
Abstract
Keywords
Although stimulant medications have been used successfully for decades to improve the behavioral impairments of hyperactivity, impulsivity, and inattention in children diagnosed with ADHD, it has repeatedly been shown that such drugs do not normalize their ability to learn and apply knowledge (Barkley & Cunningham, 1978; Cantwell & Satterfield, 1978; Carlson & Bunner, 1993; Gadow, 1983; Gualtieri & Johnson, 2008; Loe & Feldman, 2007; Swanson, Cantwell, Lerner, McBurnett, & Hanna, 1991). By the time they reach adolescence, individuals with ADHD fail more grades, have lower report card scores, lower class rankings, and worse scores on standardized achievement tests than “matched normal controls.” They take more years to complete high school and have lower rates of college attendance and graduation.
Nevertheless, the recognition that ADHD persists into adulthood (Kessler et al., 2006) has substantially increased the pharmacological treatment of adults with ADHD (Davidson, 2008; Dodson, 2005; Dopheide & Plizka, 2009 Faraone, Spencer, Aleardi, Pagano, & Biederman, 2004; Pliszka, 2007; Robison, Sclar, & Skaer, 2005), particularly in undergraduate populations (see Wilens et al., 2008, for review). Concern about such escalating use has prompted several recent surveys, all showing that most students report using stimulant medications, licitly or illicitly, to improve academic performance, specifically to increase concentration, organization, and the ability to stay up longer and study (Advokat, Martino, & Guidry, 2008; Aldhous, 2006; Barkley, Fletcher, Fischer, & Smallish, 2003; Blase, et al., 2009; Rabiner, Anastopoulos, Costello, Hoyle, McCabe et al., 2009; Rabiner, Anastopoulos, Costello, Hoyle, & Swartzwelder, 2008; 2009; Teter, McCabe, Cranford, Boyd, & Guthrie, 2005; White, Becker-Blease, & Grace-Bishop, 2006; Wilens et al., 2008). This development has raised concerns about the prevalence of stimulant diversion and misuse among undergraduates and other adults and initiated debate about the ethical implications of using drugs to improve academic performance. Expressed in terms of the morality of “cognitive enhancement,” this issue has been the subject of several recent editorials (Butcher, 2003; Farah et al., 2004; Greely et al., 2008; Harris, 2009; Monastersky, 2008; Sahakian & Morein-Zamir, 2007).
Such concern seems ironic in the face of so much evidence that the currently available drugs don’t make you “smarter,” or at least, don’t “normalize” the long-term academic accomplishments of ADHD-diagnosed children and adolescents. Intuitively, it would seem logical that drugs that improve attention and concentration would improve learning and academic achievement. Yet for more than 30 years, the data show that this is not the case (Advokat, 2009). These considerations prompted our investigations of the cognitive effects of stimulant medications, with the goal of gaining insight into their lack of long-term, intellectual effectiveness.
The purpose of this initial study was to obtain information about the academic behavior of college students with, and without, an ADHD diagnosis. Because youth diagnosed with ADHD are less likely to attend college than others in their cohort, ADHD-diagnosed undergraduates are a unique subset of all adults with the disorder. It was possible that they might have developed ways of gaining more intellectual benefit from stimulant medications than other adults with this condition. If so, it would be of interest to find out how they were able to make such good use of the drugs in pursuing their academic goals so that their strategies could be broadly implemented. On the other hand, in view of growing concerns about escalating abuse and diversion of the drugs, it would be equally important to know whether stimulant medications did not provide any academic advantage for ADHD-diagnosed undergraduates.
In this study, we compared the self-reported study habits and strategies of ADHD-diagnosed and nondiagnosed undergraduates, to determine whether they differed in response to the academic demands of the college curriculum. We administered a questionnaire to find out whether there was a substantial difference in how these two groups approached their schoolwork and whether there was any corresponding difference in their respective grade point averages (GPA).
Method
Undergraduate college students were recruited through the psychology department extracredit system. Respondents received extra credit in their respective classes for completing the survey; some also received US$5.00 when they participated in an additional phase of the experiment involving computer-based cognitive tasks. For participants with ADHD, criteria to participate included a self-report of the clinical diagnosis and a current prescription for ADHD medication.
The Academic Assessment of College Students Questionnaire was created by CA and SL to obtain information about the study habits of college students with and without a diagnosis of ADHD. It includes 40 questions; some were demographic, and some concerned the ADHD diagnosis and treatment, with most of the questions addressing academic strategies. The first section of the survey concerns information about ADHD (e.g., “At what age did you receive the diagnosis?”). Four of the academic strategy questions (deciding what to study, studying for different types of exams, reading textbooks, and motivation for self-quizzing) were taken or modified from a survey developed by Kornell and Bjork (2007). These questions have generously been made available for use in the public domain. All procedures of this study were approved by the institutional review board of Louisiana State University. A copy of the survey is available on request.
To compare the group differences, one- and two-way ANOVAs were used for parametric variables and Pearson chi-square tests were used for nonparametric variables. All statistical tests were two tailed, with an alpha level of .05 for statistical significance. All analyses were carried out using the Statistical Package for Social Sciences 15.0 for Windows.
Results
A total of 143 students without ADHD (control group) and 92 students with an ADHD diagnosis (ADHD group) completed the survey. As shown in Table 1, the average age of the two groups, approximately 21 years, did not differ, and most participants in each group were White (81.8% and 89.1% for control and ADHD, respectively), although there were significantly more men in the ADHD group (38% compared to 17.5%). Significantly more control participants (79.7%) than ADHD participants (65%) had a job during the semester, although the number of hours worked per week was the same for the two groups (19.6 and 18.0, respectively). On the other hand, ADHD respondents were more likely to belong to a Greek organization (27.25% compared to 15.4%, respectively), although the groups did not differ in regard to the number who joined other organizations/clubs or in the number of other organizations/clubs they joined. The ADHD group was more likely to smoke. Although there was no difference in the percentage of each group who drank alcohol, those in the ADHD group drank significantly more per week. However, this difference in smoking and amount of drinking could be confounded by the fact that there were statistically more men in the ADHD group.
Respondent Characteristics*
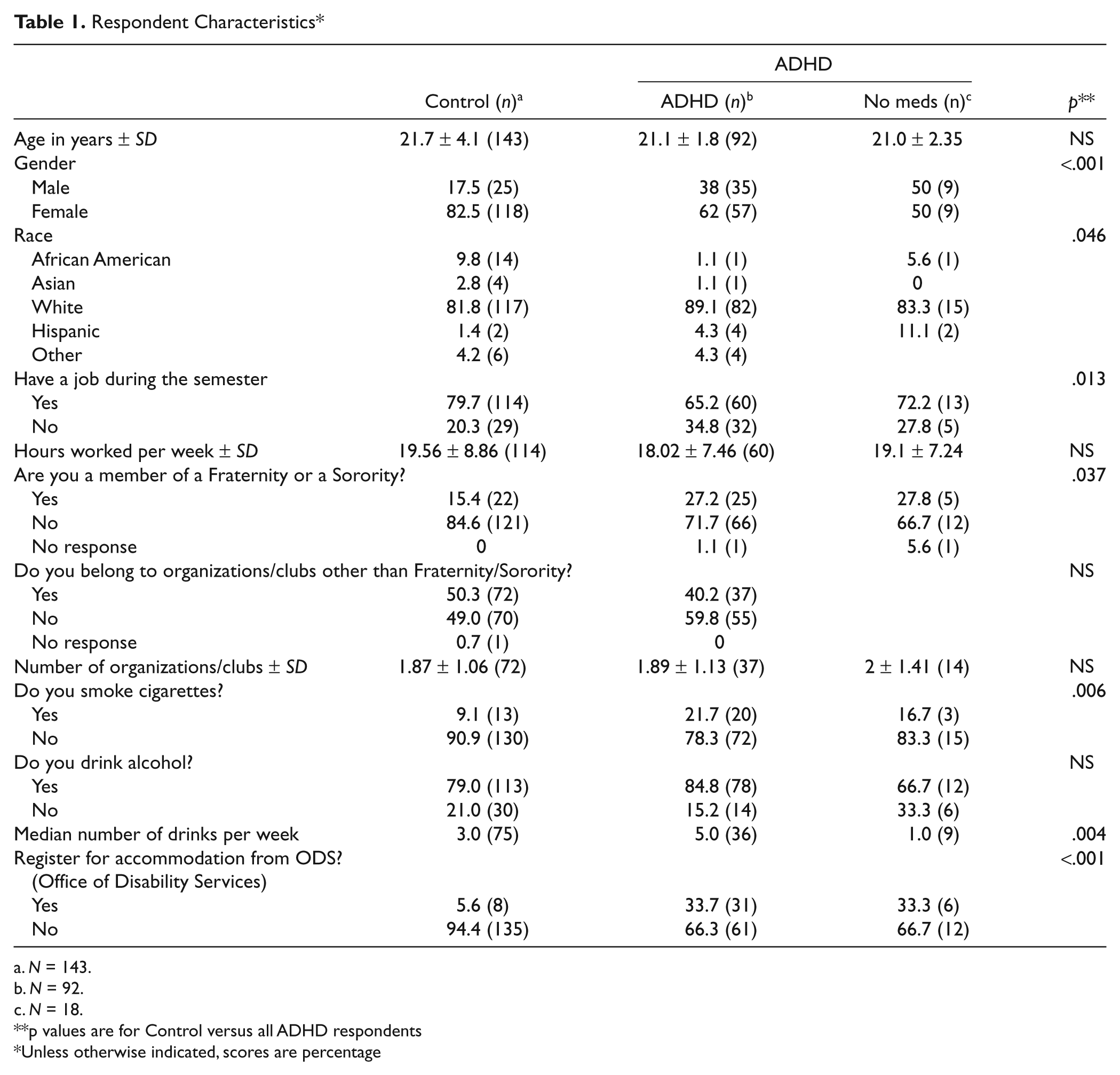
N = 143.
N = 92.
N = 18.
p values are for Control versus all ADHD respondents
Unless otherwise indicated, scores are percentage
Table 2 summarizes the clinical characteristics of college students with ADHD. The average age at which the participants received the diagnosis was between 15 and 16 years; out of 88 respondents who answered the question, 66 stated that they were first diagnosed between the ages of 13 and 19, even though one of the criteria for the disorder is a childhood diagnosis (Diagnostic and Statistical Manual of Mental Disorders [4th ed., Text Revision; DSM IV-TR; American Psychiatric Association, 2000]). Nevertheless, this means that most ADHD students had the diagnosis for about 5 years before they started college. Not surprisingly, most of the ADHD group, more than 50%, had the inattentive subtype, whereas 25% had the combined subtype of ADHD, with only 7.6% given the diagnosis of hyperactive only. However, 14% said they didn’t know what type of ADHD they were diagnosed with. Although nearly 98% had taken ADHD medication, only 78.3% (72 respondents) were currently using the drugs, whereas 19.6% (18 respondents) stated that they were not currently taking the medications. When asked why they might not be taking stimulant medications, the majority cited the problem of side effects. Although specific side effects were not always mentioned (“I did not like the way it made me feel; . . . make me feel crappy; the negative side effects out weigh the positives”), some individuals cited headaches, irritability, temporary heart rate elevation, nausea, sleep interference, and “antisocial” feelings as examples of undesirable reactions. Nearly one third of this subgroup also stated that they either didn’t need the drugs anymore or they wanted to see whether they didn’t need them anymore.
Clinical Characteristics of College Students With ADHD*
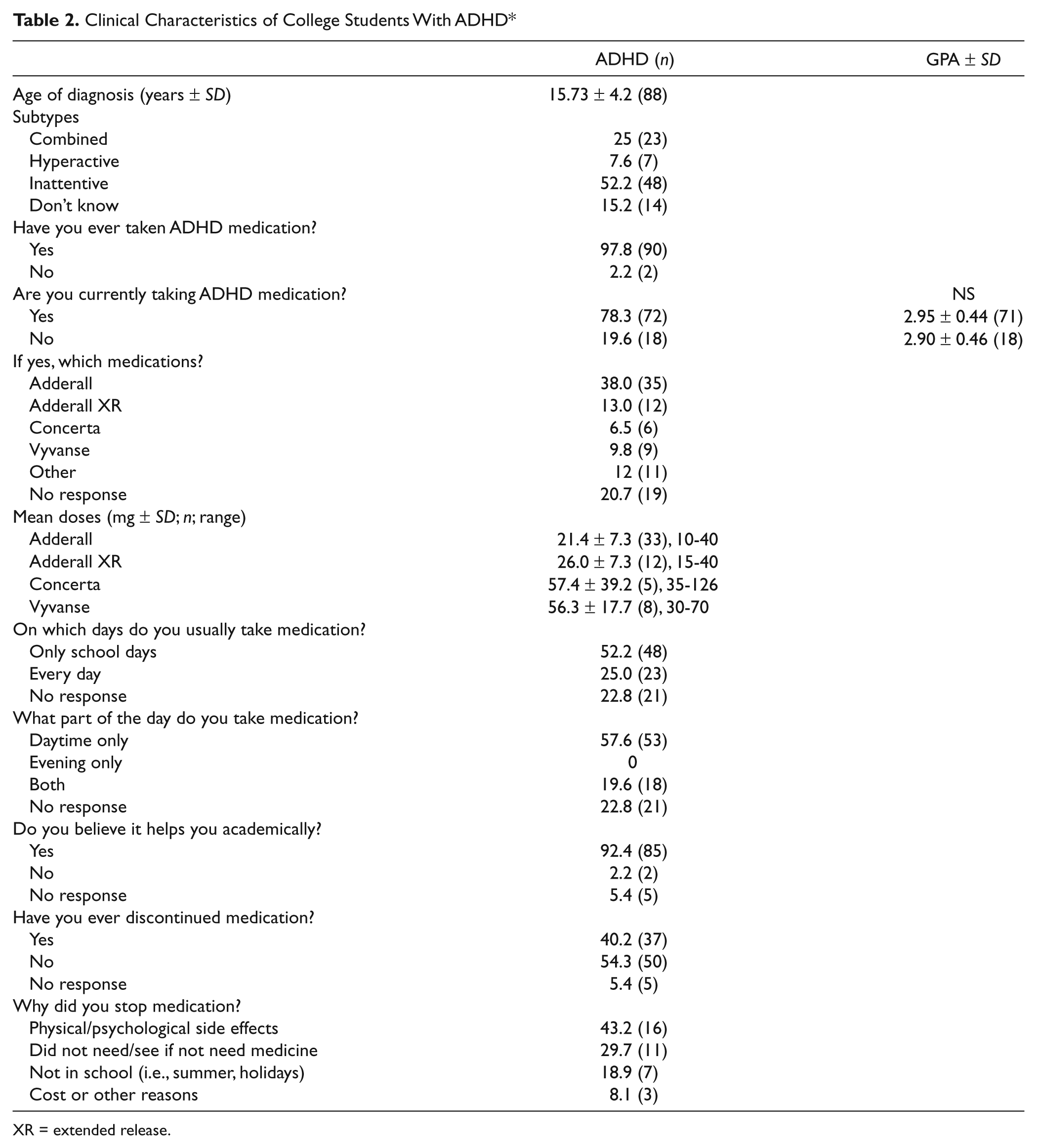
XR = extended release.
With regard to specific medications, most ADHD students used the amphetamine agent, Adderall, with most of those stating that they used the short-acting formulation rather than the extended release (XR) version. However, a substantial proportion of those who said they took medication, nearly 21%, did not answer this question. The average doses provided by the respondents were in the recommended ranges. Maximum recommended adult daily dosages are 40 mg for Adderall, 20 mg for Adderall XR, 70 mg for Vyvanse, and 72 mg for Concerta. However, 9 out of 12 students taking Adderall XR exceeded the maximum daily dosage of 20 mg, and 1 out of 5 students taking Concerta exceeded the maximum daily dosage of 72 mg.
More than 90% of the students with ADHD endorsed the statement that medications help them academically. Most of them stated that the drugs help them focus or concentrate better, that is, pay attention, stay awake, avoid distractions, and organize their studying. However, relatively few students (n = 6) with ADHD specifically stated that they took medication to avoid distractions. These responses are generally consistent with the fact that most respondents stated that they used the stimulants only during the day and mostly on school days. Nevertheless, a substantial subgroup either did not answer these questions (21 respondents), used the drugs throughout the day (18 respondents), or every day (23 respondents).
Table 3 summarizes the academic variables on which the control and ADHD groups did not differ. (Responses from 2 or fewer participants are not listed on this and subsequent tables, for the sake of clarity).
Academic Variables That Did Not Differ Between Controls and ADHD-Diagnosed College Students*
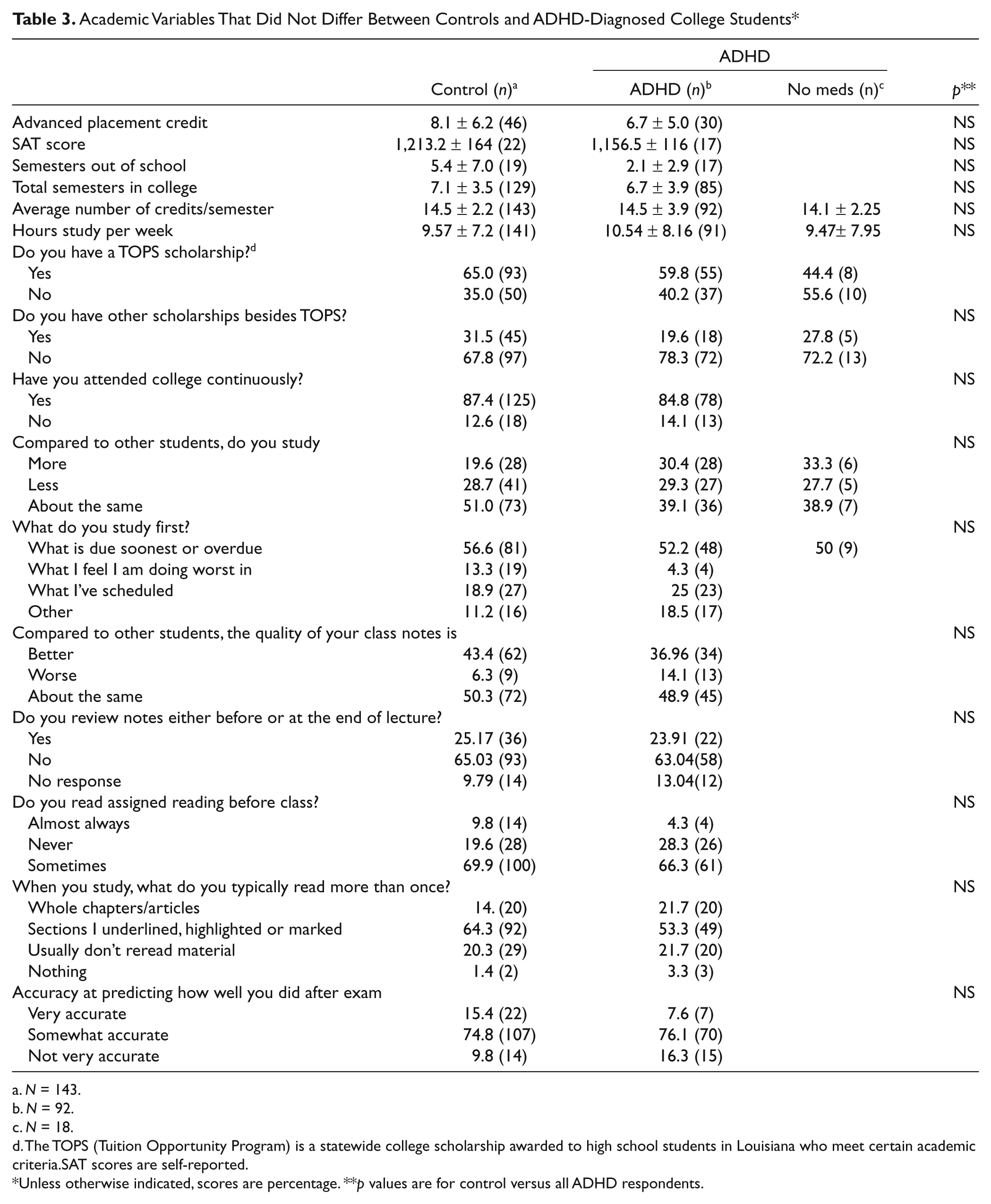
N = 143.
N = 92.
N = 18.
The TOPS (Tuition Opportunity Program) is a statewide college scholarship awarded to high school students in Louisiana who meet certain academic criteria.SAT scores are self-reported.
Unless otherwise indicated, scores are percentage. **p values are for control versus all ADHD respondents.
Control and ADHD students took the same amount of advanced placement credits (an average of 8.1 for the controls and 6.7 for ADHD students). For those few who took the SAT test in each group, there was no difference in their self-reported SAT scores. They did not differ in the number of scholarships awarded, were enrolled for the same number of semesters (between 6 and 7), took the same number of credits per semester (about 14.5), and studied the same number of hours per week (about 9.5 to 10.5). ADHD students did not differ significantly from controls in comparing themselves to other students with respect to: How much they study (consistent with the finding they reported studying a similar number of hours), what material they studied first (i.e., whatever was due soonest or was overdue), the perceived quality of their class notes, and whether they reviewed their notes), whether they read assignments ahead of time (both groups rarely did that) and whether they reread material when they studied (again, this rarely happened), how accurately they predicted their test performance.
Although not listed in Table 3, controls and ADHD students were also comparable when asked what they did to avoid distraction while studying. Most of them stated they studied alone or went to a quiet place, typically the library. Some students used ear plugs or listened to music to block distractions. Other strategies included turning off the TV/computer/cell phone/or other electronics and taking timed breaks.
Academic variables on which the two groups differed are summarized in Table 4. ADHD students had a significantly lower high school GPA and ACT (American College Testing) score than controls. Although small, this difference was detected in spite of the fact that a minimum high school GPA and ACT score were required for admission to the university. The LSU (Louisiana State University) GPA of ADHD students was also statistically lower than that of the controls. ADHD students were significantly more likely to withdraw from a class, to say that they were worse than other students at planning for and completing class assignments, at frequently taking class notes at studying ahead of time for exams, and at avoiding distractions.
Academic Variables That Differed Between Controls and ADHD-Diagnosed College Students*
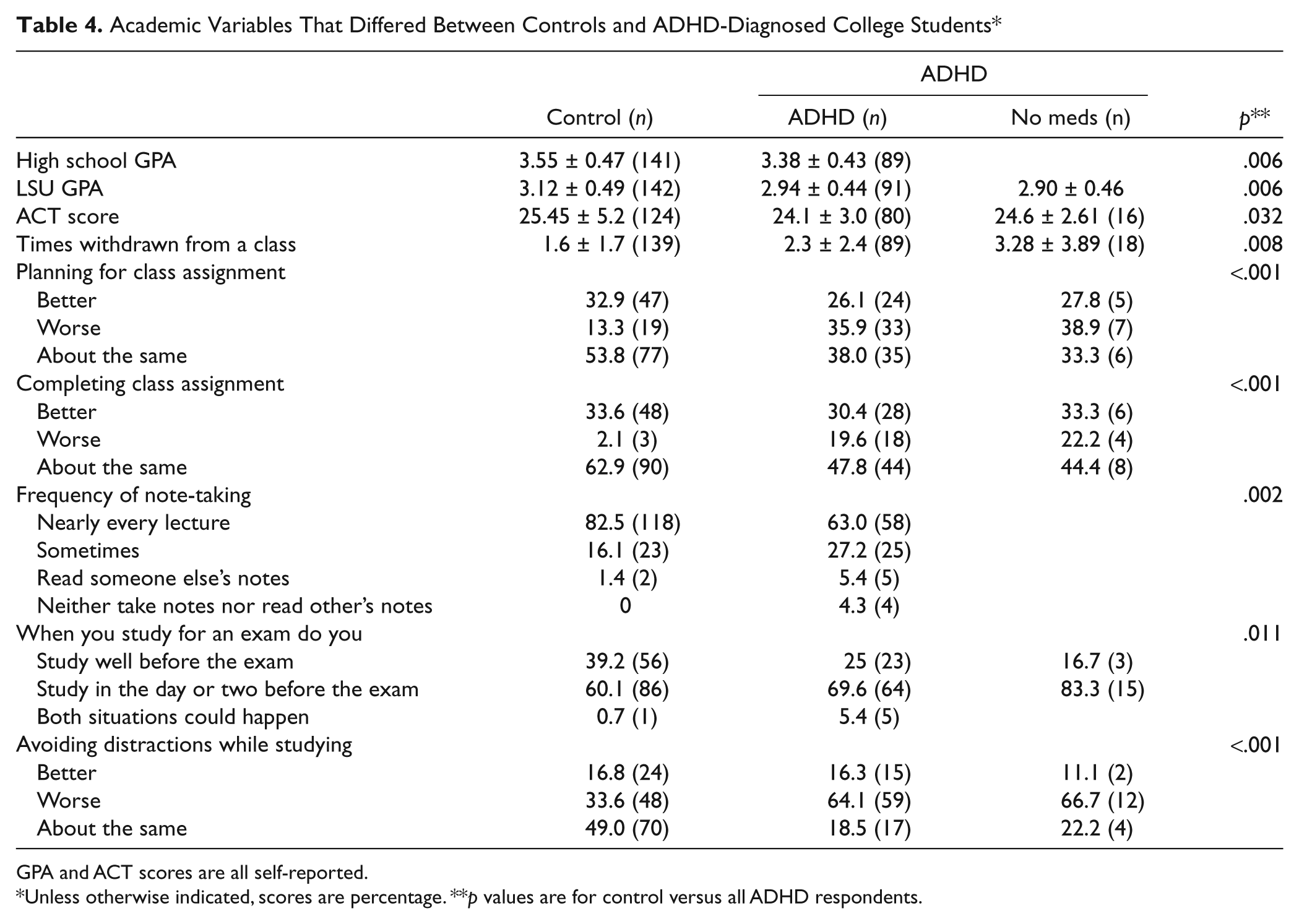
GPA and ACT scores are all self-reported.
Unless otherwise indicated, scores are percentage. **p values are for control versus all ADHD respondents.
These results show that control and ADHD-diagnosed students differ in some of their self-reported study habits. But these data alone don’t tell us whether these endorsements are relevant to the academic achievement of either group. In other words, we didn’t know whether the statistically significant differences in professed study habits were related to the respective GPAs. We, therefore, analyzed the answers to some of the questions on which the two groups differed (Table 4), as a function of GPA. The results are summarized in Table 5. As indicated, there were significant differences within the groups, as a function of whether the students said they were “Better, Worse, or About the Same as other students” on several measures. In the control group, there was a significant difference in GPA among students with respect to “planning for” and “completing” class assignments, “frequency of note taking,” and “avoiding distractions while studying.” Post hoc analyses revealed that students who state they are “better” at planning and completing assignments, who take frequent notes in class, and who avoid distractions have higher GPAs than those who say they are average or worse at these tasks. However, the GPA of these control students did not differ as a function of whether or not they said that they studied “ahead of time” or just days before an exam.
Factors Affecting College GPA ± SD (n) of Control and ADHD-Diagnosed Students
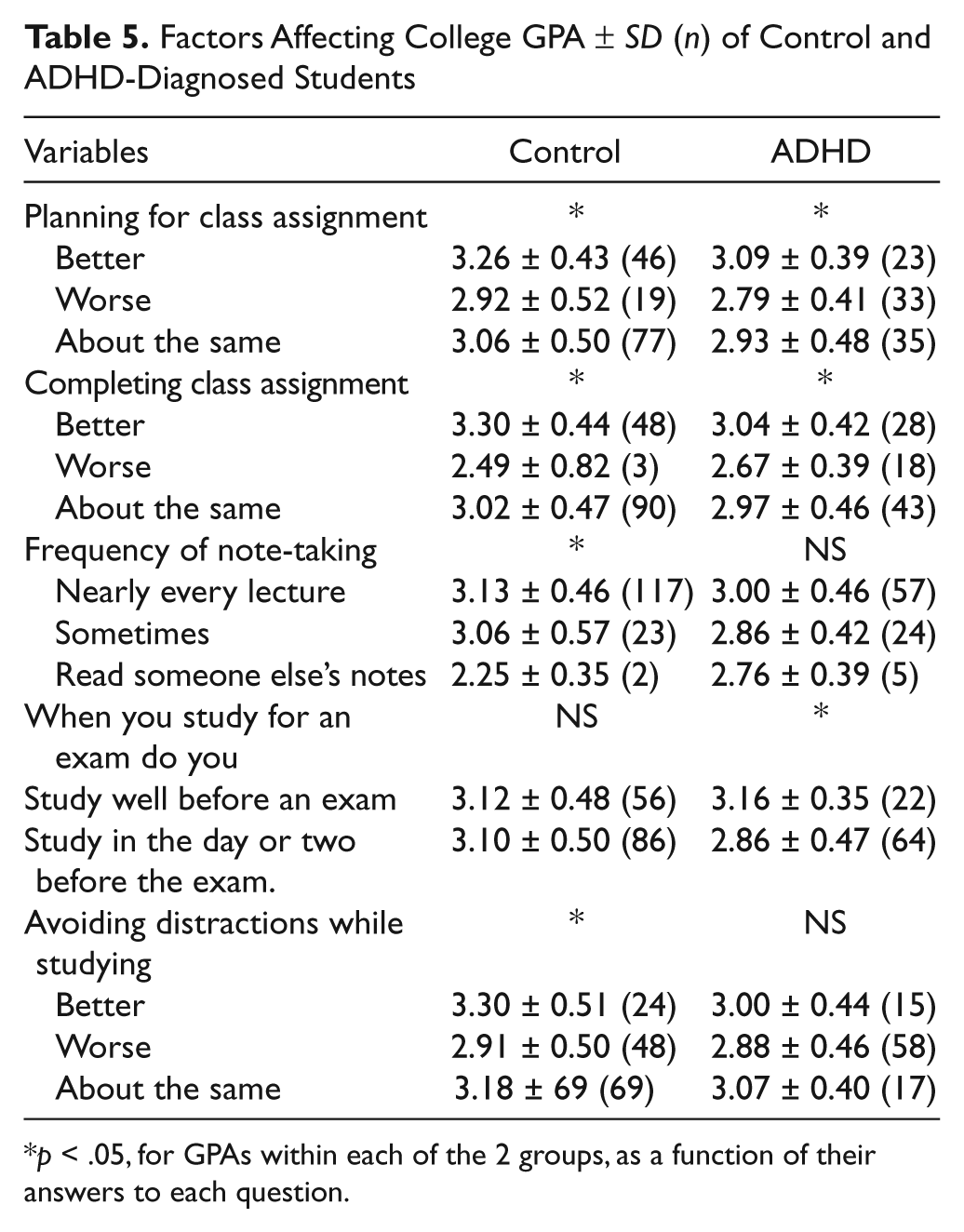
p < .05, for GPAs within each of the 2 groups, as a function of their answers to each question.
The GPA averages of ADHD students, like the scores of the control students, were statistically different with respect to planning for and completing class assignments, even though their overall GPA was lower than that of controls. However, unlike control students, there was no difference in GPA of ADHD students as a function of how often they took class notes or in how well they thought they could avoid distractions. Students with ADHD who believe they take notes more often, or can avoid distractions, did not have a better GPA than those who say they don’t. Conversely, also unlike in the control group, the GPA of ADHD students who stated that they studied “well before” an exam, was significantly higher than the GPA of those (the majority of this group) who said they study in the “day or two before an exam.” We also compared GPAs within the group of ADHD students as a function of when they took their medication (Table 2), to see whether there was an effect of the weekly duration of drug exposure. There was no difference between the 48 ADHD students who said they usually took medication during the school day (2.97 ± 0.47) and the 22 students who said they used the drugs every day (2.92 ± 0.39).
Although the data described so far did not appear to show much evidence for a cognitive benefit of medications in ADHD-diagnosed students, we appreciated the fact that not all of those undergraduates were taking the drugs. Because we had asked the students whether they were taking ADHD medications, we could distinguish between those ADHD students who said they did (n = 72) from the smaller group, who said they didn’t (n = 18). As shown in Table 2, there was no difference between these two subgroups in GPA. Furthermore, the GPA of the ADHD students who took the medications was still significantly lower than the Control group GPA (p = .022).
The existence of these subgroups allowed us to make some additional preliminary analyses. Specifically, we compared the GPA of ADHD students who did or did not take the drugs, as a function of whether or not they studied ahead of time for exams. This resulted in four groups, with the following GPAs: those who took the medications and did not study ahead of time (n = 47), 2.88 ± 0.48; those who used the drugs and did study early (n = 19), 3.15 ± 0.35; those who did not take the medications and did not study ahead of time (n = 15), 2.84 ± 0.47; and those few who did not take the drugs but did study early (n = 3), 3.19 ± 0.36. A two-way analysis of these GPAs found no effect of medication, but a statistically significant effect of study interval (F = 4.06, p = .047).
The number of students who stated that they no longer took ADHD medications (n = 18) was too small to perform statistical comparisons of responses to individual questions. However, for the sake of comparison, we included the answers they gave to several of the questions in Tables 3 and 4. In spite of the small number of individuals, there is a striking similarity on many of the measures between ADHD students who self-reported that they took the prescribed medications and those who said they didn’t.
Discussion
Previous research has shown that drug treatment of children with ADHD does not result in any long-term improvement in academic accomplishment. Even when these children become adults, such deficits do not seem to be overcome (Barkley, Fischer, Smallish, & Fletcher, 2006; Biederman, Petty, Fried, Kaiser et al., 2008; Ingram, Hechtman & Morgenstern, 1999; Mannuzza, Klein, Bessler, Malloy, LaPadula, 1993). Adults with ADHD are less likely to attain the same educational (and occupational) level as those without the diagnosis relative to what would be predicted based on their IQ, and this outcome does not appear to be improved by pharmacotherapy. It was possible, however, that the subgroup of ADHD-diagnosed adults who managed to attend college and progress through a typical large, public university, might have a better outcome. This study was conducted to see whether that might be the case.
Moreover, an undergraduate population provides an opportunity to reconsider some of the pharmacological explanations offered for the lack of cognitive benefit previously acknowledged in children and adolescents. One early hypothesis proposed that doses of stimulants required to control the hyperactivity of ADHD-diagnosed children might be greater than doses that are most effective for improving cognition. According to this argument, the amount of drug required to treat the symptom of hyperactivity is “cognitively toxic” and may induce a sort of mental “constriction,” which masks, or prevents, cognitive enhancement (Gadow, 1983). It was also speculated that perhaps the short-acting agents didn’t provide sufficient coverage during a standard school day and that daily variability in blood levels made it difficult to benefit from the intellectual advantages of the drugs.
However, unlike children, college students are less likely to be characterized as hyperactive and more commonly diagnosed with the symptom of inattention (Norwalk, Norvilitis & MacLean, 2008; Rabiner et al., 2008; Schwanz, Palm & Brallier, 2007). This was certainly the case with our population. Given that on average our participants had been diagnosed about 5 years before responding to our survey, at about 16 years of age, it would be reasonable to conclude that they also had sufficient time and experience with the medications to ensure adequate and appropriate dose adjustment. (It should be noted that there is a clinical requirement that at least some ADHD symptoms must be present before the age of 7 years, Diagnostic and Statistical Manual of Mental Disorders [4th ed., Text Revision; DSM IV-TR; American Psychiatric Association, 2000]). Duration of coverage was also less of a problem in this study as long-acting formulations are now available; however, college classes are usually not scheduled all day long. These considerations make arguments about dosage and variability of blood levels less persuasive and would predict greater efficacy in the college population.
Nevertheless, without assessing residual ADHD symptoms, we cannot say that treatment was sufficient and our sample may have had residual ADHD symptoms. This study was not designed to evaluate residual ADHD (e.g., current symptom burden), and that is a limitation. Also, it should be noted that we cannot assume that individuals were correctly treated—in fact, the “recommended doses” that many participants fell within may reflect undertreatment. Considering the outcome of this study, these issues of undertreatment and presence of residual symptoms might be worth exploring further.
There were, in fact, many similarities between the two groups in regard to their academic behavior (Table 3). ADHD students were not more likely than controls to have left college during the course of their undergraduate education. ADHD-diagnosed and nondiagnosed students were equally likely to be awarded a college scholarship, to earn the same amount of advanced placement credit, to have the same SAT scores, to take the same number of credits per semester, and to study the same number of hours per week. Although from our perspective this was a disappointingly modest amount of time, it is understandable considering that in both groups those students who had outside jobs spent almost 20 hours a week working at them. At the same time, statistically fewer ADHD students had such commitments. All of these observations are compatible with the well-established evidence that ADHD-diagnosed individuals do not have a general intellectual deficit relative to the rest of the population.
Nevertheless, despite the fact that college admission requires a minimum GPA of all applicants, ADHD students had lower high school and college GPAs and ACT scores and were more likely to have withdrawn from a college class (Table 4). This supports the well-established finding that ADHD-diagnosed adults do not attain the academic outcome expected on the basis of their IQ (Biederman et al., 2008). We note that the absolute difference in these parameters was small. Nevertheless, in a competitive environment, this numerical difference (slightly less than a B average as opposed to slightly above a B average) may certainly be sufficient to reduce the likelihood of postgraduate opportunities, such as admission to medical school, law school, and graduate school. These data answer our experimental question: Like elementary and high school students, college students with ADHD are less likely to reach the same academic level as their non-ADHD counterparts, even when they use stimulant medications, and register for institutional accommodations (Table 1).
We appreciate that several weaknesses in our study may limit our conclusions. First, our groups may not be an accurate sample of the college population as a whole because we only surveyed those students who wanted or needed extra credit. It is possible that the academic performance of such respondents was not comparable to the total undergraduate population. However, because students who need extra credit might have a lower GPA than those who don’t, the values we obtained could also be underestimates of the GPA (Advokat et al, 2008). Second, it might also be the case that some of the control students were unaware of the fact that they actually had ADHD. Third, some proportion of control students might also have been taking the stimulant medications illicitly; however, we did not ask for this information. Fourth, a few questions were not answered by a substantial portion of respondents, and our interpretation of those data may be premature. Fifth, we must rely on the honesty of our respondents, and if they didn’t pay attention to the questions or did not answer truthfully, our conclusions will be incorrect. Despite these potential issues, the fact that several demographic variables were consistent with other published studies and that we replicated our earlier finding—lower GPA of ADHD students compared to non-ADHD students—supports the validity of these results.
Control students who believed they could avoid distractions did have a much higher GPA than those who didn’t, and it was much better than the GPA of ADHD students. In contrast, the GPA of ADHD students did not differ regardless of whether or not they believed they were able to avoid distractions, suggesting that they were not accurate in this assessment. Considering that stimulant medications would be expected to help them avoid distractions, this outcome was surprising.
Although academically meaningful, the average difference in GPA between the two groups was relatively modest, and it is tempting to consider how it might be eliminated. Our data on the academic strategies of each group offer some insight. In spite of their attention deficit, ADHD students did not differ from control students in most of their study habits; both groups studied whatever was due soonest (rather than what they were not doing well in), they were both unlikely to review their notes, read assignments before class or reread their texts. ADHD students were even less likely than controls to take class notes, although the frequency of this activity (unlike controls) did not significantly influence their GPA. The fact that control students who took notes had a higher GPA than those who didn’t is consistent with research showing that test performance of college students is related to this behavior (Peverly, Brobst, Graham, & Shaw, 2003). Our finding that this did not occur in ADHD students suggests that they are less competent than their cohort in this skill, which is also consistent with previous research (Reaser, Prevatt, Petscher, & Proctor, 2007).
Interestingly, ADHD students who did not study ahead of time had a worse GPA than those who did, whereas control students did not “pay a price” in GPA for waiting until a few days before exams to study. Our preliminary analysis provided evidence that this difference occurred regardless of whether or not ADHD students used stimulant medications; that is, if ADHD students utilized the well-known strategy of studying ahead of time for exams, they could overcome their achievement deficit, even if they didn’t take the drugs. In other words, even though ADHD students are at a disadvantage in regard to academic achievement, compared to control students, this disparity could be eliminated if they were able to develop well-established study habits. Unfortunately, it is not clear from these data alone whether taking stimulant medications actually helps ADHD students to develop beneficial study habits; that is, do the stimulant drugs help students to plan ahead, for example, to begin studying ahead of time so that they can compensate for their attention deficit? It is hard to resist the conclusion that although stimulants alone are not sufficient to equalize academic achievement, the drugs, if they are used to foster good study habits, may in fact allow ADHD students to match their non-ADHD counterparts in academic accomplishment. These are issues for future research.
In summary, even with medications and some additional institutional resources, ADHD students on average, still have a lower GPA, withdraw from more classes, and don’t take notes as often as other students. They don’t study longer, or more intensely, and most don’t study ahead of time for exams. One, albeit indirect, interpretation of these results is that ADHD students use stimulant medications to make up for poor study strategies rather than to reinforce good study habits. Clearly, the drugs alone cannot overcome the detriment of insufficient preparation. Yet our data also provide some evidence that if ADHD students are able to develop the necessary organizational skills and discipline inherent in good study habits, they can overcome the achievement disparity even without stimulant medications.
Footnotes
Acknowledgements
The authors gratefully acknowledge the support provided by the Spencer Foundation for the conduct of this study. We also thank all of the students at Louisiana State University who participated in this survey.
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.