
Abstract
Background
The impact of disease and the effect of treatment can be assessed using outcome measures of health status, functional impairment, and health-related quality of life (HRQoL; Coghill, Danckaerts, Sonuga-Barke, & Sergeant, 2009). HRQoL, defined by the World Health Organization (WHO) as “the individual’s perception of their position in life, in the context of culture and value systems in which they live, and in relation to their goals, expectations, standards and concerns” (WHO, 1997), is becoming an ever more important outcome parameter in psychiatry, especially in cases when medication management can be accompanied by negative long-term outcomes that reduce the overall quality of life (Coghill, 2010). Instruments to measure HRQoL are increasingly being used to assist clinicians to identify areas of life that are particularly difficult for an individual, to tailor support provided, and in the estimation of treatment cost-effectiveness and reimbursement decisions (Coghill, 2010; Coghill et al., 2009).
ADHD, the most common childhood-onset psychological disorder, estimated to affect 5% to 7% of children worldwide (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007; Willcutt, 2012), has been shown to have a significant impact on multiple domains of HRQoL in children and adolescents (Coghill, 2010; Klassen, Miller, & Fine, 2004). Two HRQoL domains, self-esteem and social function, were identified among nine categories of outcome measures most commonly used to examine the long-term impact of ADHD (Hodgkins et al., 2011). Self-esteem outcomes include increased negative beliefs about the self that can lead to individuals developing maladaptive coping strategies, including avoidance and procrastination, and untreated ADHD has been associated with decreased social functioning skills, including poor peer or familial relationships, riskier sexual activity, and increased peer victimization/bullying (Asherson et al., 2012; Hosain, Berenson, Tennen, Bauer, & Wu, 2012; Mrug et al., 2012; Newark & Stieglitz, 2010; Sciberras, Ohan, & Anderson, 2012). Outcome measures such as self-esteem and social function are valuable as they provide an assessment of functional impairment, which is a requirement for ADHD diagnosis, in addition to the characteristic symptoms of inattention, impulsivity, and hyperactivity (American Psychiatric Association [APA], 2000; WHO, 1992). Impairments associated with ADHD include those in social, emotional, academic, and behavioral functioning (DuPaul, McGoey, Eckert, & VanBrakle, 2001; Wilson & Marcotte, 1996). ADHD-related symptoms and impairments continue through adolescence into adulthood in some individuals (Biederman, Mick, & Faraone, 2000; Faraone, Biederman, & Mick, 2006), with estimates for the prevalence of ADHD in adults ranging from 1.2% to 4.4% (Faraone et al., 2006; Kessler et al., 2006).
While the cost-effectiveness of current ADHD pharmacotherapy has been established (Wu et al., 2012), the long-term benefits of therapy have not been readily acknowledged by Health Technology Assessment Agencies (Canadian Agency for Drugs and Technologies in Health, 2011; National Institute for Health and Clinical Excellence, 2009; Nutt et al., 2007; Scottish Collegiate Guidelines Network, 2009). Recent systematic reviews described improvement in HRQoL associated with effective treatment in children, adolescents, and adults with ADHD; however, these reviews focused predominantly on clinical studies, introducing the possibility of bias and reducing the generalizability of findings (Coghill, 2010; Danckaerts et al., 2010). Nonnarrative reviews that provide a comprehensive assessment and understanding of long-term outcomes, in general and for self-esteem and social function outcomes in particular, in individuals with treated or untreated ADHD are lacking.
Objectives
The objectives of this systematic review were to assess how self-esteem and social function are impaired in ADHD; to compare the long-term outcomes of untreated and treated ADHD in childhood, adolescence, and adulthood; and to identify any factors (e.g., the effect of treatment, geographic region, age, reporter, and gender) that affect self-esteem and social function.
Method
Search Method
Long-term outcomes of children, adolescents, and adults with ADHD, who were either receiving or had received treatment of some kind (pharmacological, nonpharmacological, or multimodal treatment [MMT]), or were untreated (no documented past or present treatment), were identified through an extensive, systematic literature search of 12 databases. Long-term outcomes were defined as those ≥2 years (MTA Cooperative Group, 2004) and were distinct from the reporting of symptoms.
Eligibility Criteria and Search Strategy
Inclusion Criteria
Peer-reviewed, primary research articles published in English between January 1980 and December 2011 for which full text was available were identified from 12 databases using the electronic search engines and search strategy described in online Appendix 1. Studies were selected using criteria adapted from Hodgkins et al., 2011. Studies were eligible for inclusion if they involved individuals with a diagnosis of ADHD, or presenting with ADHD symptomatology, using any diagnostic criteria as reported by the authors of each study; if the primary disorder under investigation was ADHD, and if the study used a comparator group (e.g., non-ADHD controls) or comparison measure (e.g., pretreatment baseline assessments). Longitudinal studies were eligible for inclusion if prospective follow-up or retrospective measures were for ≥2 years. Cross-sectional studies of individuals aged ≥10 years were also eligible for inclusion. The minimum age for cross-sectional studies was set at 10 years based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) diagnostic criterion that symptoms are present before the child is 7 years old. Assessing outcomes at ≥10 years of age allowed a minimum of 2 years to elapse, in line with the definition of “long-term” being ≥2 years. Only studies reporting self-esteem and/or social function outcomes were included in this systematic review.
Exclusion Criteria
Studies examining symptoms only and not self-esteem or social function outcomes, studies in which ADHD was not a primary condition of the study participants but was secondary to another condition (e.g., Down’s syndrome or autism), meta-analyses and literature review studies, and studies reporting results for an instrument (e.g., instrument validation studies) were excluded from the analysis.
Search Strategy for Study Identification
The search strategy for study identification and study protocol has been previously published (Hodgkins et al., 2011) and details are provided in Appendix 1.
Data Analysis
Definition of Outcomes
This review focuses on self-esteem and social function outcomes as measured using the assessments listed in Appendix 2. Broad themes for self-esteem outcomes included measures of self-perception, self-concept, psychological well-being, self-worth, and self-image. Broad themes for social function outcomes included measures of social and familial relationships, work and school relationships, social skills, participation in social activities, living arrangements, dating and marital history, and sexual behavior.
Results reported in each study were summarized as a single self-esteem or social function outcome and were dichotomized as being similar to or poorer than the comparator (e.g., non-ADHD control group). Data were then analyzed by outcome; a single study may have reported results for self-esteem and social function, and would therefore contribute both a self-esteem and a social function outcome to this analysis. Results were categorized as “poorer” outcomes if they were statistically significantly worse than the comparator, or if they were recorded by the authors as worse than the comparator without the need for statistical comparison (e.g., a Norwegian study found that 80% of the male study population with ADHD was unemployed, compared with a concurrent unemployment rate for males of 3.5%; Rasmussen & Levander, 2009). Results that were not statistically significantly different from the comparator were categorized as “similar” outcomes. Outcomes that were statistically significantly better than the comparator were grouped with the “similar” outcomes in this analysis due to the small number of outcomes of this type.
A comparison of treated ADHD versus untreated ADHD was conducted in which “untreated ADHD” comparators included pretreatment baseline assessments and a group of individuals with untreated ADHD. Treatment was considered beneficial if there was a statistically significant improvement compared with untreated ADHD comparators. Treatment was considered of no benefit if there was no statistically significant difference compared with untreated ADHD comparators, or if there were poorer outcomes compared with untreated ADHD comparators. Analysis of the studies that reported only results with treatment compared with non-ADHD controls was performed separately. Treatment types included pharmacological treatment, nonpharmacological treatment (e.g., cognitive behavioral therapy), or MMT (i.e., a combination of drug and nondrug treatment). No minimum therapy duration was required for classification as treatment.
The extent of treatment benefit was examined using effect sizes that were either reported in the study or were derivable based on the information provided. Cohen’s d was calculated for continuous measures for which the mean and standard deviation (SD) were reported, such as scores on a social function scale. Cohen’s w was calculated for discrete measures of incidence, such as the number of people who were married, often derived from the related reported chi-square statistic.
Treatment outcomes vary considerably by age; therefore, data were analyzed by age group. The categorization of each study by age group (children 6-12 years; adolescents 13-17 years; young adults 18-24 years; adults ≥25 years) was primarily based on the midrange age of study participants at follow-up. The majority of studies reported participant age ranges; mean age was used for studies that did not report age range.
For geographic location, studies were grouped according to the UN Geoscheme (United Nations Statistics Division, 2012) and placed into the following categories: Northern America (United States and Canada excluding Mexico), Europe, Eastern Asia, Western Asia, Australasia (New Zealand and Australia), and Latin America (including Mexico), and the Caribbean.
Statistical Analyses
Effect sizes were calculated using Cohen’s d (from the difference between means divided by the pooled SD of the means) and Cohen’s w (from the square root of the reported χ2 divided by the study population or from a 2 × 2 contingency table; Cohen, 1988). Effect sizes reported or derivable as Cohen’s d index compared with pretreatment baseline were statistically compared among treatment modalities using SYSTAT 12 (Systat Software, Inc., Chicago, Illinois, USA). Two-sample, two-tailed t tests with separate variance, which does not assume homoscedasticity, were used to compare groups. A Type 1 error adjustment for multiple comparisons was used and the alpha level was set at .017.
Results
Details of studies included in this systematic review and reasons for exclusion are provided in Figure 1. A complete list of references reporting social function and/or self-esteem outcomes is provided in Appendix 3.
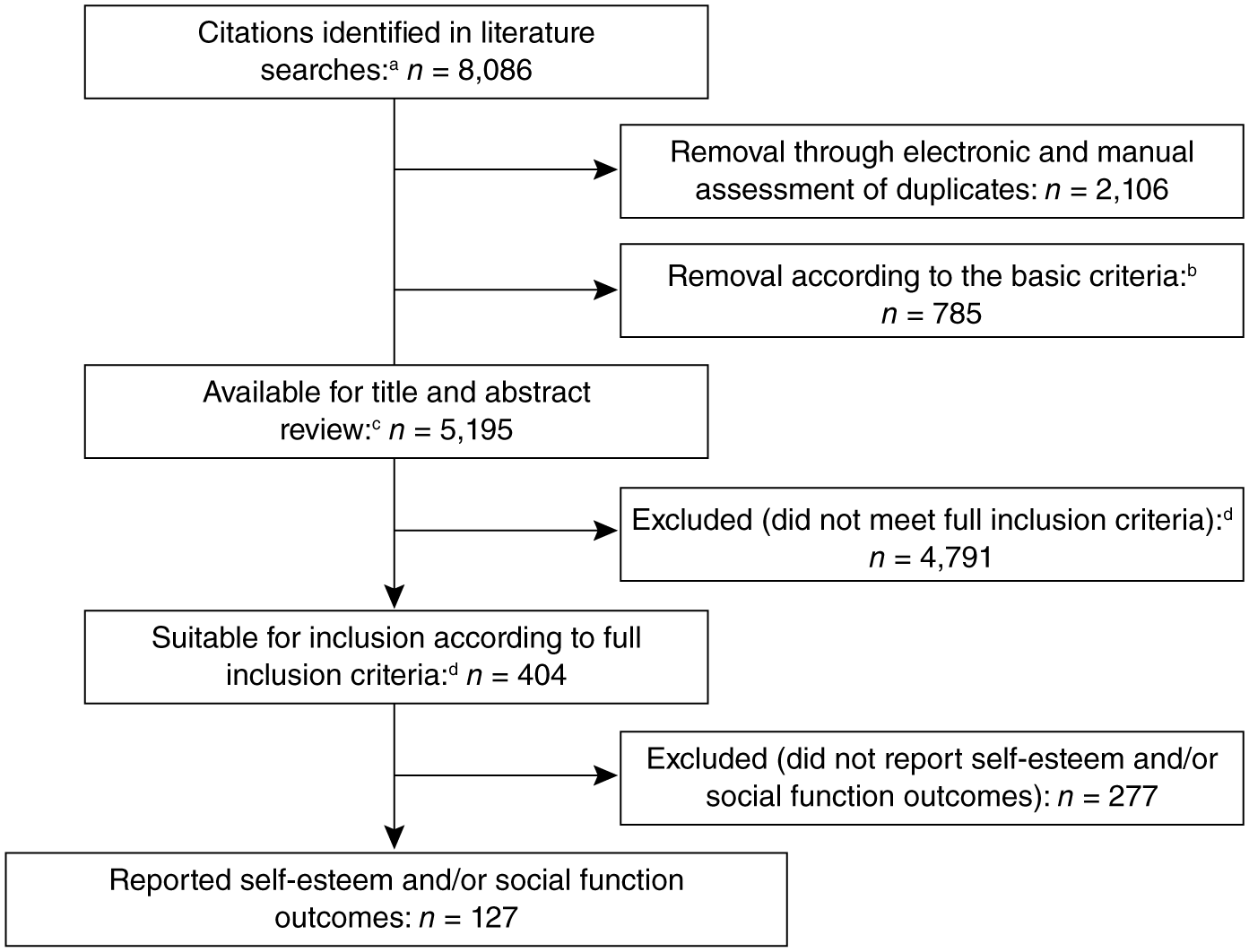
Flow diagram of screened and included studies.
Of the 127 studies included in the analysis, the sample size ranged from 12 to 8,158 individuals; longitudinal study duration ranged from 2 to 25 years, with a mean (median) duration of 7.4 (5) years.
The publication rate of articles on self-esteem and/or social function in ADHD has risen relatively steadily since 1980, with a total of 127 studies reporting 150 outcomes (the total number of outcomes is greater than the total number of studies because some studies reported self-esteem and social function outcomes; Figure 2).
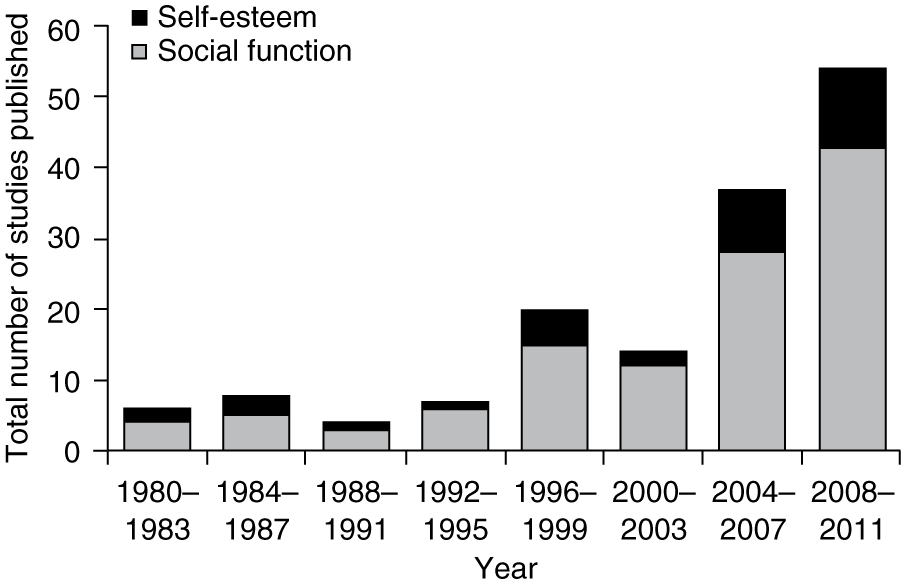
Total studies reporting self-esteem and social function outcomes published within 4-year spans.
There was a higher proportion of publications reporting self-esteem versus social function outcomes in Eastern Asia compared with Northern America, Europe, and “Other” regions (Table 1); however, the number of studies in Eastern Asia was low. The number of studies from “Other” regions (Turkey, Israel, Australia, and New Zealand) was also low, but the proportion of studies reporting self-esteem versus social function outcomes was similar to that of Northern America and Europe.
Number of Self-Esteem and Social Function Outcomes Reported by World Region.
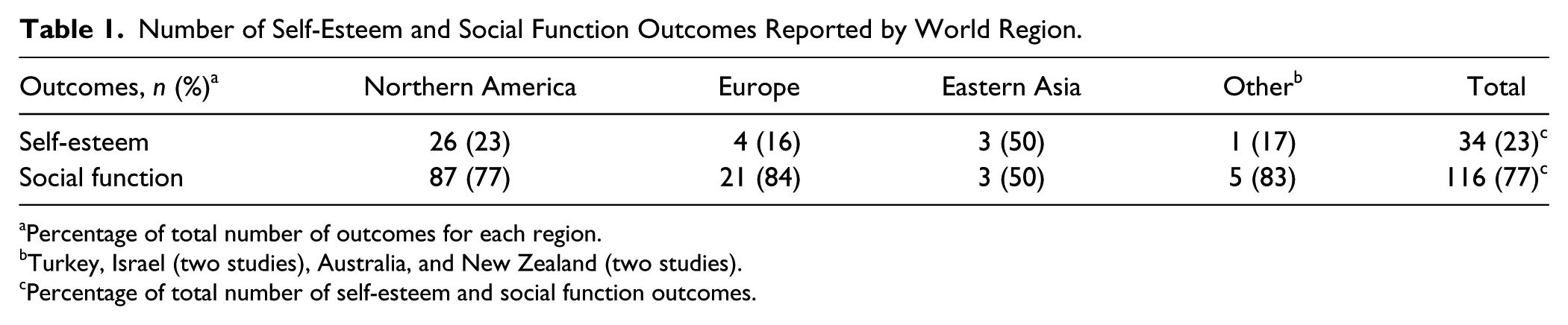
Percentage of total number of outcomes for each region.
Turkey, Israel (two studies), Australia, and New Zealand (two studies).
Percentage of total number of self-esteem and social function outcomes.
There were two social function outcomes for individuals with untreated ADHD that were reported to be significantly better than non-ADHD controls, and were included in the “similar” outcome group. These included one study that reported better social relationships at work in individuals with untreated ADHD compared with non-ADHD controls (Ercan, Coskunol, Varan, & Toksoz, 2003), and another study that reported significantly more social milestones gained for individuals with treated ADHD compared with non-ADHD controls (Canu & Carlson, 2007). Regression analysis demonstrated that there were no notable medication effects in this study, implying that untreated and treated individuals were functioning equally well and that the type of medication had no impact on this outcome. A third study reported that college students with treated ADHD were more likely to belong to collegiate Greek social organizations than non-ADHD controls (a result presented by the authors as a positive indicator of social function; Advokat, Lane, & Luo, 2011).
Untreated ADHD Outcomes
Figure 3 shows the self-esteem and social function outcomes for individuals with untreated ADHD compared with non-ADHD controls. Individuals with untreated ADHD had a higher percentage of self-esteem and social function outcomes that were poorer compared with non-ADHD controls (57% and 73%, respectively) than outcomes that were similar to non-ADHD controls (43% and 27%, respectively). The number of reported self-esteem outcomes was low and all were self-reported, except for one study in which parents reported a poorer outcome for untreated ADHD compared with non-ADHD controls.
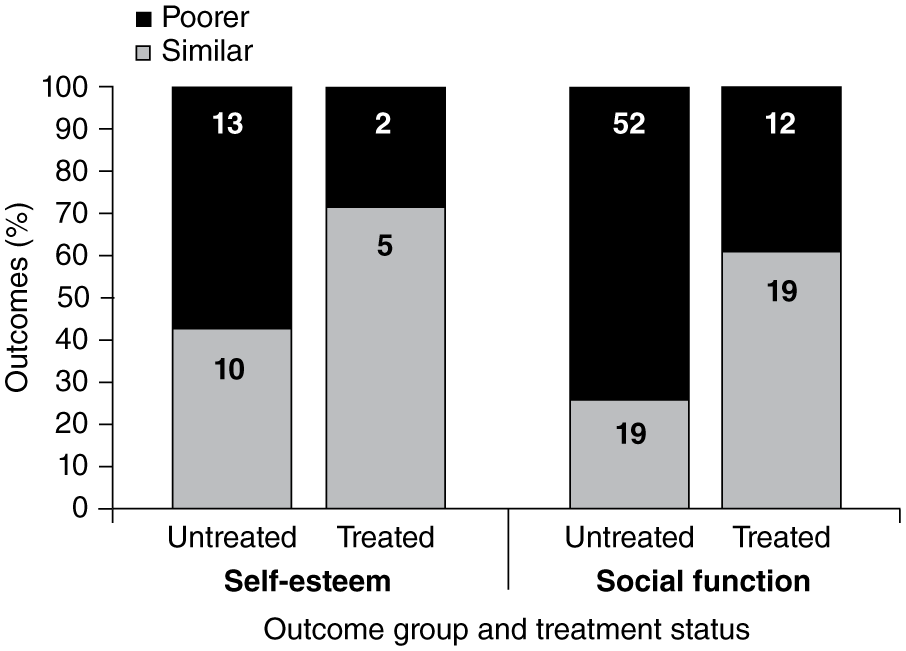
Self-esteem and social function outcomes for individuals with untreated and treated ADHD, compared with non-ADHD individuals.
Whereas self-esteem outcomes were measured using questionnaires assessing the individual’s feelings about himself or herself, social function outcomes were generated from many different domains and instruments/reporters. Studies often measured more than one aspect of social functioning, and four main domains (relationships, social skills, living arrangements, and activities/hobbies) were identified within the social function outcome group. The majority of outcomes relating to activities/hobbies (8/11; 73%), relationships (41/58; 71%), and social skills (17/26; 65%) were poorer compared with non-ADHD controls, and these areas were the main drivers of the overall negative effect of untreated ADHD on social function. In contrast, fewer poorer outcomes were reported for living arrangements (2/6; 33%).
Untreated ADHD Outcomes: Effect of Age Group
A high proportion of poorer outcomes was reported for individuals with untreated ADHD compared with non-ADHD controls across all age ranges (Figure 4). The overall proportion of poorer outcomes was highest for children (87%) followed by adults (aged ≥25 years; 70%), adolescents (69%), and young adults (aged 18-24 years; 50%). Overall proportions were largely driven by social function outcomes, for which all (100%) reported outcomes for children were poorer compared with non-ADHD controls (Figure 4). A lower proportion of reported social function outcomes was poorer for adolescents (82%), adults (70%), and young adults (46%; Figure 4). In contrast, the proportion of poorer self-esteem outcomes was highest in adults (71%) and young adults (67%), and lowest in children (50%) and adolescents (44%).
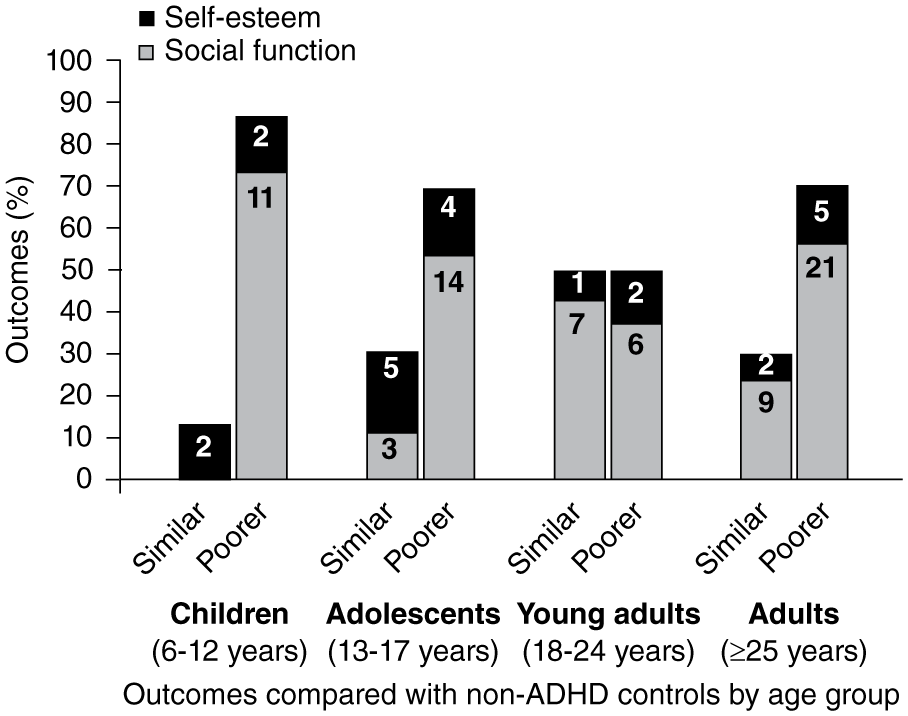
Self-esteem and social function outcomes for individuals with untreated ADHD compared with non-ADHD controls by age group.
Untreated ADHD Outcomes: Effect of Reporter
Differences in outcomes between individuals with untreated ADHD and non-ADHD controls were apparent according to the reporter (Table 2). As stated above, all self-esteem outcomes were self-reported, except for one parent-reported outcome. For social function, self-reported outcomes were most common (n = 57), of which 65% were poorer compared with non-ADHD controls (Table 2). All outcomes reported by peers (100%), and the majority of teacher-reported (89%) and parent-reported (78%) outcomes, were poorer compared with non-ADHD controls.
Social Function Outcomes for Individuals With Untreated ADHD and Treated ADHD, by Reporter.
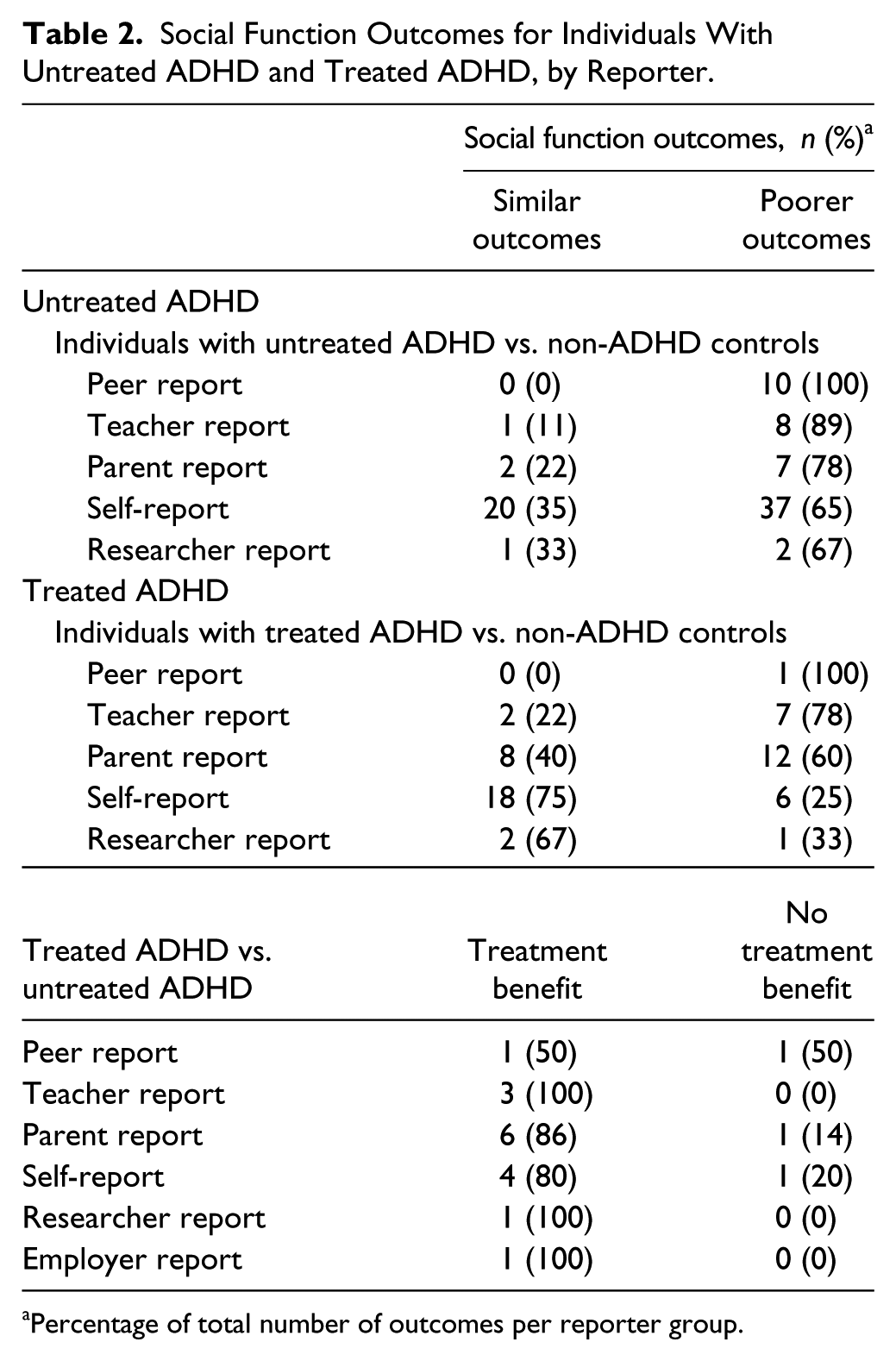
Percentage of total number of outcomes per reporter group.
Untreated ADHD Outcomes: Effect of Gender
The majority of self-esteem outcomes reported for males (4/6; 67%) and females (5/7; 71%) with untreated ADHD were poorer compared with non-ADHD controls. Poorer social function outcomes were also more commonly reported for males (13/20; 65%) and females (10/14; 71%) with untreated ADHD. Results were in keeping with the overall results for untreated ADHD versus non-ADHD controls (Figure 3), and no gender effects were observed.
Untreated ADHD Outcomes: Effect of Region
Compared with non-ADHD controls, outcomes for social function and self-esteem in individuals with untreated ADHD in Northern America (Canada and USA; United Nations Statistics Division, 2012) and Europe were similar to the overall results shown in Figure 3.
Effect of Treatment on Outcomes
The effects of treatment were reported in 52 studies (64 outcomes reported in total; 15 self-esteem outcomes and 49 social function outcomes); all self-esteem outcomes were self-reported.
A beneficial treatment response was evident in the majority of self-esteem (8/9; 89%) and social function outcomes (17/22; 77%) reported for individuals with treated ADHD versus those with untreated ADHD (Figure 5). Effect sizes indicating the degree of treatment benefit were reported in, or derivable for, 12 studies (26 effect sizes were Cohen’s d, 3 were Cohen’s w; 26 were improvements compared with pretreatment baseline; 3 were improvements compared with untreated individuals with ADHD; 6 were for self-esteem measures; and 23 were for social function measures). Overall, effect sizes ranged from small (d = 0.3) to large (d = 1.7). There were 25 Cohen’s d effect sizes for improvement in outcomes compared with pretreatment baseline, of which 4 were for self-esteem measures (mean d = 1.3, SD = 0.2), and 21 were for social function measures (mean d = 0.9, SD = 0.4). Mean Cohen’s d values for improvement above pretreatment baseline did not differ statistically by any comparison (all p ≥ .095) when analyzed separately for different treatment modalities; however, the possibility of a Type 2 error must be acknowledged because of the small sample sizes (n = 8, mean d = 0.9, SD = 0.4, for pharmacological; n = 4, mean d = 0.7, SD = 0.3, for nonpharmacological; and n = 13, mean d = 1.0, SD = 0.4, for MMT). There were only three Cohen’s w values and three effect sizes for improvement compared with untreated individuals, so these were not evaluated further.
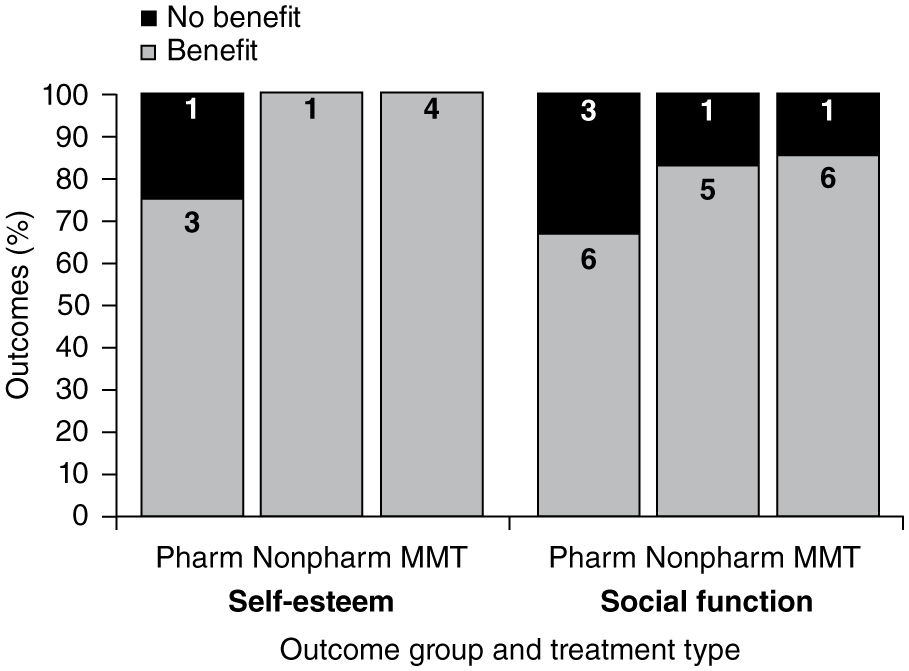
Benefit of treatment by treatment type for self-esteem and social function outcomes.
Response to treatment across treatment types (pharmacological, nonpharmacological, and MMT) for self-esteem and social function outcomes was similar, with benefit from treatment in self-esteem reported for all but one outcome (75%-100% across all treatment types), and in social function reported for 67% to 86% of outcomes (Figure 5). The number of outcomes reported was low when stratified by treatment type, however, with only one self-esteem outcome reported for nonpharmacological treatment.
Individuals With Treated ADHD Compared With Non-ADHD Controls
The reported outcomes of individuals with treated ADHD compared with outcomes from non-ADHD controls were examined. For the self-esteem category, 71% of outcomes were similar to the non-ADHD control group following treatment (Figure 3), compared with 43% for individuals with untreated ADHD. Likewise, for the social function category, 61% of the outcomes measured post-treatment were similar to the non-ADHD control group (Figure 3), compared with 26% for individuals with untreated ADHD.
Treated ADHD Outcomes: Effect of Age Group
The majority of studies reporting self-esteem and social function outcomes in individuals with treated ADHD versus untreated ADHD were in children, with fewer studies in adolescents and adults. All self-esteem outcomes in children and adolescents showed improvement following treatment, as did 6/8 social function outcomes in children and 5/5 social function outcomes in adolescents (Table 3). For young adults aged 18 to 24 years, there was one reported outcome of treatment benefit and one of no treatment benefit for self-esteem and social function. There were no studies in adults aged ≥25 years.
Treatment Benefit by Age Group: Within-Study Comparisons of Outcomes Reported for Individuals With Treated ADHD Versus Outcomes Reported for Individuals With Untreated ADHD.
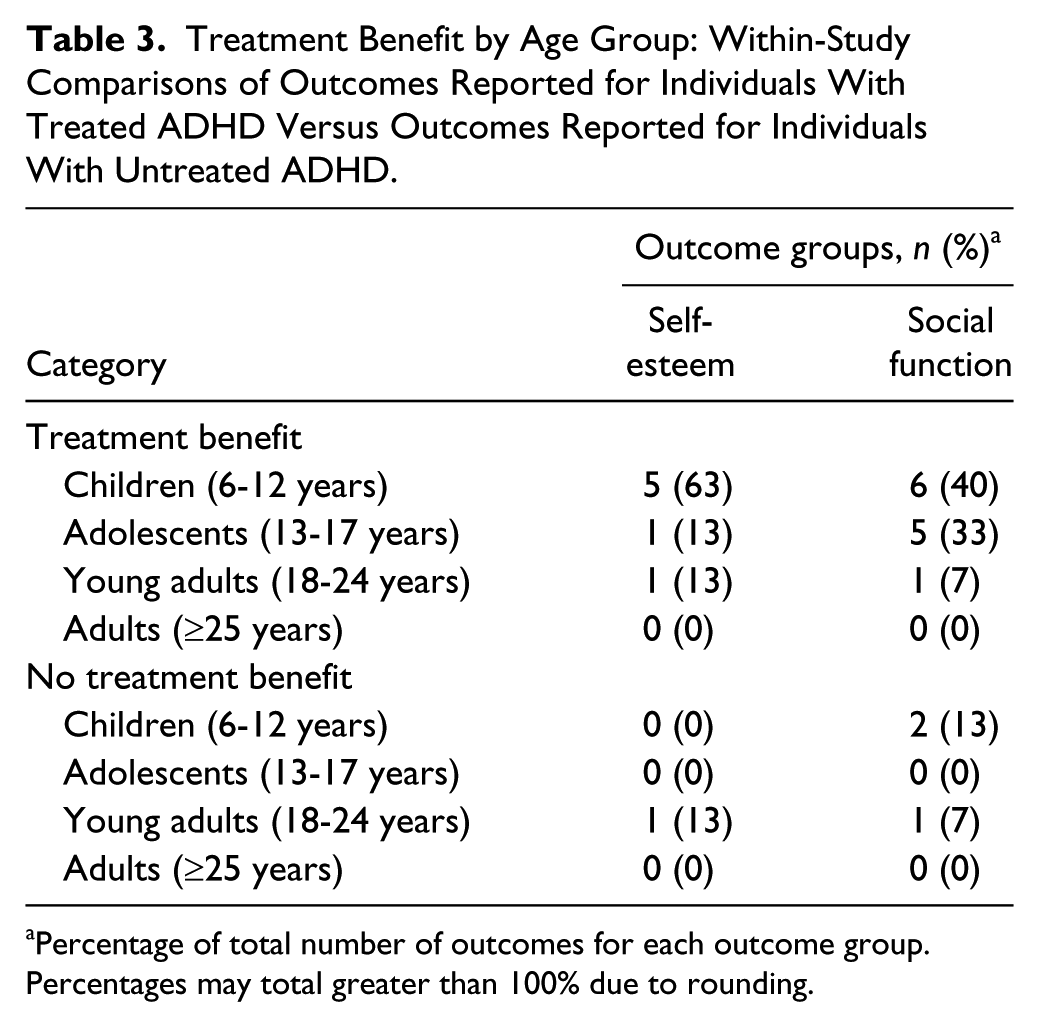
Percentage of total number of outcomes for each outcome group. Percentages may total greater than 100% due to rounding.
Treated ADHD Outcomes: Effect of Reporter
Differences in reported outcomes for individuals with treated ADHD versus non-ADHD controls, and versus individuals with untreated ADHD, were examined by type of reporter. At this level of analysis, study numbers were low for some comparisons and self-esteem outcomes were all self-reported. Most social function outcomes were also self-reported, the majority of which were similar to those of non-ADHD controls (75%; Table 2), and showed benefit with treatment when compared with untreated ADHD (80%; Table 2). Peer-reported, teacher-reported, and parent-reported outcomes for individuals with treated ADHD were more likely to be poorer compared with non-ADHD controls than self-reported or researcher-observed outcomes (Table 2). While the number of outcomes reported for individuals with treated ADHD versus untreated ADHD was low, improvement with treatment was reported for 50% to 100% of social function outcomes, regardless of the reporter of the outcome (Table 2).
Treated ADHD Outcomes: Effect of Gender
For self-esteem, 1 of 2 outcomes were similar compared with non-ADHD controls in males with treated ADHD, and 4 of 5 outcomes were similar for females. For social function, 9 of 11 and 7 of 8 outcomes were similar for males and females with treated ADHD, respectively. While the proportions of similar outcomes tended to be higher for gender-stratified data, results were in keeping with overall data for individuals with treated ADHD versus non-ADHD controls (Figure 3), and no gender effects were observed.
With respect to treatment benefit, the majority of self-esteem (2/3; 67%) and social function (4/6; 67%) outcomes were reported to exhibit treatment benefit for males. This was lower than the percentage of treatment benefit reported overall (8/9, 89% for self-esteem; and 17/22, 77% for social function outcomes; Figure 5). There were no reported self-esteem or social function outcomes of treated versus untreated ADHD specific to females.
Discussion
Our results show that the number of publications on self-esteem and/or social function long-term outcomes in individuals with ADHD has increased over the past three decades. This increase in publications suggests that self-esteem and social function are being recognized as important outcomes for the individual with ADHD. Studies reporting self-esteem and social function outcomes predominantly originated from Northern America followed by Europe, with relatively few studies originating from Eastern Asia or “Other” regions. A higher number of studies reported social function outcomes compared with self-esteem outcomes. Of these, interest in social function predominated in most regions, except Eastern Asia, where there was relatively more interest in self-esteem.
Self-esteem and social function outcomes were often reported to be poorer for individuals with untreated ADHD compared with non-ADHD controls, reflecting the burden of illness associated with ADHD, and the untreated disorder in particular (Brod, Pohlman, Lasser, & Hodgkins, 2012; Goksoyr & Nottestad, 2008); however, nearly a third of outcomes were reported to be similar between the two groups. Examination of the many different domains and instruments/reporters underlying the social function category revealed that poorer outcomes in individuals with untreated ADHD were primarily driven by poor relationships, poor social skills, and less engagement socially or with hobbies during leisure time; in contrast, living arrangements (living alone, with parents, or with a spouse) were not a primary issue.
While the majority (87%) of outcomes in children with untreated ADHD were poorer compared with non-ADHD controls (including all social function outcomes), the overall proportion of poorer outcomes in individuals with untreated ADHD versus non-ADHD controls was lower in older age groups (lowest for young adults aged 18-24 years), despite these being untreated populations. While this may indicate that problems with self-esteem and social function may ameliorate somewhat with maturity during the natural course of ADHD, the greater proportion of poorer versus similar outcomes suggests that they do not always improve over time, in agreement with findings that adults with ADHD continue to experience considerable impairments in daily life (Biederman et al., 2012; Brod et al., 2012; Hinshaw et al., 2012).
Treatment of ADHD was often reported to result in significant improvement in self-esteem and social function outcomes over pretreatment baseline assessments or compared with individuals with untreated ADHD. While it has been reported that there is a lack of effective treatment for poor social function in ADHD (Sibley, Evans, & Serpell, 2010), we found that many types of treatment were often reported to be associated with significantly improved long-term social function outcomes, often with large effect sizes. Response to treatment across treatment types (pharmacological, nonpharmacological, and MMT) was similar for self-esteem and social function outcomes, and similar between the different treatment types; however, more long-term studies are required. When compared with non-ADHD controls, a higher proportion of similar outcomes was reported for treated individuals with ADHD than for those who were untreated, demonstrating that in individuals with ADHD, outcomes are more likely to be similar to the general population following treatment for the disorder. The majority of studies for which treatment benefit could be assessed were in children, and most of these studies reported an improvement in self-esteem and social function outcomes with treatment. There were fewer studies overall in adolescents and adults reporting either self-esteem or social function outcomes, but all studies of adolescents reported a treatment benefit.
When stratified by reporter, social function outcomes reported by peers, teachers, and parents were more likely to be poorer than similar compared with non-ADHD controls for the untreated and treated ADHD groups; however, results suggest that parents, teachers, and the patients themselves were able to see improvement in social function outcomes with treatment. It should be noted that teacher- and parent-reported outcomes were observer ratings and not proxy self-reports for young children; children included in these studies tended to be at an age when they could read and write, and answer questions about self-perception. The small number of outcomes in some categories, however, must be taken into consideration when drawing conclusions from these results. Furthermore, no marked effects of gender were observed. While gender differences in brain activity have been reported for self-esteem using functional magnetic resonance imaging, outcome assessment scales may not be sensitive to such differences (Miyamoto & Kikuchi, 2012).
This review of long-term studies suggests that levels of self-esteem and social function may be higher in individuals receiving treatment for ADHD compared with those with untreated ADHD. As two of the core impairments specified in the DSM-IV-TR and International Classification of Diseases, Tenth Revision (ICD-10; APA, 2000; WHO, 1992), improvement of self-esteem and social function is an objective of treatment in ADHD. Clinicians may want to consider measuring these parameters as they monitor treatment response, and discuss appropriate goals with patients with ADHD and their families. Further research into the effects of adherence and treatment type (including combination therapy) may be valuable in guiding clinical practice.
Limitations
There are several possible limitations and risks of bias regarding the studies included in this analysis. Only articles published in English were included, which may have resulted in a publication and cultural bias. A search engine and literature database bias may have been introduced by including only articles listed in electronic databases; this was minimized by searching 12 different databases. Some studies may have been inadvertently excluded by relying on search engines for “peer-reviewed” status, or through strict adherence to the Cochrane systematic review guidelines and including only publications that were identified in the original electronic search. Extensive searching of 12 databases, however, reduced this bias.
Changes in diagnostic criteria over the past three decades or discrepancies between classification systems, in particular, differences between the definition of hyperkinetic disorder (ICD-9 or ICD-10; WHO, 1992) and ADHD (DSM-III/DSM-III-R/DSM-IV/DSM-IV-TR; APA, 1980, 1987, 1994, 2000) may have resulted in further bias; however, studies using all these classification systems were included in this analysis. While only studies in which ADHD was the primary disorder under investigation were included, study participants may have had comorbidities, whether identified in the study or not, which may have affected the outcomes. Whenever possible, the present analysis used reported results that were controlled or adjusted for comorbidities.
Available assessments of self-esteem and social function have innate limitations, and study heterogeneity, in terms of instruments used and measures recorded, makes the creation of summary data challenging. We acknowledge that dichotomizing all results into a binary variable of either “poorer” or “similar” outcomes and, with respect to treatment outcomes, either “benefit” or “no benefit,” is a simplification of the data; however, given the vast differences in study design and measurements used, drawing on a binary measure common to all of the included studies (“significantly different” and “not significantly different”) enabled us to summarize results from all the included studies in a nonstatistical manner. In accordance with the classification protocol, two publications that reported “better” outcomes were included in the “similar” group.
Despite these limitations, we highlight the need for more long-term studies examining self-esteem and social function outcomes in individuals with ADHD, and emphasize the importance of including optimal measures of self-esteem and social function in such studies.
Conclusion
There was a higher proportion of poorer outcomes in individuals with untreated ADHD compared with non-ADHD controls. Individuals receiving treatment for ADHD had better outcomes compared with pretreatment baseline assessments or individuals with untreated ADHD. Response to treatment across treatment types (pharmacological, nonpharmacological, and MMT) was similar for all treatment types for self-esteem and social function outcomes; however, the number of studies was small, highlighting the need for further long-term studies on the effects of treatment for ADHD.
Footnotes
Acknowledgements
Shire AG, Switzerland, provided funding to Caudex Medical, Oxford, UK, for support in writing and editing this manuscript. Under the direction of the authors, Clare Hall and Alyson Bexfield, employees of Caudex Medical, provided writing assistance for this publication. Editorial assistance in formatting, proofreading, copy-editing, and fact-checking was also provided by Caudex Medical. Anne Thompson from Shire Pharmaceuticals, UK, provided extensive assistance with reference retrieval. Amina Elsner, MD, from Shire AG, Switzerland, reviewed and edited the manuscript for scientific accuracy.
Authors’ Note
V.H., L.M., J.P.R., and P.H. contributed to the development of study design, critical editing of the text and figures, and approved the final version of the manuscript; J.K. participated in the design of the study, the literature search and included study identification, data analysis, creation of the figures, editing of the text, and approved the final version of the manuscript. Although Shire was involved in the topic concept and fact checking of information, the content of this manuscript, the ultimate interpretation, and the decision to submit it for publication in the Journal of Attention Disorders was made by the authors independently.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: V.H. has an unrestricted research grant awarded by Shire and was sponsored to attend the American Academy of Child and Adolescent Psychiatry (AACAP) congress in Toronto in 2011; L.M. was invited by Shire Italy to attend the AACAP congress in Toronto in 2011; J.P.R. was invited by Shire France to attend the AACAP congress in Toronto in 2011 and San Francisco in 2012; J.K. is the owner of BPS International. BPS International received funding from Shire Development, LLC to perform this analysis and participate in the writing of this manuscript; P.H. is an employee of, and owns stock/stock options in, Shire Development, LLC. Shire develops and markets treatments for psychiatric disorders including ADHD.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Shire Development, LLC.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.