
Abstract
Background:
Intratumoral heterogeneity in cervical carcinoma may influence absorbed dose distribution, treatment resistance, and response, but is not adequately captured by conventional uniform planning.
Methods:
A total of 35 patients with histologically confirmed cervical carcinoma underwent baseline theranostic imaging. Voxel-wise tumor uptake was analyzed to derive SUVmax, SUVmean, tumor-to-background ratio, coefficient of variation, entropy, and fractional low-, intermediate-, and high-uptake subregions. Voxel-based absorbed dose distributions were estimated, and a dose heterogeneity index was calculated. Conventional uniform planning was compared with theranostic-guided spatial optimization. An integrated theranostic score was developed for response prediction and risk stratification.
Results:
Nonresponders showed higher uptake intensity, greater spatial heterogeneity, larger high-uptake fractions, and higher integrated theranostic scores than responders. Tumor absorbed dose exceeded that of bladder, rectum, and normal pelvic soft tissue. SUVmean correlated positively with tumor absorbed dose, whereas uptake coefficient of variation correlated with dose heterogeneity. Theranostic-guided spatial optimization improved target coverage, conformity, and high-risk subregion coverage relative to conventional uniform planning. The integrated theranostic score demonstrated strong predictive performance for response classification (area under the receiver operating characteristic curve, 0.95; 95% confidence interval, 0.84–0.98).
Conclusions:
Radionuclide theranostic mapping provided a quantitative framework linking spatial uptake heterogeneity to dosimetry, planning benefit, and treatment response in cervical carcinoma.
Keywords
Introduction
Globally, cervical carcinoma is the leading cause of cancer-related morbidity and mortality despite the screening, vaccination, and multimodal treatment innovations. 1 Concurrent chemoradiation with image-guided treatment delivery is optimal in patients with locally advanced disease, but this remains ineffective in preventing local relapses and resistance to treatment, as this is the main limiting factor especially in bulky or biologically aggressive tumors. 2 Even with the current image-guided planning, whereby anatomical coverage and dose conformity can be improved, the vast majority of the planning strategies still depend largely on the anatomical coverage and lack consideration of biologically heterogeneous subregions within the tumor that might also play a disproportionately important role in resistance and relapse. 3
It has been shown in nuclear medicine therapy studies that imaging-determined target expression and radiotracer uptake can have a clinical impact in the choice of therapy, evaluation of response, and personalized therapy decision making.4,5 Simultaneously, the biologically directed concept of treatment, including dose painting, has highlighted the importance of spatially resolved imaging to localize intratumoral subregions with diverse risk profiles. 6 These complementary advances indicate a necessity for strong and reproducible quantitative procedures to transform functional imaging heterogeneity into clinically significant measures. The uptake patterns of diagnostic imaging biomarkers and radiotheranostic models can further aid in combining diagnostic imaging biomarker patterns with dosage estimates and outcome prediction into precision oncology processes.7,8
The authors present a radionuclide-based theranostic mapping model of cervical carcinoma to measure spatial uptake heterogeneity and describe the intratumoral composition and the development of a relationship between uptake-derived features and the distribution of absorbed dose in this study. They also assessed whether spatial optimization guided by theranostics could be better than standard uniform planning with reference to coverage of biologically high-risk tumor subregions and whether built-in theranostic capabilities may be used to predict treatment responses and risk stratify patients.
Materials and Methods
Ethical considerations and study design
This observational study was conducted in accordance with institutional research governance requirements and applicable ethical standards for research involving human data. Ethical approval for this study was obtained from the Ethics Committee of Heilongjiang University of Chinese Medicine (Ethics No. YJSKY2024-194) before data access and analysis. The study used routinely acquired clinical imaging and outcome data collected as part of standard oncologic care and was designed to evaluate imaging-derived theranostic heterogeneity, voxel-level absorbed dose distribution, planning performance, and treatment response in cervical carcinoma.
Patient cohort and clinical variables
Thirty-five patients with histologically confirmed cervical carcinoma were included. Response status was available for all patients and classified them as responders (n = 20) or nonresponders (n = 15) on the basis of post-treatment clinical and imaging assessment. Recorded clinicopathological variables included age, International Federation of Gynecology and Obstetrics stage, histological subtype, primary tumor size, and nodal involvement. Baseline theranostic imaging parameters were extracted at the lesion level, and an integrated theranostic score was generated for each patient.
Imaging acquisition and lesion delineation
Baseline radionuclide theranostic imaging was performed using standardized hybrid functional–anatomical imaging under quantitative acquisition and reconstruction conditions. Radiopharmaceutical nomenclature followed consensus recommendations for radiopharmaceutical reporting. 9 Image acquisition, reconstruction, and quantitative interpretation were performed according to the established principles for quantitative tumor imaging and standardized uptake assessment. 10 Primary tumor volumes were delineated on fused anatomical–functional images, with contour review performed to ensure consistent tumor definition and exclusion of adjacent physiological activity. Although standardized delineation procedures and review were applied, it is acknowledged that interobserver variability in tumor contouring may influence voxel-level feature extraction and derived heterogeneity metrics. Future work incorporating consensus segmentation protocols and reproducibility assessment will be important to ensure robustness of theranostic feature quantification.
Intratumoral uptake segmentation and feature extraction
Voxel-wise uptake values within each delineated tumor volume were extracted to calculate maximum standardized uptake value, mean standardized uptake value, and tumor-to-background ratio. Intratumoral heterogeneity was quantified using the coefficient of variation and entropy. To characterize spatial uptake composition, tumor voxels were partitioned into three predefined intensity-based subregions: low uptake (<10 SUV), intermediate uptake (10–20 SUV), and high uptake (>20 SUV). These thresholds were selected to provide a standardized and interpretable stratification of voxel-level uptake into biologically relevant intensity ranges, facilitating consistent comparison across patients and lesions. While these cutoffs are not intended to represent absolute biological boundaries, they enable reproducible compartmentalization of uptake heterogeneity. It is acknowledged that alternative thresholding strategies or adaptive segmentation approaches may yield different subregion definitions, and sensitivity to threshold selection should be explored in future studies. The fractional volume of each subregion was then calculated for each lesion. Feature computation and reporting followed standardized quantitative imaging biomarker principles where applicable. 7
Absorbed dose estimation and spatial dosimetry
Absorbed dose distributions were estimated using a voxel-based dosimetry framework informed by quantitative imaging and dose modeling principles. 11 In this framework, voxel-level activity concentration derived from quantitative imaging is assumed to be proportional to local energy deposition, and absorbed dose was estimated using a voxel S-value-based formalism consistent with the established Medical Internal Radiation Dose methodology. Specifically, the dose at each voxel was approximated as the convolution of the spatial activity distribution with voxel-level dose kernels, enabling representation of nonuniform intratumoral energy deposition. This approach provides a reproducible and computationally tractable approximation of spatial dosimetry under clinically realistic imaging constraints. Voxel-level dose estimation followed established internal dosimetry approaches for nonuniform activity distributions 12 and image-based dosimetry practice guidance relevant to radiopharmaceutical therapy. 13 Mean absorbed dose was evaluated for the tumor and for selected normal tissue regions, including the bladder, rectum, and adjacent normal pelvic soft tissue. To quantify spatial dose nonuniformity within the tumor, a dose heterogeneity index was defined as the coefficient of variation of voxel-level absorbed dose. This index was compared with uptake-derived heterogeneity metrics to assess the relationship between functional heterogeneity and absorbed dose variation. From a clinical perspective, higher values of the dose heterogeneity index reflect increased spatial nonuniformity of dose delivery within the tumor, which may correspond to the coexistence of adequately treated and relatively underdosed subregions. Such heterogeneity has potential implications for treatment resistance, as biologically aggressive or high-uptake regions may require preferential dose escalation. Therefore, the dose heterogeneity index provides a quantitative link between imaging-defined heterogeneity and the need for spatially adaptive treatment strategies.
Spatially optimized treatment planning framework
Two planning strategies were compared. The first was a conventional uniform planning strategy designed to provide homogeneous target coverage across the gross tumor volume. The second was a theranostic-guided spatial optimization strategy designed to preferentially enhance coverage of imaging defined high-uptake, biologically high-risk subregions while maintaining acceptable normal tissue exposure. In this context, spatial optimization was implemented under the constraint of preserving clinically acceptable dose levels to adjacent organs at risk, including the bladder and rectum. The framework therefore reflects a balance between enhancing dose delivery to biologically high-risk intratumoral regions and avoiding excessive redistribution of dose that could compromise normal tissue safety. These considerations are critical in pelvic malignancies, where anatomical proximity imposes strict constraints on dose escalation strategies. Planning performance was assessed using target coverage, conformity index, and coverage of the high-risk subregion. The relatively high-risk subregion coverage increase by the theranostic-guided strategy versus the conventional uniform strategy was called optimization benefit. Plan evaluation was viewed with respect to the principles of set target coverage and conformity reporting.
Response assessment, integrated score, and risk stratification
Standardized criteria of clinical and imaging-based assessment were used to determine a responder or nonresponder status in clinical response status based on the assessment criteria recorded in the medical record and interpreted based on published response evaluation systems in solid tumors. 14 An integrated theranostic score was generated using a prespecified multivariable combination of uptake intensity, uptake heterogeneity, and dose heterogeneity features, producing a single continuous score for each patient. The score was scaled to facilitate patient-level interpretation and comparative ranking. Risk stratification was performed in two complementary ways. First, phenotype-based stratification was derived using unsupervised clustering of z score-standardized theranostic features to define low- and high-risk phenotypes. Second, score-based clinical risk groups were defined by dividing the integrated theranostic score distribution into low-, intermediate-, and high-risk categories for descriptive clinical interpretation. If functional imaging response contributed to response classification, metabolic response interpretation was considered in the context of established PET response assessment principles.
Statistical analysis
Continuous variables were summarized as mean ± standard deviation or median with interquartile range, as appropriate, and categorical variables were summarized as number and percentage. Between-group comparisons were performed using the Student t-test or Mann–Whitney U test for continuous variables and the χ2 test or Fisher exact test for categorical variables, as appropriate. Associations between uptake-derived parameters and absorbed dose metrics were evaluated using Pearson or Spearman correlation analysis according to data distribution. Receiver operating characteristic analysis was used to quantify the discriminative performance of the integrated theranostic score, and the area under the receiver operating characteristic curve with confidence intervals (CIs) was estimated using accepted nonparametric methods. 15 Statistical reporting and interpretation were informed by transparent reporting guidance for multivariable prediction models 16 and by established considerations regarding risk of bias in prediction model studies. 17 All tests were two-sided, and p < 0.05 was considered statistically significant.
Results
Baseline cohort characteristics and theranostic uptake heterogeneity
Baseline clinicopathological characteristics and imaging-derived theranostic features are summarized in Table 1. Nonresponders more frequently presented with advanced International Federation of Gynecology and Obstetrics stage, larger primary tumors, and higher rates of pelvic nodal involvement, indicating greater baseline disease burden. Although formal subgroup analysis was beyond the scope of the present cohort size, these observations suggest that disease stage and tumor burden may influence theranostic heterogeneity patterns and integrated score distribution. Stratified evaluation across clinically defined subgroups will be important in future studies to determine whether the predictive and planning relevance of theranostic features varies according to disease extent. In parallel, baseline theranostic measurements showed less favorable uptake and heterogeneity profiles among nonresponders, including higher SUVmax, SUVmean, tumor-to-background ratio, uptake coefficient of variation, entropy, high-uptake fraction, and integrated theranostic score.
B
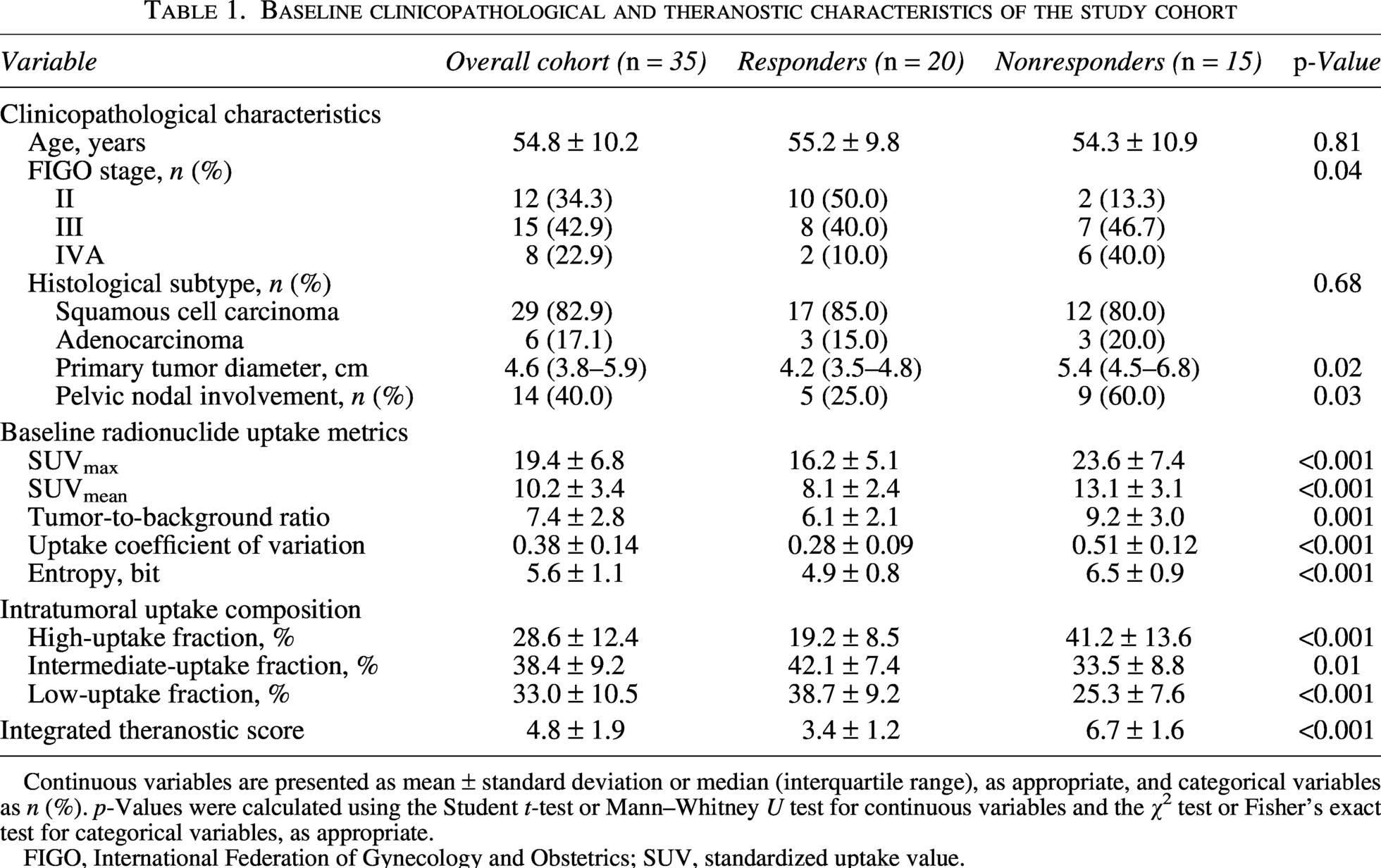
Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate, and categorical variables as n (%). p-Values were calculated using the Student t-test or Mann–Whitney U test for continuous variables and the χ2 test or Fisher’s exact test for categorical variables, as appropriate.
FIGO, International Federation of Gynecology and Obstetrics; SUV, standardized uptake value.
The representative fused whole-lesion theranostic imaging showed significant intratumoral uptake heterogeneity in the primary cervical lesion (Fig. 1A), which was evident in axial, sagittal, and coronal views (Fig. 1B). The lesion was further regionalized at the voxel level to partition it into spatially different high-, intermediate-, and low-uptake compartments (Fig. 1C) to demonstrate nonuniform tracer distribution at the intratumoral level.
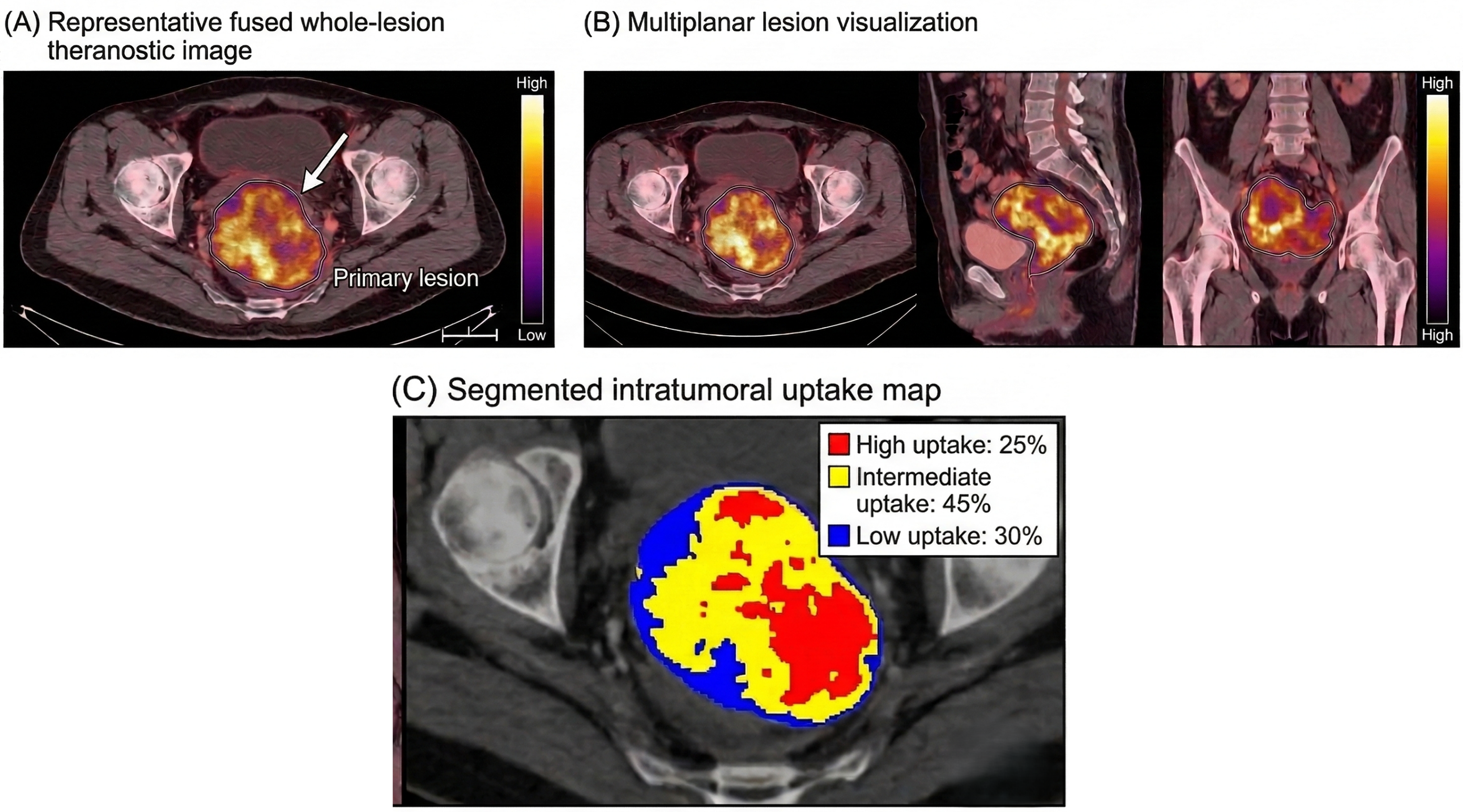
Baseline radionuclide theranostic imaging patterns in cervical carcinoma.
Considering the cohort level, there was significant interlesional variability at the level of SUVmax, SUVmean, tumor-to-background ratio, uptake coefficient of variation, as well as entropy (Fig. 2A). The heatmap visualization at the patient level showed orderly covariation of uptake intensity, heterogeneity, and uptake fraction characteristics and apparent differences by the response group (Fig. 2B). Voxel-intensity distribution also suggested that lesions had strong spatial heterogeneity in radiotracer accumulation, for example, low uptake (<10 SUV), intermediate uptake (10–20 SUV), and high uptake (>20 SUV) with classification (Fig. 2C).
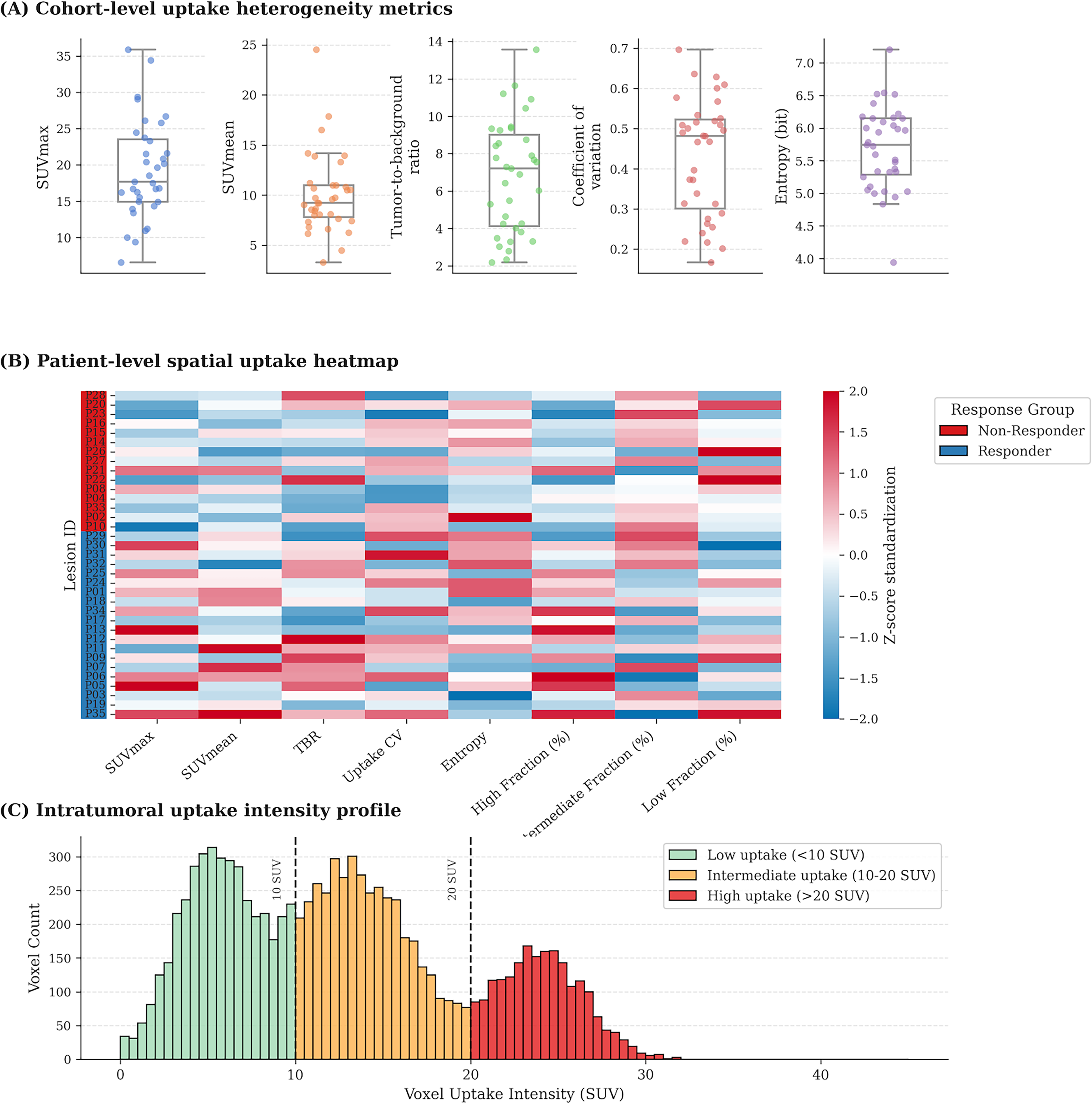
Quantitative spatial heterogeneity of radionuclide uptake in cervical carcinoma.
Spatial dosimetry and dose–uptake relationships
The results of dosimetrics are summarized in Table 2. The mean absorbed dose was significantly higher in tumor tissue compared with the bladder, rectum, and adjacent normal pelvic soft tissue. An absorbed dose representative map showed obvious intratumoral nonuniformity of dose, whereby the main lesion had spatially discrete regions of higher and lower dose compared with the surrounding pelvic anatomy (Fig. 3A). Cohort-level analysis also revealed preferential dose accumulation in tumor over normal tissues (Fig. 3B).
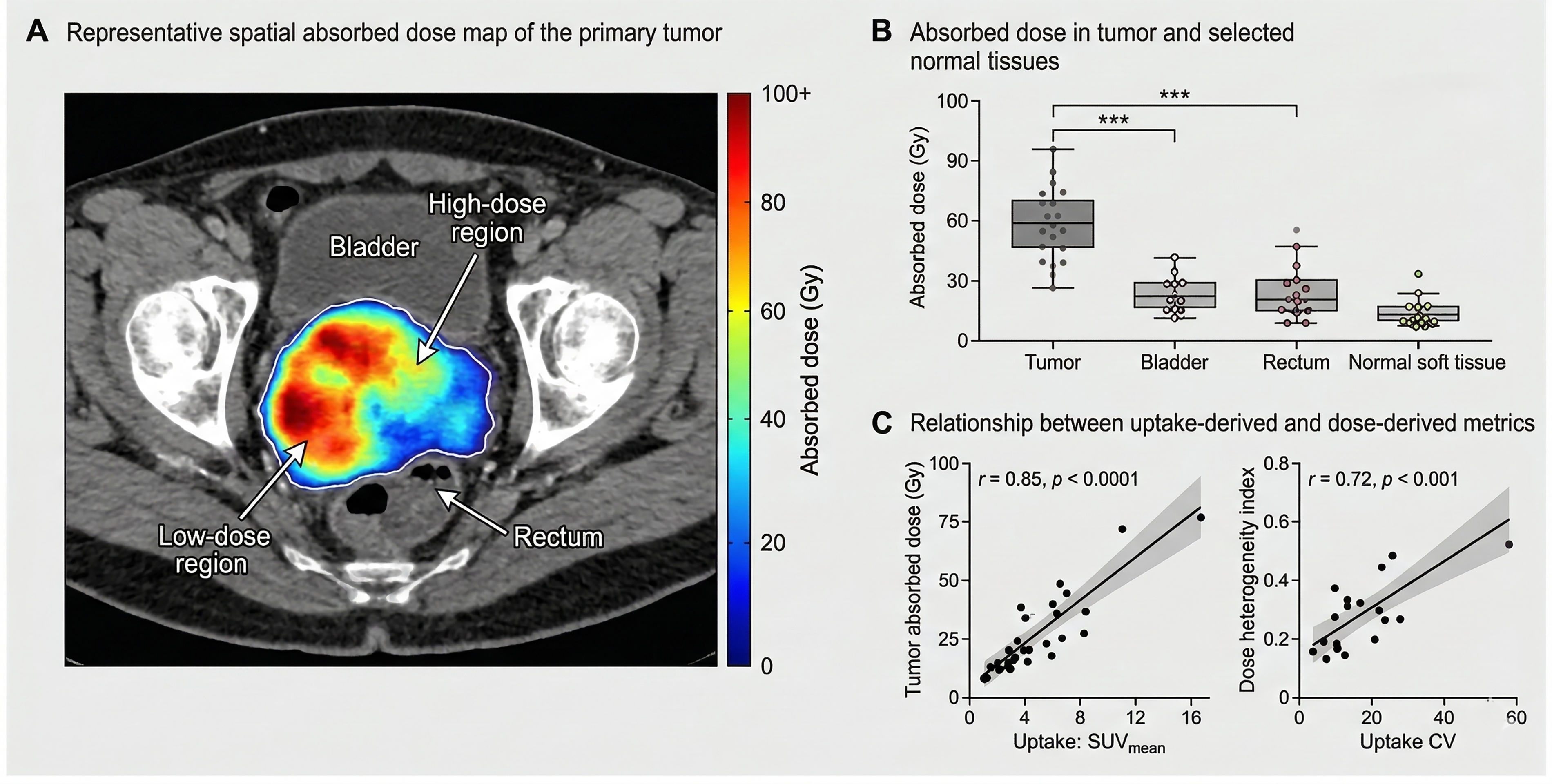
Spatial absorbed dose distribution and dose–uptake relationships in cervical carcinoma.
D
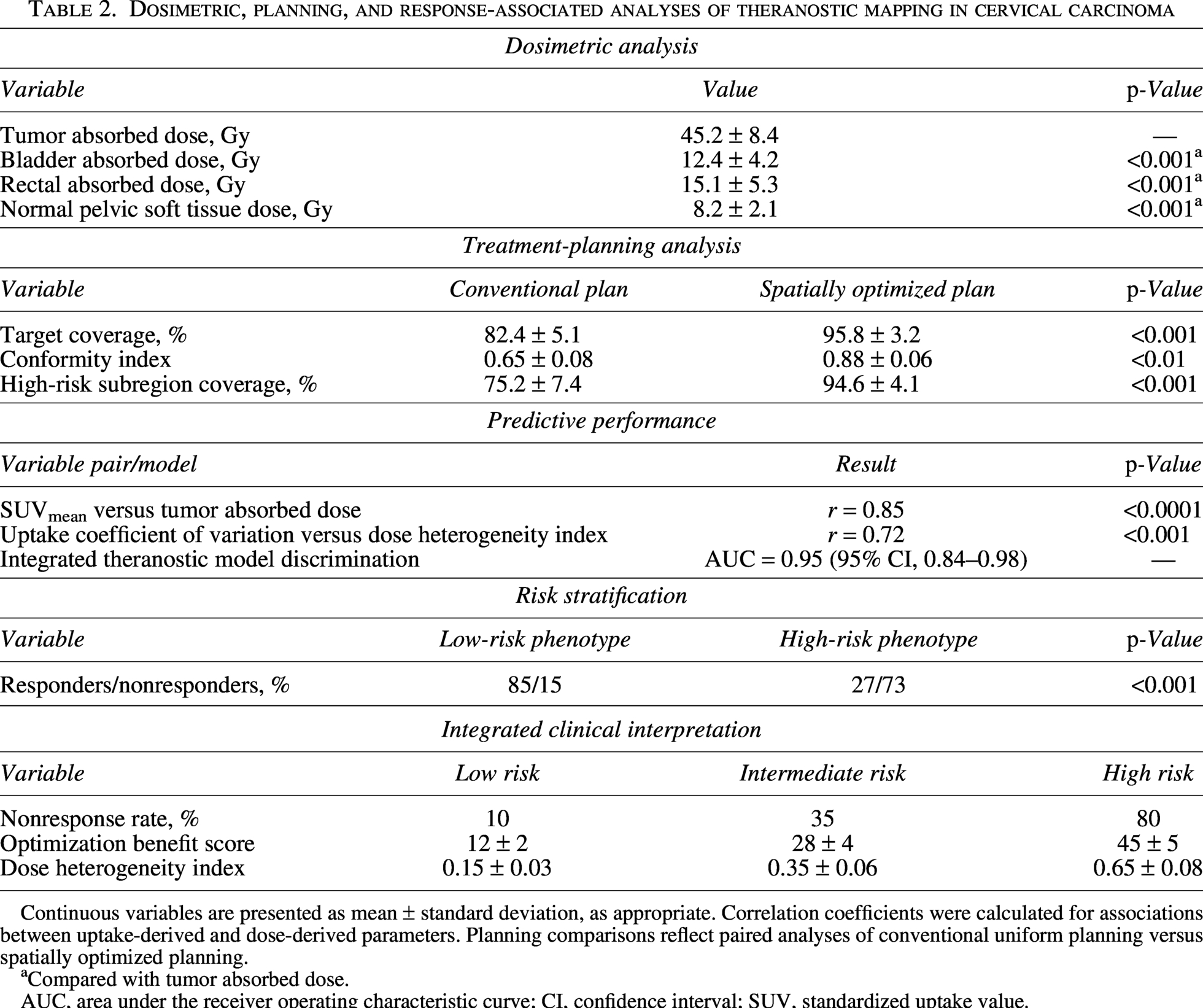
Continuous variables are presented as mean ± standard deviation, as appropriate. Correlation coefficients were calculated for associations between uptake-derived and dose-derived parameters. Planning comparisons reflect paired analyses of conventional uniform planning versus spatially optimized planning.
Compared with tumor absorbed dose.
AUC, area under the receiver operating characteristic curve; CI, confidence interval; SUV, standardized uptake value.
The correlation results indicated a strong positive relationship between SUVmean and tumor-absorbed dose (Fig. 3C), supporting the relationship between uptake intensity and modeled intratumoral dose deposition. There was also a positive association between uptake coefficient of variation and dose heterogeneity index indicating that increased uptake nonuniformity was characterized by increased spatial variation of the absorbed dose. Based on these findings, the relationship between imaging-defined heterogeneity and individualized dosimetric behavior is biologically relevant.
Spatially optimized planning improves target coverage and conformity
Comparison between representative plans revealed that the traditional uniform planning method resulted in relative undercoverage of high-uptake tumor subregions and incomplete alignment between the biologically target areas and the dose delivered. By contrast, theranostic-guided spatial optimization enhanced targeting of the high-risk intratumoral regions and delivered more focused dose deposition while improving biological targeting relative to anatomically uniform planning (Fig. 4A). Importantly, prioritization of high-uptake subregions must be interpreted within the context of competing dose constraints in adjacent pelvic organs, including the bladder and rectum. Therefore, theranostic-guided optimization should be viewed as a constrained redistribution strategy rather than an unrestricted dose escalation, requiring integration with established normal tissue tolerance thresholds in clinical implementation.
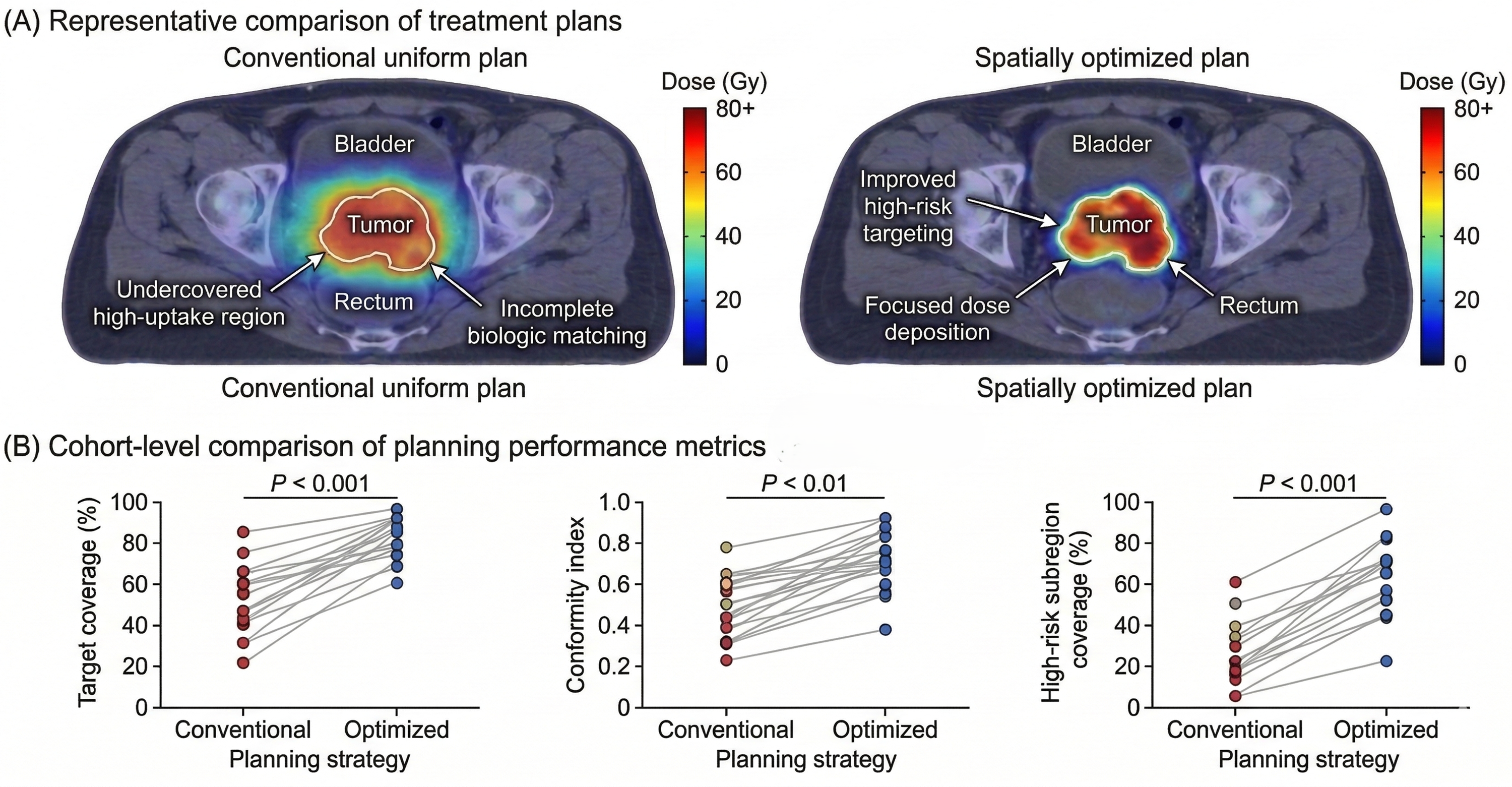
Spatially optimized treatment planning improves target coverage and conformity in cervical carcinoma.
Spatial optimization at the cohort level led to a high target coverage, conformity index, and high-risk subregion coverage with improved coverage than the conventional uniform planning (Fig. 4B). These observations suggest that the coverage of biologically relevant targets can be enhanced by the inclusion of spatial theranostic information compared with the coverage of biologically relevant targets obtained with a uniform planning strategy.
Response association and predictive performance of the integrated theranostic score
The integrated theranostic score showed a clear difference between the responders and nonresponders, with higher scores observed in the nonresponder group (Fig. 5A). This segregation was in line with the summary of baseline disparities in uptake intensity, heterogeneity, and high-uptake fraction.
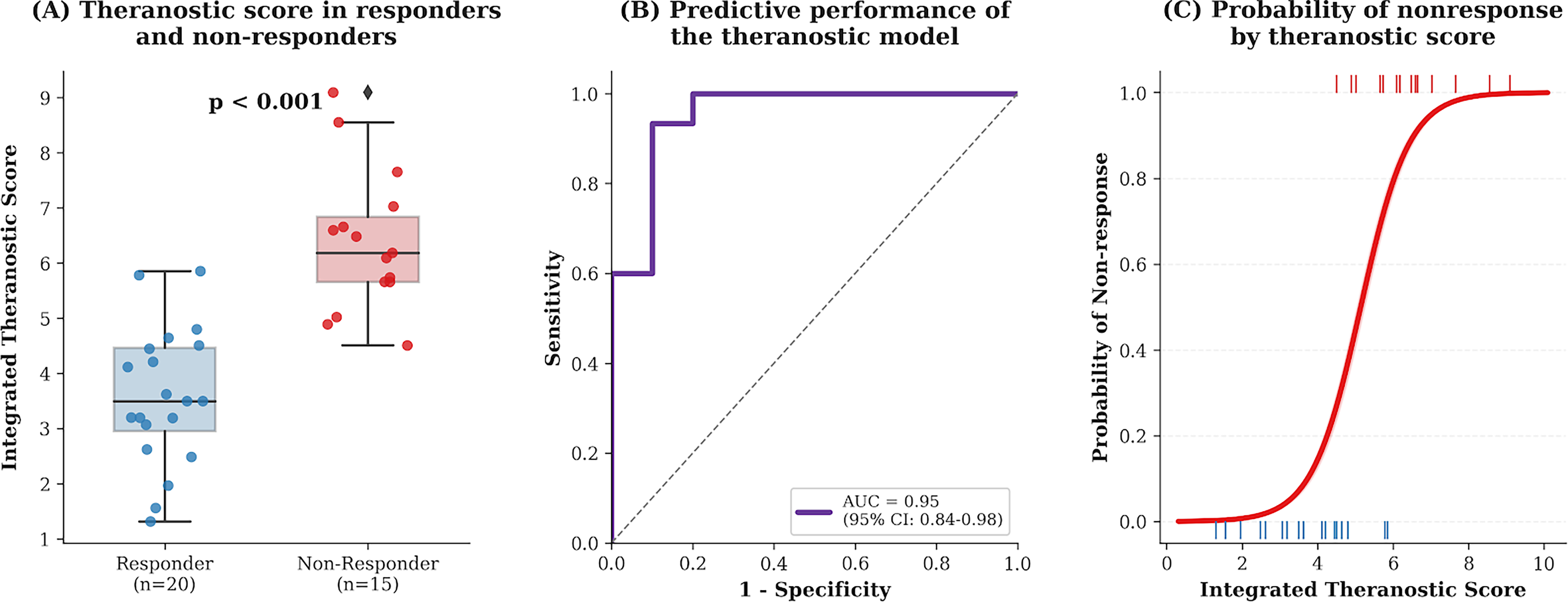
Association of spatial theranostic features with treatment response in cervical carcinoma.
The integrated theranostic model was able to perform exceptionally in response classification with the analysis of receiver operating characteristics having an area under the curve of 0.95 (95% CI, 0.84–0.98) (Fig. 5B). Logistic regression analysis also revealed that the predicted nonresponse probability rose steadily with an increasing integrated theranostic score (Fig. 5C), which argues continuous estimation of patient-specific risks, as opposed to a dichotomous one. This continuous risk representation supports potential clinical application of the integrated score as a decision-support tool, enabling identification of patients who may benefit from intensified treatment, closer monitoring, or adaptive planning strategies based on individualized theranostic risk profiles.
Phenotype-based risk stratification and integrated clinical interpretation
The unsupervised clustering of standardized theranostic features gave two different phenotypic groups (low-risk and high-risk signatures) (Fig. 6A). There was a significant difference in response distribution between these groups, with a significantly higher percentage of no response in high-risk phenotype (Fig. 6B).
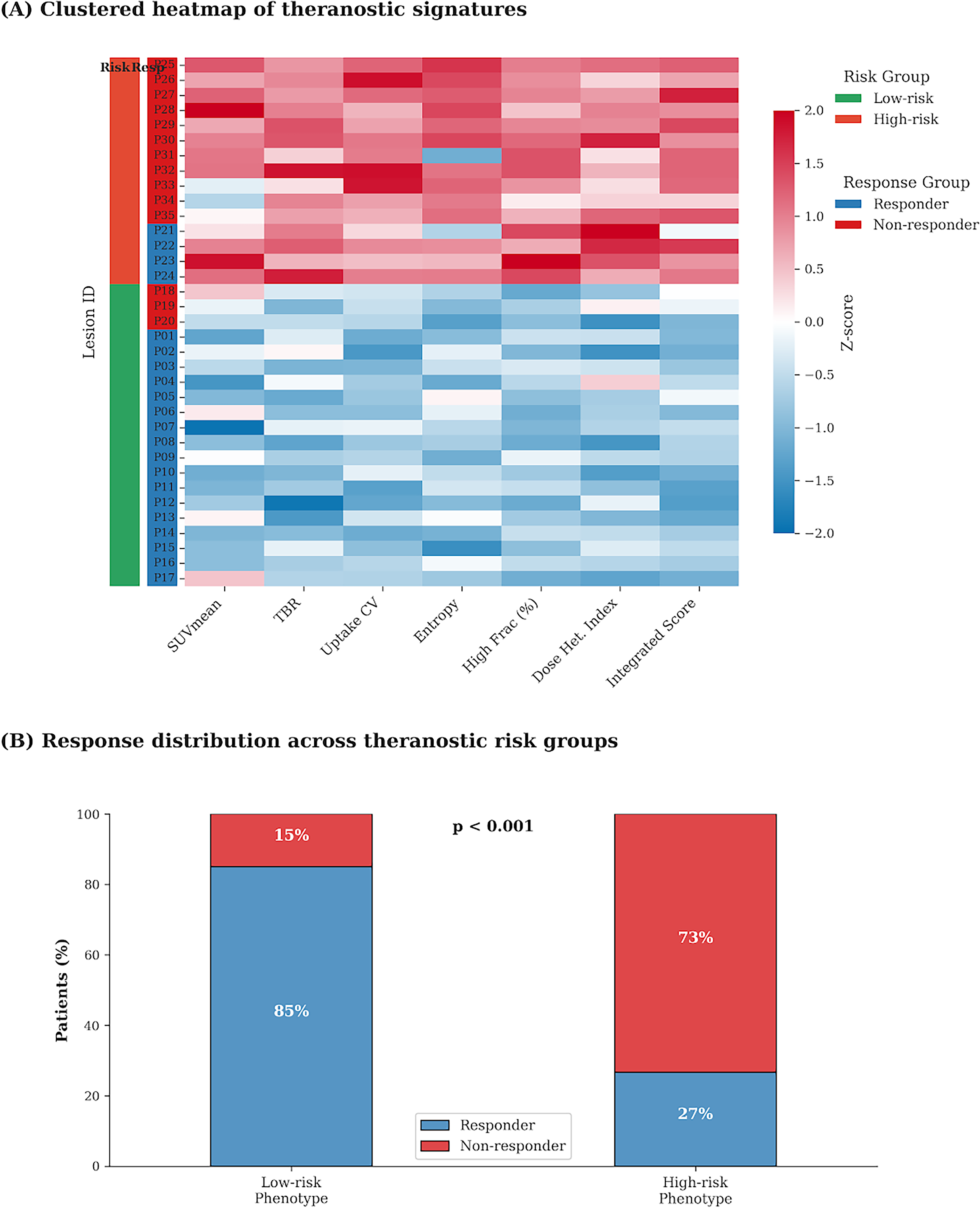
Spatial risk stratification based on theranostic mapping signatures in cervical carcinoma.
The visualization of the integrated theranostic score in the ranked form also showed a continuum between the low-risk and high-risk patient profiles, with greater scores focused on nonresponders (Fig. 7A). There were progressive differences in nonresponse rate, optimization benefit, and dose heterogeneity index across the low-, intermediate-, and high-risk groups (Fig. 7B). Taken together, these results suggest that the theranostic framework has clinically interpretable stratification of biological aggressiveness, dosimetric complexity, and benefit in planning cervical carcinoma.
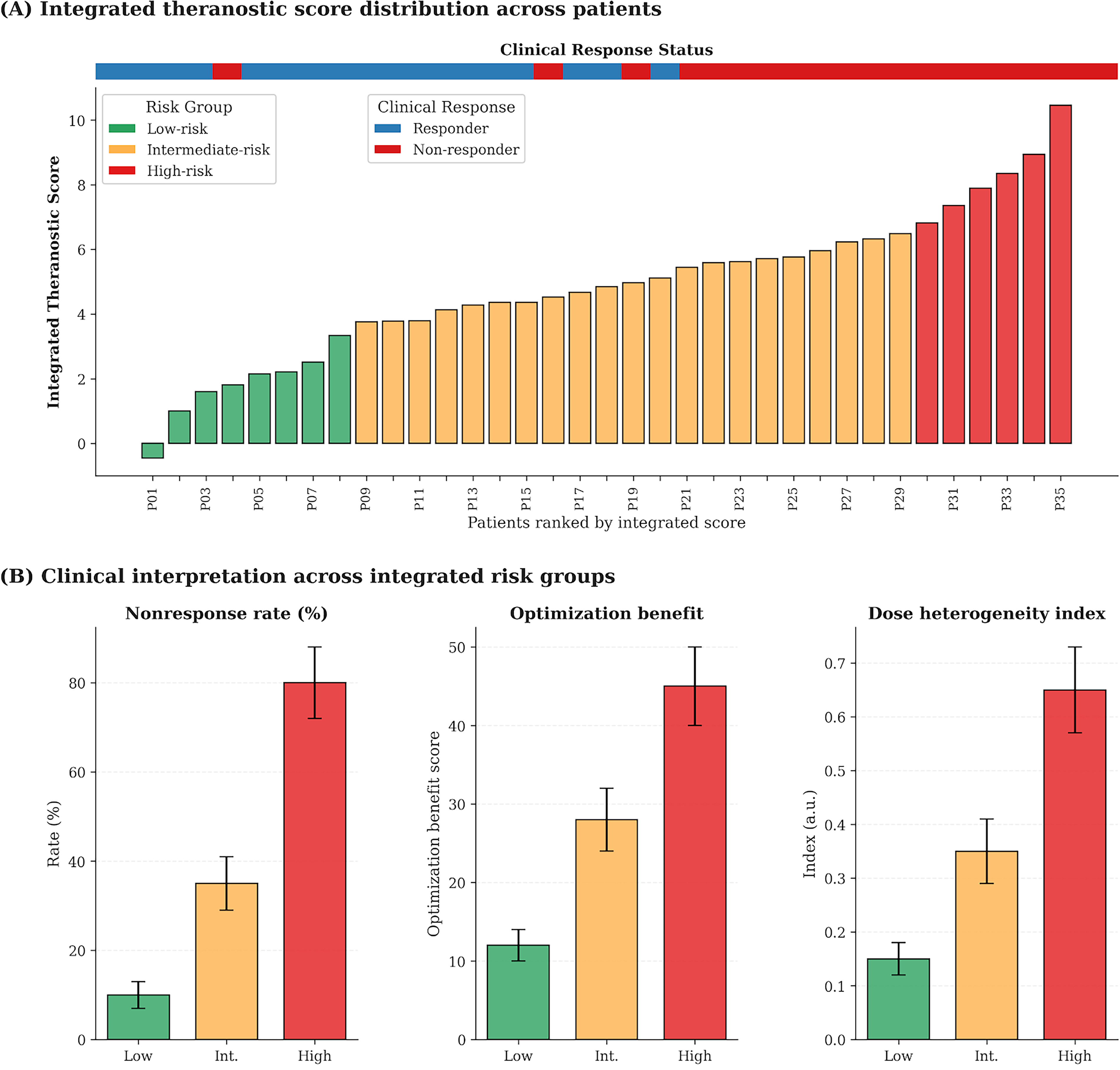
Integrated clinical interpretation of radionuclide theranostic mapping in cervical carcinoma.
Discussion
This study demonstrates that radionuclide theranostic mapping can capture clinically relevant intratumoral heterogeneity in cervical carcinoma and translate that heterogeneity into absorbed dose nonuniformity, treatment-planning benefit, and response stratification. The observed differences between responders and nonresponders across uptake intensity, heterogeneity, intratumoral composition, and the integrated score support the principle that medical images contain quantifiable phenotypic information beyond visual interpretation.18,19 In this setting, the combined evaluation of voxel-level uptake structure, dose heterogeneity, and integrated theranostic scoring provides a practical framework for translating functional imaging into clinically interpretable biomarkers. From a clinical perspective, higher uptake intensity and greater spatial heterogeneity may reflect regions of increased tumor aggressiveness, variable perfusion, or differential radiosensitivity, whereas more homogeneous uptake patterns may indicate more uniform treatment susceptibility. Accordingly, heterogeneity metrics can be interpreted as indicators of potential intratumoral resistance patterns and targets for spatially adaptive intervention. The strong association between SUVmean and tumor absorbed dose, together with the positive relationship between uptake coefficient of variation and dose heterogeneity index, further supports the biological and dosimetric relevance of imaging-defined spatial heterogeneity for individualized treatment assessment. 20
A key finding of the present study is that theranostic-guided spatial optimization improved target coverage, conformity, and high-risk subregion coverage compared with conventional uniform planning. Importantly, these improvements should be interpreted within the context of competing normal tissue constraints, particularly in the pelvic setting where bladder and rectal tolerance limit the extent of dose redistribution. The present framework demonstrates the feasibility of biologically informed dose adaptation while maintaining acceptable normal tissue exposure, but prospective evaluation incorporating explicit dose–volume constraints is required to establish clinical applicability. These results extend established image-guided planning concepts by defining the high-risk target not solely on anatomical grounds but on spatially heterogeneous uptake behavior within the lesion. 21 Such an approach is particularly relevant in cervical carcinoma, where bulky tumors, resistant subregions, and close proximity to dose-limiting pelvic organs complicate treatment individualization. In this context, the proposed theranostic framework can be viewed as an extension of established radiotherapy paradigms, including biologically guided dose painting and image-guided adaptive therapy, and may complement systemic treatment strategies by providing imaging-derived biomarkers for risk stratification and response prediction within precision oncology workflows. The present findings also support a broader theranostic treatment model in which diagnostic tracer distribution is used not only for lesion identification but also for biologically informed dose design. This concept is consistent with the growing emphasis in radiopharmaceutical therapy on individualized dosimetry, imaging-guided optimization, and patient-specific therapeutic planning rather than reliance on fixed activity alone. 22 In addition, the phenotype clustering and ranked risk-group analyses suggest that patients with greater heterogeneity and higher integrated score may derive greater benefit from spatial optimization, indicating that heterogeneity may function both as a risk marker and as an actionable planning target.
Several limitations should be considered when interpreting these findings. First, the analysis was based on baseline theranostic imaging and does not capture the temporal evolution of intratumoral heterogeneity during or after treatment. Longitudinal imaging could provide additional insight into dynamic changes in uptake patterns, dose redistribution effects, and treatment response and represents an important direction for future investigation. The cohort was modest in size, and although the integrated theranostic score showed strong discriminative performance, prediction modeling in small datasets remains vulnerable to optimism and limited generalizability. Accordingly, the present model should be viewed as a translational and hypothesis-generating framework requiring prospective validation in larger and ideally multi-institutional cohorts with harmonized imaging, segmentation, and dosimetry workflows. 23 In addition, feature estimates and voxel-level dose calculations may be influenced by acquisition parameters, reconstruction methods, contouring choices, and modeling assumptions, all of which should be formally assessed in future robustness studies. Response classification was based on standardized clinical and imaging assessment, but variability in timing and follow-up methodology may still affect outcome categorization; where appropriate, integration of functional response endpoints may provide complementary biological information beyond conventional anatomical assessment. 24 More broadly, the relevance of this framework is supported by clinical experience in other theranostic settings, including peptide receptor radionuclide therapy, where uptake variability, dosimetric diversity, and response heterogeneity have already highlighted the value of individualized treatment strategies. 22 Future work should therefore focus not only on model discrimination but also on clinical utility, including whether score-guided stratification can improve treatment decisions and decision-analytic benefit in real practice. 25
Conclusions
Radionuclide-based theranostic mapping in cervical carcinoma quantified spatial intratumoral heterogeneity, demonstrated strong uptake–dose associations, and identified absorbed dose nonuniformity relevant to individualized dosimetric assessment. Theranostic-guided spatial optimization improved target coverage, conformity, and high-risk subregion coverage compared with conventional uniform planning. In addition, the integrated theranostic score enabled response prediction and clinically interpretable risk stratification, supporting a translational framework for personalized imaging-guided treatment planning in precision oncology with potential to inform risk-adapted treatment strategies and biologically guided dose optimization in future clinical workflows.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Heilongjiang University of Chinese Medicine (Ethics No.: YJSKY2024-194).
Authors’ Contributions
L.L.: Conceptualization, methodology, data curation, formal analysis, and writing—original draft preparation. L.F.: Investigation, software, data curation, and visualization. Y.Z.: Methodology, validation, and formal analysis. H.C.: Investigation, experimental work, and resources. Q.L.: Supervision, project administration, and funding acquisition. S.L.: Conceptualization, supervision, writing—review and editing, and project administration.
Footnotes
Disclosure Statement
The authors declare that they have no conflicts of interest related to this research.
Funding Information
The study was supported by the