
Abstract
Introduction
In treatment studies in adult ADHD, a major focus has been pharmacological interventions (Adler, 2008; Kooij et al., 2004; Lerner & Wigal, 2008; Stein, 2008). Unfortunately, research of psychological treatments is virtually absent. There is only some preliminary evidence supporting the combination of cognitive behavioral therapy and medication (Davidson, 2008; Virta et al., 2008). In addition, not all patients respond to pharmacotherapy and they often ask for counseling or additional training. In clinical settings, interventions regarding planning and organization, or coaching are often requested. Although there is abundant neuropsychological knowledge of ADHD, this is not used on a regular basis in current treatment programs. There are several neuropsychological models that consider ADHD as a primary deficit in inhibitory control, which is an aspect of executive dysfunction. Barkley (1997) also suggested that ADHD is primarily a deficit in inhibitory processes involving executive function (Barkley, 1997). He relates this inhibitory deficit to prefrontal lobe functioning, possibly related to a delay in brain development as other authors also suggest (Shaw et al., 2007). It is a challenging opportunity to examine whether adults with ADHD benefit from an intervention directed at executive functions, notably the organization and planning of activities in daily life.
Our enquiry was whether patients with ADHD would benefit from a structured course involving several aspects of executive functioning including psycho-education. Our hypothesis was that patients who were taught an executive strategy would be able to cope better with cognitive failures and would display fewer cognitive complaints compared with a control group of patients who received psycho-education only. van Hooren et al. (2007) investigated the effect of a 6-week structured course on the executive functioning of older adults in a controlled study (van Hooren et al., 2007). Their findings indicated that a combination of psycho-education and training had the potential to change the attitude of patients toward their functioning.
The aim of the present study was to investigate the efficacy of cognitive strategy training in adults with ADHD. Because executive functioning skills are often compromised in adults with ADHD (Barkley, Edwards, Laneri, Fletcher, & Metevia, 2001; Boonstra, Oosterlaan, Sergeant, & Buitelaar, 2005; Marchetta, Hurks, Krabbendam, & Jolles, 2008), we developed an intervention based on the Goal Management Training (GMT) for use in adults with ADHD (Levine, 2000). GMT involves different aspects of goal management, which include defining problems, encoding, retrieval strategies, and self-monitoring. Because adults with ADHD often suffer from mood swings and low self-esteem, we added psycho-education to GMT to provide the patient with more insight into their condition. The aim of psycho-education was to give the patients an additional tool to control their behavior and enable the selection of the most efficient coping strategy. The psycho-education was concerned with various aspects of ADHD and various neurocognitive functions, like attention, memory, planning, distraction, and coping strategies, in particular. These issues were presented in a fixed order in every session. The intervention evaluated in the present article consisted of 11 group sessions (1 session per week) and 1 individual session per participant.
The intervention was performed in an evidence-based fashion. A randomized waiting-list control group design was used and we examined whether this intervention was effective in reducing complaints and in improving cognitive functioning. During the course, the emphasis was on complaints experienced by the participants. We therefore expected that this new neuropsychological treatment program would have an effect on general functioning and on cognitive complaints in particular rather than on actual cognitive performance. The study was carried out in a controlled manner using two active interventions. There were two complementary methods used to assess the effects of the intervention studied. First, a neuropsychological test battery as well as questionnaires were used, which are known for their sensitivity in this type of intervention study (Valentijn et al., 2005; van Hooren et al., 2007). Second, a completely new approach was taken to evaluate the effect of the neuropsychological intervention. This involved a procedure that has proved its merits in evidence-based pharmacotherapeutic trials in psychiatric or neuropsychiatric patients (Martinez-Martin, Rodriguez-Blazquez, Forjaz, & de Pedro, 2009; Quinn et al., 2002; Schneider et al., 1997). In short, an experienced clinician blinded to the actual intervention, which each individual received, assessed the patient on various aspects of psychological and neuropsychological functioning. This clinician used a standardized clinical rating scale to evaluate change in cognitive and global functioning in the participants with adult ADHD. The clinical rating scale used here was based on the Clinician’s Interview-Based Impression of Severity and Change (CIBIS and CIBIC), which was originally used in, and is a familiar element of, pharmacological studies (Schneider et al., 1997).
Method
Procedure
A baseline assessment (T1) and two follow-up assessments (T2, T3) were used. All participants were screened for cognitive complaints, expectations of the program, and prior treatments. Demographic variables, medication, and complaints of cognitive functioning were obtained. After screening, participants were randomly assigned to the intervention group (GMT+) or the psycho-education-only group (psycho-education). The follow-up assessments were carried out after 12 weeks (T2) and again after 24 weeks (T3). As stated before, the current study was completed in a controlled manner using two active interventions.
Participants
Participants were referred for treatment of cognitive problems from the outpatient facility for adults with ADHD at Mondriaan Maastricht, the Netherlands. All participants had a diagnosis of ADHD (this diagnosis was made by a physician experienced in ADHD) and were 18 years of age or older. Major comorbid disorders according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; both Axis 1 and Axis 2; American Psychiatric Association [APA], 2000) were excluded from the treatment program. The use of psycho-stimulants was not an exclusion criterion (because of ethical considerations). In our sample, 89% of the participants used psycho-stimulants. Three participants did not use psycho-stimulants (two participants in the experimental group and one participant in the control group). Every participant was screened by a certified psychologist on his or her motivation before the start of the training. None of the participants had participated previously in a neuropsychological treatment/research program. All participants gave informed consent. They were randomly assigned to the GMT and psycho-education group (GMT+ group) or the psycho-education-only group. In total, four groups (two GMT+ groups and two psycho-education-only groups) were evaluated.
Two participants of the experimental group dropped out; one because of health issues (severe migraine) and the other participant because of comorbid depressive disorder. In the second assessment, two participants were unable to participate; one because of house renovation/work and the other participant did not show up at several appointments. One participant was unable to take part in the clinical interview at T3 (because of annual leave) and one participant was unable to fill in the Symptom Check List–90 (SCL-90) and Cognitive Failures Questionnaire (CFQ), because of other responsibilities (work).
See Table 1 for information on the participants. Participants in the two groups did not differ according to age, sex, and level of education. Twelve participants were included in the experimental group; the control group comprised 15 participants. At baseline there were group differences on the clinical rating subscales (cognition and general). The control group displayed less interference in daily activities through subjective cognitive complaints.
Patient Characteristics.
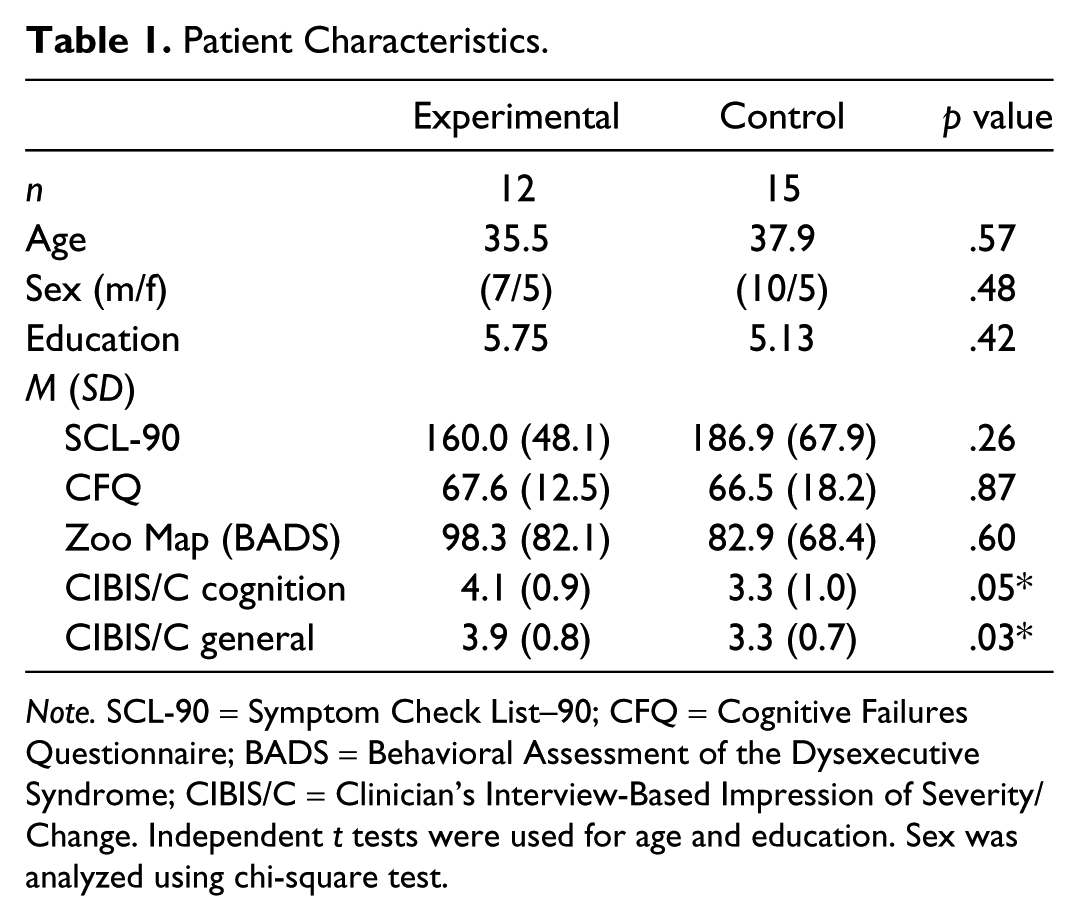
Note. SCL-90 = Symptom Check List–90; CFQ = Cognitive Failures Questionnaire; BADS = Behavioral Assessment of the Dysexecutive Syndrome; CIBIS/C = Clinician’s Interview-Based Impression of Severity/Change. Independent t tests were used for age and education. Sex was analyzed using chi-square test.
However, the SCL-90 score was high for both the experimental and the control group compared with Dutch norm groups. Also, the CFQ total score was high in both groups compared with Dutch norm groups, as expected.
Treatment Program
GMT plus psycho-education for ADHD patients
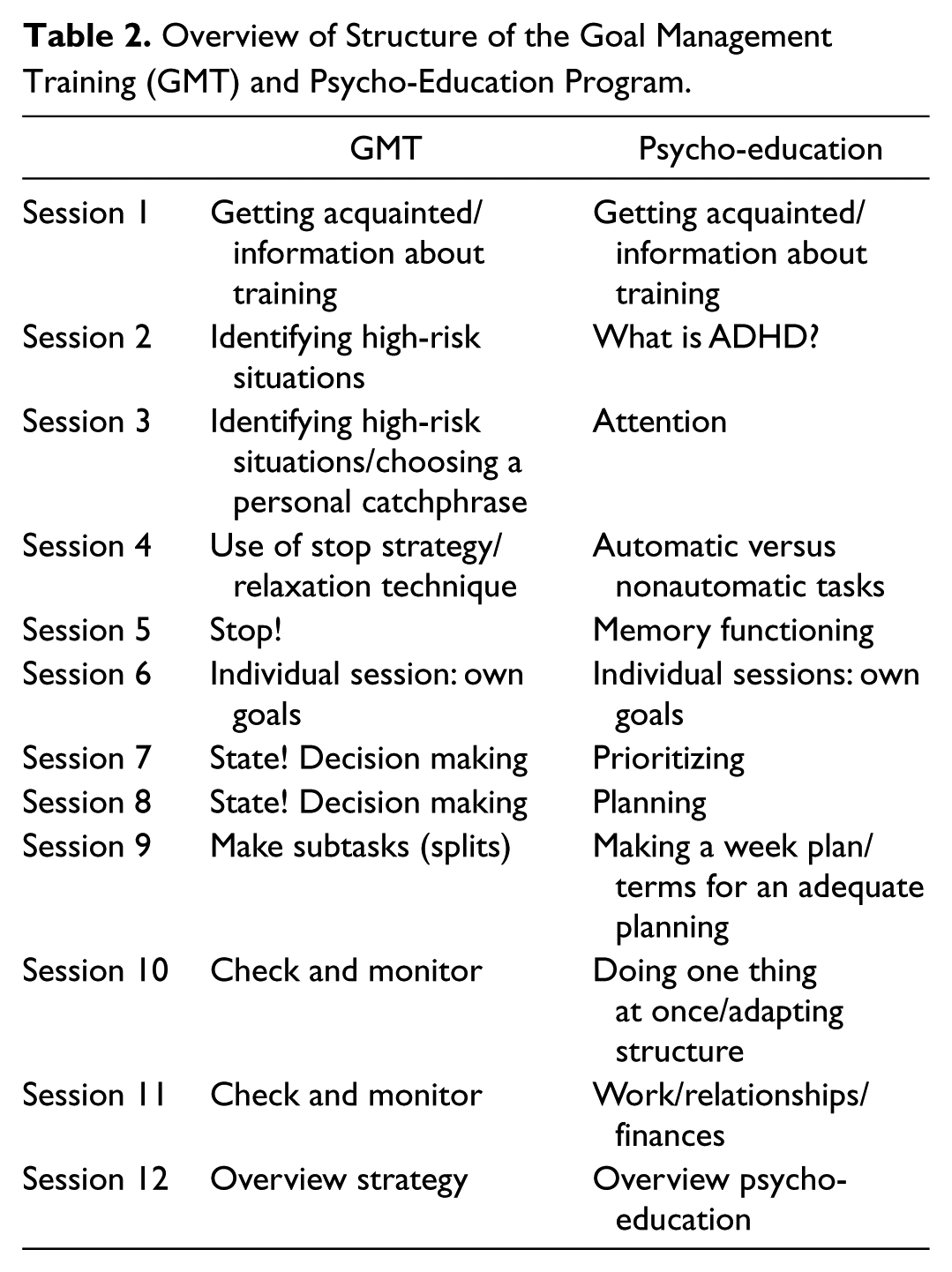
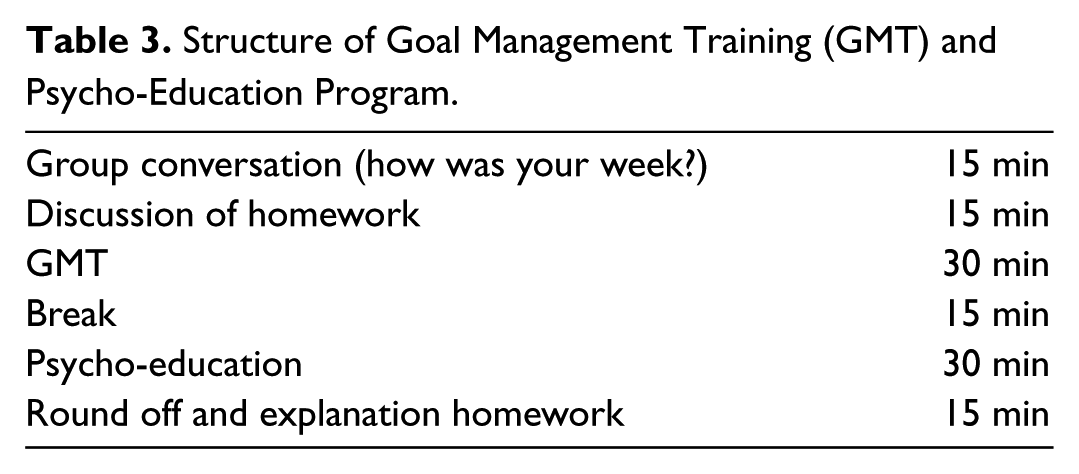
The aim of GMT is to teach patients a strategy to improve planning activities and to structure intentions. The training manual was previously translated into Dutch for use by older adults (Levine et al., 2000; Levine, 2000; van Hooren et al., 2007). van Hooren et al. (2007) have shown previously that a combination of psycho-education and training had the potential to change the attitude of older patients toward their functioning (van Hooren et al., 2007). One major addition to GMT for ADHD patients concerns the nature of “psycho-education,” that is, an explanation of the various cognitive functions and the clinical picture of ADHD in adults in general. Furthermore, specific examples of cognitive failures in ADHD were discussed in the group. These examples were based on examples from GMT used by van Hooren et al. (van Hooren et al., 2007). Because of the addition of psycho-education, the program was adapted to consist of 12 sessions, 1 individual session and 11 group sessions. The content of each session and the order in which the topics were addressed were structured in a protocol (see Table 2). The group session was coordinated by two clinical neuropsychologists: a trainer and an assistant. At the start of the program, each group comprised a minimum of 6 and a maximum of 8 persons to ensure that the training group could function optimally. There were 2-hr sessions for 12 consecutive weeks. A manual containing the full text and tasks used by the trainer was available. The trainer included examples put forward by the participants in the session. All sessions were structured (see also for an elaboration; van Hooren et al., 2007). In the group sessions, the participants discussed their cognitive problems with peers and had the opportunity to support each other. At the end of each session, participants received homework exercises as well as hand-outs containing a summary of the session. All topics were illustrated with practical examples or exercises. The goal of the first session was to get acquainted with the trainers and other participants as well as with the goals of the program. The expectations of the program and increasing insight into the complaints about executive functioning were discussed. Psycho-education on ADHD in adults was examined and participants were asked to reflect on what ADHD meant to them. In the second, third, and fourth sessions, high-risk situations were identified, the stop strategy was introduced using an automatic pilot metaphor, and a personal catchphrase was chosen, for instance, “time-out,” “ho!,” or “wait a minute.” In the fifth session psycho-education with respect to memory functioning was offered. The stop strategy was extended in Sessions 4 and 5 by means of a relaxation technique; information processing and working memory were also discussed (see Table 2). In the sixth session, expectations of the course, (individual) personal problems, and goals were talked about. Sessions 7 and 8 focused on setting a goal. In Sessions 7 and 8, psycho-education on prioritizing and planning was discussed. Session 9 was used to discuss splitting a complex task into subtasks and then to prioritize these subtasks. In this session, psycho-education on planning and organization was presented. The main theme of Sessions 10 and 11 was to check current behavior, for instance, to check whether the goals set were still adequate. Psycho-education for this session was “doing one thing at the time.” In the final session, an overview was given and participants received an assignment in which they had to use the strategies learned and translate those to their daily lives. This assignment was then discussed in the group (Table 3).
Overview of Structure of the Goal Management Training (GMT) and Psycho-Education Program.
Structure of Goal Management Training (GMT) and Psycho-Education Program.
Psycho-education only
For the control group “psycho-education only,” the psycho-education in every session did not contain the strategy training. In the control group, conversation was allowed and homework was discussed. The psycho-education was structured and presented in exactly the same order and in a similar manner as to the GMT+ group. Therefore, the sessions of the psycho-education group (from T1 until T2) lasted 1.5 hr, instead of the 2 hr for the GMT plus psycho-education group. In the final session (Session 12), an overview of the psycho-education was given. After the psycho-education program had finished, the participants of the control group were given the strategy training.
Outcome Measures
Subjective Functioning
CFQ
CFQ was used to evaluate the frequency of everyday cognitive failures, including subjective executive functioning. The scale is validated in Dutch and consists of 25 items measuring the frequency of everyday cognitive failures in the domains of memory, attention, perception, and action (Broadbent, Cooper, FitzGerald, & Parkes, 1982; Ponds, Commissaris, & Jolles, 1997). Participants were asked to indicate on a 5-point scale how often they experienced particular cognitive failures (very often, quite often, occasionally, very rarely, never). Answers were recoded following Dutch instructions (Ponds et al., 1997). A higher score on the CFQ indicates a larger number of cognitive failures.
SCL-90
This is a multidimensional, self-reporting inventory of psychopathology (Derogatis, Rickels, & Rock, 1976). The scores for the Anxiety, Depression, and Sleep subscales ranged from 0 to 50, 0 to 80, and 0 to 15, respectively. On all three scales, a higher score is considered indicative of a larger number of symptoms. The SCL-90 total score was used as a measure of distress.
Objective Executive Functioning
Zoo Map From the Behavioral Assessment of the Dysexecutive Syndrome (BADS)
The Zoo Map subtest is a planning test. It provides information about the ability to plan a route to visit 6 of a possible 12 locations in a zoo. The outcome measure chosen was the time needed to plan a route (unstructured version), because GMT involves teaching participants to stop their ongoing behavior and take more time to plan (Burgess, Alderman, Evans, Emslie, & Wilson, 1998; Krabbendam, de Vugt, Derix, & Jolles, 1999).
Clinical Rating Scale
A certified and experienced clinical neuropsychologist who was not involved in the treatment program and blind to the condition or group (GMT+ or psycho-education only) interviewed the participants. He rated participants at baseline and at the two follow-up meetings (after intervention) with respect to six areas of functioning. This included cognition, everyday functioning, work/social functioning, mood, and general functioning according to the CIBIS and CIBIC (Schneider et al., 1997)). Prior to the clinical rating, the neuropsychologist explained to the participants that he was blind to their condition and would not discuss themes from the program. At baseline, participants were rated on a 7-point scale: 1 = no cognitive disorders, 2 = subjective complaints, no interference in daily life, 3 = subjective complaints and moderate interference in daily life, 4 = subjective complaints and severe interference in daily life, 5 = mild disorders, 6 = moderate disorders, and 7 = severe disorders.
At the two follow-up assessments, participants were again rated on a 7-point scale: 1 = very much improved, 2 = much improved, 3 = minimally improved, 4 = no change, 5 = minimal worsening, 6 = moderate worsening, and 7 = severe worsening. The aspects most interesting in this study were the ratings of everyday functioning in general and cognition in particular as GMT was developed to teach patients a strategy for improving planning activities and to structure intentions and therefore diminish cognitive complaints.
Other Measures
Age was used as a continuous variable. Level of education was indexed on an 8-point ordinal scale, ranging from primary to university education (De Bie, 1987).
Statistical Analyses
Although the participants were randomly assigned to the two groups, possible differences could exist between these by chance. We first examined whether there were important demographic differences between the experimental and control groups. Using independent t tests, we compared age and level of education between the two groups. We also compared the level of distress (as measured by the SCL-90), cognitive failures, planning time, and CIBIS at baseline between the two groups (see Table 1). A chi-square test was used to analyze group differences with respect to sex. General Linear Model (GLM) with repeated-measures ANOVA was applied to examine the effect of intervention. Analyses were carried out with group (two levels: experimental and control group) as between-subject factor and time (three levels: baseline, first follow-up, and second follow-up) as the within-subject factor. Second, as we were primarily interested in differences between the two groups at T2, difference scores were calculated for all outcome measures (T2 − T1), except for the ratings on the clinical rating scale (as “change” was already measured in the clinical rating). To examine the effects of intervention on cognitive complaints as well as planning time at Assessment 2 (T2) and 3 (T3), independent t tests were carried out in both groups.
The 15th version of the Statistical Package for the Social Sciences (SPSS) for Windows was used for the statistical analyses (SPSS Inc., Chicago), with p = .05 as significance level.
Results
Effects of GMT Plus Psycho-Education for ADHD Patients
In the second assessment, a significant effect was found between the two groups on the clinical rating scale for the domain “cognition,” F(1, 22) = 0.656, p = .024 (Table 4). The clinician rated the participants in the experimental group as cognitively more improved between baseline (T1) and first follow-up (T2). The two groups did not differ on the clinical rating scale for the domain “general functioning,” F(1, 22) = 0.028, p = .438. Second, GLM showed an effect of time for SCL-90 total score, CFQ total score, and zoo planning time, F(1, 21) = 11.86, p = .002), F(1, 20) = 35.66, p = .000, F(1, 22) = 6.99, p = .015. There were no interaction effects between group and time on any of the measures (Figures 1, 2, and 3).
Means, Standard Deviation, Difference Scores (T2 − T1) and p Values of the Independent t Tests.

Note. FU1 = Follow-Up 1; FU2 = Follow-Up 2; CFQ = Cognitive Failures Questionnaire total score; Exp = experimental; SCL-90 = Symptom Checklist–90 total score; Zoo Map = planning time in seconds (Behavioral Assessment of the Dysexecutive Syndrome [BADS]); CIBIC = Clinician’s Interview-Based Impression of Change.
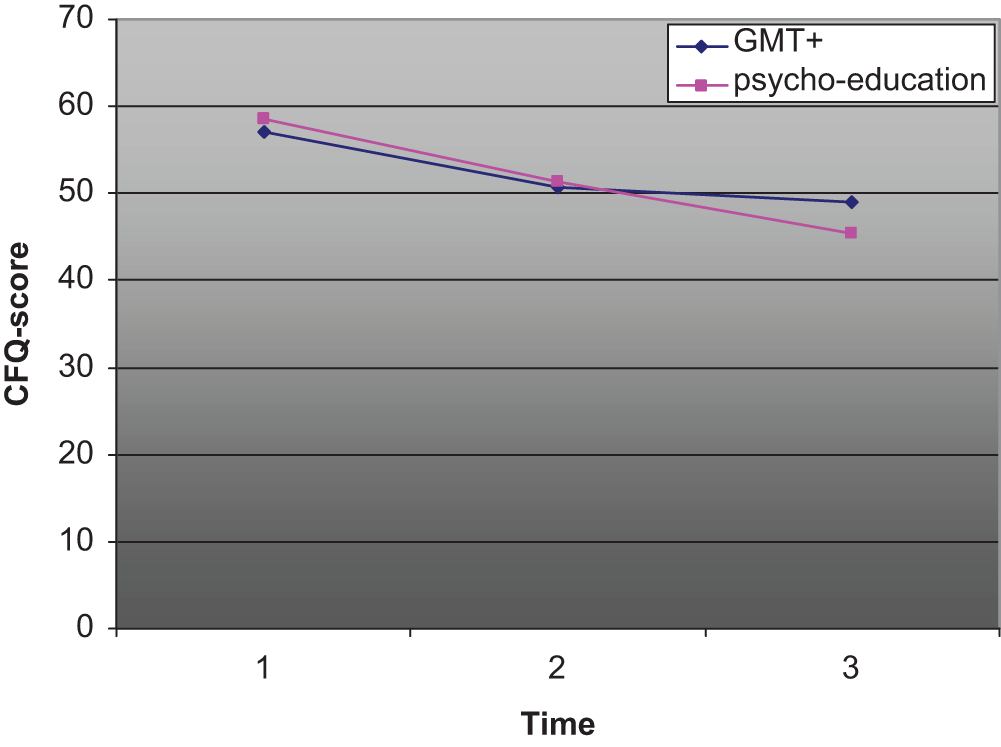
CFQ total score for the GMT+ group and psycho-education-only group at baseline (1), follow-up after 12 weeks (2), and follow-up after 24 weeks (3).
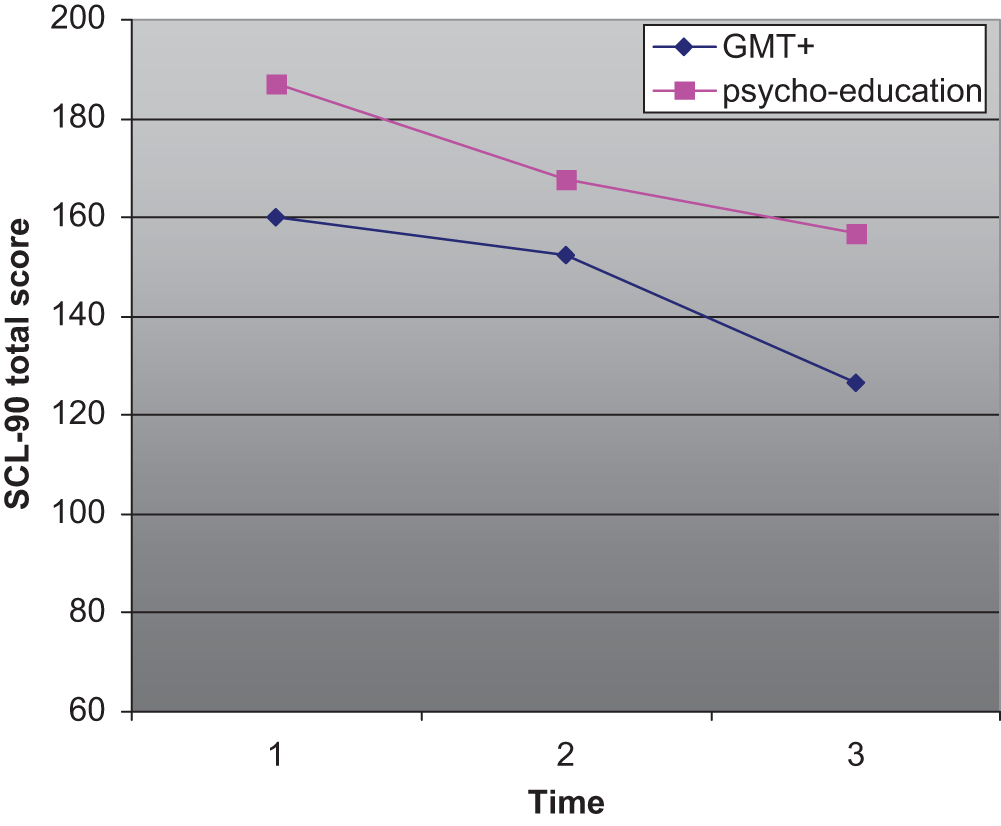
SCL-90 total score for the GMT+ group and psycho-education-only group at baseline (1), follow-up after 12 weeks (2), and follow-up after 24 weeks (3).
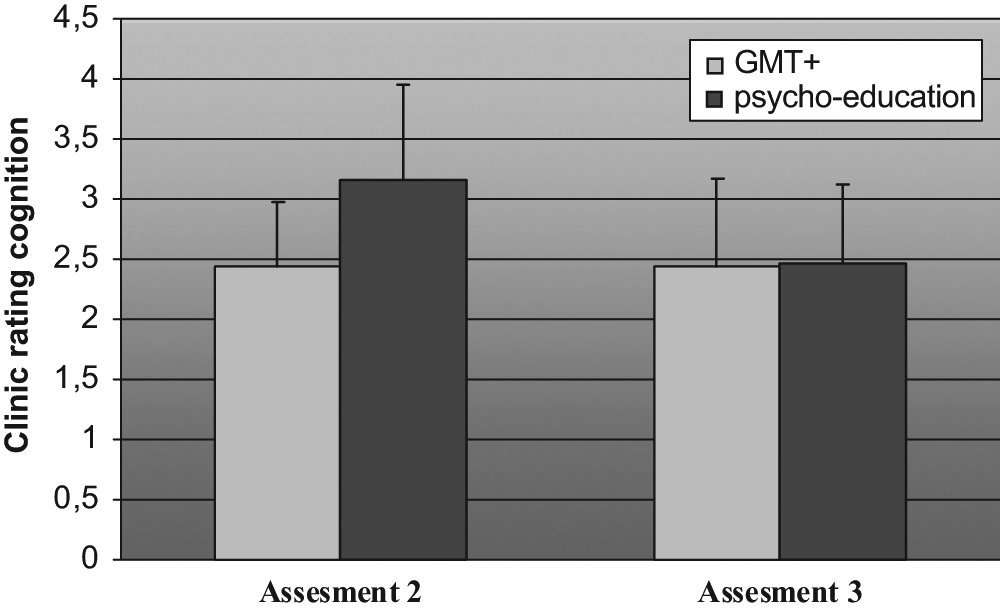
Clinical rating with respect to “cognition” for the GMT+ group and psycho-education-only group at follow-up after 12 weeks (2), and follow-up after 24 weeks (3).
No significant effect was found with respect to the difference scores between Follow-Up 1 (T2) and Follow-Up 2 (T3) on level of distress as measured by the SCL-90, F(1, 21) = 0.000, p = .983. Also, no significant effect was found with respect to the difference scores between Follow-Up 1 (T2) and Follow-Up 2 (T3) on cognitive failures, F(1, 21) = 0.064, p = .434. Finally, no significant differences were found with respect to the planning time (Zoo Map subtest from the BADS) at Follow-Up 1 (T2), F(1, 22) = 0.882, p = .781. Post hoc additional nonparametric analyses were done to examine whether the changes we found were in fact in the right direction (that is GMT-associated changes). The Kruskal-Wallis (with the use of a “grouping” variable) revealed a significant effect for the domain “cognition” at first follow-up as rated by the experienced clinician (p = .04; Table 5).
Mean Scores and Standard Deviations Over Time for the Two Groups (Experimental vs. Control).
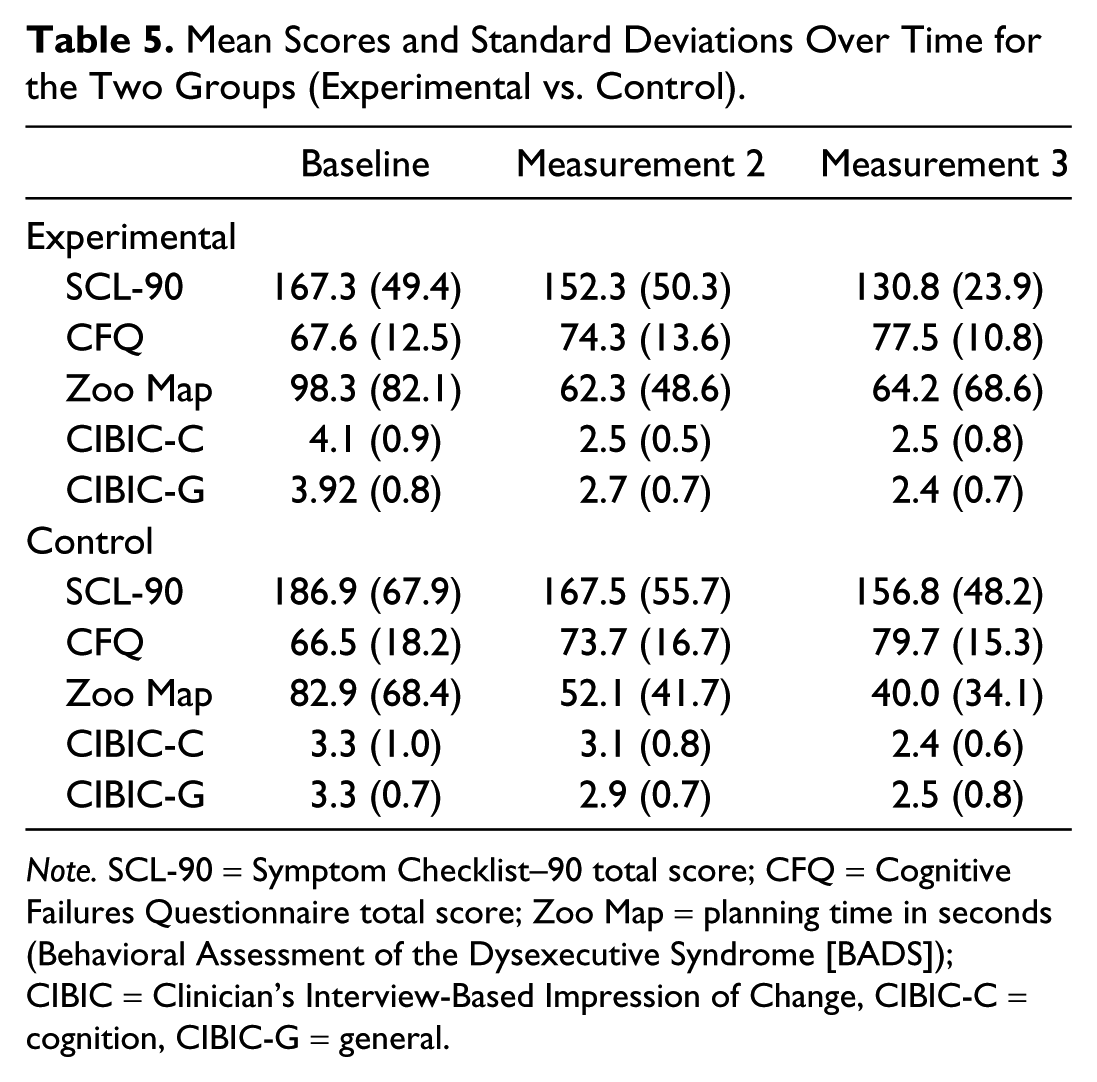
Note. SCL-90 = Symptom Checklist–90 total score; CFQ = Cognitive Failures Questionnaire total score; Zoo Map = planning time in seconds (Behavioral Assessment of the Dysexecutive Syndrome [BADS]); CIBIC = Clinician’s Interview-Based Impression of Change, CIBIC-C = cognition, CIBIC-G = general.
Discussion
The aim of this investigation was to establish whether patients with ADHD would benefit from a structured course based on neuropsychological insights and including several aspects of executive functioning. A new research tool was used to evaluate the possible effect of the intervention in this controlled clinical study. For this purpose, a clinical rating scale, the CIBIC/CIBIS, was used. The main hypothesis was that patients who were taught an executive strategy would be able to cope better with cognitive failures and would have fewer cognitive complaints compared with patients who received psycho-education only. The first finding in this study was that there were no significant differences between the two groups (experimental and control) with respect to age, level of education, or level of distress. The clinician, however, rated that there was more interference in daily life activities for the experimental group. Both groups scored high on measures of distress and frequency of cognitive failures. Although participants with severe comorbidity were excluded from the intervention, the mean level of distress and complaints in several domains like depression, anxiety, and sleep was overall high. There was also a great variance between individuals with respect to the level of distress. Although comorbid psychiatric disorders were described as an exclusion criterion, the level of distress between participants in both groups strongly varied. For instance, the range of the SCL-90 total score was between 110 and 289.
A second finding of the present study was the significant effect of time on subjective and objective test measures in both groups. On the CIBIC, the experimental group improved more in the domain of cognitive functioning. This was in line with our hypothesis. In the current study, the CIBIC was used for the first time in a controlled neuropsychological intervention study. The rating procedure carried out by a health professional blind to the protocol and who uses the CIBIC has the potential in detecting changes over time. The present study proves that this is true not only for pharmacological treatment but also for nonpharmacological treatment. Interestingly, the present study showed that the CIBIC was sensitive to detecting clinical changes, whereas regular measurements, such as the level of complaints and objective test measures were not. Furthermore, an important advantage of the CIBIC is that the clinician is blinded to the condition and that the rating is based on a clinical interview.
As stated before, on other subjective and objective test measures, no group differences were found. Our hypothesis that participants involved in GMT would display less distress and fewer cognitive complaints could only partly be confirmed (by using the CIBIC). Our research was aimed at investigating whether GMT would have an additional effect on psycho-education. The present study has not found very strong evidence for this. One explanation is that, in hindsight, our control group was given a full intervention (“active” control), which included peer interaction and providing information, which could have a positive treatment effect on increasing awareness of cognitive problems in itself. Therefore, our “control” group was not in all respects an actual control group, but was in fact another active treatment program. The fact that peers interacted with each other about their complaints and discussed factors like personality, coping styles, and cognitive problems seems to have had an effect on the results. A limitation of this study was that the control group did not receive the same duration of treatment sessions as the GMT group. In fact, the control group received more group sessions. It would have been welcome if both groups received an equal amount of group sessions. However, it is encouraging that the GMT group seems to improve more than the control group though less group sessions are involved. Another factor that needs to be considered is the fact that the group of participants was very heterogeneous. The diagnosis of ADHD is based on the DSM-IV-TR criteria for children (APA, 2000). The main symptoms are inattentiveness, hyperactivity, and impulsivity. Participants in this study were heterogeneous with respect to ADHD symptoms. Qualitative information showed that some participants improved a lot after the GMT program whereas other participants did not benefit from the training. Future research should be aimed at gaining insight into what type of participants are “sensitive” to GMT and what factors contribute to this.
Qualitative information showed that the experimental group improved 12 weeks after the intervention program stopped (T3). This is very promising information as it could be possible that the effects of the strategy training need time to become a new automatic process. Because of ethical reasons, the control group received the strategy training between T2 and T3. Therefore, we were unable to measure actual long-term effects of GMT in adults with ADHD. Future research could include investigating GMT in adults with ADHD compared with a waiting-list control group. In this study, it was ethically not allowed to make the “control” group wait because of the high level of distress it could cause and need of care of participants. It could be assumed that because the “control” group had the advantage of “distributed practice,” the “control” group would in fact improve more over time (Wilson, 2003).
This study found an effect of GMT over and above psycho-education for adults with ADHD in a clinical interview. The CIBIC was sensitive to detect clinical change and has potential in the contribution to the evaluation of neuropsychological intervention. Future research should include larger groups and a waiting-list control group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.