
Abstract
Background:
The enhancement of the therapeutic window (TW) in oncology remains a significant challenge, as the majority of anticancer treatments face difficulties in achieving optimal tumor control while minimizing adverse effects. Traditional chemotherapeutic agents, while demonstrating efficacy, are constrained by their limited TWs and the occurrence of systemic adverse effects.
Objective:
Recent advancements in precision medicine have revolutionized this paradigm by facilitating targeted tumor intervention via molecularly guided therapies, immuno-oncology strategies, and biomarker-driven patient classification. Novel approaches, including nanomedicine, antibody–drug conjugates, and prodrug formulations, improve therapeutic selectivity through the optimization of drug delivery, biodistribution, and release kinetics.
Methodology:
The concurrent advancements in radiotherapy, adaptive dosing methodologies, and toxicity assessment instruments have expanded the potential to enhance treatment intensity while preserving the integrity of normal tissues. In the future, the convergence of artificial intelligence (AI), multiomics profiling, and systems biology is anticipated to enhance therapeutic decision-making and expedite the creation of more personalized and adaptive interventions.
Results:
The efficacy of cancer treatments is substantially limited by notable shortcomings in research, despite progress in precision oncology. Tumor heterogeneity, the emergence of resistance mechanisms, and the absence of reliable biomarkers for anticipating treatment outcomes present significant impediments. The utilization of multiomics data and AI in clinical decision-making remains in its early stages, constrained by limitations in data validation and standardization. Furthermore, the translation of transdisciplinary concepts into accessible treatments is crucial, especially in environments with limited resources. Consequently, addressing these multifaceted issues is essential for improving the efficacy and safety of cancer treatments.
Conclusion:
This review integrates contemporary strategies and examines prospective pathways for expanding the TW, highlighting the intersection of technology, biology, and clinical innovation in the progression of cancer treatment.
Keywords
Introduction: The Challenge of the Therapeutic Window in Oncology
Cancer remains a major global health issue, causing about 10 million deaths each year. In the last few decades, biomedical science has made quick progress, leading to powerful new treatments that have changed oncology from a field with few options to one that offers longer survival and, in many cases, the chance of a cure. 1 Even with these improvements, there is still a significant problem that limits the effectiveness and safety of cancer treatments: the limited therapeutic window (TW). 2 This idea has to do with the delicate balance between the dose of a drug that produces the desired therapeutic effect and the dose that causes unacceptable toxicity. 3 In many areas of medicine, this range is quite wide, which lets doctors change the doses to make them more effective while also lowering the risk of side effects. In oncology, the TW is typically narrow, often forcing clinicians to choose between inadequate cancer treatment and overtreatment of the patient. 4
The biological characteristics of cancer and the pharmacological mechanisms of the drugs used to treat it are what make this problem so hard. A lot of cancer treatments work by disturbing important cellular processes, such as DNA replication, making the mitotic spindle, or making nucleotides. 5 The dysregulation of these processes in malignant cells is in stark contrast to their essential function in the survival and proliferation of normal tissues, particularly in regions with high cellular turnover, such as the bone marrow, gastrointestinal mucosa, and hair follicles. 6 As a result, systemic toxicity is an unwanted feature of chemotherapy. Patients often fear the negative effects of drugs, such as myelosuppression, mucositis, alopecia, nausea, and organ damage. 7 These effects are not just random; they are directly related to how the drugs work. The convergence of therapeutic and toxic mechanisms constricts the TW, requiring precise dosing and meticulous monitoring (Table 1).
Example of Drugs with Narrow Versus Wide Therapeutic Windows 8
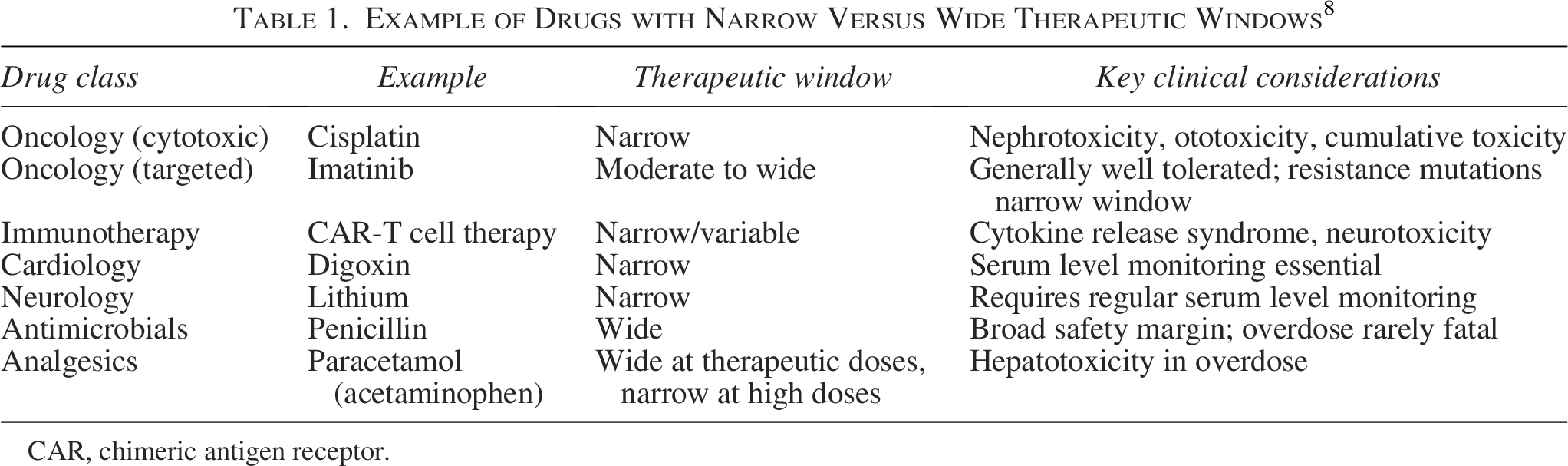
CAR, chimeric antigen receptor.
Interventions targeting genetic drivers of cancer
A defining characteristic of cancer is the buildup of genetic and epigenetic changes that fuel unregulated cell division, enable evasion of programmed cell death, and facilitate immune system avoidance. Therapeutic approaches within this domain are designed to rectify, impede, or leverage these oncogenic irregularities. 9
Targeting oncogenes and tumor suppressor genes
Cancer often involves the dysregulation of oncogenes such as MYC and RAS, which leads to continuous signaling that promotes cell growth. Although directly targeting these proteins has been difficult, recent developments in small-molecule inhibitors and RNA-based treatments are starting to overcome these challenges. 10 For example, inhibitors that target the RAS pathway, such as KRAS G12C inhibitors, have shown clinical success in certain types of tumors.
Tumor suppressor genes, including TP53, frequently undergo inactivation within malignant tumors. Therapeutic approaches encompass the reactivation of mutant p53 or the reestablishment of its downstream signaling cascades. Compounds such as rebecsinib and other p53 modulators are designed to reinstate apoptotic function and genomic integrity.
Chromosomal abnormalities and translocations
Chromosomal rearrangements, such as the t(8;14) translocation found in Burkitt lymphoma, lead to abnormal gene expression, such as the overexpression of MYC. These alterations can be targeted with therapeutic strategies that use precision medicine, including inhibitors of downstream signaling pathways or epigenetic modulators. 11
Impairment of antigen presentation mechanisms
Tumors can circumvent immune surveillance by diminishing the expression of major histocompatibility complex (MHC) molecules, frequently via deletions or mutations within chromosomal areas such as 6q or 15q. Therapeutic strategies are designed to reinstate antigen presentation, encompassing interferon-based treatments or epigenetic agents that enhance MHC expression.
Virus-induced oncogenesis
Certain oncogenic viruses, including the Epstein–Barr virus and human papillomavirus, instigate malignant transformation via integration into the host genome and the expression of viral oncogenes. Therapeutic approaches encompass antiviral agents, therapeutic vaccines, and immune-based targeting of antigens expressed by the virus.
Targeted molecular therapies
Tyrosine kinase inhibitors (TKIs) are fundamental to targeted therapy, acting to block abnormal signaling cascades that are essential for both tumor proliferation and survival. Illustrative examples encompass the following:
Sunitinib and donafenib: Multitargeted TKIs that impact angiogenesis and tumor proliferation.
Tofacitinib: A JAK inhibitor with relevance in specific malignancies and inflammatory pathways.
These therapeutic agents exemplify precision oncology, in which treatments are customized according to the molecular alterations present within the tumor.
Agents that directly kill tumor cells
This category includes treatments that directly kill cancer cells, either through biochemical actions or by using the immune system. 12 Conventional chemotherapy continues to be a fundamental component of cancer management. These cytotoxic agents exert their effects on rapidly proliferating cells by disrupting DNA replication, mitosis, or essential metabolic pathways. Frequently encountered classes of these agents encompass the following:
Alkylating agents
Cyclophosphamide, antimetabolites, including methotrexate and 5-fluorouracil, microtubule inhibitors exemplified by paclitaxel, notwithstanding their therapeutic benefits, these drugs are linked to systemic toxicity, a consequence of their nonspecific action.
Monoclonal antibodies
Antibodies that target specific receptors bind to particular antigens found on tumor cells. This binding then leads to either a halt in tumor growth or immune-mediated cell death. A well-known example of this is HER2-targeted therapy for breast cancer, such as trastuzumab. This therapy works by blocking receptor signaling and triggering antibody-dependent cellular cytotoxicity. 13
Chimeric antigen receptor T cell therapy
Chimeric antigen receptor (CAR) T cell therapy entails the genetic modification of T cells harvested from a patient, enabling them to express receptors that target antigens unique to tumors. Following reinfusion, these engineered cells initiate direct tumor cell destruction via cytotoxic processes. This therapeutic strategy has demonstrated considerable efficacy in treating hematological malignancies, especially B cell leukemias and lymphomas. 14
Immune-modulating therapies that boost tumor immunogenicity
These therapies, instead of directly attacking tumor cells, stimulate or restore the host immune system’s ability to recognize and eliminate cancer.
Augmenting antigen presentation and immunogenicity
The immunogenicity of tumors can be augmented through the upregulation of human leukocyte antigen expression and the facilitation of antigen presentation. This can be achieved through several approaches: Cancer vaccines, which introduce tumor-associated antigens to initiate immune responses. Immunostimulants and adjuvants, which enhance dendritic cell activation and T cell priming. Cytokine therapies, such as interferons, which increase MHC expression and antigen processing.
Activation of innate immunity
Innate immune agonists, including toll-like receptor agonists and STING pathway activators, stimulate early immune responses and foster a proinflammatory tumor microenvironment (TME), thereby promoting adaptive immunity.
Mitigating tumor-induced immunosuppression
Tumors use various mechanisms to actively suppress immune responses, encompassing checkpoint pathways and immunosuppressive cell populations. 15 Several key therapeutic strategies are used: Immune checkpoint inhibitors (ICIs), which are antibodies that target PD-1, PD-L1, or CTLA-4, serve to restore T cell activity. Regulatory T cell depletion reduces immunosuppressive signaling. Myeloid-derived suppressor cell inhibition enhances antitumor immunity. Tumor-associated macrophage reprogramming shifts macrophages from a protumor (M2/type II) to an antitumor (M1) phenotype. These approaches have significantly advanced oncology, particularly in the treatment of melanoma, lung cancer, and other solid tumors.
Is evolving to adapt to selective pressures over time that can change? Cancers are distinguished by a heterogeneous composition of subclonal populations, whereas infectious diseases are generally attributed to more uniform pathogens, even within a singular tumor mass. 9 The responsiveness of these subclones to treatment may demonstrate considerable variability. An appropriate dosage sufficient to eradicate one population may preserve another, thereby promoting relapse and the emergence of resistance. Health care professionals often deal with this problem by adding to treatment plans, raising drug dosages, or using a mix of therapeutic agents. However, this usually makes the body more toxic. 10 On the contrary, lowering the dose to lessen side-effects may make the drug less effective, which is why resistant clones are so common. As a result, oncologists often have to negotiate the risks of both undertreatment and overtreatment. The patient’s TW is the only way to find a cure or control that works. 11
This pathway is further restricted by the unique characteristics of each patient. Age, performance status, comorbidities, and organ function are all very important when figuring out how much treatment a person can safely handle. An older person with kidney or liver problems may experience severe toxicity at doses that a younger, healthier person can usually handle. Genetic variations that affect how drugs are broken down have significant effects. 12
For instance, a lack of thiopurine methyltransferase (TPMT) has a significant effect on how the body breaks down thiopurines, while changes in UGT1A1 affect how the body gets rid of irinotecan. Not recognizing these differences could result in standard dosing schedules that unintentionally expose patients to toxicities beyond their tolerance, completely ruining the TW. 13 Advancements in pharmacogenomics and biomarker-driven therapy are progressively improving the potential for personalized dosing; nonetheless, the present state of oncology practice remains constrained by narrow limitations. 14
The TME adds another layer of difficulty. Malignant tissues often exist in a difficult microenvironment characterized by hypoxia, abnormal blood vessel formation, acidic pH levels, and dense stromal barriers. These traits make it harder for drugs to uniformly spread through tumor through the tumor tissue. 15 To get through these barriers, systemic drug concentrations may need to be raised in some cases. However, this also makes healthy tissues more likely to be exposed to toxic effects. In addition, cells in tumors that are hypoxic or low in nutrients may not respond as well to treatments that target quickly growing cells. 16 This forces doctors to choose between increasing treatment with the risks that come with it or accepting less than ideal tumor control. As a result, the TW should be seen as a variable trait that comes from the drug, the biology of the tumor, and the host’s physical condition. 17
The historical quest for the optimization of this equilibrium has profoundly impacted the evolution of cancer treatment methodologies. The first few years of chemotherapy were marked by drugs that worked very well but had bad side-effects. 18 The rates of remission rose for some leukemias and lymphomas, but this was accompanied by serious side-effects, the development of secondary cancers, and death from treatment. Combination regimens were developed to address this challenge: By utilizing agents with complementary mechanisms of action and unique toxicological profiles, it became possible to increase the therapeutic intensity while staying within acceptable limits of tolerability. 19 New ideas in supportive care, such as using antiemetics, hematopoietic growth factors, and organ-protective adjuvants, have aided to slightly widen the TW, allowing for higher dose intensity while keeping the risk level acceptable. Despite these improvements, the fundamental problem of finding a balance between effectiveness and toxicity was still not solved. 20
The arrival of molecularly targeted therapies at the start of the century signaled a possible change in the way medicines work. Imatinib and other drugs that specifically target the BCR-ABL tyrosine kinase that causes chronic myeloid leukemia (CML) have shown that treatment plans can be very effective while keeping toxicity levels low by focusing on the specific molecular weaknesses in tumors. 21 This accomplishment has fostered optimism concerning the capacity to substantially enlarge the TW in oncology through precision medicine. Targeted therapies have shown great effectiveness in some cancers, such as gastrointestinal stromal tumors and some lung cancers, while keeping side-effects manageable. 22 However, the overall experience has been more sobering. Many targeted therapies not only block the specific oncogenic drivers, but they also affect kinases that are structurally similar in normal tissues. This can cause off-target toxicities such as high blood pressure, skin problems, or heart problems. In addition, the emergence of resistance mutations often necessitates higher dosages or more potent combinations, thereby further narrowing the therapeutic margin. 23
Immunotherapy means a significant change with significant effects on the TW. Checkpoint inhibitors and CAR-T cell therapies do not directly target cancer cells; instead, they work by activating or changing the immune system’s response. Their unique mechanisms of action avoid some of the common side-effects of chemotherapy, but they also create new problems. Adverse events related to the immune system, including colitis, hepatitis, pneumonitis, and endocrinopathies, can manifest with considerable severity, unpredictability, and, in certain cases, may be fatal. 24 Cytokine release syndrome (CRS) and neurotoxicity in cellular therapies show how immune modulation can quickly move patients out of the TW. 25 To effectively manage these toxicities, new ways of monitoring, quick use of immunosuppressive therapies, and access to helpful drugs such as tocilizumab are all needed. 26 As a result, the TW in immunotherapy is less about raising the dosage and more about finding the right balance between activating the immune system enough to kill tumors and keeping it from attacking healthy tissues. 27
There are still efforts going on in many areas to extend this short time frame. Pharmacogenomic testing and biomarker-guided dosing are intended to customize therapeutic interventions by aligning medication selection and dosage with the patient’s unique biological traits. 28 Drug delivery systems, such as liposomal formulations, nanoparticles, and antibody–drug conjugates (ADCs), are meant to increase the amount of cytotoxic agents that build up in tumor tissues while reducing the amount that healthy tissues are exposed to. 29 Supportive interventions, such as growth factors, organ-protectants, and anti-inflammatory agents, are designed to lower dose-limiting toxicities while maintaining the treatment’s intensity. Recently, artificial intelligence (AI) and machine learning have been used to predict the best ways to dose medications. These methods use patient data, tumor genomics, and real-world results to make models that find the best and safest treatment windows for each patient. These innovations collectively exemplify the ongoing quest for solutions, while concurrently underscoring the complex nature of the issue at hand. 30
Ultimately, the challenge of the TW in oncology includes not only technical issues but also moral and human issues. Oncologists and patients face decisions that weigh the prospective advantages of tumor management against the risks linked to treatment-induced adverse effects. Intensive treatment approaches can extend survival, although they frequently lead to a diminished quality of life. 31 On the contrary, more conservative treatment plans may make you more comfortable but also put you at risk of the disease getting worse. The acceptable TW for each person depends on his or her preferences, goals for care, and willingness to take risks. Regulatory authorities and clinical guidelines strive to create evidence-based frameworks; however, in practice, the boundaries of the TW are often established through negotiation at the bedside between the physician and patient, shaped by both values and empirical data. 32
The TW is a way of thinking about things in both scientific and clinical settings. It shows the main problem in oncology: the need to eliminate cancerous cells while keeping the patient’s overall health. 33 Even though there have been significant improvements in the last few decades, the TW is still small for most treatments. This restriction shows how complicated the interactions are between cancerous and normal tissues, how complex the TME is, and how different each person’s response is. 34 Targeted therapies, immunotherapies, and advanced drug delivery systems are beginning to change the limits of this window, creating both new chances and problems. However, the goal is still not met. For progress to happen in the future, molecular precision, systems biology, AI, and a focus on patient-centered care will all need to keep coming together. 35 Only through these all-encompassing methods can oncology hope to turn the TW from a limiting barrier into a helpful opportunity. This will make sure that cancer treatment reaches its full potential with the least amount of negative side-effects. 36
Defining the TW: Concepts and Clinical Implications
The term “TW” is very important in pharmacology and clinical medicine. It is one of the most useful and important ideas in drug development and clinical practice. The TW is the range of drug doses that can cause the desired therapeutic effect without causing too much toxicity. 37 In short, it is the safe and effective space that doctors and nurses must work in. Drugs with a wide TW let you change the dose and have a low risk of serious side-effects, even if you make a small mistake when giving them. 38 On the contrary, medications with a narrow TW require precise dosing, careful monitoring, and tailored adjustments, as even minor deviations can result in significant toxicity or therapeutic failure. It is especially clear in oncology how hard it is to work with limited TWs, but the idea works for all areas of pharmacology. 39
The therapeutic index (TI) is a common way to measure the TW from a pharmacological point of view. It is the ratio of the dose that causes toxicity in 50% of subjects (TD50) to the dose that causes a desired therapeutic effect in 50% of subjects (ED50). 40 A low TI means that the window is narrow, while a high index means that the safety margin is wide. However, this numerical definition has problems when used in real-life clinical settings. Not all patients exhibit toxicity at the same dosage, nor is the response invariably binary. 41 The effective and toxic dose curves for numerous medications, particularly oncology drugs (Fig. 1), exhibit considerable overlap, indicating that certain patients may experience severe side-effects at dosages that are ineffective for others. Because of this overlap, the practical TW is a moving target that is more affected by how each patient reacts than by the average for the whole group. 42
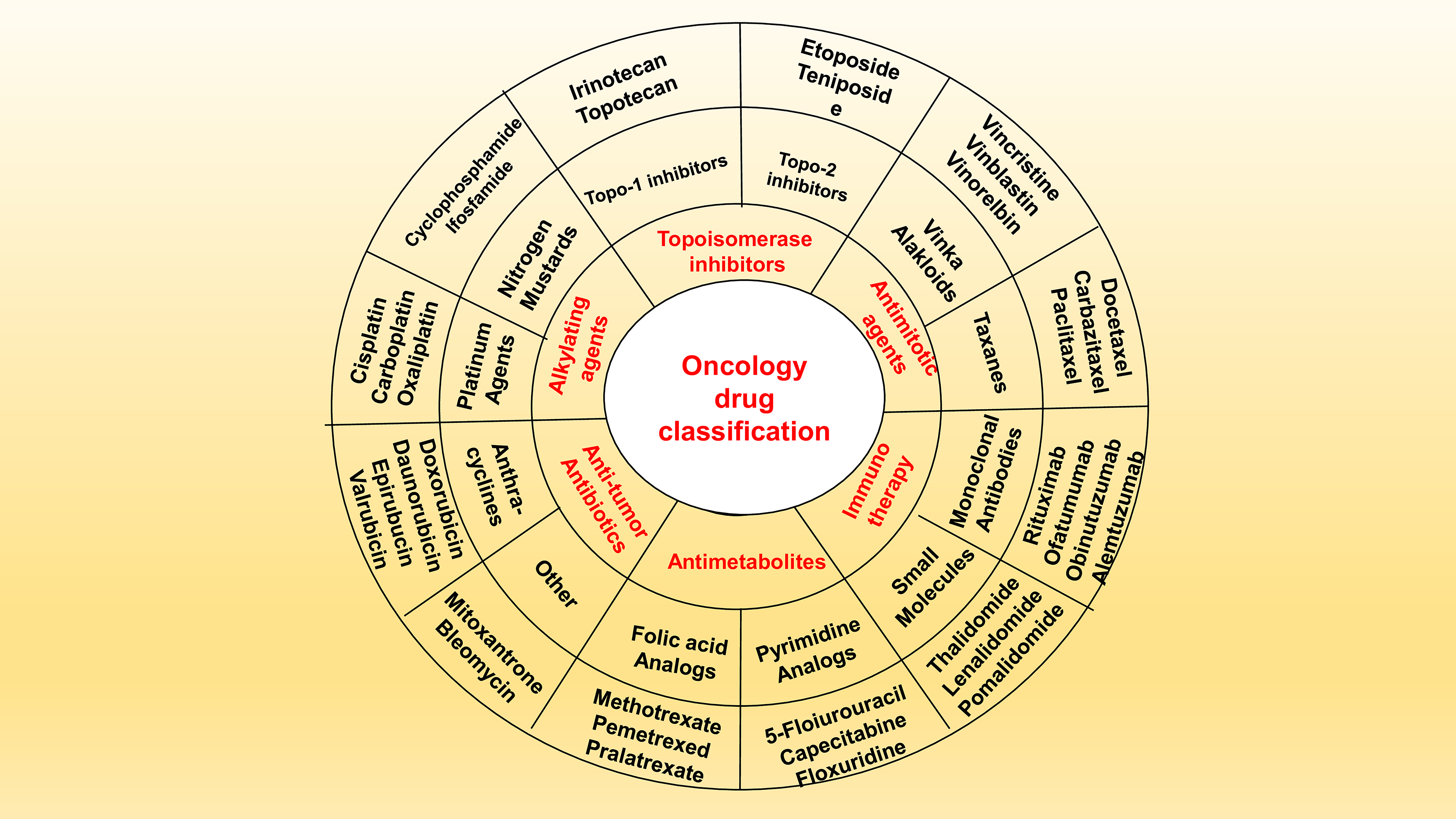
Classification of oncology pharmaceuticals according to their mode of action: The figure shows the most important types of drugs used to treat diseases, such as alkylating agents, antitumor antibiotics, topoisomerase inhibitors, antimitotic agents, antimetabolites, and immunotherapy. For each category, there are examples of drug classes and drugs that show the range of pharmacological strategies used in modern oncology to improve efficacy and safety profiles.
Also, the TW should be thought of as a changing idea rather than a fixed property of a drug. The location of the window for each patient is contingent upon various factors. Pharmacokinetics (PK), which includes absorption, distribution, metabolism, and excretion, determines how much of a drug is in the systemic circulation and target tissues. 43 Pharmacodynamics (PD) shows how a drug interacts with its molecular targets and determines how strong and long-lasting both therapeutic and toxic effects are. Genetic polymorphisms that affect transporters, metabolizing enzymes, or drug targets can change the window by changing how sensitive or tolerant a person. 44 Environmental factors such as diet, concurrent medications, comorbidities, and organ function introduce further variability. Consequently, the TW is an emergent characteristic arising from the complex interplay among the drug, patient, and disease, rather than merely a trait of the drug itself. 45
This complexity has important effects on clinical practice. In their daily work, clinicians have to adjust therapy for each patient, often using surrogate indicators of efficacy or toxicity to aid them make decisions. For drugs with wide TWs, such as most antibiotics or painkillers, dosing can be standardized because most patients will be safely within the effective range. 46 Individualized monitoring is essential for medications with narrow TWs, such as digoxin, lithium, warfarin, certain antiepileptics, and nearly all anticancer agents. Pharmacogenomic testing, therapeutic drug monitoring (TDM), laboratory assays, and clinical observation are used to keep the patient in the right corridor. In oncology, this usually means keeping a close eye on organ function, blood counts, and side-effects, and changing the dose as needed to keep the treatment level high without going over the safety limit. 47
The discovery of the TW changed the way doctors worked in the past. Because early drugs were often given without a clear understanding of how dose–response relationships worked, it was common for people to take too much or too little. The development of dose–response curves and the concept of a TI in the early 20th century made it possible to use drugs in a more logical way. 48 Clinicians found that every drug can be both a poison and a cure, depending on the dose. They also found that knowing where the line is between toxicity and efficacy is important for safe treatment. This understanding has shaped modern regulatory frameworks, which now require clinical and preclinical data to establish the therapeutic range before granting approval (Table 2).
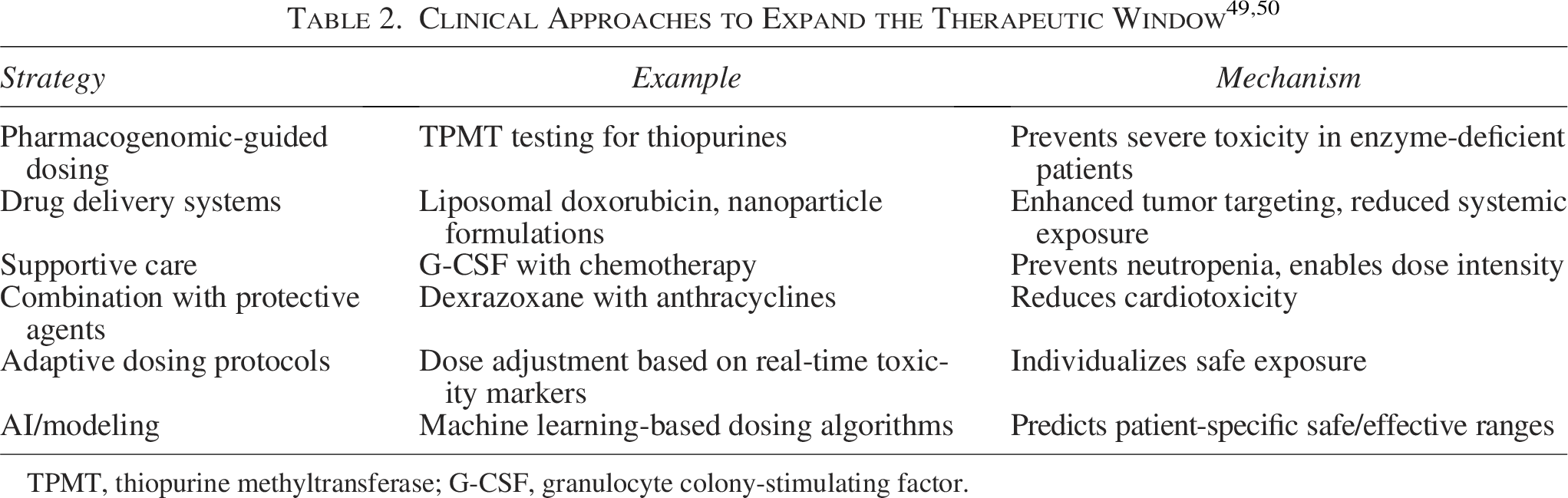
TPMT, thiopurine methyltransferase; G-CSF, granulocyte colony-stimulating factor.
Dose-finding studies, especially Phase I and II trials, are meant to find the edges of the TW. They often find the minimum effective dose and maximum tolerated dose (MTD) to use as starting points for further clinical development. 51
Because cancer can kill you and the treatments are harsh, the TW is especially important. If higher intensity means killing more tumors, then the MTD has been used for a long time as a stand-in for the best dose. The emergence of targeted therapies and immunotherapies, which may achieve efficacy at doses significantly lower than those inducing toxicity, has challenged this assumption. 52 In these cases, the TW is based on the smallest dose needed to saturate the target and have a biological effect, not the highest dose of toxicity that can be tolerated. This change highlights the need for a nuanced understanding of the TW that goes beyond simple thresholds or ratios.
Another important clinical implication is that the TW changes over time during treatment. The patient’s physiology alters during treatment; resistance may modify tumor biology, comorbidities may emerge, or organ function may decline. Over time, the window may get smaller because of cumulative toxicity, such as neuropathy caused by platinum or cardiomyopathy caused by anthracycline. 53 Adaptive changes to TMEs, such as hypoxia or stromal remodeling, may also raise the threshold for efficacy by making it harder for drugs to get through. Because a dose that is okay in the first cycle may not be okay in later cycles, and because the initial efficacy may go down even with stable dosing, doctors must always reevaluate and change treatment. 54
The TW also has more significant effects on patient-centered care. Toxicity and efficacy are both experiences that patients have, not just biological events. The meaning of “unacceptable” toxicity changes based on the situation, the patient’s values, and the patient’s goals. One patient might not be able to handle mild nausea, while another might be able to handle extreme exhaustion if it means living longer. 55 The patient’s risk tolerance, treatment goals, and quality of life all play a role in determining the practical TW. This understanding has sped up the use of patient-reported outcomes in clinical trials and practice, making sure that TWs are based on both laboratory values and how well patients can handle them in the real world. 56
Advances in precision medicine and drug delivery are actively broadening TWs. Nanoparticle formulations, liposomes, and ADCs can shift the toxicity curve away from the efficacy curve by concentrating active drugs in tumors and leaving healthy tissues alone. Pharmacogenomics enables preventive dose adjustments that ensure safety without sacrificing efficacy by predicting which patients may experience toxicity at standard doses. 57 AI models that use clinical, pharmacological, and genomic data have the potential to personalize the TW with a level of accuracy that has never been seen before. These advancements illustrate that, despite persistent challenges, the TW represents a domain of clinical pharmacology innovation. 58
The effects on society and rules are just as important. A drug with a very narrow TW needs a lot of infrastructure and monitoring, which makes it more expensive and harder to get in places with few resources. Conversely, medications with wider windows can be safely utilized in primary care or outpatient environments, enhancing their accessibility. When looking into new treatments, policymakers, payers, and health care systems need to keep these things in mind. They need to know that a drug’s practical usefulness depends on how well it works and how easy it is to manage its TW. 59
The TW is one of the most basic and useful ideas in pharmacology. It sets the fine line between toxicity and efficacy, which affects drug development, regulatory approval, clinical practice, and the patient experience. The TI can be expressed as a number, but its true nature is contextual, personalized, and dynamic. This is especially true in oncology, where the difference between toxic and effective doses is very small and making a mistake could be deadly. 60 The TW, on the contrary, controls the safe and effective use of many drugs, not just those used in cancer treatment. It is still very important for all medical professionals to understand the theory behind it and how it works in practice. As medicine becomes more personalized, the TW will be based more on the unique interaction between biology, disease, and patient preference than on population averages. So, the future of therapeutics could be seen as the future of the TW: making it more significant, more personalized, and eventually changing it from a barrier to an opportunity for truly safe and effective care. 61
The concept of enhancing the TW presents an intriguing prospect. Its novelty and practical significance are more readily apparent when considering how particular approaches directly augment the TI, which represents the equilibrium between a treatment’s efficacy and its adverse effects. A comprehensive elucidation of the underlying mechanisms not only fortifies the scientific foundation but also establishes a connection with precision oncology. 62
Receptor-mediated targeting and selective drug accumulation
A well-known way to improve the TW is through receptor-mediated targeting. This involves using drug delivery systems that are modified with ligands, such as antibodies, peptides, or aptamers. These ligands are designed to bind specifically to receptors that are more common on tumor cells, such as HER2, epidermal growth factor receptor (EGFR), or folate receptors. 63
Mechanistically, this strategy enhances the TI through several key mechanisms:
By elevating the local drug concentration at the tumor site, PD efficacy is amplified. Off-target exposure within healthy tissues is diminished, thus mitigating systemic toxicity. Receptor-mediated endocytosis is facilitated, which in turn improves intracellular drug delivery and retention.
As an illustration, ADCs leverage highly specific antigen recognition to deliver cytotoxic payloads directly into cancer cells. This spatial selectivity alters the dose–response curve, enabling effective tumor cell killing at doses that would otherwise be toxic if administered systemically.
TME modulation
The TME, distinguished by hypoxia, an acidic pH, aberrant blood vessel formation, and immunosuppressive signaling, significantly impedes the effectiveness of treatments. Interventions designed to alter the TME can substantially broaden the TW by enhancing both drug availability and the degree of response. 64
Essential mechanisms encompass the following:
pH-sensitive systems that leverage the acidic nature of tumor environments to initiate localized drug release. Hypoxia-activated prodrugs, which are rendered cytotoxic exclusively in low-oxygen settings, thereby protecting healthy tissues that are well-oxygenated. Normalization of tumor vasculature (e.g., via antiangiogenic agents), improving drug penetration and reducing interstitial pressure. Immune modulation (e.g., checkpoint inhibitors) that reactivates antitumor immunity without increasing systemic cytotoxic burden.
By selectively enhancing drug activity within the tumor niche while maintaining minimal activity in normal tissues, TME-targeted approaches effectively widen the TI.
Nanoparticle-triggered and stimulus-responsive drug release
Nanomedicine introduces a powerful platform for spatiotemporally controlled drug delivery, which is central to TW enhancement. Nanoparticles can be engineered to release drugs in response to internal (pH, enzymes, redox gradients) or external (light, heat, magnetic field, ultrasound) stimuli. 65
Mechanistically, this process facilitates the expansion of TI through several key mechanisms. These include controlled release kinetics, which mitigate premature drug leakage and consequently diminish systemic toxicity. Furthermore, the enhanced permeability and retention (EPR) effect allows for preferential accumulation within tumor tissues, a result of the leaky vasculature characteristic of such environments. On-demand drug activation is another critical factor, ensuring that cytotoxic agents are released precisely at the intended site and time.
As an illustration, thermosensitive liposomes are designed to release their therapeutic payload upon exposure to mild hyperthermia, thereby enabling localized chemotherapy while minimizing systemic exposure. Similarly, enzyme-responsive nanoparticles can degrade specifically within tumor-associated environments, thereby ensuring precision in drug delivery. 66
AI-Integrated Nanomedicine and Multiomics-Guided Adaptive Therapy
To enhance the article’s impact and underscore its originality, it is crucial to move beyond a mere recitation of established methodologies and instead highlight novel integrative paradigms, specifically AI-integrated nanomedicine and multiomics-guided adaptive therapy. These represent the forefront of precision oncology, where data-driven intelligence is combined with advanced therapeutic platforms to actively broaden the TW and improve clinical outcomes.
AI’s integration into nanomedicine
AI’s integration into nanomedicine represents a significant departure from traditional, passive, or preprogrammed drug delivery systems, moving toward adaptive and intelligent platforms. Traditional nanocarriers are typically designed based on static parameters; however, AI facilitates dynamic optimization throughout various stages of drug development and delivery. 67
Mechanistic contributions
Design optimization is facilitated by machine learning algorithms, which can forecast the ideal nanoparticle size, surface charge, ligand density, and composition to enhance tumor targeting while mitigating systemic toxicity. Patient-specific targeting is achievable through AI models, which, when trained on clinical and molecular datasets, can pinpoint patient-specific biomarkers, thereby enabling the creation of personalized nanocarriers designed to address tumor heterogeneity. 68 Furthermore, real-time treatment adaptation is possible through the integration of imaging and biosensing technologies, allowing AI systems to monitor drug distribution and therapeutic response, thus enabling feedback-controlled drug release. Predictive toxicology is another area where AI proves valuable, as it can forecast nanoparticle biodistribution and potential adverse effects, consequently reducing the need for trial-and-error experimentation and improving safety profiles.
Impact on TI
AI-integrated nanomedicine enhances the TW by simultaneously increasing precision in drug delivery, which in turn elevates efficacy. Minimizing off-target accumulation and toxicity is crucial for reducing adverse effects.
Novelty contribution
This article distinguishes itself by proposing a closed-loop therapeutic system. In this system, AI not only aids in nanoparticle design but also continuously refines treatment based on patient responses. This approach surpasses current static nanomedicine strategies. 69
Multiomics-guided adaptive therapy: Dynamic personalization of treatment
While genomics has long been used to inform targeted therapies, the integration of multiomics data—including genomics, transcriptomics, proteomics, metabolomics, and epigenomics—enables a comprehensive understanding of tumor biology. Furthermore, when combined with adaptive therapy principles, this approach allows for the continuous modification of treatment strategies in response to tumor evolution.
Mechanistic contributions
Comprehensive tumor profiling, facilitated by multiomics data, elucidates not only genetic mutations but also functional protein expression, metabolic pathways, and epigenetic modifications that drive disease progression. Furthermore, biomarker discovery enables the identification of dynamic indicators that predict drug response, resistance, and toxicity. Adaptive dosing strategies allow for real-time adjustments to treatment regimens, informed by longitudinal omics data, thereby preventing resistance and maintaining tumor control. Conversely, network-level targeting, rather than concentrating on isolated pathways, permits therapies to target interconnected signaling networks, thus mitigating compensatory resistance mechanisms. 70
Impact on TI
Consequently, enhanced efficacy is achieved through precise pathway targeting and resistance mitigation. The reduction in toxicity was achieved by avoiding treatments that were either ineffective or not needed.
Novelty contribution
The authors can emphasize a feedback-driven therapeutic model. This model uses multiomics data to continuously adjust treatments, changing therapy from a fixed protocol to a dynamic, evolving strategy. 71
Synergistic integration: AI + multiomics + nanomedicine
The most significant advancement comes from combining these technologies, creating a highly sophisticated and personalized therapeutic system. 72
Proposed integrative framework
Data acquisition: Multiomics profiling generates complex patient data.
AI analysis: Machine learning algorithms process and analyze these datasets to pinpoint ideal therapeutic targets and forecast patient responses.
Nanomedicine implementation: AI-generated nanocarriers facilitate drug delivery with both spatial and temporal accuracy.
Feedback loop: The system is continuously refined through the reintegration of real-time clinical and molecular data.
Transformative potential: The development of patient-specific “digital twins” for simulation-driven therapy optimization. The creation of self-regulating drug delivery systems capable of autonomous dose adjustment. The realization of true precision oncology, in which treatment strategies adapt in concert with tumor evolution.
Mechanisms of Toxicity in Cancer Therapy
Cancer treatment can save lives, but it can also have bad side-effects that come from both on-target and off-target processes. In oncology, the TW is frequently constrained by the inadequacy of numerous cancer treatments to completely distinguish between malignant and healthy rapidly proliferating cells. Toxicity is not only an undesirable side-effect but also an inherent aspect of the pharmacological activity of most anticancer medications. 62 To improve treatment, make medicines that are safer, and improve the quality of life for people who are getting treatment, it is important to understand the main causes of toxicity (Table 3).
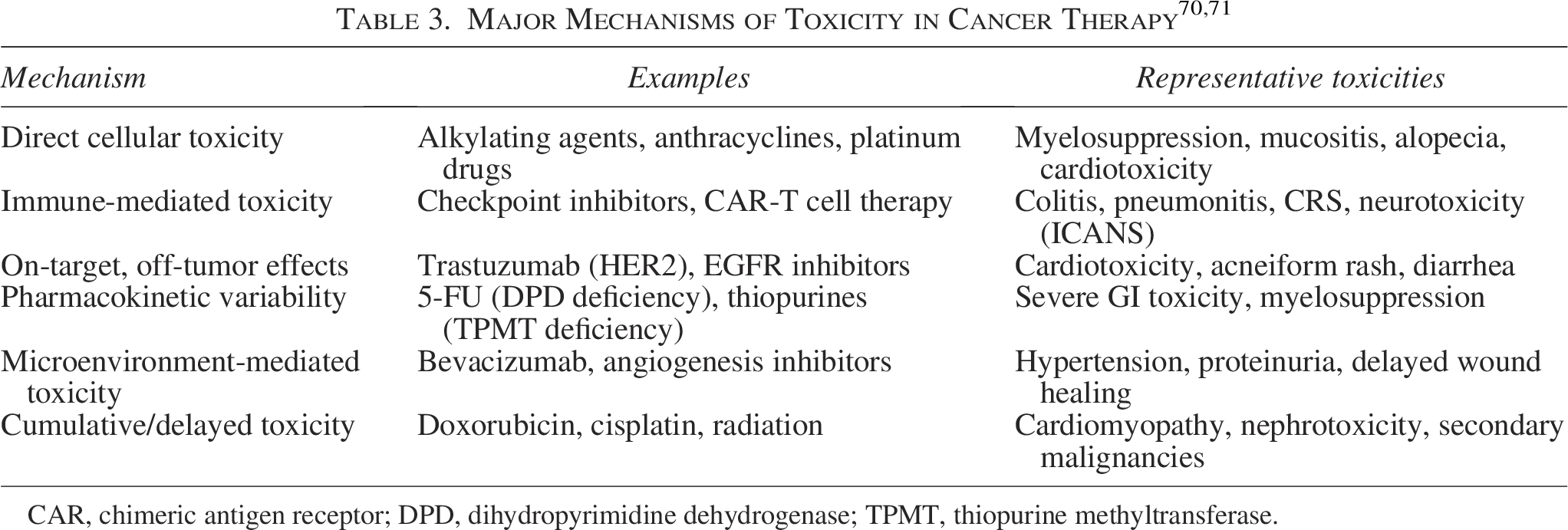
CAR, chimeric antigen receptor; DPD, dihydropyrimidine dehydrogenase; TPMT, thiopurine methyltransferase.
Direct cellular toxicity
A principal mechanism of toxicity in cancer therapy is the direct annihilation of healthy cells that share biochemical characteristics with tumor cells. Alkylating agents, platinum compounds, and antimetabolites are examples of traditional cytotoxic drugs that only affect DNA synthesis, replication, and repair. 63 Tumor cells divide quickly, and so do other normal tissues, such as bone marrow, the lining of the stomach and intestines, and hair follicles. This makes them more likely to get sick. This leads to expected side-effects such as myelosuppression, mucositis, and hair loss, which are known as “class effects” of some chemotherapies. 64
Drugs that damage DNA, such as doxorubicin and cisplatin, make reactive oxygen species and free radicals. These cause problems with the mitochondria and lipid peroxidation, which can lead to long-term toxicities such as cardiotoxicity and nephrotoxicity (Fig. 2). Cumulatively, some toxicities are significant, showing a level of organ damage that becomes clinically apparent after several rounds. 65
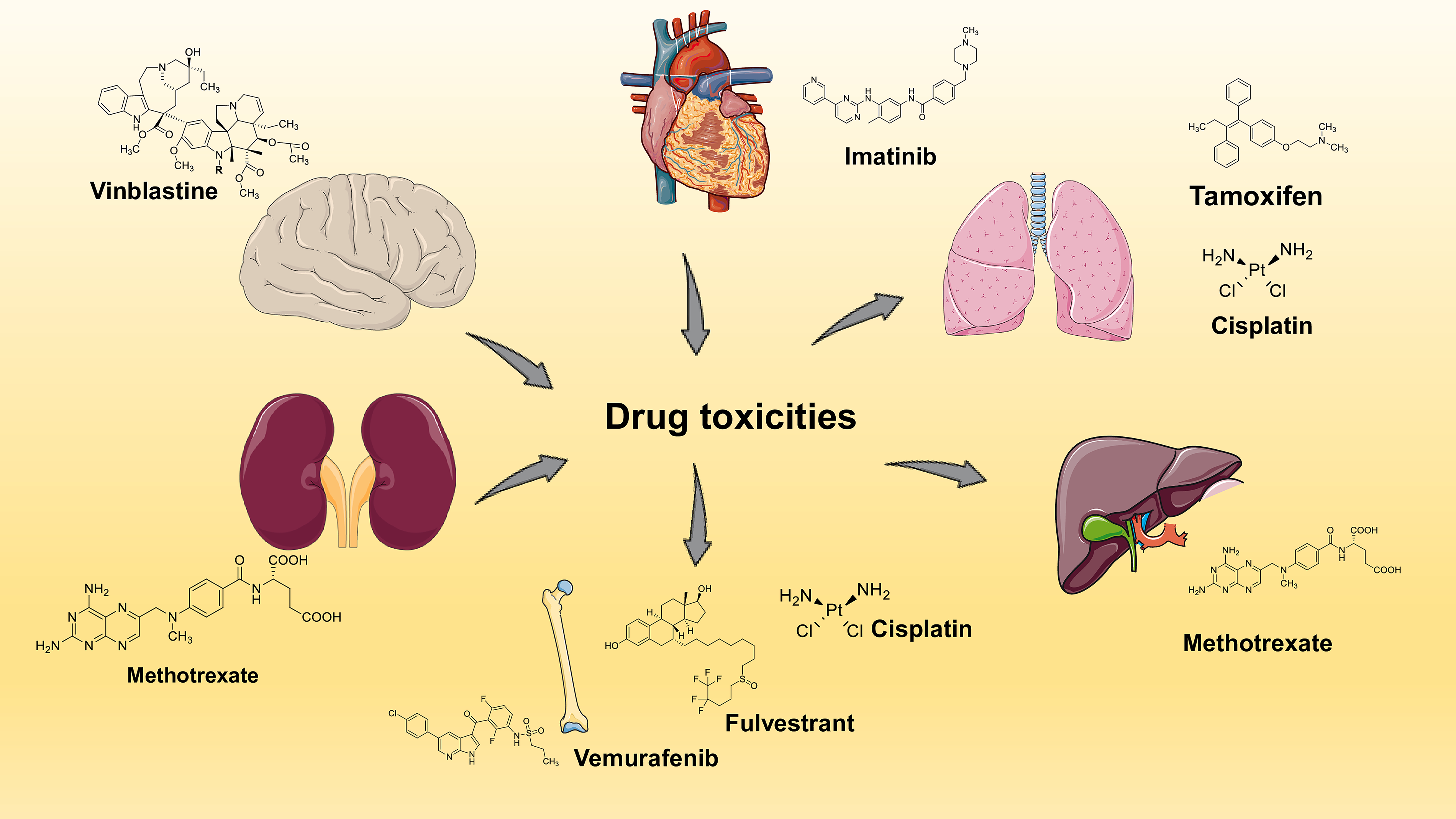
Illustration of drug toxicities associated with oncology therapeutics: The figure shows the most important organ-specific toxicities and lists some common anticancer drugs and their chemical structures that can cause problems in the brain (vinblastine), heart (imatinib), lungs (tamoxifen, cisplatin), liver (methotrexate), kidneys (methotrexate), and bones (vemurafenib, fulvestrant, cisplatin). This diagram shows how important it is to find a balance between effectiveness and safety when trying to widen the therapeutic window in modern cancer treatment.
Immune-mediated toxicity
The advent of immunotherapies, such as checkpoint inhibitors and CAR-T cell therapy, has made immune-related adverse events (irAEs) a major concern. 66 These toxicities occur due to hyperactivation of the immune system, causing damage to autologous tissues. Checkpoint blockade (anti-CTLA-4, anti-PD-1/PD-L1 antibodies) removes inhibitory signals from T cells, boosting antitumor immunity but also causing autoimmune-like diseases such as colitis, dermatitis, thyroiditis, pneumonitis, and hepatitis. 67
CAR-T cell treatments cause CRS, which is characterized by an increase in interleukins and interferons that leads to fever, low blood pressure, and failure of multiple organs. 68 Neurotoxicity (ICANS) is a distinct immune-mediated mechanism marked by endothelial dysfunction, compromise of the blood–brain barrier, and cytokine infiltration, culminating in encephalopathy and seizures. These immunological toxicities are frequently unforeseen, display varying levels of severity, and may necessitate high-dose corticosteroids or cytokine inhibitors such as tocilizumab for management. 69
Target-mediated toxicity (on-target, off-tumor)
Targeted medications, such as TKIs and monoclonal antibodies, are designed for specificity; however, toxicities can occur due to the expression of therapeutic targets in normal tissues. HER2 is overexpressed in breast and gastric cancers, and it is also found in cardiac tissue, which explains the cardiotoxicity linked to trastuzumab. EGFR inhibitors (erlotinib, cetuximab) also mess up signaling in the skin and intestines, which can cause acneiform rash and diarrhea. 72
On-target, off-tumor effects are particularly relevant in solid tumors where molecular targets are not exclusively tumor specific. These toxicities highlight the molecular interplay between cancer and normal physiology, underscoring that “precision” treatment is relative rather than absolute. 73
Pharmacokinetically induced toxicity
The onset of toxicity is affected by the PK of drugs, including absorption, distribution, metabolism, and excretion. There are differences in toxicity profiles because of significant differences in how different patients metabolize medications. 74 Patients exhibiting reduced dihydropyrimidine dehydrogenase (DPD) activity cannot metabolize 5-fluorouracil effectively, leading to severe and potentially fatal toxicity. Polymorphisms in TPMT likewise enhance vulnerability to thiopurine medication toxicity. 75
Hepatic and renal dysfunction exacerbates drug clearance, leading to dose-dependent accumulation and increased toxicity. Drug–drug interactions, such as those between azole antifungals and TKIs, can make the body more exposed to drugs. Pharmacogenomic screening and therapeutic medication monitoring are necessary tools for predicting and mitigating PK-induced toxicity. 76
Microenvironment-induced toxicity
The TME not only fosters resistance but also influences toxicity. Drugs that stop angiogenesis, such as bevacizumab and vascular endothelial growth factor (VEGF) inhibitors, throw off the balance of the blood vessels, which can cause high blood pressure, proteinuria, and slow wound healing. Normal endothelial cells, pericytes, and stromal fibroblasts share pathways with their malignant counterparts, which explains why toxicities happen in healthy tissues. Hypoxia in tumors may alter drug metabolism, leading to the production of toxic metabolites that damage the surrounding healthy cells. 77
Cumulative and delayed toxicity
Several toxicities emerge months to years after treatment, in contrast to immediate adverse effects. Anthracyclines, such as doxorubicin, induce delayed cardiomyopathy through mitochondrial DNA damage and prolonged oxidative stress. Platinum compounds can cause cumulative nephrotoxicity and neurotoxicity by cross-linking DNA in neurons and renal tubular cells that are not replicating. Radiation therapy also leads to more cancers decades later. 78
Delayed toxicities show that cancer treatment has long-lasting effects on the body, which shows how important it is to keep an eye on the survivors and take steps to prevent problems. 49
There are many ways that cancer treatment can be toxic, such as direct cytotoxic effects, problems with the immune system, differences in how drugs work in different people, and changes in the environment around the tumor. They may occur suddenly or with a delay, frequently overlapping with the processes of treatment efficacy. 79 A mechanistic understanding clarifies detrimental effects and informs preventive strategies, dosage adjustments, and the formulation of safer therapies. To widen the TW for cancer patients, future oncology practice must use pharmacogenomics, advanced drug delivery systems, and AI-driven prediction models to lower toxicity while keeping antitumor activity. 80
Strategies to Enhance Efficacy While Minimizing Toxicity
The TW in oncology remains one of the most significant constraints in clinical practice. The goal of cancer treatment is to eliminate cancer cells, but chemotherapy often hurts healthy tissues a lot. 81 People have come up with different ways over time to make this treatment window longer by boosting its antitumor activity and cutting down on side-effects. These strategies encompass pharmacological innovation, medication delivery systems, personalized medicine, supportive care, and the incorporation of cutting-edge technology. 82 Together, they show a shift in oncology from strategies that only focus on tumors to precision medicine that focuses on the patient (Table 3).
Enhancement of pharmaceutical delivery mechanisms
One of the best ways to lower toxicity is to improve drug delivery systems that make it easier to target tumors and limit systemic exposure. 83 Liposomal formulations, such as pegylated liposomal doxorubicin, encapsulate drugs within nanocarriers, altering their PK and reducing cardiotoxicity compared with conventional doxorubicin. Similarly, albumin-conjugated nanoparticle paclitaxel improves solubility and tumor targeting without the use of toxic solvents. 84
It is important to explicitly connect each modality—ADCs, nanocarriers, and prodrugs—to quantifiable and mechanistic improvements in the TW. Rather than describing these platforms broadly, the discussion should articulate how they shift the balance between efficacy (tumor kill) and toxicity (off-target damage) through measurable PK, PD, and biodistribution changes. 85
ADCs: Precision targeting and intracellular drug release
ADCs are composed of a monoclonal antibody linked to a potent cytotoxic payload via a cleavable or noncleavable linker. Their ability to enhance the TW is rooted in target specificity and controlled intracellular release.
Mechanistic basis
Antigen-specific binding: ADCs selectively bind to tumor-associated antigens (e.g., HER2, CD30), leading to preferential accumulation in malignant cells.
Receptor-mediated endocytosis: Following binding, the ADC–antigen complex is internalized, allowing intracellular trafficking to lysosomes. Linker cleavage and the subsequent payload release, facilitated by enzymatic degradation or pH-sensitive cleavage, ensure that the active drug is specifically released within tumor cells. 86
Quantitative improvements
ADCs demonstrate a significantly increased tumor-to-plasma drug ratio, often several fold higher than that of free drugs, contingent upon antigen expression levels. Furthermore, systemic exposure is reduced, as evidenced by a decrease in the area under the curve (AUC), because the cytotoxic payload remains largely inactive while circulating, thereby mitigating systemic toxicity. Consequently, the MTD is elevated; this is attributable to the reduced off-target toxicity, which permits the administration of highly potent drugs that would otherwise be intolerable. 87
Impact on TW
The TW is positively affected, specifically by increasing effectiveness, which is achieved through better delivery of strong cytotoxins inside cells. Reduced toxicity is observed with minimal exposure of healthy tissues that do not express the target antigen. Consequently, ADCs improve the TI by enhancing tumor selectivity and limiting systemic drug distribution.
Nanocarriers: Improved tumor accumulation and controlled PK
Nanocarriers, including liposomes, polymeric nanoparticles, and dendrimers, enhance the TW primarily by altering biodistribution and controlling drug release kinetics.
Mechanistic basis
The EPR effect, which is a result of the leaky nature of tumor blood vessels with holes ranging 100–800 nm, allows nanoparticles to build up in the tumor tissue. In addition, reduced kidney clearance aids nanoparticles avoid being filtered out quickly, thus extending their time in the bloodstream. Surface modifications, achieved through PEGylation or attaching ligands, improve both stability and targeting. Moreover, controlled release profiles can be created, allowing for sustained, delayed, or stimulus-triggered drug release, depending on factors such as pH, enzyme activity, or temperature. 88
Quantitative enhancements
Nanocarriers exhibit the ability to substantially prolong the half-life (t½) of therapeutic compounds, thereby extending their circulation duration from the brief periods characteristic of free drugs, which are measured in minutes, to several hours or, in some instances, days.
Higher AUC at the tumor site results in prolonged drug exposure within the tumor. A diminished peak plasma concentration (Cmax) correlates with reduced systemic toxicity, as it eliminates abrupt concentration surges. Tumor accumulation efficiency is frequently observed to be 2–10 times greater than that of the free drug, contingent upon the formulation and the specific tumor model used. 89
Spatiotemporal control is achieved through spatial and temporal mechanisms. Spatial control is facilitated by preferential accumulation at the tumor site, which can be mediated by EPR effects or active targeting strategies. Temporal control is established through sustained or stimuli-responsive release profiles, thereby ensuring drug availability over an extended duration or in response to specific triggers.
Impact on TW
Efficacy is improved due to prolonged and enhanced tumor exposure. Toxicity is decreased because of lower systemic exposure and reduced off-target accumulation. Therefore, nanocarriers expand the TW by changing PK parameters and enabling drug delivery to specific sites.
Prodrugs: Selective activation and reduced systemic toxicity
Prodrugs are inactive or less active forms that become active drugs through biotransformation, which occurs in specific physiological or pathological conditions. 90
Mechanistic basis
Prodrugs are activated by enzymes that are overexpressed in tumors, such as esterases and proteases. Furthermore, drug release is triggered by the acidic environments found in tumors. Activation also occurs in response to hypoxia, a condition commonly seen in solid tumors.
Quantitative improvements
The inactive prodrug form circulates with minimal toxicity, leading to reduced systemic bioactivity. In addition, drug activation is localized, resulting in a higher effective concentration at the tumor site compared with the plasma. Improved TI is achieved by diminishing the impact of the toxic dose (TD50) while preserving or augmenting the effective dose (ED50). Spatiotemporal advantages are realized through spatial selectivity, which restricts activation to the TME, and temporal control, in which the drug’s activation is contingent upon its arrival at the target site, thereby mitigating premature toxicity. 91
Impact on TW
The TW is positively impacted by an increase in efficacy, characterized by a high local drug concentration following activation, and a decrease in toxicity, which is reflected in minimal systemic exposure to the active drug. Consequently, prodrugs improve the TW by dissociating systemic distribution from pharmacological activity.
ADCs are a significant step forward because they link cytotoxic drugs to monoclonal antibodies that only attack proteins that are linked to tumors. 85 ADCs, for instance, demonstrate antigen-specific distribution and intracellular drug release; nanocarriers enhance systemic circulation and increase tumor accumulation through the EPR effect; and prodrugs remain inactive during systemic circulation, experiencing selective activation within the TME. These changes to PK should then be directly linked to PD results, such as increased tumor cytotoxicity, decreased off-target toxicity, longer drug exposure, and control of drug activation in time and space. A comparative visualization, such as plasma concentration–time curves and dose–response relationships, can further clarify diminished peak plasma levels (Cmax), an elevated tumor-specific AUC, and a distinct separation between efficacy and toxicity curves (ED50 vs. TD50), ultimately illustrating TI expansion. 92 Adding such a figure not only makes it easier to compare the benefits of each platform, but it also supports the main point that improving the TW is done by carefully changing the PK/PD relationships through spatial targeting and controlling when the drug is released, which greatly improves both efficacy and safety.
Brentuximab vedotin (anti-CD30) and trastuzumab emtansine (anti-HER2) are two drugs that work better and cause less damage to healthy tissue. These improvements show how better delivery methods can make treatments more effective while causing less damage to the surrounding tissues. 86
Tailored medicine and pharmacogenomics
Pharmacogenomic profiling has transformed the ability to predict individual patient risks of toxicity. Testing for DPD deficiency lowers the risk of serious side-effects from fluoropyrimidines, and TPMT and NUDT15 genotyping aids with thiopurine therapy. Polymorphisms in CYP2D6 also change how tamoxifen is broken down, while mutations in EGFR or ALK predict how well targeted treatments will work. 87 By classifying patients according to genetic predisposition, physicians can tailor pharmacotherapy and dosage to maximize efficacy while reducing adverse effects.
Tumor-specific indicators, in addition to germ line genetics, aid choose the best treatment. PD-L1 expression, mismatch repair deficiency, and tumor mutational load function as predictive biomarkers that guide the application of ICIs. 88 This biomarker-driven customization reduces the risk of being exposed to ineffective and potentially harmful treatments.
Supportive care and toxicity mitigation
Even with better regimens, supportive care is still very important for keeping the treatment effective and reducing harm. Hematopoietic growth factors, such as granulocyte colony-stimulating factor, enable dose-intensive chemotherapy by alleviating neutropenic effects. 89 Antiemetics, including 5-HT3 antagonists and NK1 receptor antagonists, significantly improve the tolerance of highly emetogenic treatment regimens.
Medicines that protect organs have been made such as dexrazoxane to reduce the heart damage caused by anthracyclines, mesna to stop bleeding cystitis from ifosfamide, and amifostine to protect against cisplatin nephrotoxicity and radiation damage. 90 Nutritional support, pain management, and psychological interventions all bolster the patient’s resilience to treatment. Supportive care is not just for easing symptoms; it also aids in keeping the intensity of therapy high and improving survival rates. 91
Adaptive dosing and therapeutic drug surveillance
Cancer treatment is very dynamic, and because each patient is different, the dosages need to be flexible. Adaptive dosing uses real-time information about how well a patient is responding and how toxic a drug is to make changes to the dosage, rather than just following set schedules. 92 For example, procedures for increasing or decreasing the dose of targeted medicines aid find the right balance between effectiveness and tolerance. TDM of medications such as methotrexate or busulfan ensures therapeutic levels while mitigating systemic toxicity. 93 AI-powered PK models are being created that use clinical and genetic information from individual patients to predict the best dosage regimens. These adaptive strategies aid avoid giving too much treatment to sensitive patients and too little treatment to resistant tumors, which aids find the best balance between the two. 94
A pertinent illustration involves the application of machine learning-driven predictive oncology models. These models utilize algorithms such as random forests, support vector machines, and deep neural networks, which are trained on extensive clinical and molecular datasets to forecast drug response and toxicity. As an example, multiparameter models that incorporate genomic mutations, transcriptomic signatures, and clinical variables have been used to stratify patients for targeted therapies, such as EGFR inhibitors or immunotherapies. 95 This allows for the identification of responders while simultaneously excluding those at high risk. Consequently, this methodology has demonstrated a reduction in unnecessary drug exposure and its associated toxicities, thereby enhancing the TI by tailoring treatment to the specific biology of each patient.
Furthermore, another significant category involves PK/PD modeling, which is integrated with AI, commonly known as model-informed precision dosing. These models integrate population PK data with individual patient attributes, including age, organ function, and genetic variations, to facilitate real-time predictions of optimal dosing strategies. Such systems have proven effective in oncology and critical care settings, where they have successfully mitigated dose-limiting toxicities while preserving therapeutic effectiveness. 96 For instance, Bayesian adaptive dosing models have been used to modify chemotherapy or antimicrobial dosing, resulting in a decreased frequency of adverse drug reactions and enhanced clinical outcomes. Mechanistically, this approach directly influences parameters such as Cmax and AUC, ensuring they remain within safe and effective limits. Furthermore, the incorporation of multiomics data via network-based systems biology models offers another compelling illustration of this approach.
These models construct networks that show how genes, proteins, and metabolites interact. This aids identify important regulatory points that drive disease progression and drug resistance. Computational methods, such as network pharmacology and pathway enrichment analysis, are used to predict drug combinations that work together by targeting multiple signaling pathways at the same time. 97 This approach reduces compensatory resistance mechanisms, allowing for lower doses of each drug. As a result, toxicity is reduced while maintaining or improving effectiveness. In cancer research, these methods have guided the development of combination therapies that are more effective and less toxic than treatments using a single drug.
In addition, digital twin models, which are virtual copies of individual patients created using long-term clinical and multiomics data, represent a cutting-edge application of AI and systems biology. These computational models facilitate the simulation of disease advancement and therapeutic responses across diverse treatment paradigms, thereby allowing for in silico refinement of treatment approaches before their clinical application. Initial implementations have yielded enhanced predictions regarding tumor growth patterns and treatment results, thereby assisting clinicians in selecting regimens that optimize therapeutic effectiveness while minimizing undesirable side-effects. 98
Furthermore, AI has found utility in the design and optimization of nanomedicine, with deep learning models used to forecast nanoparticle behavior, encompassing biodistribution, cellular uptake, and toxicity profiles. By simulating the impact of alterations in size, surface chemistry, or ligand density on biological interactions, these models facilitate the rational design of nanocarriers characterized by improved tumor targeting and diminished off-target accumulation. 99 This approach directly facilitates the expansion of the TW by enhancing delivery accuracy and reducing systemic exposure.
Moreover, platforms designed for toxicity prediction, which utilize AI such as the QSAR models and deep learning-based toxicogenomics, have been used to early identify potential adverse effects of drug candidates during development. These systems analyze the chemical structure, biological activity, and omics data to predict organ-specific toxicity, thereby allowing for the elimination or modification of high-risk compounds before clinical trials. This not only enhances safety but also diminishes the likelihood of late-stage drug failure. 100
Incorporating these examples into the article transforms the section from a conceptual overview into a discussion grounded in mechanistic understanding and supported by evidence. AI and systems biology methodologies contribute to an expanded TW through several mechanisms. 101 These include the following: improved patient stratification, which enhances efficacy and reduces unnecessary exposure; the optimization of dosing strategies, which ensures PK parameters remain within safe limits; the prediction and prevention of toxicity, thereby decreasing adverse events; the guidance of combination therapies, which increases efficacy while allowing for lower doses; and the facilitation of rational drug and nanocarrier design, which improves targeting precision. By explicitly correlating these computational models with quantifiable PK/PD outcomes and clinical advantages, this article effectively illustrates how data-driven precision medicine approaches are reshaping TW enhancement in contemporary oncology and pharmacotherapy.
Combination therapy and sequencing
When carefully calibrated, combining medicines with complementary modes of action may improve tumor eradication while lowering toxicity. 95 For instance, switching between cytotoxic chemotherapy and targeted inhibitors could lower the total amount of each drug that a person is exposed to. Immunotherapy combined with chemotherapy has demonstrated improved survival rates in lung cancer; however, meticulous monitoring for concurrent toxicities is essential. 96
The sequence of therapy is also important. Giving less toxic targeted treatments before chemotherapy may delay exposure to systemic toxicities, and giving immunotherapy after debulking chemotherapy in a planned order may make immune-related side-effects less severe. 97 Rational combinations and sequencing constitute an advanced strategy for enhancing efficacy while mitigating proportional increases in toxicity. Using the TME for selectivity therapies that exploit the unique attributes of the TME may improve selectivity. 98 Hypoxia-activated prodrugs are inactive in normoxic normal tissues but demonstrate cytotoxicity in the hypoxic tumor milieu. In the same way, pH-sensitive nanoparticles release drugs more easily in the acidic environment of tumors. 99 Targeting angiogenesis is a good example of how VEGF inhibitors work. These drugs only affect the abnormal blood vessels in tumors. However, systemic effects such as high blood pressure are a significant problem. Therapies exploit microenvironmental variations to target tumor-specific vulnerabilities while safeguarding healthy tissues. 100
Mitigating immunotherapy-associated toxicities
Immunotherapy has changed oncology, but irAEs are still a problem. Strategies to mitigate these factors encompass meticulous patient selection utilizing predictive biomarkers, swift identification of subclinical immune activation, and preventive measures for high-risk individuals. 101 Researchers are looking into combination regimens that use lower doses of checkpoint inhibitors with targeted treatments to make them work better while keeping the immune system safe. 102
The use of IL-6 inhibitors (tocilizumab) to block cytokines in CAR-T cell-driven CRS shows how personalized treatments for dangerous pathways can stay effective. As a result, immunological therapy needs both preventative and curative methods. 103
Technological advancements: AI and digital health care
AI is more important for predicting how well a treatment will work and how toxic it will be. Machine learning algorithms can combine genetic, clinical, and radiological data to predict the likelihood of negative events, which lets doctors make changes to treatment plans before they happen. 104 Wearable biosensors and digital health systems allow for constant monitoring of a patient’s physiology, including early warnings of toxicity before the patient’s condition gets worse. 105 These digital methods allow for precise management on an unprecedented scale, enabling the transition of toxicity monitoring from a reactive to a proactive paradigm. 106
Improving cancer treatment while lowering toxicity is not a one-time effort; it requires progress in drug design, precision medicine, supportive care, and new digital health technologies. 107 No method can completely eliminate toxicity, but combining pharmacogenomics, adaptive dosage, nanotechnology, and immunomodulatory methods has greatly increased the TW. 108 Future plans include using real-time monitoring, AI-powered predictive models, and personalized approaches to make sure that cancer treatment gives patients both a better chance of survival and a better quality of life over time. 109
Implementing AI-driven therapeutic personalization presents considerable regulatory and validation hurdles, stemming from the evolving, data-reliant characteristics inherent in these systems. Unlike conventional therapeutics, AI models, frequently categorized as Software as a Medical Device, necessitate stringent validation to ensure accuracy, generalizability, and reproducibility across varied patient demographics; however, they are often trained on datasets that are either limited or biased, thereby raising concerns regarding both reliability and equitable access. 110 Regulatory agencies mandate “locked” algorithms for approval, a requirement that conflicts with the adaptive learning capabilities of AI, thus necessitating novel frameworks, such as predetermined change control plans, to govern updates. Furthermore, the absence of standardized, high-quality multiomics and clinical data complicates the processes of model training and validation, while the “black box” nature of numerous algorithms impedes interpretability and clinician confidence. 111
Patient safety and accountability represent a significant area of concern, especially when determining liability in instances of inaccurate predictions or negative results. Moreover, conventional clinical trial methodologies frequently prove inadequate for assessing AI systems, thereby necessitating adaptive trials and real-world evidence. 82 Addressing these challenges necessitates the establishment of rigorous validation pipelines, the development of transparent and explainable models, continuous postmarket surveillance, and the evolution of regulatory frameworks to facilitate the secure and effective incorporation of AI into clinical practice.
Dose Optimization and Scheduling
The efficacy of anticancer therapy depends not only on the selected pharmacological agent but also on its timing of administration. To get the best results in killing tumor cells while causing the least damage to normal tissues, it is important to find the right dose and schedule. 110 The challenge arises from the narrow TW of numerous anticancer agents, in which slight dose modifications may lead to therapeutic failure or unacceptable toxicity. 111 In the last few decades, improvements in pharmacology, pharmacogenomics, and clinical oncology have made dosage strategies better by moving from one-size-fits-all approaches to personalized, evidence-based plans. 82
Pharmacological foundation of dose optimization
Historically, traditional chemotherapy was governed by the MTD principle, which involved escalating treatment intensity until dose-limiting toxicities occurred. 112 This approach was based on the idea that higher doses lead to better tumor removal. However, therapies based on MTD can sometimes cause serious side-effects in patients without guaranteeing better outcomes for all types of cancer.
The PK and PD of anticancer agents demonstrate considerable variability among individuals. 113 Age, organ function, comorbidities, and genetic polymorphisms can all affect how drugs are absorbed, distributed, metabolized, and excreted. This can lead to unexpected toxicity. By using PK and PD ideas in dosage, doctors can make the best use of regimens that keep therapeutic medication concentrations steady while lowering peaks that could cause toxicity or troughs that could lead to undertreatment. 114
The strategy for targeted therapeutics has evolved from MTD to optimum biological dose (OBD)—the least amount of drug needed to effectively inhibit the target while causing the least amount of harm. This shows that kinase inhibitors, monoclonal antibodies, and immunotherapies have their own unique kinetics, which means that effectiveness does not always depend on dosage. 115
Therapeutic drug surveillance and dynamic dosing
TDM has become an essential tool in optimizing dosages, especially for medications with narrow TWs. Monitoring serum concentrations of high-dose methotrexate is necessary to guide leucovorin rescue and prevent renal damage. Busulfan is commonly utilized in conditioning regimens for hematopoietic stem cell transplantation and is administered based on plasma concentrations to enhance efficacy while reducing pulmonary and hepatic risks. 116
Adaptive dosing goes beyond TDM by taking into account changing patient factors for real-time changes. Dosage algorithms take into account tests of kidney and liver function, body surface area, and signs of toxicity. New AI-driven PK/PD models use clinical, genetic, and biochemical data to predict the best dosage regimens. This reduces the guesswork that comes with changing doses based on what works for you. 117
From traditional cycles to metronomic approaches in scheduling techniques: Conventional chemotherapy is given in cycles, with breaks in between for normal tissues to heal. This approach, although advantageous in certain contexts, frequently allows tumor cells to repopulate during treatment pauses. To lessen this limitation, different scheduling models have come into being. Dose-dense regimens reduce the time between cycles without necessarily increasing the total dose. This approach, which started with doxorubicin and cyclophosphamide for breast cancer, makes treatment more effective by reducing the chances of the tumor coming back. 118
Metronomic chemotherapy is a different way to give drugs: Low doses are given all the time or at regular intervals without long breaks. Metronomic treatments target tumor angiogenesis and immunological regulation instead of solely relying on direct cytotoxicity. This method is associated with reduced toxicity compared with conventional high-dose regimens and is particularly relevant in palliative care or resource-limited settings. 119
Different scheduling methods are needed for targeted treatments and immunotherapies. 120 Imatinib and osimertinib are examples of kinase inhibitors that are often given continuously to keep the target from being activated. 121 ICIs, on the contrary, are given at regular intervals to keep the immune system active for a long time while avoiding immune-related side-effects. 122
Chronotherapy: Synchronizing treatment with biological rhythms
Chronotherapy, which means giving medicine at the same time as the body’s natural circadian cycles, is a new way to plan doses. Many biological processes, including DNA repair, metabolism, and cell cycle regulation, demonstrate circadian rhythms. Giving chemotherapy when normal tissues are most resistant and cancer cells are most vulnerable may improve the therapeutic ratio. 121
For example, oxaliplatin and 5-FU have lower toxicity to the digestive system and blood when given at certain times of the day. Chronotherapy is a new way to tailor treatment to the biology of the tumor and the physiology of the host, even though it requires careful monitoring of each patient. 122
Modifications of dosage and de-escalation in contemporary oncology
In the past, it was thought that lowering the intensity of chemotherapy doses meant that they were less effective. Recent studies show that lowering the dose may keep therapeutic effects in some patients, especially when it comes to targeted treatment and immunotherapy. Lower doses of imatinib may aid people with CML stay in remission while lowering the risk of long-term side-effects. 123 In the same way, researchers are looking into personalized checkpoint inhibitor regimens to get the best long-term responses while lowering the risk of irAEs. At the same time, dosage escalation studies based on biomarker feedback are being done for resistant illness to make sure that subtherapeutic exposures do not make resistance worse. 124 Because of this, flexible dosage adjustment is becoming more and more important for long-term illness management and improving quality of life.
The basis of effective and acceptable cancer treatment is finding the right dose and schedule. Strategies are changing from standard MTD-driven chemotherapy to OBD-guided targeted treatments that focus on customization. 125 TDM, adaptive dosage, metronomic treatment, and chronotherapy are all examples of how medicine is moving away from trial-and-error methods and toward more precise regimens. In the end, the right dose and timing are important steps to widening the TW, keeping patients’ quality of life high, and improving long-term results. 126
Targeted Therapies and Precision Medicine
Targeted medicines and precision medicine have changed the field of cancer in a significant way. Conventional chemotherapy indiscriminately targets rapidly proliferating cells, whereas targeted therapies are specifically designed to disrupt biochemical pathways essential for tumor proliferation and survival. This shift in thinking has made it possible to move from standardized, empirical treatments to personalized therapies that are tailored to the genetic, epigenetic, and phenotypic characteristics of each patient’s cancer. There have been significant enhancements in survival rates and quality of life for numerous cancers. 127
Principles of targeted therapy
Targeted therapies are based on the idea that cancers have specific molecular changes that make them more likely to spread. By hindering these drivers, cancer cells may be specifically rendered nonfunctional while safeguarding normal tissues. 128 The effectiveness of imatinib in CML marked a significant advancement, illustrating that the inhibition of the BCR-ABL fusion protein could yield prolonged remissions with significantly lower toxicity relative to chemotherapy (Table 4). 129 Classes of targeted medications comprise the following:
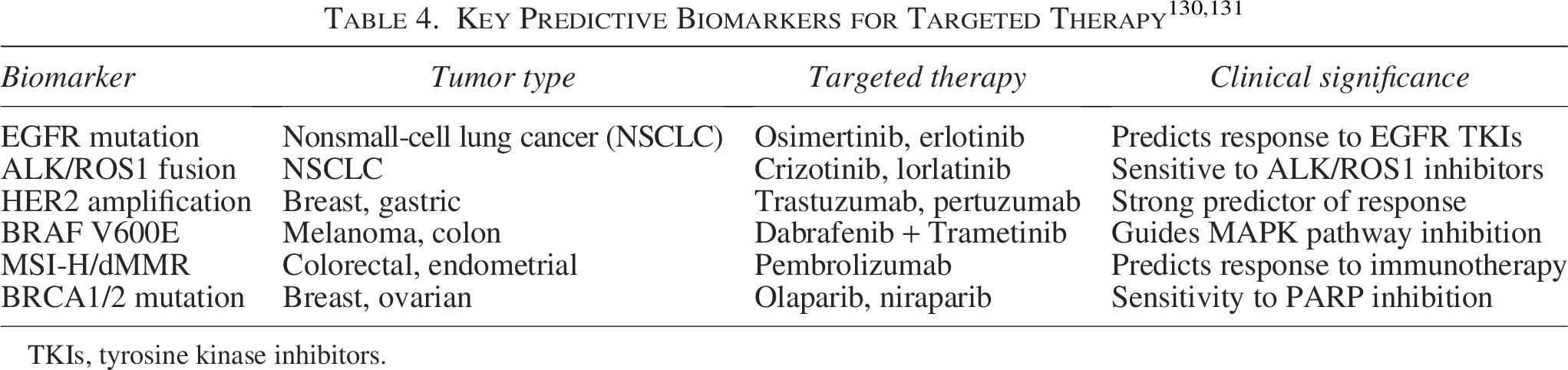
TKIs, tyrosine kinase inhibitors.
TKIs: Inhibit abnormal signaling pathways (e.g., EGFR, ALK, BRAF, VEGFR).
Monoclonal antibodies: Attach to extracellular targets, inhibiting ligand–receptor interactions or enlisting immune effectors (e.g., trastuzumab targeting HER2).
ADCs: Integrate the specificity of antibodies with cytotoxic agents (e.g., trastuzumab emtansine).
PARP inhibitors: Utilize synthetic lethality in BRCA-mutant neoplasms.
These medicines illustrate that cancer is not a homogeneous illness but rather a conglomerate of genetically distinct subgroups, each necessitating customized strategies. 132
Precision medicine: The incorporation of genomics
Precision oncology goes beyond just making new drugs; it also includes diagnostic, prognostic, and therapeutic parts. High-throughput sequencing and molecular profiling make it easier to find mutations that can be acted upon in some cancers. Next-generation sequencing (NGS), whole-exome sequencing, and liquid biopsies are some of the technologies that let doctors see a tumor’s genetic structure in real time. 133
For instance:
EGFR mutations in nonsmall-cell lung carcinoma forecast responsiveness to EGFR TKIs such as osimertinib. ALK and ROS1 rearrangements dictate the administration of crizotinib and subsequent generation inhibitors. HER2 amplification in breast and gastric malignancies forecasts advantages from trastuzumab and novel HER2-targeted therapies. MSI-H/dMMR status in colorectal and endometrial malignancies predicts sustained responses to immune checkpoint drugs.
134
These advancements demonstrate the efficacy of incorporating diagnostics and medicines into a seamless cycle of individualized care.
Obstacles and resistance mechanisms
Notwithstanding their efficacy, targeted treatments encounter several constraints, including the development of drug resistance. Resistance may be classified as primary, whereby tumors exhibit no response, or acquired, where originally sensitive malignancies develop mechanisms to evade treatment.
135
Mechanisms include the following:
Secondary mutations in the target protein, such as EGFR T790M and ALK G1202R. Activation of bypass pathways, enabling tumors to use alternate signaling paths. Phenotypic alteration, exemplified by small-cell transformation in lung malignancies initially susceptible to EGFR TKIs.
136
Surmounting resistance necessitates advanced inhibitors, strategic medication combinations, and adaptive dosing methodologies informed by real-time tumor evolution monitoring. Liquid biopsies that identify circulating tumor DNA (ctDNA) are very useful for monitoring resistance dynamics. 137
Broadening the parameters: Transcending genomics
Precision medicine is progressively incorporating additional dimensions of biological complexity beyond genetics. Epigenomics, proteomics, metabolomics, and immunoprofiling yield additional insights into tumor biology that may improve therapeutic options. 138 The TME, the immune system of the host, and the gut microbiome all have an effect on how well treatment works. Gut microbial diversity has been demonstrated to affect outcomes with checkpoint inhibitors, suggesting possible strategies for therapeutic modulation. Combining multiomics with AI and machine learning could lead to the discovery of new biomarkers, the prediction of how well a treatment will work, and the identification of druggable weaknesses that genetic analysis alone cannot find. 139
Clinical implications and prospective trajectories
The impact of personalized medications and precision medicine is evidenced by enhanced survival rates in diverse malignancies. The 5-year survival rate for people with CML who are taking imatinib is similar to that of the general population.
140
Patients with nonsmall-cell lung cancer possessing driver mutations can now anticipate years of disease management, in contrast to the months typically associated with chemotherapy. BRAF and MEK inhibitors quickly make melanoma worse, but combining them with immunotherapy makes the effects last longer.
141
Future prospects include
Pan-cancer targeted therapies predicated on molecular drivers rather than the tissue of origin (e.g., NTRK fusion inhibitors). Utilization of empirical data to authenticate biomarkers and enhance therapeutic approaches. AI-driven adaptive clinical trials that modify treatment arms according to molecular responses. Patient-centered care paradigms prioritizing both survival and quality of life.
142
To improve the practical application of this review, it is essential to directly link preclinical discoveries with clinical outcomes. This can be achieved by including examples from recent clinical trials, regulatory approvals, and significant setbacks that underscore current constraints. For example, ADCs such as trastuzumab deruxtecan and sacituzumab govitecan have successfully translated targeted delivery strategies into tangible clinical advantages, as evidenced by enhanced response rates and subsequent approvals from the U.S. Food and Drug Administration. 143 Similarly, nanocarrier-based formulations, such as Doxil, illustrate how PK adjustments (e.g., reduced Cmax and extended circulation time) can lessen cardiotoxicity while preserving therapeutic effectiveness. Conversely, numerous nanoparticle platforms that exhibited robust preclinical efficacy have faltered in clinical trials, primarily due to inadequate tumor accumulation in human subjects, thereby highlighting the limitations of the EPR effect and interspecies variability. 144
Furthermore, although immune-targeted treatments demonstrate efficacy, they frequently present unforeseen toxicities within clinical contexts, thereby highlighting the challenges inherent in extrapolating findings from controlled preclinical settings to diverse patient cohorts. These instances, taken together, emphasize that despite the capacity of preclinical models to elucidate mechanisms for optimizing TWs, clinical results frequently expose limitations in terms of predictability, delivery effectiveness, and safety profiles.
Elevated development expenses and budgetary limitations, compounded by biological hurdles, constitute a significant translational obstacle. Sophisticated platforms such as ADCs, nanomedicines, and AI-driven personalized therapeutics necessitate intricate manufacturing procedures, comprehensive characterization, and stringent regulatory approval, thereby substantially escalating research and development expenditures. 145 The financial strain is further exacerbated by the costs associated with extensive clinical trials, especially those using biomarker stratification or adaptive designs. These financial considerations not only restrict accessibility but also discourage investment in high-risk, novel therapeutics, particularly when clinical outcomes are uncertain. Moreover, challenges pertaining to scalability and reproducibility in manufacturing—especially concerning nanocarriers and biologics—present additional impediments to ensuring consistent quality across production batches.
These challenges together highlight that, although mechanistic methods to improve the TW are scientifically valid, their use in clinical settings requires overcoming obstacles related to predicting toxicity, patient selection, cost-effectiveness, and large-scale production. 5 Therefore, a more integrated and collaborative approach is needed to facilitate the transition from laboratory research to practical medical applications.
Targeted therapies and precision medicine represent a significant advancement in oncology. By combining research on drugs with molecular biology and a patient’s unique profile, they have turned tumors that were once thought to be impossible to treat into chronic illnesses that can be managed. However, there are still problems such as drug resistance, high costs, and unequal access. The next step in precision oncology will use multiomics, real-time monitoring, and advanced computer models to make medicines that work better and are more tailored to each patient. 143
Immunotherapy: Balancing Response and Adverse Events
Immunotherapy has profoundly transformed the treatment paradigm of oncology by harnessing the body’s immune system to detect and eliminate cancerous cells. Immunotherapeutic approaches, including ICIs, adoptive cell transfer, cancer vaccines, and cytokine therapies, offer the potential for enduring clinical outcomes, in contrast to traditional chemotherapies that induce extensive cytotoxic effects. Nonetheless, the mechanism that underpins their efficacy concurrently increases the probability of irAEs, underscoring the challenge of maintaining a beneficial treatment window. 144
One important thing about immunotherapy is that it can start T cell-mediated responses against tumor-associated antigens. Monoclonal antibodies, such as anti-CTLA-4 and anti-PD-1/PD-L1, have demonstrated significant survival advantages in malignancies, including melanoma, nonsmall-cell lung cancer, and renal carcinoma. These treatments universally augment immunological function; however, they may induce systemic toxicity by undermining self-tolerance. 145 Clinical manifestations range from mild dermatological reactions and colitis to severe endocrinopathies, hepatitis, or pneumonitis. The frequency and severity of irAEs vary according to the type of immunotherapy, the length of treatment, and the characteristics of the patient. 5 To find the right balance between antitumor efficacy and acceptable toxicity, one needs to carefully choose patients, keep a close eye on them, and act quickly. Corticosteroids and immunosuppressive drugs are the main treatments for most irAEs. However, they must be used carefully so as not to reduce the effectiveness of the treatment. In addition, discontinuation of therapy may be imperative in severe cases, highlighting the critical need for predictive markers to identify individuals at heightened risk. 146
Recent advancements in biomarker research suggest promising opportunities. The baseline immunological profile, circulating cytokines, T cell clonality, and microbiome composition correlate with both efficacy and toxicity. 147 A diverse gut microbiota appear to enhance the efficacy of checkpoint inhibitors while affecting the occurrence of immune-mediated colitis. Similarly, a high tumor mutational burden, while suggesting antitumor efficacy, may also correlate with an augmented risk of adverse effects. Adding these indicators to standard care could make it easier to do proactive risk assessments and create personalized immunotherapy plans. 148 Future efforts to improve the TW in immunotherapy will involve examining modified dosing regimens, localized delivery techniques (e.g., intratumoral injections), and novel checkpoint inhibitors with enhanced safety profiles. New technologies such as synthetic biology and modified regulatory T cells could aid make immune regulation more precise. 149
In short, immunotherapy has changed how one treats cancer by giving long-lasting responses that traditional medicines could not provide. The challenge lies in mitigating immune-mediated toxicities that hinder widespread application. To get the best clinical results while lowering the risk to patients, success depends on combining biomarkers, personalized treatment plans, and new immunomodulatory technologies. Achieving this balance will be essential to realizing the full potential of immunotherapy in cancer treatment. 24
Combination Therapies: Synergies and Risks
Combination therapy is essential in modern oncology, predicated on the notion that simultaneously targeting diverse oncogenic pathways and resistance mechanisms may augment efficacy. Combining traditional chemotherapy, targeted therapy, radiation, and immunotherapy into strategic combinations has led to significant improvements in survival rates for many types of cancer. However, making a drug more effective often makes it more toxic, which makes it very hard to keep a TW that is acceptable. 129
The potential of combination strategies is based on synergistic interactions. Chemotherapy and radiation can enhance immunogenic cell death, leading to increased antigen release and thereby improving the efficacy of checkpoint inhibition. Similarly, targeted therapies that inhibit signaling pathways (e.g., VEGF or MAPK inhibitors) may modulate tumor vasculature or enhance T cell infiltration, thereby creating a more favorable environment for immunotherapy. 150 These methods have shown great results in melanoma, renal carcinoma, and nonsmall-cell lung cancer, where dual checkpoint inhibition or combinations of targeted therapy and immunotherapy led to longer responses than monotherapy. The rise in potency inevitably heightens concerns regarding toxicity. Combination therapies often result in additive or synergistic adverse effects, such as hematologic suppression, gastrointestinal toxicity, vascular complications, or aggravated immune-mediated reactions. 151 The simultaneous inhibition of CTLA-4 and PD-1, while effective, underscores this challenge by elevating the occurrence of severe toxicities compared with monotherapy. In targeted immunotherapy combinations, increased hepatotoxicity and colitis are frequently noted.
To reduce these risks, the drug schedule, dosage, and order of administration must be carefully optimized. Adaptive trial methods now make it easier to find dose levels that maximize synergistic efficacy while keeping toxicity levels acceptable. 97 Furthermore, temporal sequencing (e.g., induction chemotherapy followed by immunotherapy) may offer benefits by stimulating the immune system while reducing concurrent toxicities. New drug delivery technologies, such as nanoparticle formulations, can send drugs directly to the TME, which reduces the burden on the whole body. 152 A feasible strategy is biomarker-driven patient selection to maximize advantages from specific combinations. PD-L1 expression, tumor mutational burden, and oncogenic driver status can aid figure out when to combine immunotherapy with chemotherapy or targeted therapy. Learning about the different types of TMEs, such as T cell inflamed and “cold” phenotypes, can aid understand them better. 153
For successful use in clinical practice, there needs to be a scientific basis and thorough monitoring of toxicity. Multidisciplinary care teams, standardized toxicity management protocols, and proactive patient education are essential components. 154 Clinical trial designs that evaluate both efficacy and toxicity as coprimary outcomes are equally important, enhancing the understanding of long-term risk–benefit ratios. The effectiveness of combination therapies depends on finding a balance between synergistic efficacy and acceptable safety. Precision-guided combinations, enhanced by pharmacological innovations and predictive biomarkers, will be essential for expanding the treatment window. 155
Biomarkers for Patient Stratification and Toxicity Forecasting
Biomarkers are important tools that aid doctors decide on the treatment and predict how well it will work and what side-effects it might have. Their growing usefulness comes from improvements in genomes, proteomics, transcriptomics, and liquid biopsy technologies. They make it easier to use personalized strategies, improve results, and lower the risk of serious side-effects. 156 To get the most out of multiomic markers and digital platforms, they need to keep getting better and be used more widely in cancer treatment. By grouping patients based on predictive and prognostic indicators, doctors can improve treatment protocols and lower risk, which opens up more treatment options. Selecting patients based on biomarkers makes it easier to create a personalized plan for cancer treatment. 154 The presence of PD-L1 on tumor cells signifies the suitability for ICIs, while driver mutations in genes such as EGFR or ALK identify patients most likely to benefit from targeted therapy. This precision improves the therapeutic success rates and minimizes exposure to ineffective or excessively detrimental treatments. Somatic mutations, gene fusions, and amplifications identified through NGS are becoming increasingly standard in guiding the selection of medications, including TKIs and monoclonal antibodies. 129
The forecast of toxicity holds equal importance. Germ line variations in drug metabolism genes (e.g., TPMT, DPYD, UGT1A1) signify an elevated risk of adverse drug reactions to agents such as mercaptopurine, fluorouracil, or irinotecan. Recognizing these signs makes it easier to change the dose or try a different treatment, which can aid avoid serious problems. 157 Along with DNA, protein indicators, cytokine profiles, and ctDNA make it much easier to guess what will happen and what side-effects will happen. In immunotherapies, baseline levels of C-reactive protein or inflammatory cytokines have been associated with the likelihood of irAEs. 137 Microbiome signatures, a novel category of biomarkers, affect response rates and toxicity in immunotherapy, demonstrating the complex interactions among the host, environment, and medication. Liquid biopsies, which give real-time, noninvasive assessments, are being used more and more in clinical settings to keep an eye on how well the treatment is working, how the disease is getting worse, and possible side-effects. Serial ctDNA evaluations may indicate early relapse or resistance and, in specific cases, predict the emergence of toxicity before clinical presentation (Table 5).158–160
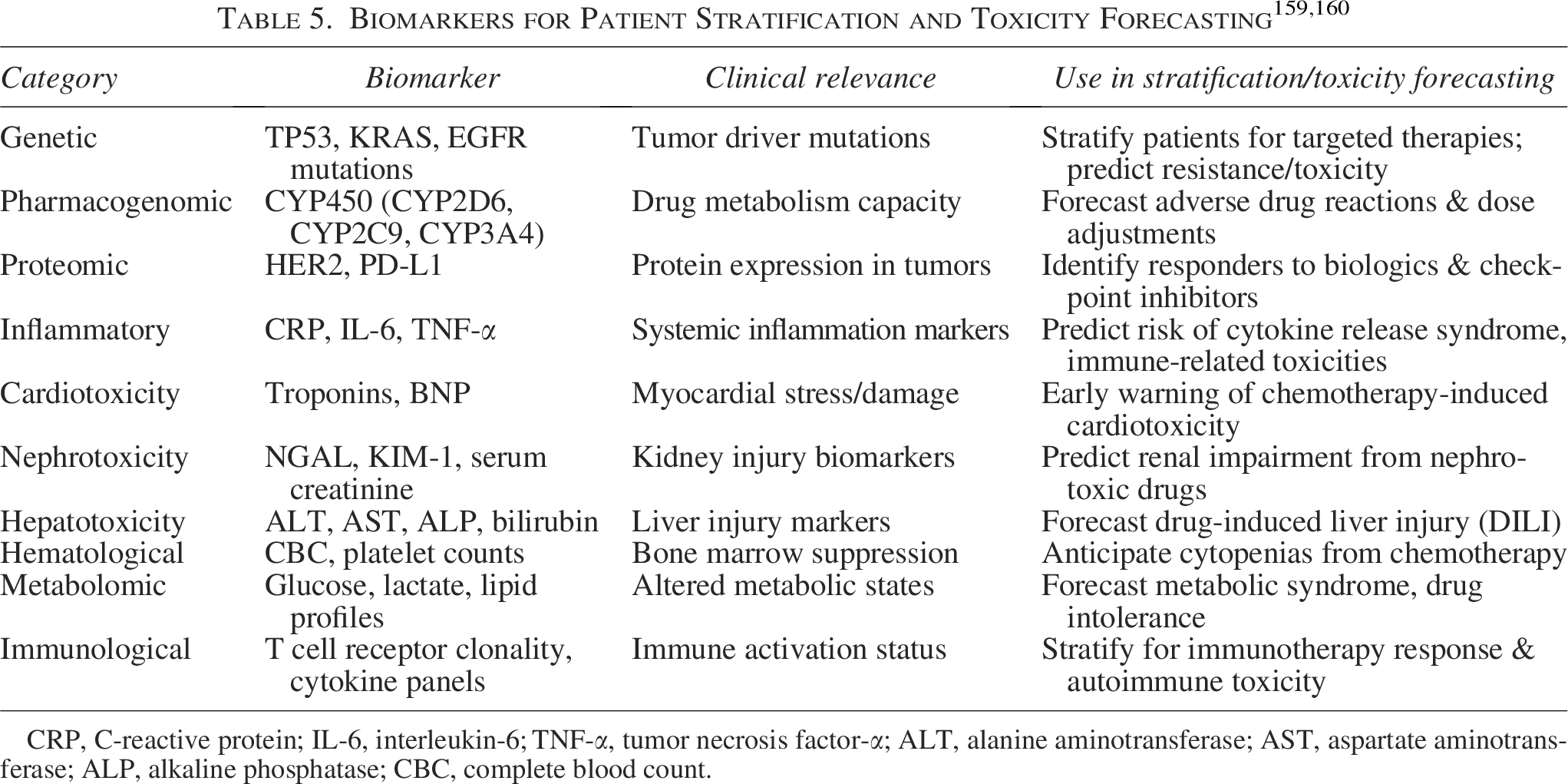
CRP, C-reactive protein; IL-6, interleukin-6; TNF-α, tumor necrosis factor-α; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; CBC, complete blood count.
The challenge remains in validating biomarkers for extensive use. It is imperative to undertake prospective clinical studies and establish rigorous analytical frameworks to validate repeatability and clinical applicability. The implementation of electronic health records and AI-driven decision support systems is anticipated to further improve stratification and toxicity prediction. 161
Enhancements in Drug Delivery Systems to Expand the TW
Improvements in drug delivery systems have made it much easier to tailor cancer treatment to each patient, opening up new ways to make it more effective and less harmful. Conventional systemic medications often damage healthy tissues; however, contemporary delivery techniques can precisely target tumor cells, broaden the TW, and improve patient outcomes. 162
Nanoparticles, liposomes, dendrimers, and micelles are widely used platforms for encapsulating chemotherapeutic drugs or biologics. Nanoparticle carriers take advantage of the increased permeability and retention effect in tumors to aid medicines build up at the site of disease. Liposomal doxorubicin is authorized for breast cancer and recurrent ovarian cancer, exhibiting reduced cardiotoxicity compared with its conventional counterpart. 163 Paclitaxel bound to albumin improves tumor delivery while protecting healthy tissues. ADCs represent a substantial progression in precision medicine. ADCs improve delivery to the tumor site while lowering off-target effects by linking strong cytotoxins to monoclonal antibodies that target tumor antigens (e.g., trastuzumab emtansine for HER2 in breast cancer). This method has led to the approval of many drugs and made it possible to use effective drugs in more situations. 164
Implantable devices and depot formulations enable extended drug release near malignancies. Intratumoral injections of immunotherapeutic agents, nanoparticles, or cytokines ensure localized exposure while reducing systemic harm. Researchers are looking into using hydrogels, wafers, and reservoir devices for direct surgical implantation at the tumor site. 165 Stimuli-responsive (smart) administration, where medication release is triggered by internal (pH, enzymes) or external (ultrasound, light, magnetic fields) signals, pushes the field even further. These methods enable controlled, on-demand release that improves safety and extends therapeutic effectiveness. 166
Difficulties with these advancements include the complexity of manufacturing, the immunogenicity of carriers, and the different TMEs that may affect targeting. For integration to work, there must be regulatory standards for safety profiles and a lot of clinical validation. 167 Innovations in medication distribution are necessary for reducing treatment-related toxicities and improving efficacy. Ongoing interdisciplinary collaboration that includes material science, engineering, molecular biology, and clinical research will be very important for turning these new methods into standard cancer treatments. 168
Surveillance and Administration of Toxicities: Clinical Protocols and Innovative Instruments
Traditional methods, although advantageous, may inadequately support early diagnosis and proactive management, especially given that new medications demonstrate unique and potentially unforeseen adverse event profiles. Modern oncology puts a lot of emphasis on monitoring toxicity in real time and responding across disciplines. 169
Electronic patient-reported outcomes (ePROs) have changed the way symptoms are tracked by letting patients consistently report bad effects through digital platforms. Studies show that using ePROs makes it easier to quickly find symptoms such as diarrhea, fatigue, neuropathy, or immune-mediated events. 170 This leads to quick actions that improve the quality of life and, in some cases, survival rates. Wearable technologies and mobile health applications improve the tracking of physiological indicators, activity, and sleep, enabling digital phenotyping of therapeutic side-effects.
Standardized clinical pathways for managing drug toxicity have been established. 171 There are already established management algorithms for irAEs that support the use of ICIs. These algorithms usually start treatment with corticosteroids and, in cases that do not respond, use specific immunosuppressants such as infliximab for colitis. Growth factor administration and infection prevention strategies are used to treat chemotherapy-induced neutropenia before it happens. 172 Targeted drugs such as VEGF or EGFR inhibitors, which can cause high blood pressure, rashes, or liver damage, are treated with pharmacological and nonpharmacological interventions that are tailored to the specific side-effects of the drugs.
New tools that use AI and predictive analytics open up new possibilities. 173 AI models that have been trained on large datasets can tell how likely it is that a treatment will be toxic before or during it. These models use patient genomes, comorbidities, polypharmacy, and baseline laboratory markers to make risk classification very personalized. Integration with electronic health records improves clinical decision support and makes sure that alerts and actions are sent out on time. 174 Telemedicine and remote monitoring platforms make long-term care better, especially for outpatient therapy and oral medications. They cut down on the number of trips to the hospital, which lowers health care costs, and they make patients happier. There are still problems in dealing with symptoms that are not reported enough, differences in digital literacy, and uneven access to technology. In addition, synchronizing the integration of clinical technologies across care settings is crucial to prevent care fragmentation. 175
Case Studies: Effective Extension of the TW in Oncology
Case studies provide critical insights into the secure and efficient advancement of cancer treatment methodologies. These cases illustrate the interplay among innovation, personalized therapy, and rigorous clinical care. A significant example is the development and clinical application of liposomal doxorubicin (Doxil) for metastatic breast and ovarian cancer. 176 Conventional doxorubicin, while effective, is associated with dose-dependent cardiotoxicity. The reformulation into a liposomal encapsulated medication takes advantage of the tumor’s permeable blood vessels to deliver the drug to the right place, which lowers the risk of heart problems and allows for a longer cumulative dose (Fig. 3). Subsequent clinical trials demonstrated comparable (or superior) efficacy with markedly improved safety profiles, highlighting how innovations in drug delivery could broaden the TW. 177 Another important example is ADCs, such as brentuximab vedotin for Hodgkin’s cancer. ADCs make targeted delivery easier by linking cytotoxic drugs to antibodies that target CD30. This also lowers the toxicity to normal tissues (Fig. 3). This method made it possible to use medications that were once dangerous more widely, which improved outcomes for patients with refractory lymphoma and reduced hematologic toxicity. 178

Conceptual depiction of the therapeutic window in oncology treatment: The graph shows how drug dose affects the body. It shows areas of no effect or toxicity, tolerable toxicity (the therapeutic window), and intolerable toxicity. The figure shows that the therapeutic window is the range of doses that cause a therapeutic effect with acceptable side-effects. Going above this range causes toxicity that cannot be tolerated. This picture shows some typical chemical structures of anticancer drugs and stresses how important it is to find the right dose to widen the therapeutic window.
ICI therapy for melanoma encountered challenges initially due to increased instances of irAEs linked to combination regimens. By optimizing dosages and using biomarker-guided selection (such as PD-L1 expression and TMB), doctors have made therapy more personalized, which has led to higher response rates and fewer severe side-effects. 179 Studies suggest that limiting the duration of therapy or using sequential regimens may further reduce risk without undermining therapeutic effectiveness. DPYD gene testing in colorectal cancer identifies patients susceptible to 5-fluorouracil-related toxicity, facilitating personalized dosing and significantly decreasing life-threatening side events resulting from a successful application of pharmacogenomic testing to avert serious toxicity. 180 The introduction of oral targeted therapies, such as imatinib for CML, has revolutionized both efficacy and tolerability. By identifying the genetic driver (BCR-ABL), treatment was tailored, leading to extended remissions with minimal toxicity.
Prospective Trajectories: Innovative Methodologies and Technologies
The oncology field is on the verge of major changes because new technologies and ideas are expected to improve the TW and change how safe and effective cancer treatments are. 181 Future directions are predicated on multidisciplinary innovation, amalgamating advancements from gene editing, synthetic biology, immunoengineering, AI, and precision pharmacology.
Gene editing tools, especially CRISPR-Cas9, can directly fix mistakes that cause cancer or make tumor cells more likely to be found by the immune system. 182 Initial clinical trials utilizing CRISPR-modified T cells, obstructing immunological checkpoints or augmenting tumor-antigen specificity, have shown feasibility and signs of prolonged response, while also potentially diminishing off-target toxicities through improved genetic specificity. 183 The continuous improvement of gene editing provides “intelligent” cell therapies that can adapt to changes in the TME in real time. 184
Synthetic biology and programmable biotherapeutics are used to create circuit-based immune cells integrated with logic gates that activate exclusively in response to specific antigenic or environmental signals indicative of malignant tissue. 185 These systems mitigate damage to healthy cells, thereby improving the safety profile of cell-based immunotherapies and other biological agents. 111 In early-phase trials, researchers are testing strategies such as “on-switch” CAR-T cell treatments and split-receptor designs.
AI will play a significant role in making cancer treatment more personalized. AI-driven systems are used to guess how well treatments will work, find drug combinations that work well together, figure out the best dose and schedule, and figure out how likely it is that dose-limiting toxicities will happen. 82 AI techniques, when combined with multiomic biomarkers and large amounts of clinical data, are ready to make treatment algorithms that are specific to each patient in real time. 186 Personalized dosage algorithms, informed by pharmacogenomics, body composition, real-time medication monitoring, and analytical modeling, offer novel strategies to maintain efficacy while mitigating toxicity. 187 Advancements in TDM, especially for oral targeted therapies and immunotherapies, allow clinicians to adjust dosages dynamically, particularly in fluctuating clinical scenarios such as hepatic or renal dysfunction.188–190 New types of drugs, such as bispecific antibodies, multispecific T cell engagers, and next-generation ADCs, are making it possible to target more types of drugs. These compounds focus on tumor selectivity, improved effectiveness, and better control of side-effects. 191
In the end, patient-centered technologies such as digital twins, wearable sensors, remote monitoring, and interactive mobile health apps make it easier to keep an eye on patients and act quickly in a wide range of places and situations. These improvements are changing how cancer patients live and how they deal with chronic illnesses. The future of cancer requires not only scientific and technological progress but also systemic changes, including data integration, regulatory framework revision, and ensuring equitable access to these innovations. If done right, these changes could change the way one thinks about medicines from treating toxicities to making medicines where side-effects are rare exceptions instead of expected trade-offs.192–194
Conclusion: Advancing Safer and More Efficacious Cancer Therapies
It is a difficult job to keep trying to expand the TW in oncology. This job uses new discoveries in molecular biology, drug development, clinical practices, and digital technology. The main goal has always been to improve antitumor efficacy while minimizing harm to patients. This has led to decades of slow, and more recently, transformative progress in cancer treatment.
The previous limitations were defined by the narrow margins between efficacy and toxicity inherent in early cytotoxic therapies. Recent advancements enable enhanced patient selection, real-time monitoring, targeted delivery systems, adaptive dosing, and personalized therapeutic approaches. Immunotherapy has yielded enduring responses in previously resistant malignancies; however, meticulous toxicity surveillance is imperative. Using combination therapies wisely, with the aid of biomarkers and advanced delivery systems, improves this balance.
The conclusion, although proficiently predicting future strategies for extending the treatment window, might be improved by a more comprehensive analysis that clearly delineates the existing constraints impeding practical use and broader acceptance. A significant constraint arises from the intrinsic heterogeneity of tumor biology; specifically, the inter- and intratumoral variability in genetic alterations, receptor expression, metabolic profiles, and microenvironmental influences substantially impacts treatment outcomes. Even targeted therapeutics such as trastuzumab deruxtecan exhibit variable efficacy due to disparities in antigen expression and tumor proliferation, thereby underscoring the challenge of achieving consistent therapeutic results. A critical impediment is the absence of standardized or predictive preclinical models. Conventional 2D cell cultures and animal models frequently fail to faithfully recapitulate the intricacies of human malignancies.
Digital health, AI, and patient-reported outcome tools are making it easier for everyone to monitor their symptoms and get aid. This turns episodic care into ongoing participation. The expanding range of molecular diagnostics and gene-editing technologies suggests a future of truly individualized therapy, distinguished by high efficacy and minimal adverse effects.
However, for these ideas to work, they need to be carefully tested and put into practice fairly. To get over the problems now, the authors need to work together across disciplines, make real-world evidence, and get patients involved. Regulatory bodies, insurers, and health care systems must adapt to ensure access and sustainability.
The growing TW is a sign of scientific progress and a guide for the future. Ongoing progress will depend on the combination of new technologies, clinical knowledge, patient-centered care, and changes to the system as a whole. Together, these will make cancer treatment safer, more effective, and more tailored to each patient.
Authors’ Contributions
M.M.A., M.G., and J.S.M. were involved in writing and drafting the article. N.S., R.P., and C.B. were involved in reviewing the text. S.D. was involved in editing and illustration of the work.
Footnotes
Availability of Data and Material
For appropriate requests for the current study’s datasets, contact the corresponding author.
Disclosure Statement
The authors say that they do not have any financial ties that could affect their work.
Funding Information
It is financed independently; no financial support was received from a corporation, financing organization, or nonprofit research institution.