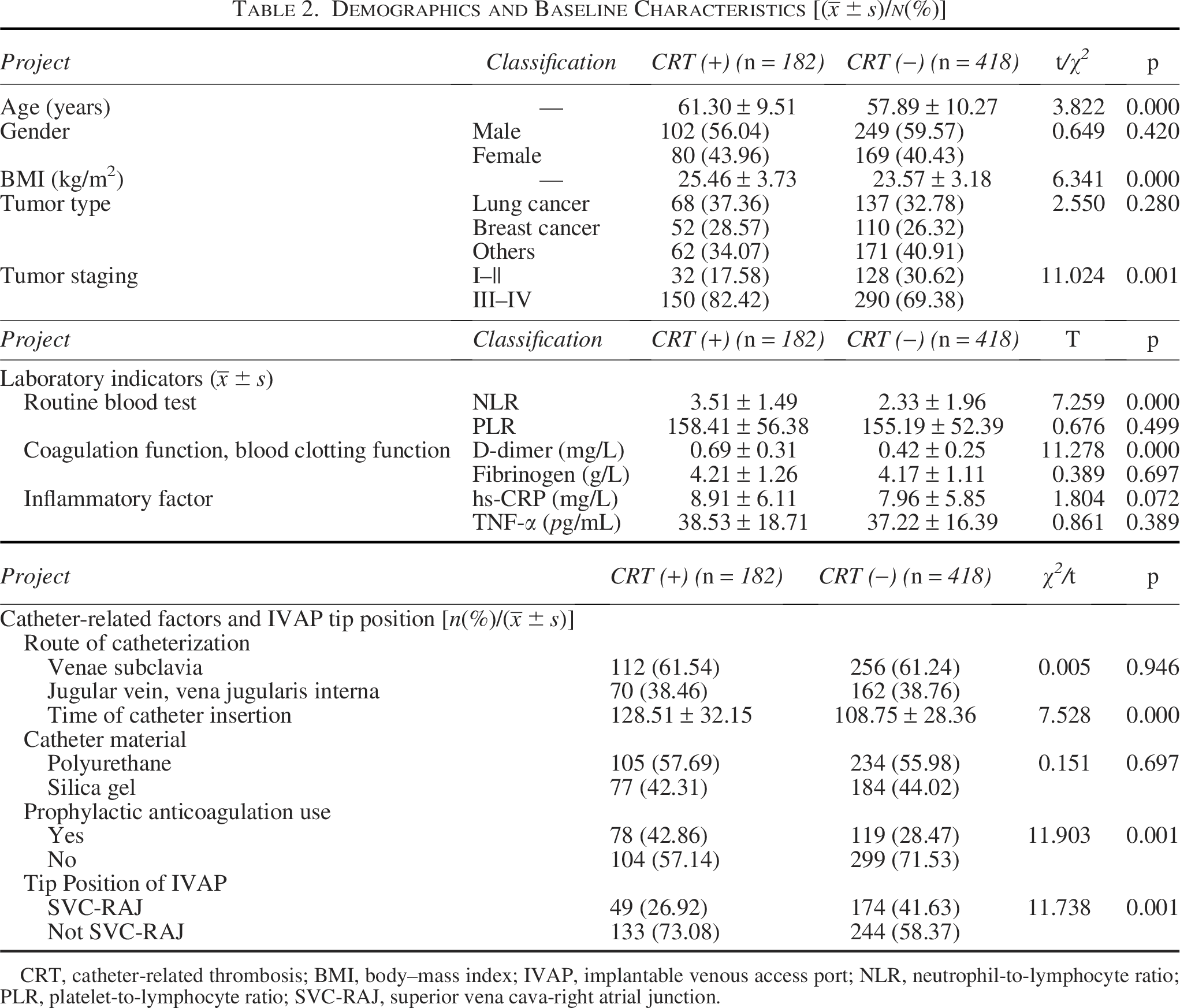
CRT, catheter-related thrombosis; BMI, body–mass index; IVAP, implantable venous access port; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SVC-RAJ, superior vena cava-right atrial junction.
Logistic regression analysis of risk factors for CRT in IVAP patients
Using CRT diagnosis as the dependent variable factors with p < 0.05 in univariate analysis, age, BMI, tumor stage, NLR, D-dimer, catheterization duration, tip position, and prophylactic anticoagulation status were incorporated as independent variables into a logistic regression model. The results demonstrated that all aforementioned factors were independent risk factors for CRT development (p < 0.05). These findings are presented in Tables 3 and 4, Figure 1 shows prediction of CRT line chart of related independent risk factors, Figure 2 shows DCA validation curve of the prediction model for CRT risk in IVAP patients, and Figure 3 shows the calibration curve of the CRT risk prediction model for IVAP patients.
Variable Assignment
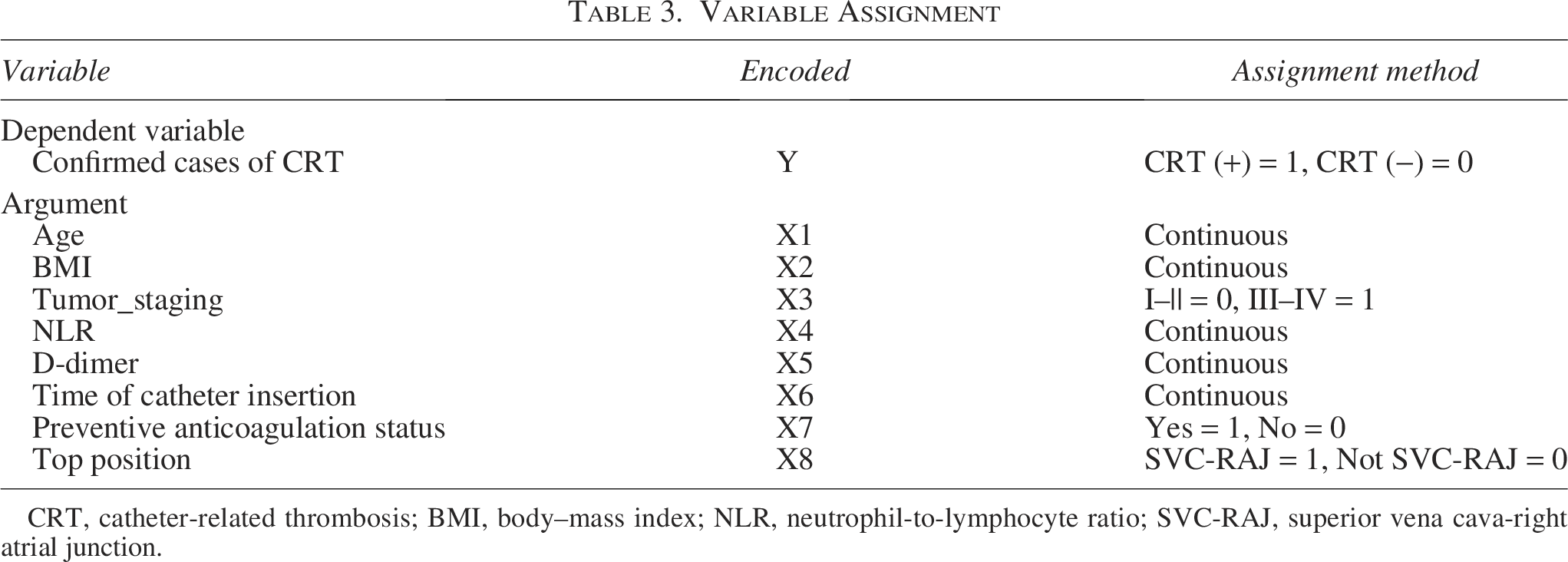
CRT, catheter-related thrombosis; BMI, body–mass index; NLR, neutrophil-to-lymphocyte ratio; SVC-RAJ, superior vena cava-right atrial junction.
Logistic Regression Analysis of Risk Factors for Catheter-Related Thrombosis Risk in Implantable Venous Access Port Patients
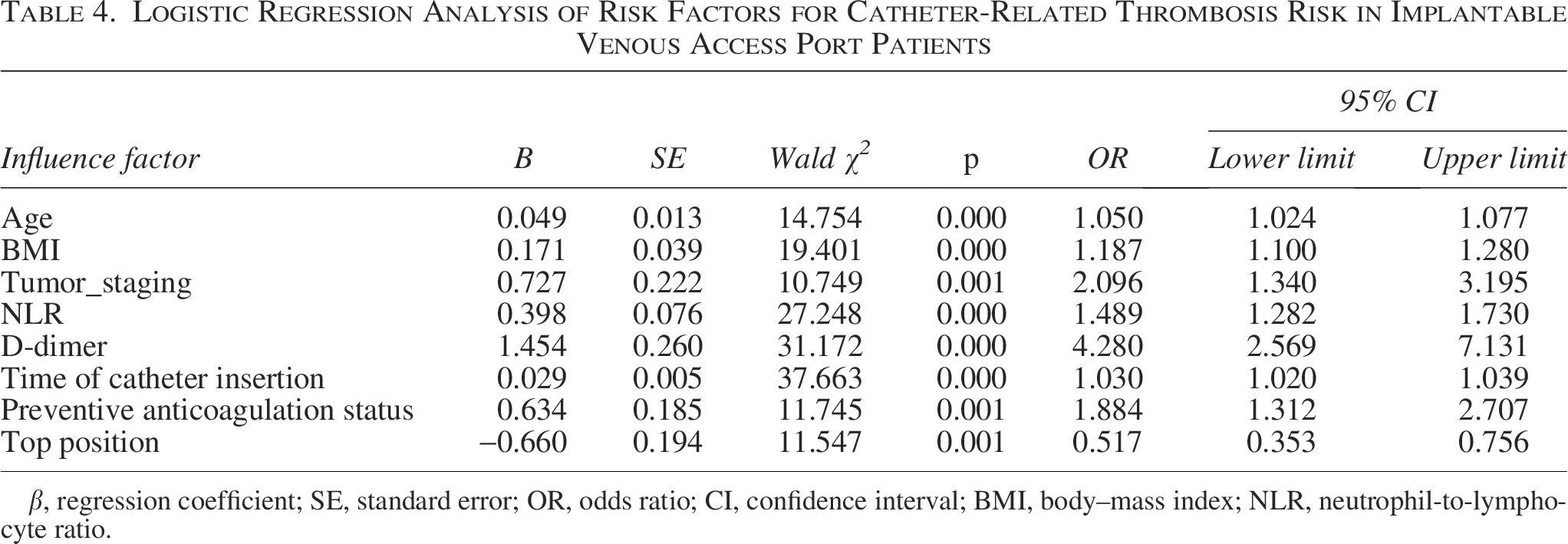
β, regression coefficient; SE, standard error; OR, odds ratio; CI, confidence interval; BMI, body–mass index; NLR, neutrophil-to-lymphocyte ratio.
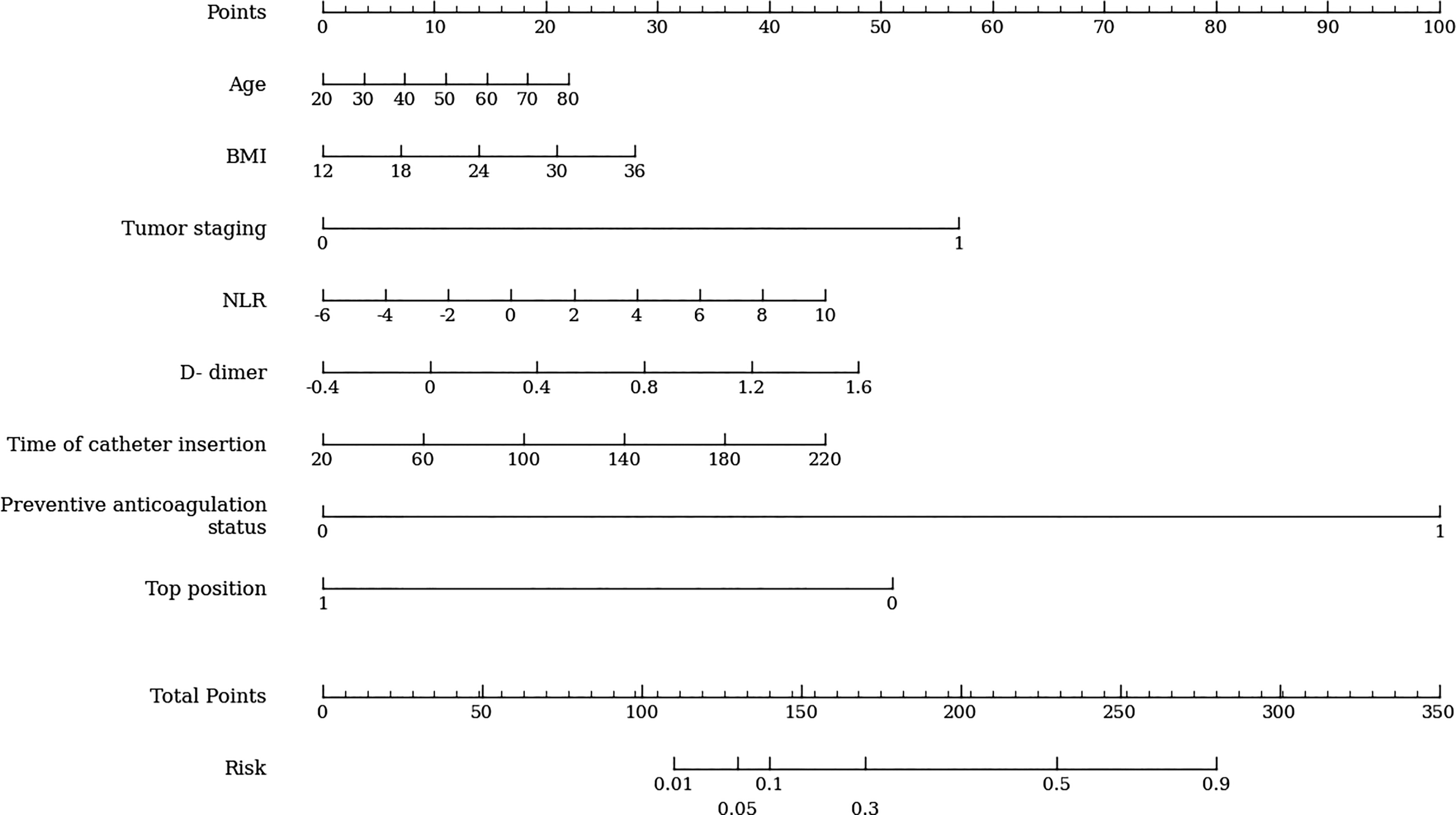
Prediction of catheter-related thrombosis (CRT) line chart of related independent risk factors.
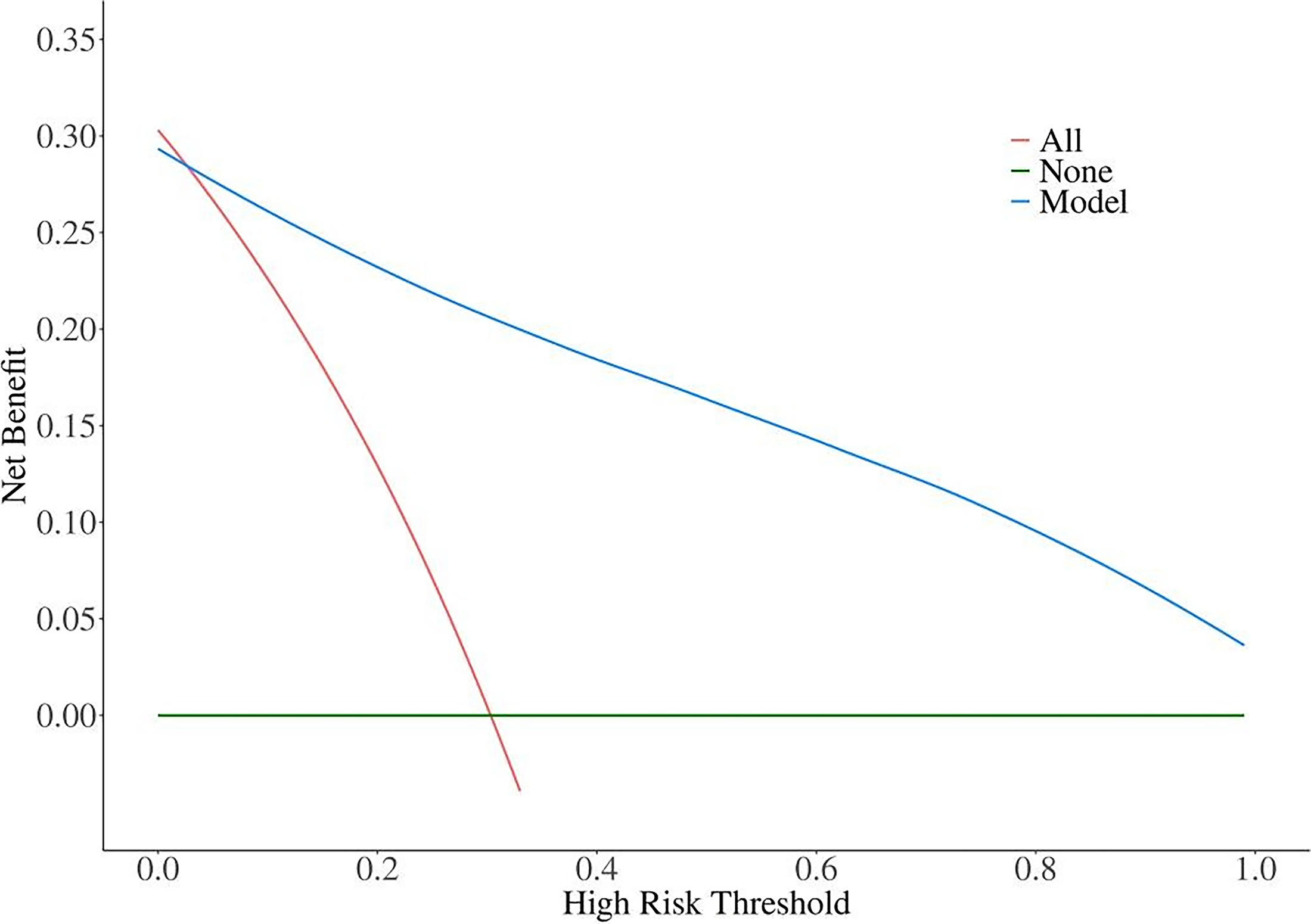
DCA validation curve of the prediction model for catheter-related thrombosis (CRT) risk in implantable venous access port (IVAP) patients.
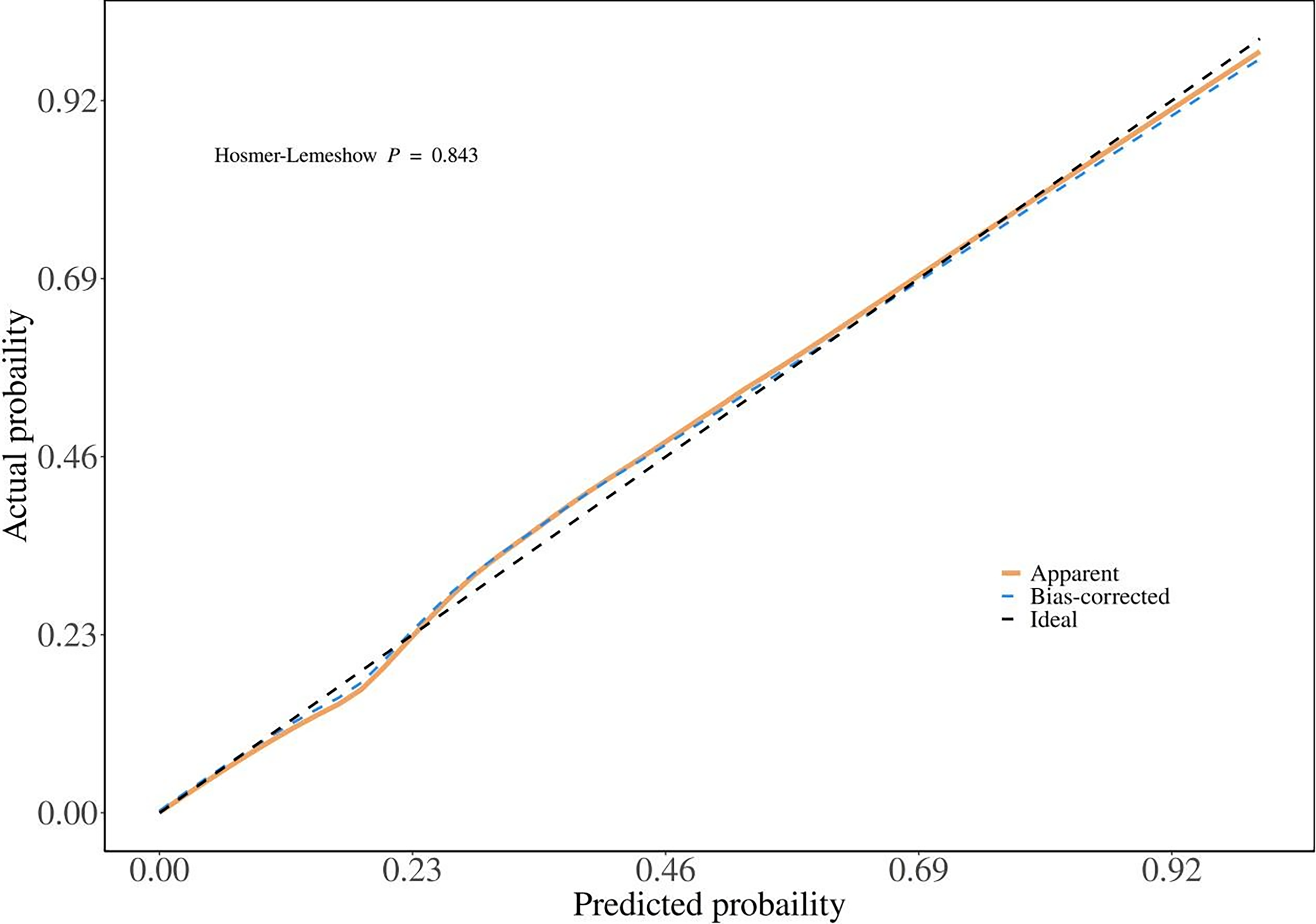
Calibration curve of catheter-related thrombosis (CRT) risk prediction model for implantable venous access port (IVAP) patients.
ROC curve analysis of the prediction model
Based on the regression coefficients, a prediction model was constructed: Logit (P) = β1X1 + β2X2 + β3X3 + … (where P represents probability, X represents relevant influencing factors, and β represents the regression coefficient of the corresponding independent variable). The regression coefficients and ORs for each variable were calculated.
The resulting regression equation for the combined prediction model was as follows:
Logit (P) = 0.049 × Age + 0.171 × BMI + 0.727 × Tumor stage + 0.398 × NLR + 1.454 × D-dimer + 0.029 × Catheterization duration + 0.634 × Prophylactic anticoagulation status − 0.660 × IVAP tip position. The prediction model was evaluated using ROC curves, with calculation of the AUC and 95% CI. Results indicated that the combined prediction model demonstrated higher AUC values than any single parameter assessment. Detailed results are presented in Table 5, and Figure 4 shows the ROC curves of single prediction and joint prediction.
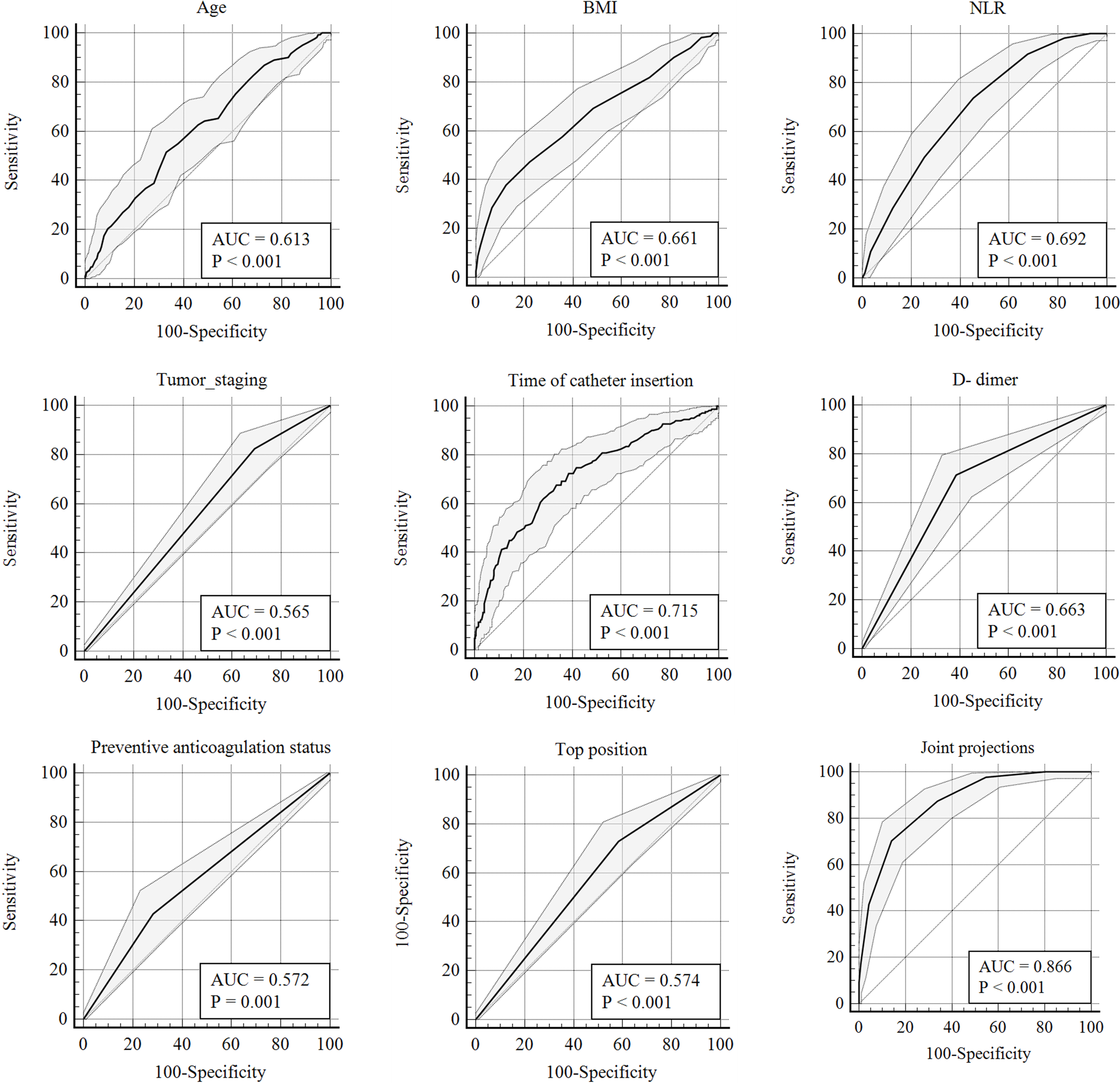
Receiver operating characteristic (ROC) curves of single prediction and joint prediction.
Receiver Operating Characteristic Prediction Value Curve Analysis of Single and Combined Predictions of Catheter-Related Thrombosis Risk in Implantable Venous Access Port Patients
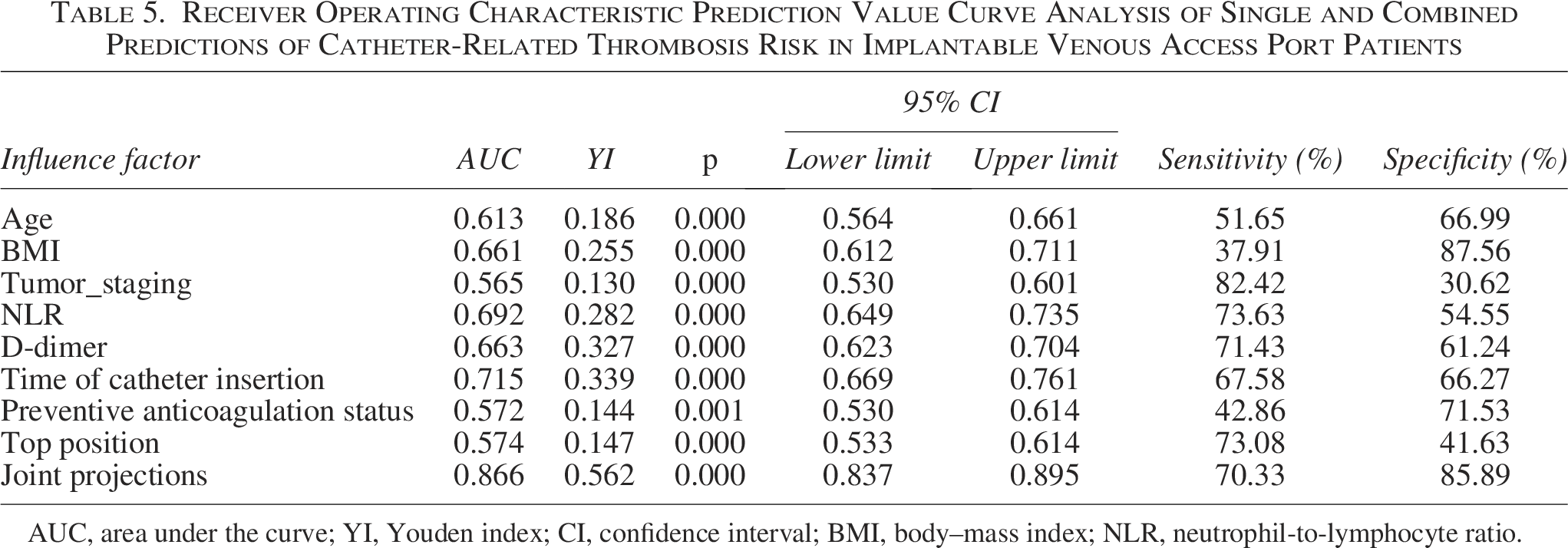
AUC, area under the curve; YI, Youden index; CI, confidence interval; BMI, body–mass index; NLR, neutrophil-to-lymphocyte ratio.
Discussion
Real-time ultrasound-guided positioning of IVAP catheter tips at the SVC-RAJ significantly reduced CRT in adult cancer patients (22.42% versus 38.73% in non-SVC-RAJ, p < 0.001), supporting ultrasound guidance as a clinically actionable risk-mitigation strategy in oncology supportive care. This is consistent with prior evidence that ultrasound-guided positioning improves accuracy (reported >92%) and reduces malposition-related issues. 16 From a mechanistic perspective, the SVC-RAJ region is characterized by higher flow velocities and atrial washout, which may shorten the time window for fibrin sheath formation and thrombus initiation, 17 while the relatively stable vessel diameter may reduce catheter-wall contact and mechanical endothelial injury.18,19 Compared with conventional X-ray positioning, real-time ultrasound (combined with intracardiac ECG and Doppler signal confirmation in this workflow) provides dynamic confirmation during placement and aids avoid respiratory-motion measurement errors reported with X-ray-based approaches, 20 which may reduce the need for repeated readjustments and thereby lower thrombosis-promoting endothelial trauma. 21 Importantly, multivariate analysis confirmed tip position as an independent protective factor (OR = 0.517, 95% CI: 0.353–0.756), indicating that the benefit of SVC-RAJ targeting persists beyond baseline patient differences. While this single-center study did not conduct subgroup-specific interaction analyses, the relatively narrow CIs for the primary predictors indicate statistical stability within the overall cohort. Future multicenter studies should formally evaluate interaction effects across demographic and clinical strata. The primary endpoint was CRT incidence, no systematic increase in infusion resistance, catheter dysfunction, or need for repositioning was observed during follow-up in the SVC-RAJ group according to routine clinical documentation. While functional endpoints were not predefined outcomes in this retrospective analysis, these observations suggest that SVC-RAJ positioning did not compromise port usability in daily practice.
Risk prediction modeling represents a central component of this study and requires consideration across methodological, biological, and translational layers. Beyond tip position, this model suggests that CRT risk reflects the combined impact of hypercoagulability, tumor burden, inflammation, and procedural exposure. Variable selection for multivariable modeling was based on statistical significance in univariate analysis to reduce the risk of overfitting in this single-center dataset. While this approach may exclude clinically meaningful predictors that do not reach initial statistical thresholds, variables with established biological plausibility such as tumor stage, inflammatory indices, and coagulation markers were retained when statistically supported. Future studies with larger cohorts may allow broader candidate variable inclusion or penalized regression approaches to enhance robustness. D-dimer showed the strongest association (OR = 4.280), consistent with coagulation activation as a core driver of CRT in cancer and the broader framework of Virchow’s triad, 22 and prior work supporting D-dimer as a sensitive biomarker for thrombotic risk stratification.23,24 Advanced tumor stage (III–IV) increased CRT risk (OR = 2.096), plausibly linked to higher procoagulant activity and systemic inflammation in progressive malignancy.25,26 Tumor stage was modeled categorically according to AJCC classification, without stratification by cancer type. While this approach standardizes staging severity across malignancies, potential heterogeneity among different tumor types was not formally examined and warrants future investigation. Elevated NLR (OR = 1.489) further supports an inflammation-coagulation axis contribution to catheter-related events in oncology patients.27,28 The association between prophylactic anticoagulation and higher CRT risk (OR = 1.884) may reflect confounding by indication, whereby patients perceived as high risk were more likely to receive anticoagulation. Formal causal inference testing was beyond the scope of this retrospective study, and this variable should be interpreted cautiously. 29
Ultimately, the nomogram exhibited robust discrimination (AUC = 0.866) and satisfactory calibration, endorsing its clinical application for personalized CRT risk assessment and the implementation of risk-adapted prevention strategies, consistent with the Special Issue’s focus on clinical risks. In routine oncology practice, IVAP implantation is frequently conducted under time constraints, particularly in high-volume chemotherapy centers. Therefore, it is pertinent to elucidate how ultrasound-guided SVC-RAJ targeting can be integrated into standard procedural workflows. In this protocol, ultrasound was routinely used for vascular puncture, and tip positioning confirmation was achieved within the same procedural session using real-time Doppler flow assessment, followed by standard postprocedural chest X-ray verification. As tip localization was incorporated into the natural sequence of catheter advancement, no additional procedural steps beyond standard confirmation were necessary. These findings indicate that ultrasound-guided SVC-RAJ targeting can be assimilated into fast-paced clinical settings within established procedural workflows, while being associated with a reduced incidence of CRT in this cohort. A practical translation pathway involves treating ultrasound-guided SVC-RAJ targeting as the procedural first-line risk-control measure, while reserving intensified monitoring and anticoagulation strategies for patients exceeding a predetermined predicted-risk threshold. Prior to routine clinical adoption, prospective multicenter validation with predefined assessment of discrimination, calibration, and clinical utility is essential to confirm generalizability and refine implementation thresholds.
For clinical translation, predicted probabilities derived from the nomogram can be stratified using ROC-derived optimal cutoff values. In this cohort, the YI-based threshold corresponded to a predicted probability that may serve as an initial reference for distinguishing higher-risk patients, although external validation is necessary before defining standardized risk categories. In this cohort, the combined model yielded a YI of 0.562, which may serve as a reference threshold for identifying patients who could benefit from intensified surveillance or preventive strategies. Beyond individual risk estimation, practical implementation requires consideration of procedural standardization across centers. Given the inevitable multicenter variation in implantation techniques, standardized ultrasound-based positioning protocols, including clearly defined anatomical landmarks, measurement criteria, and reproducibility verification, may aid reduce intercenter variability. The high ICC observed in this study supports the feasibility of achieving reproducible positioning when structured measurement procedures are applied. Integrating risk prediction into preimplantation multidisciplinary planning discussions represents a practical translational step. During preprocedure assessment, input of routinely available variables (age, BMI, tumor stage, NLR, D-dimer, catheterization duration, anticoagulation status, and planned tip position) into the nomogram may facilitate individualized risk estimation and inform decisions regarding enhanced monitoring or procedural precision strategies. Preprocedural identification of high-risk patients may guide decisions regarding intensified monitoring, individualized consideration of anticoagulation, and precision targeting of catheter tip placement within the SVC-RAJ region.
Conclusion
The authors recommend routine use of real-time ultrasound-guided techniques for IVAP placement in cancer patients, with catheter tip targeting at the SVC-RAJ (approximately 1–2 cm above the junction) as a standardized approach to reduce CRT risk. For patients with higher predicted risk (older age, elevated BMI, advanced tumor stage, increased NLR, elevated D-dimer, and longer catheterization duration), preprocedure risk stratification using the nomogram may support individualized prevention and closer ultrasound surveillance. In high-risk patients, preventive strategies should be selected using a risk–benefit framework and aligned with institutional thromboprophylaxis guidance, with attention to bleeding risk and treatment continuity. Future work should prioritize multicenter prospective validation across tumor types, incorporation of ultrasound-derived hemodynamic parameters to strengthen mechanistic interpretation, and evaluation of multimodal biomarkers (e.g., circulating tumor cells and extracellular vesicles) to refine prediction accuracy, thereby advancing ultrasound-enabled, risk-focused supportive care pathways in oncology.
Authors’ Contributions
Q.L.: Conceptualization, methodology, data curation, formal analysis, and writing—original draft. Y.Y.: Investigation, data curation, validation, and writing—review and editing. J.W.: Investigation, resources, data acquisition, and writing—review and editing. J.L.: Formal analysis, visualization, software, and writing—review and editing. Y.C.: Supervision, project administration, conceptualization, funding acquisition, and writing—review and editing.
Footnotes
Acknowledgments
Disclosure Statement
The authors declare they have no competing interests regarding this research.