
Abstract
Introduction
ADHD is one of the most prevalent childhood disorders, occurring in 3% to 5% of school-age children (Costello, Mustillo, Erkanli, Keeler, & Angold, 2003). The core symptoms of inattention and impulsivity/hyperactivity can adversely affect a child’s academic and social emotional development (Pliszka & AACAP Work Group on Quality Issues, 2007). Because higher levels of motor activity and poorer performance on attention tests also characterize younger children, a developmental lag of cognitive functions has long been hypothesized to underlie ADHD (Barkley, 1998; Doehnert, Brandeis, Imhof, Drechsler, & Steinhausen, 2010; Kinsbourne, 1973). Deficits in attentional control, reflected in increased reaction times and an increased variability in reaction times measured during Continuous Performance Tests (CPT), are commonly observed in children with ADHD (Altink et al., 2009; Castellanos, Sonuga-Barke, Milham, & Tannock, 2006; Geurts, van der Oord, & Crone, 2006; Oosterlaan, Logan, & Sergeant, 1998; Schachar, Mota, Logan, Tannock, & Klim, 2000; Slaats-Willemse, Swaab-Barneveld, De, & Buitelaar, 2005; Soreni, Crosbie, Ickowicz, & Schachar, 2009; Stins et al., 2005; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). Individuals with ADHD are also frequently impaired on behavioral inhibition tasks as well as on measures of visuo, motor integration and fine motor control (Alderson, Rapport, & Kofler, 2007; Barkley et al., 1990; Flapper, Houwen, & Schoemaker, 2006; Hartsough & Lambert, 1985; Jakobson & Kikas, 2007; Lijfijt, Kenemans, Verbaten, & Van Engeland, 2005; Mourik et al., 2009; Oosterlaan et al., 1998; Piek, Pitcher, & Hay, 1999; Pitcher, Piek, & Hay, 2003).
The potential role of environmental factors in ADHD has been a major focus of research. A strong scientific literature documents that maternal smoking and increased maternal stress during pregnancy, as well as pregnancy and delivery complications (i.e., toxemia, eclampsia, poor maternal health, advanced maternal age, long duration of labor, fetal distress, antepartum hemorrhage, and low birth weight [LBW]), are risk factors for ADHD (Grizenko, Shayan, Polotskaia, Ter-Stepanian, & Joober, 2008; Huizink, de Medina, Mulder, Visser, & Buitelaar, 2002; Langley, Rice, van den Bree, & Thapar, 2005; McIntosh, Mulkins, & Dean, 1995; Mick, Biederman, Faraone, Sayer, & Kleinman, 2002a, Mick, Biederman, Prince, Fischer, & Faraone 2002b; Milberger, Biederman, Faraone, Chen, & Jones, 1998; Motlagh et al., 2010; Phares et al., 2004; Rodriguez & Bohlin, 2005; Ward, 1991).
For example, maternal smoking during pregnancy has been consistently associated with a two- to four-fold increased risk for ADHD in both case-control and cohort studies (Altink et al., 2009; Langley et al., 2005; Linnet et al., 2003). Prenatal exposure to smoking has also been shown to be associated with deficits in cognitive function and academic performance including selective and sustained attention, problem solving, and memory (Batstra, Hadders-Algra, & Neeleman, 2003; Batty, Der, & Deary, 2006; Breslau et al., 2007; Martin, Dombrowski, Mullis, Wisenbaker, & Huttunen, 2006; Milberger, Biederman, Faraone, Chen, & Jones, 1996; Trasti, Vik, Jacobsen, & Bakketeig, 1999), as well as problems with eye–hand co-ordination (Cornelius, Ryan, Day, Goldschmidt, & Willford, 2001; Julvez et al., 2007). However, few of these findings have been replicated in population-based studies, particularly after controlling for maternal education (Kafouri et al., 2009).
In the current study we tested for associations between measures of attentional control, motor inhibition, visual-motor integration, and fine motor coordination and prenatal exposure to heavy maternal smoking and severe maternal psychosocial stress during pregnancy in a large group of children with well-characterized ADHD.
Method
Participants
Participants included 81 children and adolescents (64 boys, 17 girls, mean age = 11.7 years; SD = 2.6) who participated in one or more studies of childhood neuropsychiatric disorders conducted at the Yale Child Study Center (Bloch et al., 2006, 2009; Motlagh et al., 2010; Peterson, 2003; Schultz et al., 1998; Sukhodolsky, Landeros-Weisenberger, Scahill, Leckman, & Schultz, 2009). Participants with a primary diagnosis of ADHD were recruited either through the Yale outpatient clinic or through a local chapter of Children and Adults with Attention Deficit Disorder (CHADD). Children with a history of neurological illness, past seizures or history of head trauma with loss of consciousness, severe learning disabilities, pervasive developmental disorder, psychosis, or severe major depression were excluded. Socioeconomic status was estimated with the Hollingshead four-factor index (Hollingshead, 1975) and the majority of families were middle to upper-middle class. After complete description of the study to the participants, written informed consent was obtained from the parents and assent was obtained from children.
Procedures
The main sources of information for establishing a diagnosis of ADHD were in-person structured interviews, administered by an experienced master-level clinician with each child and parent and the participant’s medical record. Comorbid psychiatric diagnoses were established though comprehensive clinical evaluation and administration of the Kiddie-Schedule for Affective Disorders and Schizophrenia—Present and Lifetime Version (Kaufman et al., 1997). Following a review of all available information, two senior clinicians independently assigned Diagnostics and Statistical Manual of Mental Disorders (4th ed., DSM-IV; American Psychiatric Association, 1994) diagnoses using the best-estimate procedures (Leckman, Sholomskas, Thompson, Belanger, & Weissman, 1982). Children’s ADHD symptoms during the past 3 months were assessed with the parent-rated DuPaul ADHD scale (DuPaul, 1991; Thapar et al., 2003). Each item was rated on a 4-point ordinal scale (range: 0-3) and the scores for each item were summed for the total score on the DuPaul ADHD scale (range 0-53).
To evaluate prenatal exposure to smoking, all mothers were interviewed directly using the Modified Schedule for Risk and Protective Factors in Early Development (MSRPFED; Leckman et al., 1990; Santangelo et al., 1994; Vasconcelos et al., 2007; Walkup & Leckman, 1988). Information regarding pregnancy was collected blindly with regard to the diagnostic status and psychiatric symptom severity of the child. The mothers were asked if they smoked on average more than 10 cigarettes per day during their pregnancy. Based on their YES/NO response, we created a binary variable to test the association of heavy prenatal smoking and neuropsychological performance. The MSRPFED interview also included questions concerning the family’s life circumstances during the pregnancy. Detailed questions were asked concerning potential psychosocial stressors across a range of areas including the home environment, the marital relationship, the availability of emotional supports, parental employment and family’s financial status, the parents’ physical health, and any legal issues. After completing the MSRPFED interviews, two experienced raters (LK and NT) using five-point ordinal scales (range: 1-5) were asked to rate, independently and blind to the participant’s diagnoses, the severity of the life stressors using the Level of Stress Severity scale (LSS; Leckman et al., 1990). Given the distribution of this variable and the small number of participants with severe scores (LSS = 5), we created a binary variable (LSS scores < 4 vs. ≥ 4) to test the association of prenatal severe maternal stress and neuropsychological performance.
The child birth weight was obtained by maternal reporting at the time of interview. A birth weight of less than 2,500 grams was defined as LBW and this binary variable was incorporated into the initial models as a covariate.
Neuropsychological Battery
All participants also completed a battery of neuropsychological measures. Research assistants administering these measures were blind to the diagnostic status of the participants. During these evaluation procedures, medicated children were on their usual dose and type of medication, with the exception of psychostimulants. In the case of psychostimulants, parents were asked to refrain from giving their child their daily dose(s) of psychostimulants on the day of neuropsychological testing. The administration of neuropsychological tests was counterbalanced to rule out possible effects of fatigue on the tests.
Wechsler Intelligence Scale for Children (WISC-III; Wechsler, 1991)
The Vocabulary and Block Design subtests of the WISC-III were used to estimate the child’s verbal and nonverbal intelligence.
The Conners’ Continuous Performance Test (CPT, version 3.0; Conners, 1995)
It is a measure of sustained attention and inhibitory control, which requires the participant to respond to the target letters by a button press and to withhold the response to the nontarget letter “X.” There is a total of 360 trials of which 36 (10%) are the nontargets. Thus, the motor system is primed to respond, and the participant must inhibit that prepotent response in the nontarget trials. The 360 trials are presented in 6 blocks, with three 20-trial sub-blocks which have different interstimulus intervals (1, 2, or 4 seconds). Each letter is displayed for 250 milliseconds. Average administration time is 14 minutes. Percent of omission and commission errors, the mean and SD reaction time (RT) for hits, and between blocks RT variability were used as dependent variables (Conners, Epstein, Angold, & Klaric, 2003).
The Stroop Color-Word Interference Test (Stroop, 1935)
It is a widely used test of cognitive inhibition. It consists of three conditions: (a) color naming, (b) word reading, and (c) color-word interference. In the color naming condition participants were asked to name, as quickly as possible, the color (red, green, or blue) of 126 dots, arrayed randomly in nine columns and 14 rows on a sheet of white paper (8.5×11 inches) and scanned left to right and then top to bottom. In the word reading condition participants were asked to read, as quickly as possible, an equal number of similarly arrayed words (“red,” “green,” or “blue”) printed in black ink. In the color-word reading condition, participants were asked to name a similar array of words written in incongruent colors as quickly as possible. The time to completion of each task was recorded in seconds. Stroop interference score was calculated as C – [(A × B)/(A + C)] (Golden, 1978).
Developmental Test of Visual Motor Integration (VMI, 4th ed., Beery, 1997)
It is a paper-and-pencil test that consists of 24 geometric designs, arranged in order of increasing difficulty, that the child copies. It assesses visual-graphic ability or the degree to which visual perception and finger–hand movements are coordinated. The Beery standard score was used as the dependent variable.
Purdue Pegboard Task (PPT; Tiffen, 1968)
It is a measure of fine motor control and designed to measure finger and hand dexterity. This instrument includes a 12×18-inch board, 50 one-inch pins, 20 collars, and 40 washers that are located in four cups at the top of the board (Lafayette Instrument Company, 1985). The participant must place pins in one of the two columns, each of which have 25 slots. The number of correctly placed pins in each of the test’s 30 second conditions (dominant hand, nondominant hand, and bimanual) were used as dependent variables. Reported reliabilities range between 0.60 to 0.76 for single trial scores and 0.82 to 0.91 for three trial scores (Tiffin, 1968).
Data Analysis
Separate MANCOVAs were used to examine the association of each of the two risk factors evaluated in this study with the Conners’ CPT and the PPT. ANCOVAs were used for the Stroop and the VMI. Pearson’s correlations were used to examine the associations among normally distributed continuous variables, and Chi-square statistics were used to test the differences between categorical variables.
The initial models were adjusted for the child’s age (years), gender (male or female), their IQ estimate, LBW (birth weight less than 2,500 grams), maternal education, and the family’s socioeconomic status. All covariates were run in the initial models. If they significantly contributed to the variance in the initial model they were retained in a final General Linear Models (GLMs).
Results
Maternal Smoking During Pregnancy
During pregnancy 12 (14.8 %) of the mothers reported that they smoked on average more than 10 cigarettes per day during their pregnancy. Demographic and clinical characteristics of the ADHD patients with or without prenatal exposure to maternal smoking are presented in Table 1. Patients who had been exposed to heavy prenatal maternal smoking did not differ from those who had not been regarding their age, gender, mother or father’s level of education, or the frequency of LBW or comorbid conditions with other neuropsychiatric disorders such as Tourette syndrome. However, at trend level, a significant difference was observed for socioeconomic status. The children exposed to maternal heavy smoking during pregnancy, at a trend level, also had higher Inattentive, Hyperactivity, and Total scores on the parent-rated DuPaul scale (Table 1).
Demographic and Clinical Characteristics in Children With ADHD by Heavy Maternal Smoking Exposure During Pregnancy
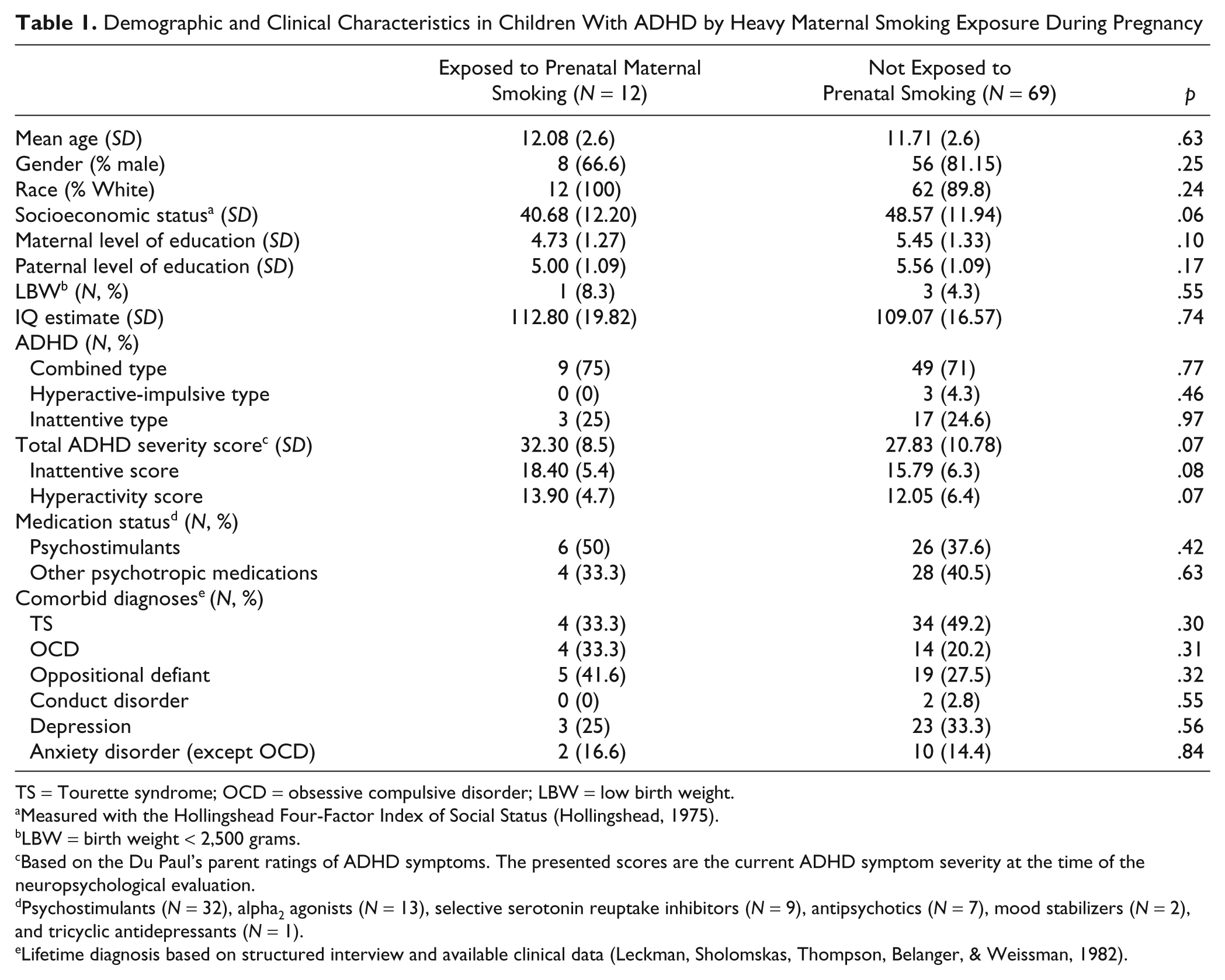
TS = Tourette syndrome; OCD = obsessive compulsive disorder; LBW = low birth weight.
Measured with the Hollingshead Four-Factor Index of Social Status (Hollingshead, 1975).
LBW = birth weight < 2,500 grams.
Based on the Du Paul’s parent ratings of ADHD symptoms. The presented scores are the current ADHD symptom severity at the time of the neuropsychological evaluation.
Psychostimulants (N = 32), alpha2 agonists (N = 13), selective serotonin reuptake inhibitors (N = 9), antipsychotics (N = 7), mood stabilizers (N = 2), and tricyclic antidepressants (N = 1).
Lifetime diagnosis based on structured interview and available clinical data (Leckman, Sholomskas, Thompson, Belanger, & Weissman, 1982).
In the initial models, the effect of heavy maternal smoking during pregnancy reached significance for the three outcome measures of Connors’ CPT, including errors of omission (F = 4.94, p = .028), reaction time (F = 7.45,p = .007), and reaction time variability (F = 10.22, p = .002). ADHD children exposed to heavy prenatal smoking performed worse compared to children who were not exposed (Table 2). These analyses controlled for the child’s age, gender, IQ, LBW, level of maternal education, and socioeconomic status. In the initial model only the child’s chronological age was significant. In the final model the child’s chronological age remained a significant covariate for errors of omission (F = 13.58, p < .001), reaction time (F = 14.7, p < .001), and reaction time variability (F = 3.87, p = .006).
Neuropsychological Performance of Children With ADHD With and Without Heavy Maternal Smoking During Pregnancy
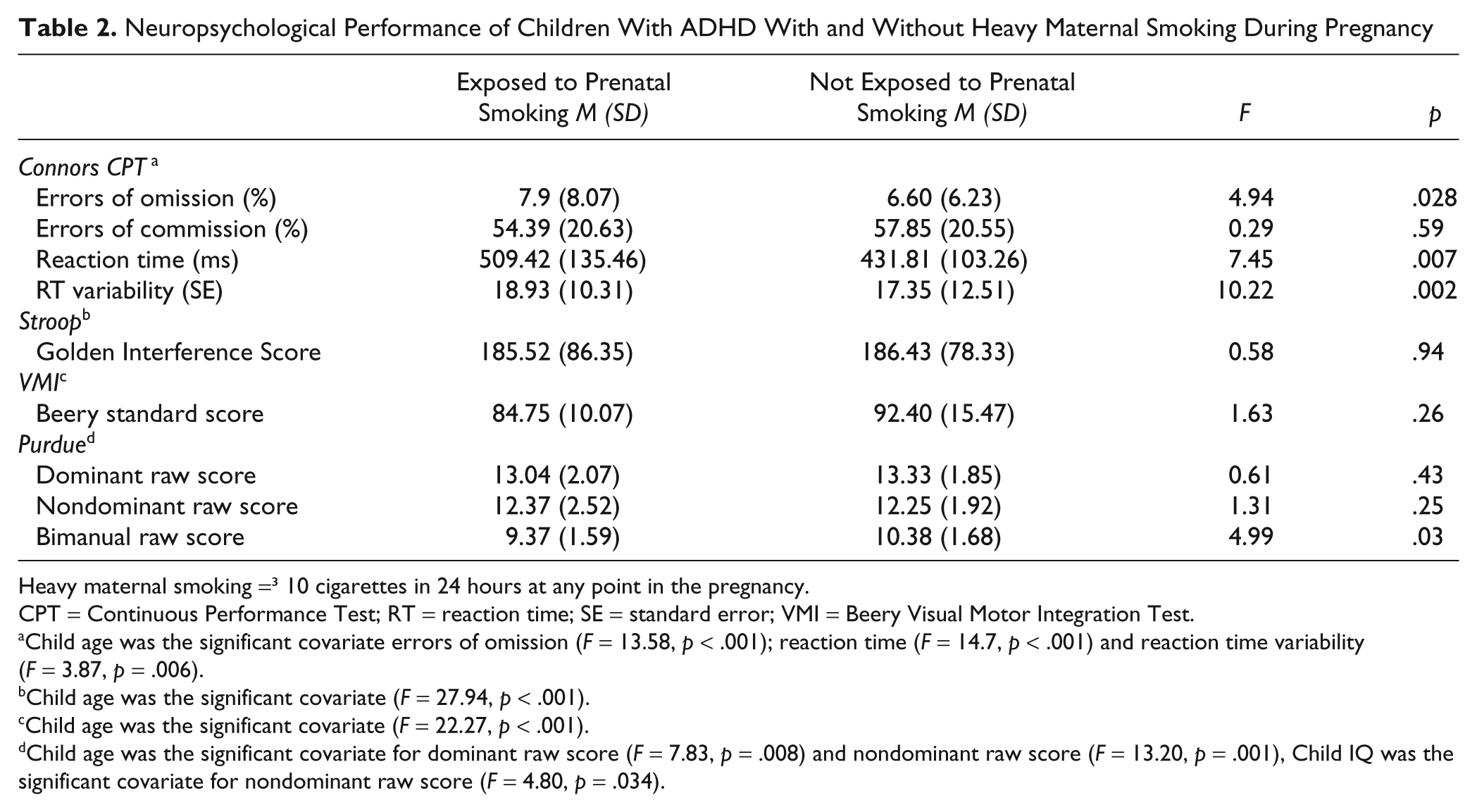
Heavy maternal smoking =3; 10 cigarettes in 24 hours at any point in the pregnancy.
CPT = Continuous Performance Test; RT = reaction time; SE = standard error; VMI = Beery Visual Motor Integration Test.
Child age was the significant covariate errors of omission (F = 13.58, p < .001); reaction time (F = 14.7, p < .001) and reaction time variability(F = 3.87, p = .006).
Child age was the significant covariate (F = 27.94, p < .001).
Child age was the significant covariate (F = 22.27, p < .001).
Child age was the significant covariate for dominant raw score (F = 7.83, p = .008) and nondominant raw score (F = 13.20, p = .001), Child IQ was the significant covariate for nondominant raw score (F = 4.80, p = .034).
In the model of heavy maternal smoking and fine motor ability, the effect of smoking was not significant either for performance with the dominant (F = 0.61, p = .43) or the nondominant hand (F = 1.31, p = .25) raw scores on the PPT. However, the child’s exposure to heavy prenatal smoking during pregnancy was significantly associated with lower scores on the bimanual performance of Purdue (F = 4.99, p = .028). These analyses controlled for the child’s age, gender, IQ, LBW, level of maternal education, and socioeconomic status. The covariate effect of LBW, level of maternal education, and socioeconomic status were not significant and these covariates were excluded in the final GLM.
Inhibition control measured by the Stroop and visuomotor integration measured by the VMI were not affected by prenatal maternal smoking. Child’s age remained a significant covariate on the Stroop (F = 42.93, p < .001) and IQ remained a significant covariate for VMI (F = 18.55, p ≤ .001).
Severe Maternal Stress During Pregnancy
Severe maternal psychosocial stress during pregnancy was judged to be present in 19 (23.5%) of the cases. Demographic and clinical characteristics of the ADHD patients with and without prenatal exposure to severe psychosocial stress during pregnancy are presented in Supplemental Table 1.
Multivariate ANCOVAs revealed nonsignificant effects of severe maternal stress on the attentional control measured by the CPT and fine motor ability measured by the PPT (Supplemental Table 2). Likewise, no significant effects of severe maternal stress were seen in the separate ANOVA analysis of the Stroop and VMI tasks (Supplemental Table 2).
Discussion
This study examined the effect of relatively high exposure to maternal smoking during pregnancy (>10 cigarettes per day) on neuropsychiatric functioning of children with ADHD while controlling for potential covariates. The effect of heavy maternal smoking on attentional control was evident in measures of both reaction time (p = .007) and reaction time variability (p = .002) on the CPT.
Nicotine exposure during pregnancy is a risk factor for ADHD-related disorders among children, and literature supporting an association between exposure to environmental tobacco smoke and subsequent symptoms of ADHD is consistent and robust (Cornelius & Day, 2009; Herrmann, King, & Weitzman, 2008). The potential neurotoxic effects of tobacco have a strong foundation in both animal and human studies, and reasonable evidence supports potential biologic pathways mediating the observed effects. Systematic meta-analyses have shown a dose-relationship with the number of cigarettes smoked during pregnancy, and several biologically plausible mechanisms could account for this association (Gatzke-Kopp & Beauchaine, 2007; Langley et al., 2005; LeSage, Gustaf, Dufek, & Pentel, 2006; Winzer-Serhan, 2008).
Although we included a range of variables that are known to be linked with smoking (age, gender, IQ, birth weight, maternal education, and SES), fetal exposure to prenatal risk factors, especially those linked to offspring mental health, is not random (Plomin, DeFries, McClearn, & McGuffin, 2008). In our subjects there was no association between maternal smoking and Hollingshead scores, nor between Hollingshead scores and ADHD severity which suggests that socioeconomic status or maternal education are not likely to be risk factors for increased symptom severity in our subjects.
An alternative explanation for the observed association of maternal smoking and attentional control in children with ADHD is that it is a proxy for ADHD and/or smoking risk genes (Altink et al., 2009; Thapar et al., 2009). For example, Thapar et al. (2009) using a novel naturalistic design, found that the magnitude of association between maternal smoking during pregnancy and ADHD was significantly greater in genetically related mother–offspring pairs than in the unrelated pairs. This finding suggests that this well-established link between maternal smoking in pregnancy and offspring ADHD symptoms might represent an inherited rather than a true environmental risk effect. Similarly, Altink et al. (2009) found a relationship between paternal smoking and the number of genetic risk factors in fathers including risk alleles of the dopamine D4 receptor and the dopamine transporter genes.
The retrospective nature of this study, the relatively small number of subjects, and the absence of information about paternal smoking are fundamental limitations of this study. Our findings are solely based on the recollections of mothers. Previous studies have suggested that there is a high degree of concordance between the data recorded in hospital records and the memories of mothers regarding prenatal events (Buka, Goldstein, Spartos, & Tsuang, 2004; Leckman et al., 1990; Rice et al., 2007; Tomeo et al., 1999). Studies in adults also show close agreement between self-reported cigarette smoking and its biochemical marker, plasma cotinine (Patrick et al., 1994). In addition, even distant (≥30-year) recall of cigarette consumption during pregnancy demonstrates a high level of agreement with archived data on smoking collected during pregnancy (Batty et al, 2006; Tomeo et al., 1999). Fewer data are available concerning the degree of agreement for more qualitative measures such as the level of maternal stress or coping ability. Some degree of recall bias is likely to be present. This may be particularly true for mothers who have a child with a disorder. In addition, compared to many recent ADHD studies, the sample size of the current study is small so that we had limited power to detect even large differences between two groups.
Other important limitations of this study include the use of a binary risk variable to assess maternal smoking and the failure to assess the presence of ADHD in the mothers. Future studies are needed to determine if there is a linear relationship between the number of cigarettes smoked during the pregnancy and the severity of the attentional problems. Likewise, information on parental ADHD would have allowed us to explore, in a preliminary fashion, the contribution of family-genetic risk to these findings.
Another limitation is the absence of a control population of typically developing children. Although we have comparable perinatal and neuropsychological data on a matched group of 65 typically developing children, the rate of maternal smoking during pregnancy was too low to provide sufficient power to perform these analyses (Motlagh et al., 2010). Nevertheless, if replicated, the specificity of the associations seen in this study indicates that maternal smoking may be linked specifically to the neural mechanisms underlying attentional control and not other neuropsychological deficits.
Identification of risk factors that affect the cognitive deficits seen in ADHD can improve our understanding of the etiology of ADHD. A possible shared genetic predisposition between neuropsychological components of ADHD and smoking provides more information about the underlying neural mechanisms. For example, the involvement of dopaminergic and cholinergic systems and gene–gene interactions may lead to novel therapeutic approaches for ADHD. The rate of heavy maternal smoking during pregnancy in this sample of ADHD cases was 14.8% which is higher than that typically seen in population-based samples. In most samples the rate of heavy maternal smoking in the general population is under 5% (Centers for Disease Control and Prevention [CDC], 2004). For example in a recent German study, an overall rate of any maternal smoking was 11.8% compared with a rate of 4.6% for women who were heavy smokers (>10 cigarettes/day; Meyer et al., 2009).
Public health efforts are needed to reduce the frequency of maternal smoking during pregnancy, specifically in high-risk populations (CDC, 2004; Phares et al., 2004; Pomerleau, Pomerleau, Snedecor, Gaulrapp, & Kardia, 2004; Wilens & Dodson, 2004). Thus far, prevention programs that address this issue have been shown to have beneficial results (Lumley et al., 2009).
Demographic and Clinical Characteristics in children with ADHD by exposure severe maternal stress during pregnancy

Note: ADHD = attention-deficit/hyperactivity disorder; OCD = obsessive compulsive disorder; Severe psychosocial stress = >4 ordinal Level of Stress Severity scale (1-5 ordinal scale,Leckman et al., 1990)
Measured with the Hollingshead Four-Factor Index of Social Status (Hollingshead, 1975)
Low birth weight = birth weight <2500 g
Based on the Du Paul’s Parent and teacher ratings of ADHD symptoms. The presented scores are the current ADHD symptom severity at the time of interview.
Included stimulants (N = 32), alpha2 agonists (N = 13), selective serotonin reuptake inhibitors (N = 9), antipsychotics (N = 7), mood stabilizers(N = 2), and tricyclic antidepressants (N = 1).
Lifetime diagnosis based on structured interview and available data.
Neuropsychological performance of children with Attention Deficit Hyperactivity Disorder (ADHD) with and without exposure to severe maternal stress during pregnancy
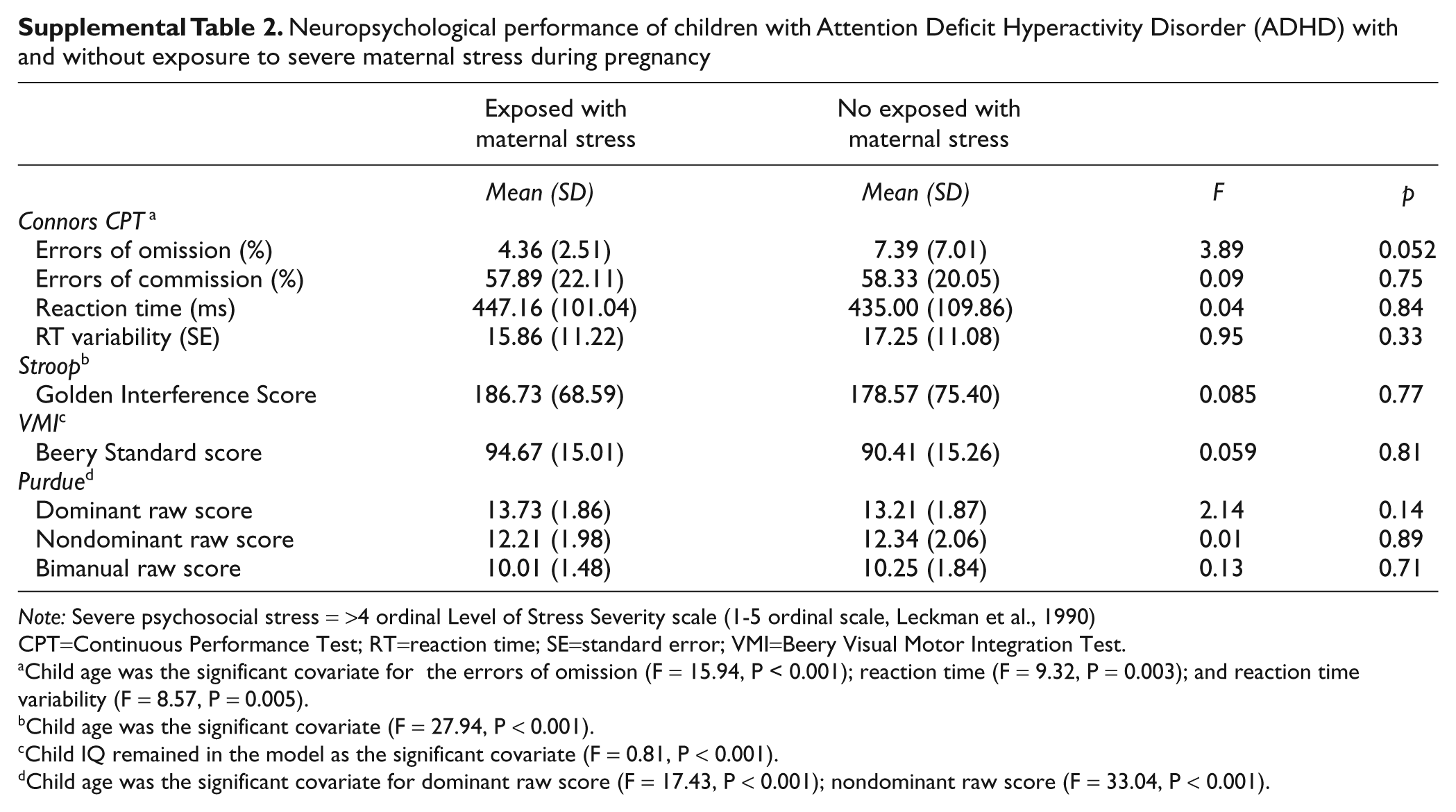
Note: Severe psychosocial stress = >4 ordinal Level of Stress Severity scale (1-5 ordinal scale, Leckman et al., 1990)
CPT=Continuous Performance Test; RT=reaction time; SE=standard error; VMI=Beery Visual Motor Integration Test.
Child age was the significant covariate for the errors of omission (F = 15.94, P < 0.001); reaction time (F = 9.32, P = 0.003); and reaction time variability (F = 8.57, P = 0.005).
Child age was the significant covariate (F = 27.94, P < 0.001).
Child IQ remained in the model as the significant covariate (F = 0.81, P < 0.001).
Child age was the significant covariate for dominant raw score (F = 17.43, P < 0.001); nondominant raw score (F = 33.04, P < 0.001).
Footnotes
Acknowledgements
The authors wish to thank Virginia Eicher for her invaluable assistance in completing this study.
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
This research was funded in part by the Echlin Foundation, and the Kaiser Family. This research was also supported by NIH Grants MH066187, P01MH049351 (JFL), K05 MH076273 (JFL), K02 MH074677-01 (BSP), R01 MH59139 (BSP) and RR00125.