
Abstract
Introduction
Psychostimulant medications used to manage the core symptoms of ADHD are highly effective for most patients (Greenhill et al., 2002). Nevertheless, a small body of clinical literature (Carlson & Kelly, 2003; Cox et al., 2008; Porrino, Rapoport, Behar, Ismond, & Bunney, 1983; Sarampote, Efron, Robb, Pearl, & Stein, 2002; Swanson et al., 2004) along with case reports (Sarampote et al., 2002) indicate that some youths experience symptom rebound. Symptom rebound is a deterioration in behavior when psychostimulant medication wears off, which can be severe enough to warrant treatment discontinuation. During a rebound episode, parents may describe their child as more hyperactive/impulsive than at baseline, more prone to sudden shifts in mood that are not appropriate to context, and more likely to exhibit tearfulness, crying, temper outbursts, aggression, and irritability (Carlson & Kelly, 2003; S. Pliszka, 2007).
Whereas rebound is generally accepted as a valid phenomenon, the lack of an established, working definition as applied to ADHD has resulted in very little clinical research directly describing its nature, frequency, and clinical significance (Carlson & Kelly, 2003; Cox et al., 2008). As reviewed by Cox et al. (2008) and Connor (2006), rebound has been operationally defined as deterioration in behavior so that symptoms are more severe than observed at baseline or placebo conditions and which occur in the late afternoon or evening after morning treatment with a psychostimulant (Cox et al., 2008). Although this operational definition has face validity, it has not yet been empirically tested, so construct validity has not been established. Defining rebound as it relates specifically to ADHD treatment and in an ADHD population subgroup, such as children, offers potential for improved understanding of factors that may affect management of ADHD.
In one investigation, psychiatrically hospitalized children with an ADHD diagnosis were observed for evidence of rebound, based on assessment across the day of non-ADHD symptoms common to rebound (i.e., euphoria, insomnia, irritability, and sadness/excessive crying; Carlson & Kelly, 2003). Of 149 patients, 87 (58.4%) had no rebound, 17 (11.4%) had worse behavior in the evening with and without psychostimulant treatment, and 32 (21.5%) had transient symptom rebound lasting no more than 1 week. Only 13 (8.7%) had rebound symptoms for more than 50% of the evenings, which resulted in discontinuation of psychostimulant medication. The report by Carlson and Kelly (2003) provides important insights into the nature and frequency of rebound and rebound-like emotional symptoms. However, it remains unclear whether core ADHD symptoms, such as inattention or hyperactivity/impulsivity, exhibit late-day rebound. Studies characterizing rebound in terms of currently available validated, scale-based assessments that measure symptom outcomes are needed.
Another challenge to investigating symptom rebound is the presence at baseline of emotional lability (EL), defined as changes in emotional expression marked by moods that go up and down quickly, or by distinct periods of irritability or euphoria (Carlson, 1998; Carlson & Kelly, 1998), or psychiatric comorbidities. EL is seen in a large proportion of children with ADHD (American Academy of Pediatrics Subcommittee on Attention-Deficit/Hyperactivity Disorder and Committee on Quality Improvement, 2001; American Psychiatric Association, 2000; Sobanski et al., 2010; Strine et al., 2006). In one recent report (Sobanski et al., 2010), among children 5 to 18 years old with ADHD, a composite EL measure was derived from the parent- and teacher-rated Conners’ Global Index: EL, which includes items on unpredictable mood changes, temper tantrums, tearfulness, and low frustration tolerance. Mild to moderate EL was seen in 50% of the children, and 25% showed severe EL with scores three standard deviations above the normative mean (Sobanski et al., 2010). Despite common occurrence of EL, emergent or worsened EL-type symptoms as an adverse event (AE) leading to discontinuation of medication appear to be rare (~1%-3%) in pediatric clinical trials of long-acting psychostimulant treatment for ADHD (Swanson et al., 2004; Weisler et al., 2006; Wilens et al., 2006). It is unclear whether the presentation of EL may overlap with and appear similar to rebound symptoms.
Rebound may go largely undetected in most clinical trials due to the lack of a universally accepted definition of rebound across categories of symptoms; clinical investigators may be unable to consistently detect and document its occurrence. If clinically significant rebound occurs in only a limited proportion of participants, as indicated by Carlson and Kelly (2003), late-day worsening of core ADHD symptoms and EL scores may be “lost” in group data analyses. Alternatively, describing rebound based on AE reports of EL does not account for timing of postdose occurrence and for relationship to other core symptoms such as hyperactivity/impulsivity. To date, no scale-based definition of rebound that takes into account both core ADHD symptoms and EL symptoms has been investigated in a controlled clinical trial.
Lisdexamfetamine dimesylate (LDX; Vyvanse®, Shire US Inc.) is a long-acting prodrug stimulant and is indicated for the treatment of ADHD in children 6 to 12 years, adolescents 13 to 17 years, and in adults (Vyvanse [package insert], 2012). In a 4-week, placebo-controlled trial in children with ADHD, LDX improved ADHD symptoms (vs. placebo) throughout the day (Biederman, Krishnan, Zhang, McGough, & Findling, 2007) based on the Conners’ Parent Rating Scale–Revised: Short Form (CPRS-R:S; Conners, 2008). In a recent post hoc analysis of this trial, LDX improved EL (vs. placebo), both across the day and over 4 weeks (Childress et al., 2009). However, no study of rebound symptoms with LDX treatment has been conducted in any age group of patients with ADHD. Characterizing the extent of occurrence of rebound and the profile of symptoms during treatment with a long-acting prodrug stimulant may provide useful information for clinicians making treatment decisions in the management of children with ADHD.
The objective of the current post hoc analysis of this trial (Biederman et al., 2007) was to examine the occurrence of clinically significant response and rebound of core ADHD symptoms over the course of the day based on assessment using the CPRS-R:S. The relationship of rebound to EL was also examined. An operational definition for rebound based on the discussion above served as the basis for devising rebound criteria for the present analysis. This definition and these criteria are discussed in the “Method” section.
Method
Study Design Overview
This was a randomized, double-blind, placebo-controlled, forced dose-escalation trial, as previously described (Biederman et al., 2007). Participants were randomized to receive LDX (30, 50, or 70 mg/day) or placebo during a 4-week period. All participants who were randomly assigned to LDX treatment began with the 30-mg/day dose; for those assigned to 50 mg/day or 70 mg/day, the initial 30-mg/day dose was increased in 20-mg increments at weekly intervals.
This study was performed in accordance with the Declaration of Helsinki and the International Conference on Harmonization guidelines for Good Clinical Practice. Parents/guardians of all participants provided written informed consent, and participants gave assent prior to the conduct of any study procedures.
Participant Selection Criteria
Detailed entry criteria have been previously reported (Biederman et al., 2007). Eligible participants were children (6-12 years) with a primary diagnosis of ADHD with moderate to severe symptoms (baseline ADHD Rating Scale IV [ADHD-RS-IV]; DuPaul, Power, Anastopoulos, & Reid, 1998; Faries, Yalcin, Harder, & Heiligenstein, 2001; total score ≥ 28). Participants with predominantly inattentive subtype were excluded. Also excluded were individuals with comorbid psychiatric disorders, history of seizures, history or family history of specific cardiac conditions, hypertension or taking medication (except current ADHD therapy) that affects blood pressure, and a current diagnosis or family history of Tourette disorder.
Efficacy Measures
The primary efficacy measure was the ADHD-RS-IV; these primary outcomes have been described previously (Biederman et al., 2007) and are not presented here. For the current post hoc analysis, objective scale-based criteria for rebound were based on its broad definition as ADHD symptoms that (a) return after initially being adequately controlled following morning treatment (e.g., “response” must occur before “rebound”) and (b) are worse than at baseline. Whether participants with ADHD symptom rebound exhibited a concomitant worsening in EL was also determined using a CPRS-R:S-derived composite EL score as described below.
Response, rebound, and EL patterns following a morning dose of either LDX or placebo were described based on the CPRS-R:S. The CPRS-R:S consists of 27 parent-rated questions (items) and can be divided into four subscales: Oppositional, Cognitive Problems/Inattention, Hyperactive, and the ADHD Index. The CPRS-R:S ADHD Index subscale, which consists of 12 items yielding a maximum total score of 36, was used to assess ADHD core symptom control across the day. EL was assessed based on a nonvalidated composite EL score that included 3 items (i.e., angry/resentful, loses temper, and irritable) derived from the CPRS-R:S Oppositional subscale and had a maximum score of 9. These 3 items were chosen because they address spontaneous emotions rather than willful behavior, which is expressed by the 3 items not used—defiant, actively defies or refuses to comply with adult requests, and argues with adults. Each item of the CPRS-R:S is scored on a 4-point scale ranging from 0 (not true at all; never, seldom) to 3 (very much true; very often, very frequent); higher scores indicate more severe/frequent symptoms. CPRS-R:S ratings were obtained at baseline and at the last day prior to each participant’s weekly scheduled visits. Parents/caregivers were asked to rate their child’s behavior over the preceding 2 hr: in the morning (10 a.m.
Safety
The study safety parameters or primary safety data were collected for the safety population (all participants who were enrolled into the washout phase of the study or randomized without washout) throughout the study; these data were previously reported in detail (Biederman et al., 2007). Safety evaluations included treatment-emergent AEs (TEAEs), vital signs, laboratory tests, and electrocardiogram measurements. TEAEs referred to events with onset after the first date of double-blind treatment and no later than 3 days following termination of treatment. To further examine the relationship of emotional TEAEs to rebound, the frequency of emotion-related TEAEs was also assessed; this included, but was not limited to, anger, affect lability, flat affect, tearfulness, crying, and dysphoria.
Statistical Analysis
Changes from baseline at endpoint (last valid measurement obtained post-baseline) in the CPRS-R:S ADHD Index subscale and in the nonvalidated composite EL subscale scores were analyzed post hoc for the efficacy population (i.e., all participants with a baseline ADHD-RS-IV score and at least one valid postbaseline assessment), using an estimation model approach, based on LDX least squares (LS) mean difference from placebo, with 95% confidence intervals (CIs). Proportions of participants who showed clinically significant symptom response and rebound, based on CPRS-R:S ratings in the morning, afternoon, and evening, were tabulated based on the evaluable population (i.e., participants with both baseline and endpoint scores for one or more of the same assessment time points). Criteria used to define response and rebound were based on approaches previously used in clinical trials of medication treatment for ADHD (Carlson & Kelly, 2003; Stein et al., 2003; Swanson et al., 2001). For “response,” a total score of ≤12 on the ADHD Index subscale was chosen because this suggests most items are rated as “not at all true” or “just a little true/occasionally” and a score ≤1 for each ADHD Index subscale item ensures, on average, the absence of any isolated residual symptoms that are of a moderate or severe nature. For “rebound,” participants must have initially met the criteria for response, followed later in the day by a worsening of symptoms so that they no longer met response criteria and the ADHD Index subscale score was higher (more severe) than at baseline. For the response and rebound groups, descriptive statistics for CPRS-R:S ADHD Index and the EL subscale scores were calculated.
Results
Participant Demographics and Disposition
Detailed participant disposition and demographics/baseline characteristics were previously reported (Biederman et al., 2007). Of 290 randomized participants, 285 comprised the efficacy population (LDX, n = 213; placebo, n = 72). A total of 21 participants were discontinued due to TEAEs (all LDX doses, 20 [9.2%]; placebo, 1 [1.4%]). Overall baseline demographic/disease characteristics were similar across groups. Briefly, the majority of participants were male (62.2%-74.6%); ~50% were Caucasian (45.9%-59.7%); 12.5% to 23.0% were Hispanic/Latino; and 48.6% to 65.8% were 6 to 9 years old. Nearly all participants were diagnosed with ADHD combined subtype, with moderate to severe symptoms at baseline assessment. With regard to the CPRS-R:S, there were 279 evaluable participants at endpoint (LDX, n = 207; placebo, n = 72). Of note, at each CPRS-R:S time point (morning [10 a.m.], afternoon [2 p.m.], and evening [6 p.m.]), 2 to 3 participants missed assessments; therefore, response/nonresponse percentages may not equal 100%.
Efficacy
CPRS-R:S ADHD Index Subscale Scores
As shown in Figure 1, at study endpoint, ADHD core symptoms, as assessed based on mean CPRS-R:S ADHD Index subscale scores, were significantly improved in the combined LDX treatment group compared with the placebo group at the morning, afternoon, and evening assessment time points (all p < .0001).
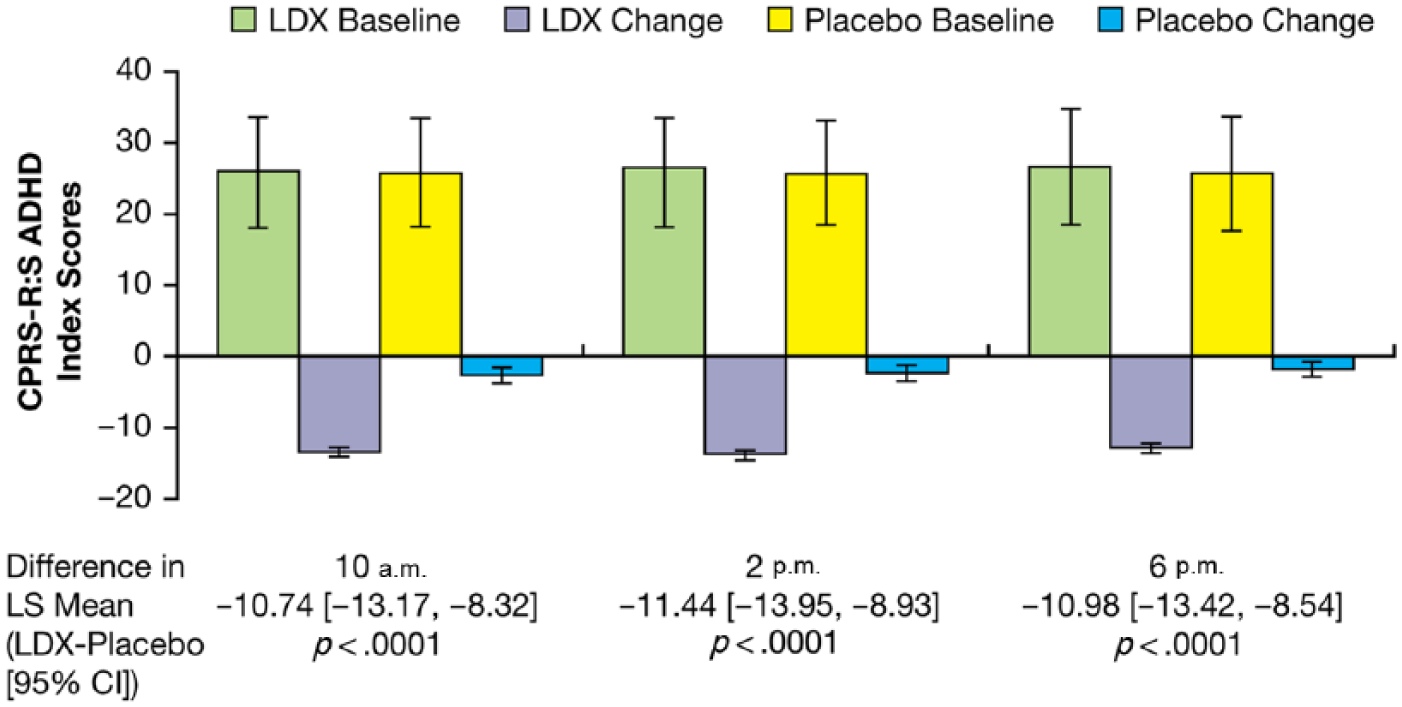
CPRS-R:S ADHD Index subscale scores at baseline (M [SD]) and change from baseline at endpoint (LS M [SD]).
Response and Rebound Analysis
Based on CPRS-R:S ADHD Index subscale scores, with LDX, approximately half (50.7%-55.6%) of evaluable participants met criteria for response at each time point examined across the day and at endpoint (Table 1). By contrast, with placebo, few participants met criteria for response at any of the time points assessed (11.1%-22.2%). As summarized in Table 1, mean (SD) ADHD Index scores were higher across the day in placebo responders than in LDX responders.
Characterization of Response and Rebound of ADHD Symptoms by Index and Emotional Lability Composite Scores.
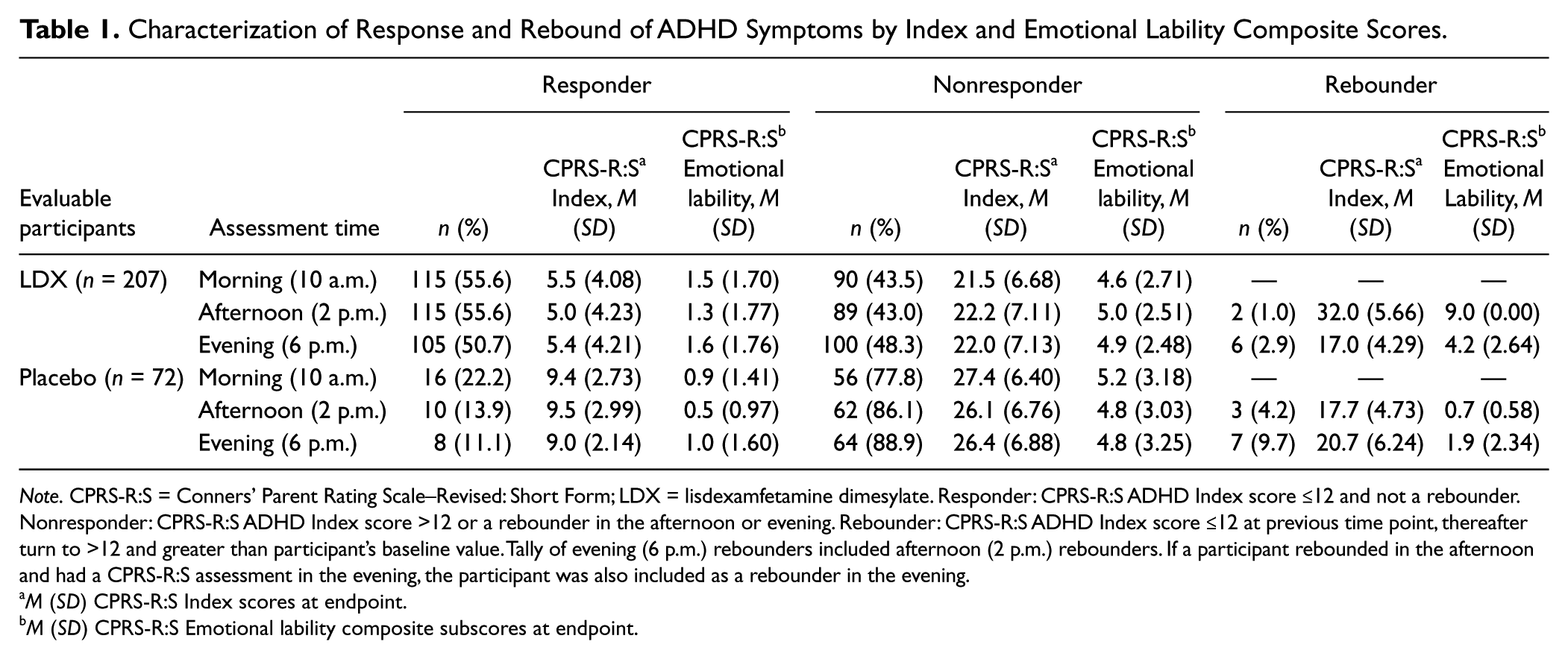
Note. CPRS-R:S = Conners’ Parent Rating Scale–Revised: Short Form; LDX = lisdexamfetamine dimesylate. Responder: CPRS-R:S ADHD Index score ≤12 and not a rebounder. Nonresponder: CPRS-R:S ADHD Index score >12 or a rebounder in the afternoon or evening. Rebounder: CPRS-R:S ADHD Index score ≤12 at previous time point, thereafter turn to >12 and greater than participant’s baseline value. Tally of evening (6 p.m.) rebounders included afternoon (2 p.m.) rebounders. If a participant rebounded in the afternoon and had a CPRS-R:S assessment in the evening, the participant was also included as a rebounder in the evening.
M (SD) CPRS-R:S Index scores at endpoint.
M (SD) CPRS-R:S Emotional lability composite subscores at endpoint.
Rebound was seen in seven (3.4%) LDX-treated participants and seven (9.7%) placebo-treated participants. Table 1 summarizes the rates of rebound seen in the afternoon and evening with LDX and placebo. One participant with rebound on LDX did not have an evening assessment at both baseline and endpoint, and therefore did not contribute to the mean scores at endpoint. Mean (SD) CPRS-R:S Index subscale scores were generally similar among rebounders and nonresponders in both the LDX and placebo groups (Table 1).
CPRS-R:S EL Composite Scores
With LDX, CPRS-R:S composite EL scores were significantly improved from baseline throughout the day and at endpoint (vs. placebo, all p ≤ .0004; Figure 2).
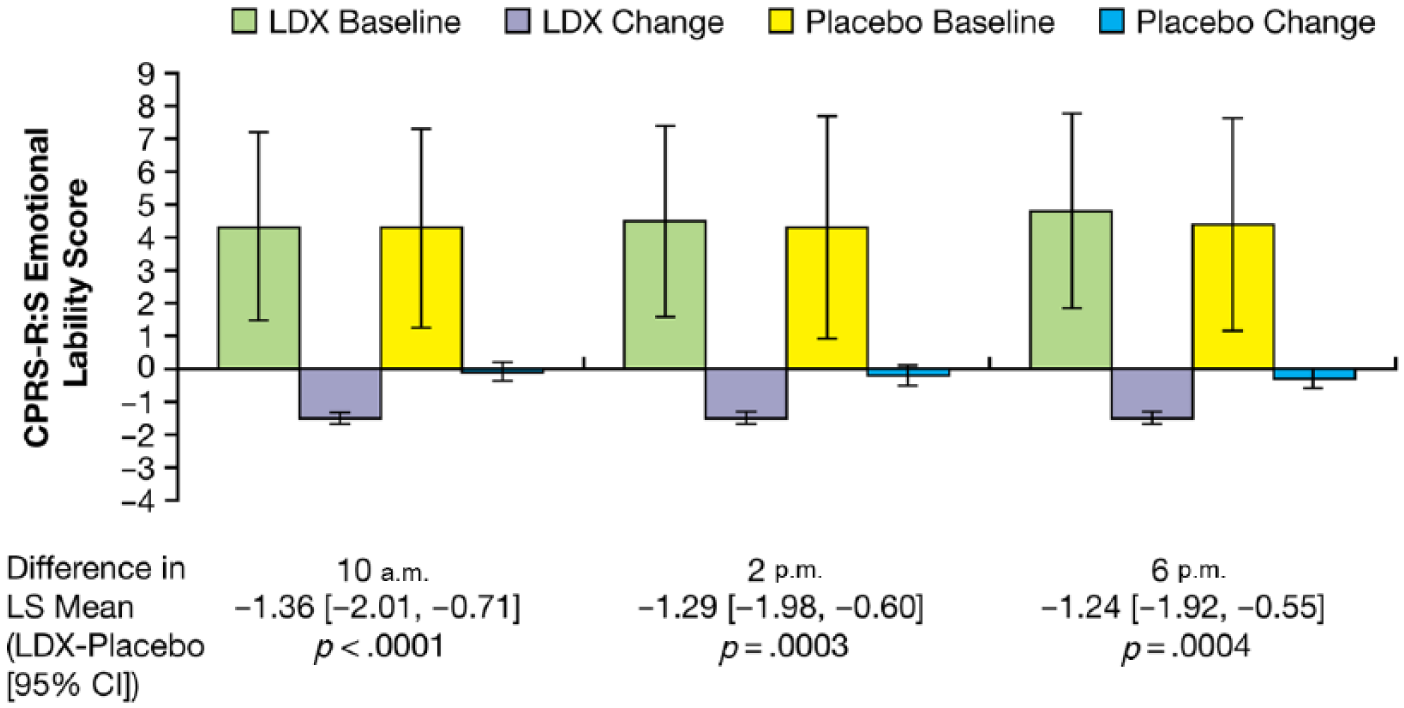
M (SD) CPRS-R:S Emotional Lability subscale scores at baseline and change from baseline at endpoint (LS M [SE]).
Results for participants who showed response, nonresponse, and rebound are presented in Table 1 as mean (SD) composite EL scores for each assessment time at endpoint. Responders in both the LDX and the placebo groups showed similar mean EL scores for each time point across the day and at endpoint. Nonresponders had higher mean EL scores than did responders at all time points (Table 1), regardless of treatment group. Rebounders on active drug, and not on placebo, had prominent emotional symptoms, as indicated by high CPRS-R:S–derived EL scores, along with their loss of ADHD symptom response (Table 1).
Safety
In the safety population (n = 290), 74.3% of participants on LDX (n = 218) and 47.2% of participants on placebo (n = 72) experienced TEAEs. Most TEAEs were mild or moderate in severity. Safety assessments, including TEAE frequency, have been reported in detail previously (Biederman et al., 2007). The most common TEAEs with LDX treatment (seen in ≥5% participants) are shown in Table 2 and included decreased appetite, insomnia, headache, and upper abdominal pain. Irritability, which may also accompany symptom rebound, was reported in 10% of participants who were assigned to LDX treatment. The occurrence of emotional TEAES was of interest as a possible indicator of rebound. In addition to irritability, noted above, emotional TEAEs reported with LDX treatment (Table 2) were affect lability (3.2%), anger (0.5%), crying (0.5%), dysphoria (0.5%), flat affect (1.4%), and tearfulness (1.8%). Because emotional TEAEs were reported exclusively in LDX-treated participants, determining if these events occurred specifically in LDX-treated rebounders was of interest. Further examination of individual participant TEAE reports showed that only two of seven LDX-treated rebounders exhibited emotional TEAEs, which included tearfulness, irritability, and agitation, indicating that not all the reported emotional TEAEs with LDX treatment were seen exclusively among rebounders. Moreover, none of the participants who showed rebound had a documented history of oppositional defiant disorder.
Incidence (%) of Any TEAE, TEAEs Occurring in ≥ 5% of Participants, and TEAEs Associated With Emotional Expression.
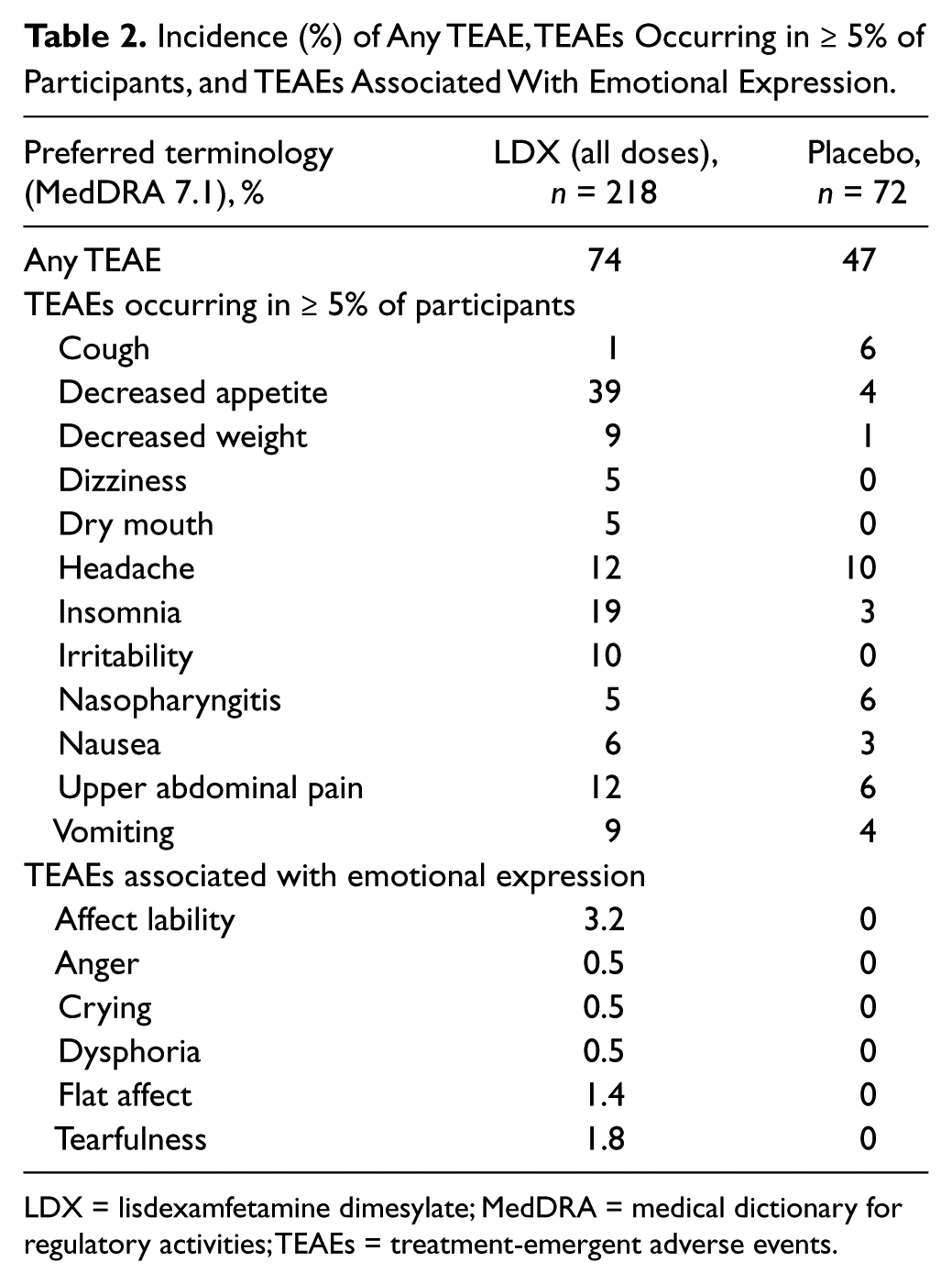
LDX = lisdexamfetamine dimesylate; MedDRA = medical dictionary for regulatory activities; TEAEs = treatment-emergent adverse events.
Discussion
Symptom rebound has been described as a phenomenon occurring in a subset of patients with ADHD when medication is wearing off, usually in the late afternoon and early evening (Carlson & Kelly, 2003; Sarampote et al, 2002) and marked by tearfulness and crying, belligerence, and worsening of ADHD symptoms beyond that seen prior to medication dosing (Barkley, 2006; Cox et al., 2008). Although this phenomenon may be highly clinically significant in some individuals, it remains largely unexamined. However, symptom rebound with stimulants remains a possibility. A similar phenomenon has been described using other types of substances, including analgesics (Vasconcellos, Pina-Garza, Millan, & Warner, 1998), caffeine (Strain, Mumford, Silverman, & Griffiths, 1994), and certain benzodiazepines (Oswald, French, Adam, & Gilham, 1982). With wear-off or withdrawal of these agents, target symptoms like pain, fatigue, or insomnia return and are more severe than prior to administration.
A beginning point to more objectively study symptom rebound is to define it, in general terms and operationally, allowing measurement and analysis within the context of a clinical trial. Working definitions of rebound have failed to differentiate stimulant-induced worsening in behavior from the natural course of untreated ADHD, where core symptoms of hyperactivity and impulsivity are more severe in the afternoon and evening hours than in the morning (S. R. Pliszka, Browne, Olvera, & Wynne, 2000). Moreover, as in the report from Johnston, Pelham, Hoza, and Sturges (1988), group outcome analyses have shown limited capacity to detect rebound. For the current analysis, to more accurately and precisely capture individual cases of true symptom rebound, participants were categorized as showing rebound only when they met stringent criteria for adequate therapeutic response prior to afternoon or late-day worsening of ADHD symptoms beyond the level seen at baseline. As such, participants given placebo were deemed unlikely to show adequate symptom improvement and therefore also less likely to falsely meet criteria for rebound. Deterioration in behavior was based on ADHD core symptoms and excluded emotional symptoms, which may occur as a TEAE with stimulant treatment or with psychiatric comorbidity. With the resulting operational definition, rebound in core ADHD symptoms following LDX administration was infrequent, with only 3.4% of LDX participants and 9.7% of placebo-treated participants meeting this criterion. Although the small numbers of participants in these groups limit the ability to draw reliable comparisons, ADHD Index subscale scores among LDX and placebo rebounders were generally similar. In addition, the rate of symptom rebound was higher with placebo than with LDX. Symptom rebound may result from wearing off of stimulant effects and may result from other causes, including end-of-day worsening of symptoms in the untreated patient with ADHD. The criteria for symptom rebound in this study required that symptoms improved relative to baseline and subsequently worsened beyond the baseline state. The finding of rebound in participants taking placebo suggests that criteria for trial inclusion or therapeutic response captured some proportion of placebo group participants who only exhibited mild ADHD symptom scores at baseline, so that even small improvements early in the day were categorized as response; subsequent symptom worsening during the day, consistent with untreated ADHD, likely resulted in being categorized as “rebound.”
The low frequency of rebound with stimulant treatment seen in this analysis is similar to that in reports from Johnston et al. (1988) and Carlson and Kelly (2003), who also observed significant rebound in subsets of their patient samples. Both in the current study and in the trial from Johnston et al., evening rebound was identified based on worsening of core ADHD symptoms following treatment with stimulants. The similarity with findings from Carlson and Kelly (2003), while encouraging, is nonetheless surprising, as these investigators defined rebound not based on ADHD symptoms, but rather on ratings of nonspecific, largely emotional symptoms that included crying, irritability, sadness, insomnia, and euphoria. For the sample as a whole, LDX treatment (vs. placebo) significantly decreased mean EL scores at endpoint. In LDX-treated rebounders, however, average EL scores were more than threefold higher during the rebound time period, compared with EL scores at the same time point in LDX-treated participants who were responders. Some evidence suggests that high levels of EL are associated with more severe core ADHD symptoms and comorbid psychopathology (Sobanski et al., 2010). Further research is needed to determine whether elevated EL scores at baseline may predict rebound and to more fully describe the nature of the relationship between core ADHD symptoms, EL, and responsiveness to stimulant therapy.
LDX demonstrated a safety profile similar to other long-acting psychostimulants. Emotional TEAEs seen with LDX but not placebo, with the exception of irritability, were infrequent and not specifically related to rebound. This suggests that the EL symptoms seen currently in LDX rebounders were not reported by parents/caregivers as TEAEs, raising the question of whether these symptoms were present at baseline in some of these participants. This is also in agreement with other reports showing a low reported frequency of rebound-related emotional AEs with stimulant treatment (Swanson et al., 2004; Weisler et al., 2006; Wilens et al., 2006). It bears noting that if emotional symptoms were not present prior to treatment, they may more appropriately be considered TEAEs, and not rebound per se, particularly if they are seen in patients with poor therapeutic response or if they do not occur specifically at the time of medication wear-off. Such findings highlight the difficulty in detecting rebound based on AE profiles and in understanding the relationship between EL and core ADHD symptoms.
The current findings should be considered in light of certain limitations. The ability to generalize these findings to clinical situations may be limited by certain study design features, such as the exclusion of individuals with predominantly inattentive ADHD subtype and those with psychiatric comorbidity, the short, 4-week treatment period, and forced-dose titration of LDX. These were exploratory post hoc analyses and were limited to descriptive statistical comparisons. The study sample was not prospectively powered to detect differences among the response, nonresponse, and rebound subgroups examined. Some subgroups were small in size and showed substantial variability in ADHD Index subscale and EL composite scores. Assessments of core ADHD symptoms and EL were based on subjective ratings from parents, who may have been able to discern whether their child was in the active treatment group versus the placebo group. Finally, LDX has been found to improve symptoms from 13 hr after dosing in children (S. B. Wigal, Kollins, Childress, & Squires, 2009) and 14 hr in adults (T. Wigal et al., 2010). CPRS-R:S parent ratings were obtained on average up to 10 to 10.5 hr postdosing. This may have decreased the ability to observe rebound that may have emerged during medication wear-off at later, nonassessed time points.
Further research into the presentation of ADHD symptom rebound both in clinical trials and clinical practice is substantially needed. In particular, the factors that may influence the likelihood of occurrence including age and sex, and aspects of presentation such as frequency versus severity are poorly understood. Importantly, further clinical research into ADHD symptom rebound would benefit greatly from developing a comprehensive, consistent, and accepted definition and clearly defined clinical correlates. Many questions also remain to be resolved regarding the relationship of rebound to core ADHD symptoms and EL. It is unclear whether rebound is always marked by worsening of both core symptoms and EL, or if a subset of patients may experience worsening of one but not the other. If we follow this approach, we would have to distinguish between symptom rebound alone and symptom rebound with EL. If worsening of ADHD symptoms and emotional symptoms were found to co-occur in the majority of cases, then it may be appropriate to characterize “rebound” as involving these two conditions.
Conclusion
Using the current exploratory definition of rebound, in which core ADHD symptom response is followed by late-day worsening, rebound with treatment with the long-acting stimulant LDX was infrequent (3.4%) and was accompanied by prominent EL symptoms. Overall, approximately half the evaluable participants (50.7%-55.6%) receiving LDX met criteria for response at each time point examined across the day at endpoint, while with placebo, few participants (11.1%-22.2%) met criteria for response at any of the time points assessed.
Footnotes
Authors’ Note
Under the direction of the authors, Michael Pucci, PhD, and Karen Dougherty, PhD, employees of SCI Scientific Communications and Information (SCI) provided writing assistance for this publication. Editorial assistance in formatting, proofreading, copy editing, and fact checking was also provided by SCI. Shire Development LLC provided funding to SCI for support in writing and editing this manuscript. Although the sponsor was involved in the design, collection, analysis, interpretation, and fact checking of information, the content of this manuscript, the ultimate interpretation, and the decision to submit it for publication in Journal of Attention Disorders were made by the authors independently.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Frank A. López receives or has received research support and acted as a consultant and/or speaker for New River Pharmaceuticals, Shire US, Novartis, Noven, Eli Lilly, Bristol-Myers Squibb, Cephalon, Pfizer, Celltech-Medeva. He has participated on Speakers Bureau for Shionogi, Novartis, Noven, Shire US and have participated on Advisory Boards for Novartis, Shire US, Shire Canada, Cephalon. Dr. Lopez had received honoraria from Speakers Bureau and from the aforementioned Advisory boards. He holds no stock in any Pharmaceutial company.
Ann Childress receives or has received research support and acted as a consultant and/or speaker for Abbott, Bristol-Myers Squibb, GlaxoSmithKline, Johnson & Johnson Pharmaceutical Research & Development, LLC, Lilly USA, LLC, NextWave, Novartis, Ortho-McNeil Janssen Scientific Affairs, Rhodes, Sepracor, Shire, Somerset, Sunovion and Pfizer.
Ben Adeyi is an employee of Shire and holds stock and/or stock options in Shire.
Bryan Dirks is an employee of Shire and holds stocks and/or stock options in Johnson & Johnson and Shire.
Thomas Babcock is an employee of Shire and holds stock and/or stock options in Shire.
Brian Scheckner is an employee of Shire and holds stock and/or stock options in Shire.
Robert A. Lasser was employee of Shire from 2008-July 2012, who held Shire stock and stock options and, from July 2012 to present is an employee of Pharmanet/i3, an inVentiv Health clinical. John Shepski is an employee of Shire and holds stock and/or stock options in Shire.
Valerie Arnold participates or has participated on clinical trials with AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, CeNeRx, Eli Lilly, Euthymics, Forest, Johnson & Johnson, Indevus, Merck/Schering Plough, Novartis, Otsuka, Pfizer, Purdue, Repligen, Rexahn, Roche, Sanofi, Sepracor, Shionogi, Shire, Sunovion, Supernus, Takeda, Targacept, Vanda and is also a member of the Shire advisory group.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The clinical research was funded by the sponsor, Shire Development LLC.