
Abstract
ADHD comprises nearly 20% of postsecondary disabilities (Raue & Lewis, 2011) and increasing numbers of students with ADHD are seeking disability services (Weyandt & DuPaul, 2008). Students with ADHD access disability services via the Americans with Disabilities Act, as Amended (ADA, 2008) and Section 504 of the Rehabilitation Act (Section 504, 1973). Under these laws, students must self-disclose a disability to receive services (U.S. Department of Education Office for Civil Rights [OCR], 2011). Methods for verifying student reports of disability have largely included documentation from qualified evaluators (Madaus, Banerjee, & Hamblet, 2010). With neither the content nor the scope of the documentation specified by law, postsecondary institutions establish their own standards to inform disability service decisions (OCR, 2011). Variability in guidelines across institutions has been demonstrated in investigations of learning disability (LD) documentation (e.g., Madaus et al., 2010); however, no studies of ADHD documentation guidelines were identified in the literature search. The purpose of this study was to examine postsecondary documentation guidelines to evaluate how institutions are attempting to meet the challenges of verifying ADHD as a disability.
ADA and Postsecondary ADHD Documentation
To qualify for ADA protections at the postsecondary level, ADHD must represent a mental impairment that substantially limits one or more major life activities. Qualifying students are entitled to reasonable accommodations in policies and procedures to ensure equal access to information and opportunity to demonstrate knowledge. The majority of postsecondary institutions implement documentation requirements that set the parameters by which disabilities are verified (Raue & Lewis, 2011). Guidelines commonly delineate recency requirements, specify evaluator types, and require information regarding diagnostic methods, documentation of assessments, a statement of disability and its functional impact, and accommodation recommendations (Lindstrom & Lindstrom, 2011).
The Challenges of Documenting ADHD as a Disability
Documentation standards warrant scrutiny due to the significant consequences of classification errors in eligibility decisions. False-negative errors discriminate against students with disabilities (SWDs), denying otherwise qualified individuals the benefits of fully participating in postsecondary programs. False-positive errors result in students receiving unwarranted services. A number of studies show that typically achieving students benefit more from accommodations than peers with disabilities (Gregg & Nelson, 2012; Lewandowski, Lovett, Parolin, Gordon, & Codding, 2007; Lewandowski, Lovett, & Rogers, 2008). Thus, unwarranted accommodations provide typically achieving students with an unfair advantage over all students, compromising program integrity (Gordon, Lewandowski, & Keiser, 1999). Furthermore, provision of unwarranted accommodations trivializes the experiences of those with authentic disabilities and diminishes essential resources.
Several clinical and legal issues make it challenging to accurately verify ADHD at the postsecondary level. Postsecondary ADHD is difficult to diagnose because it is a subjective disorder with no pathognomonic signs. Clinicians must rely on self- and collateral reports, methods with significant limitations. For instance, self-report of current and retrospective ADHD symptoms is common in nondisabled adults and college students (Lewandowski, Lovett, Codding, & Gordon, 2008; Suhr, Zimak, Buelow, & Fox, 2009). As an example, Lewandowski et al. (2008) found that over 50% of college students without ADHD endorsed being easily distracted. Collateral reports rely on individuals who may struggle to be objective (Kovner et al., 1998). Verification of childhood symptoms is difficult because historical data are often nonexistent or inaccessible (Kovner et al., 1998). Complicating diagnosis is a lack of measures with adequate psychometric properties for assessing ADHD. The specificity of neuropsychological measures and rating scales to adult ADHD has been found to be poor (Barkley, Murphy, & Fischer, 2008; Van Voorhees, Hardy, & Kollins, 2011), as has sensitivity to postsecondary ADHD (e.g., Semrud-Clikeman & Harder, 2011).
Warranting consideration when verifying ADHD is potential dishonesty, a problem prevalent within the U.S. education system (see Hughes & McCabe, 2006). Studies suggest that students are willing to feign or exaggerate symptoms to access accommodations, as well as other external incentives such government-funded services and ADHD medications for studying, recreational use, and distribution (Harrison, 2006; Sullivan, May, & Galbally, 2007). Further complicating matters, research indicates that ADHD symptoms are easy to simulate (Jachimowicz & Geiselman, 2004; Sollman, Ranseen, & Berry, 2010). Base rates of noncredible performance for postsecondary students evaluated for ADHD range from 18% to 48% (Harrison & Edwards, 2010; Suhr, Hammers, Dobbins-Buckland, Zimak, & Hughes, 2008; Sullivan et al., 2007). A number of studies have called for symptom validity assessment when evaluating for ADHD (e.g., Frazier, Frazier, Busch, Kerwood, & Demaree, 2008; Harrison, 2006).
Beyond diagnosis, postsecondary institutions must be concerned with verifying ADHD as a legal disability under the ADA. As noted in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000), diagnosis of a clinical disorder is insufficient for establishing a disability because “diagnosis does not imply a specific level of impairment or disability” (p. xxiii). More information regarding functional limitations in major life activities is required to substantiate a disabling condition relative to most people (APA, 2000). Although no studies for ADHD were identified, investigations of postsecondary LD have indicated that the ADA requirement for an absolute impairment has been frequently neglected (Sparks & Lovett, 2009a, 2009b).
Current Legal Context
Regulations implementing the amended ADA (2008),were recently released (Regulations to Implement the Equal Employment Provisions of the Americans with Disabilities Act, as Amended [Title I], 2011; Americans with Disabilities Act Title II Regulations [Title II], 2010; Americans with Disabilities Act Title III Regulations [Title III], 2010), and, whereas much has remained unchanged, a number of new specifications address documentation-related barriers faced by SWDs transitioning to college. These include making it easier for SWDs to obtain protection (Title I, 2011), broadening activities considered to be major life activities (ADA, 2008), limiting the amount and the type of analysis allowed for a disability determination (Title I, 2011), and encouraging consideration of documentation already in the student’s possession (Title III, 2010). The regulations will require institutions to review and potentially update guidelines to ensure consistency with the law.
Extant Literature
No studies examining ADHD guidelines have been conducted; however, several studies have investigated LD documentation (Gormley, Hughes, Block, & Lendman, 2005; Hatzes, Reiff, & Bramel, 2002; Madaus et al., 2010). Most frequently required were a diagnostic statement (approximately 90%; Madaus et al., 2010) and evidence of a functional impact on a major life activity (78%; Gormley et al., 2005). Examiners were often required to be “qualified,” “licensed or certified,” and/or have adult experience (Gormley et al., 2005). Nearly half required documentation from within 3 years (Gormley et al., 2005; Madaus et al., 2010), with large percentages specifying it to be “recent” or “current” (Gormley et al., 2005; Hatzes et al., 2002). Little agreement existed regarding diagnostic criteria needed to verify the presence of LD.
Current Study
The study investigated postsecondary ADHD documentation guidelines. We sought to (a) identify the information requested by postsecondary institutions to verify the diagnosis (i.e., the clinical standard) and substantial limitation in a major life activity (i.e., the legal standard); (b) review acceptable evaluators, documentation types, and recency requirements; and (c) generate recommendations for documentation guidelines.
Method
Sample
We selected our sample (n = 200) such that percentages of institution type according to the Carnegie Classification of Institutions of Higher Education would be equivalent to those of the total population of postsecondary institutions in the United States. To that end, the resulting sample included 72 two-year public (36%), 6 two-year private (3%), 46 four-year public (23%), and 76 four-year private (38%) institutions. The institutions were randomly selected from each institution category. During data collection, five institutions were replaced because they had closed (2), web links were broken (1), or were primarily Spanish-speaking institutions (2). All replacements were randomly selected from the Carnegie Classification list.
Procedure and Instrument Development
A 46-item coding instrument (available from the first author by request) was developed by three doctoral-level educational psychologists specialized in postsecondary learning and attention disorder assessment. ADHD-specific items were generated by reviewing expert recommendations (e.g., Gregg, 2009), testing agency requirements (e.g., Educational Testing Service, 2011), and DSM-IV-TR criteria (APA, 2000). General postsecondary disability items were selected by reviewing Association on Higher Education and Disability best practices recommendations (2004), recommendations for LD guidelines (Lindstrom & Lindstrom, 2011), and surveys of LD guidelines (Gormley et al., 2005; Madaus et al., 2010; McGuire, Madaus, Litt, & Ramirez, 1996).
The coding instrument included 11 items addressing providers, 7 items addressing documentation types, 2 items addressing recency, 7 items addressing testing types, 4 items addressing accommodations, 10 items addressing ADHD diagnostic methods, and 4 items addressing the ADA disability definition. The remaining item addressed the specificity of the guidelines (i.e., for just ADHD, for ADHD and LD, for all disabilities).
Data Collection
Raters coded guidelines by reviewing online information to simulate the experience of students seeking to obtain documentation meeting institution standards. Data were coded by two doctoral-level educational psychologists. Fifty cases were coded independently by both raters to determine interrater reliability. Interrater agreement was 88.35%, indicating an acceptable level of agreement (Stemler, 2004).
Raters reviewed all information presented on disability services websites to ensure identification of all requested information. This was necessary because preliminary trials indicated that ADHD requirements were frequently listed in multiple website locations (e.g., disability services webpage, student handbooks, policies and procedures manuals) and under multiple categories (e.g., general disability requirements, specific ADHD requirements). Documentation requests were not always consistent with one another within institutions. In the case of discrepancies, the more thorough guidelines were coded.
Data Analysis
Frequencies were calculated for components of ADHD documentation across varying levels of preference (e.g., required, accepted/not required, not accepted, no mention/not relevant; see Table 1 for an example). Percentages were used for ease of interpretation and comparison.
Providers: All Guidelines Percentages/ADHD-Specific Guidelines Percentages.
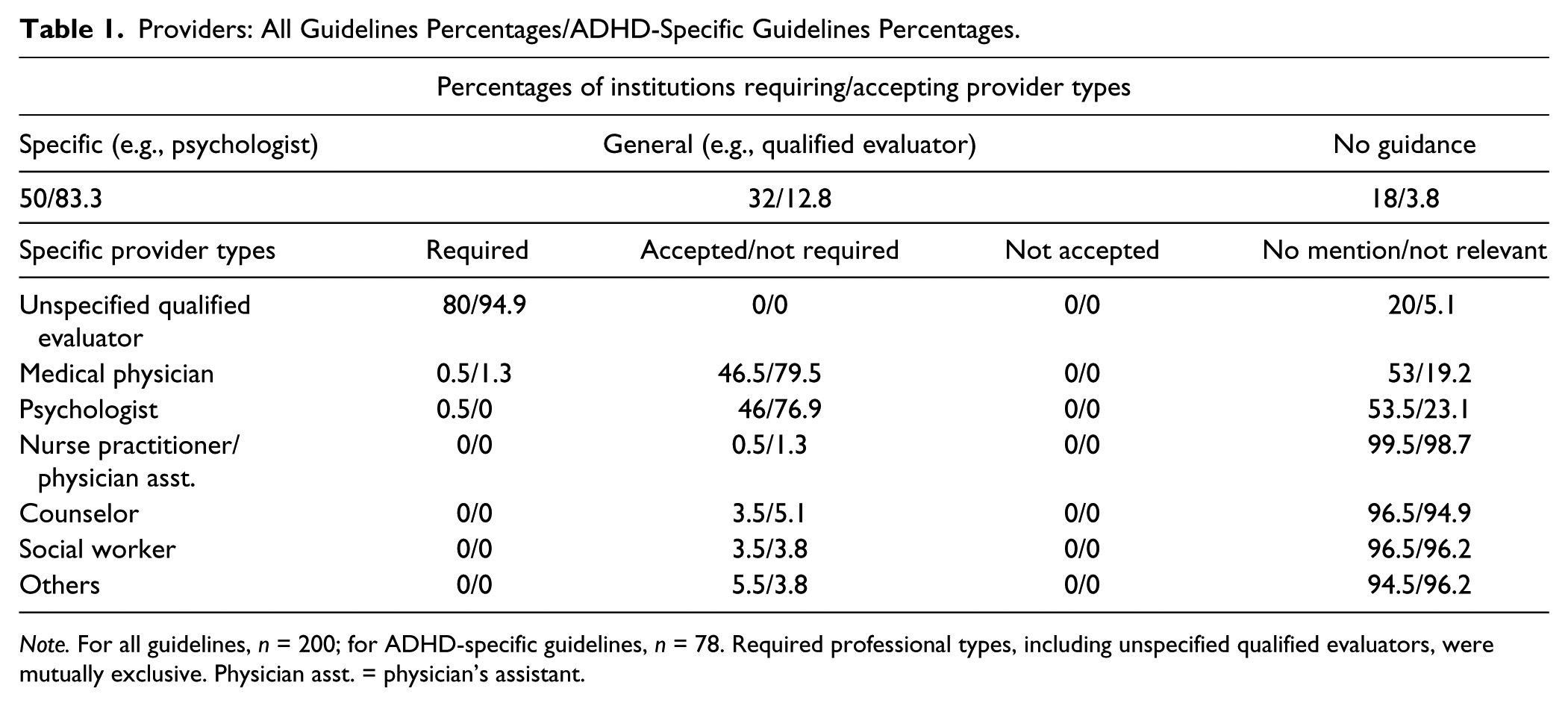
Note. For all guidelines, n = 200; for ADHD-specific guidelines, n = 78. Required professional types, including unspecified qualified evaluators, were mutually exclusive. Physician asst. = physician’s assistant.
Results
Initial analyses revealed that 56.5% of institutions did not have specific ADHD guidelines, addressing requirements in general guidelines for all disabilities or for ADHD and LD together (ADHD + LD; 4.5%). We not only analyzed all 200 cases to provide the most accurate reflection of ADHD documentation requirements but also separately analyzed the cases using ADHD-specific guidelines (n = 78) to determine how requirements might differ compared with all guidelines.
All Guidelines
Table 1 indicates that half of the institutions provided specific guidance regarding required/acceptable professionals (e.g., “clinical psychologist”). For the remainder, general (e.g., “qualified professional”) or no guidance was provided. Most required/acceptable evaluators were medical physicians or psychologists. Table 2 indicates that virtually all institutions required documentation in some form. Psychological/neuropsychological/psychoeducational reports were most often required or accepted. As shown in Table 3, 21% of institutions required some standardized assessment, though nearly half did not mention it. Table 3 also describes accommodation and medication requirements. Whereas the majority of institutions required recommended accommodations, only 39.5% required supportive rationale. Less than half required information regarding current and/or past medication use. Table 4 shows that a statement of diagnosis or disability was required by 75% of institutions. Two institutions specified that an ADHD-Not Otherwise Specified (NOS) diagnosis could qualify a student for services; the remainder made no mention of ADHD-NOS. No institutions mentioned whether ADHD-In Partial Remission would qualify.
Documentation Types: All Guidelines Percentages/ADHD-Specific Guidelines Percentages.
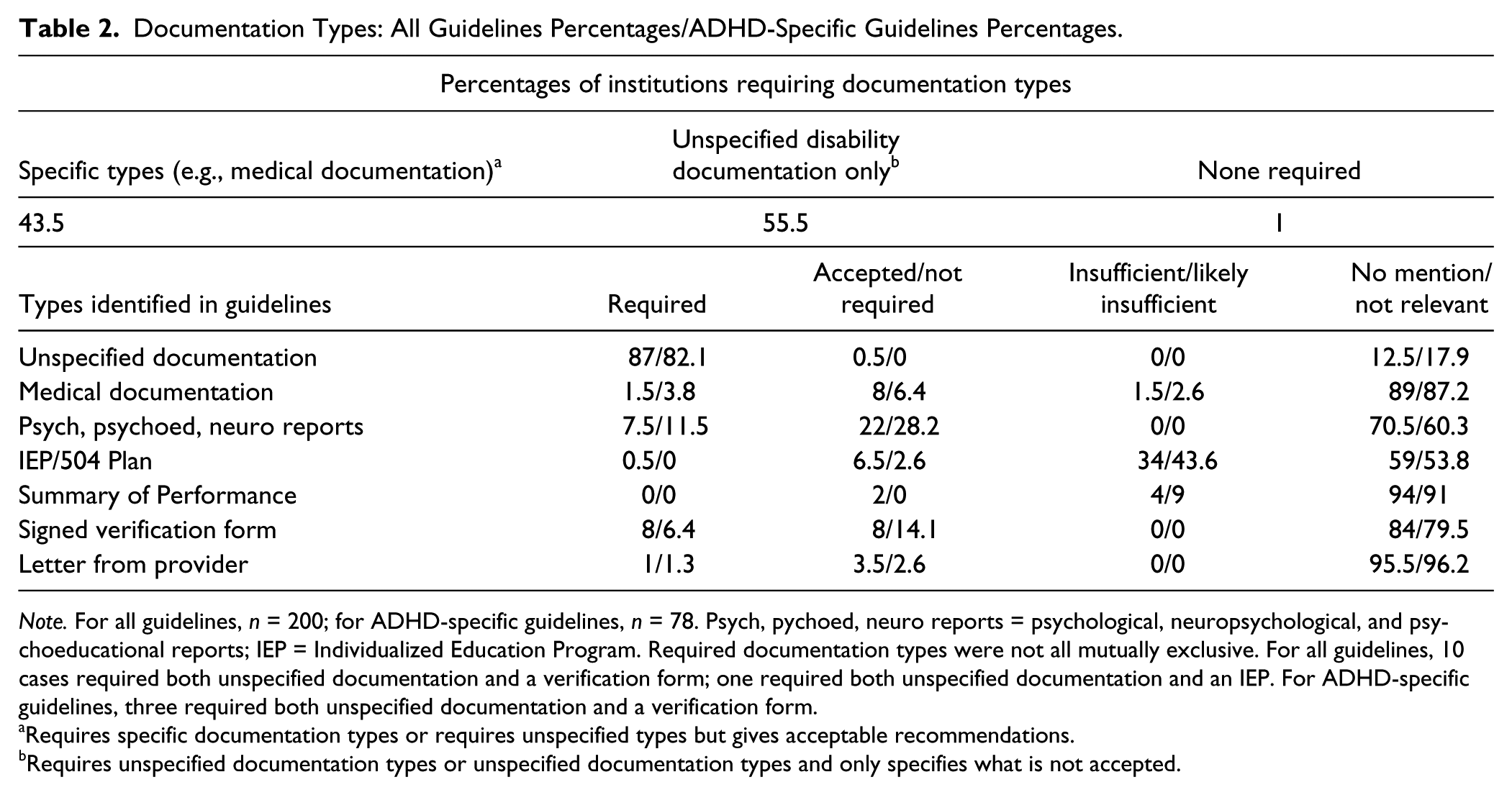
Note. For all guidelines, n = 200; for ADHD-specific guidelines, n = 78. Psych, pychoed, neuro reports = psychological, neuropsychological, and psychoeducational reports; IEP = Individualized Education Program. Required documentation types were not all mutually exclusive. For all guidelines, 10 cases required both unspecified documentation and a verification form; one required both unspecified documentation and an IEP. For ADHD-specific guidelines, three required both unspecified documentation and a verification form.
Requires specific documentation types or requires unspecified types but gives acceptable recommendations.
Requires unspecified documentation types or unspecified documentation types and only specifies what is not accepted.
Standardized Assessment Types, Accommodations, and Medication: All Guidelines Percentages/ADHD-Specific Guidelines Percentages.
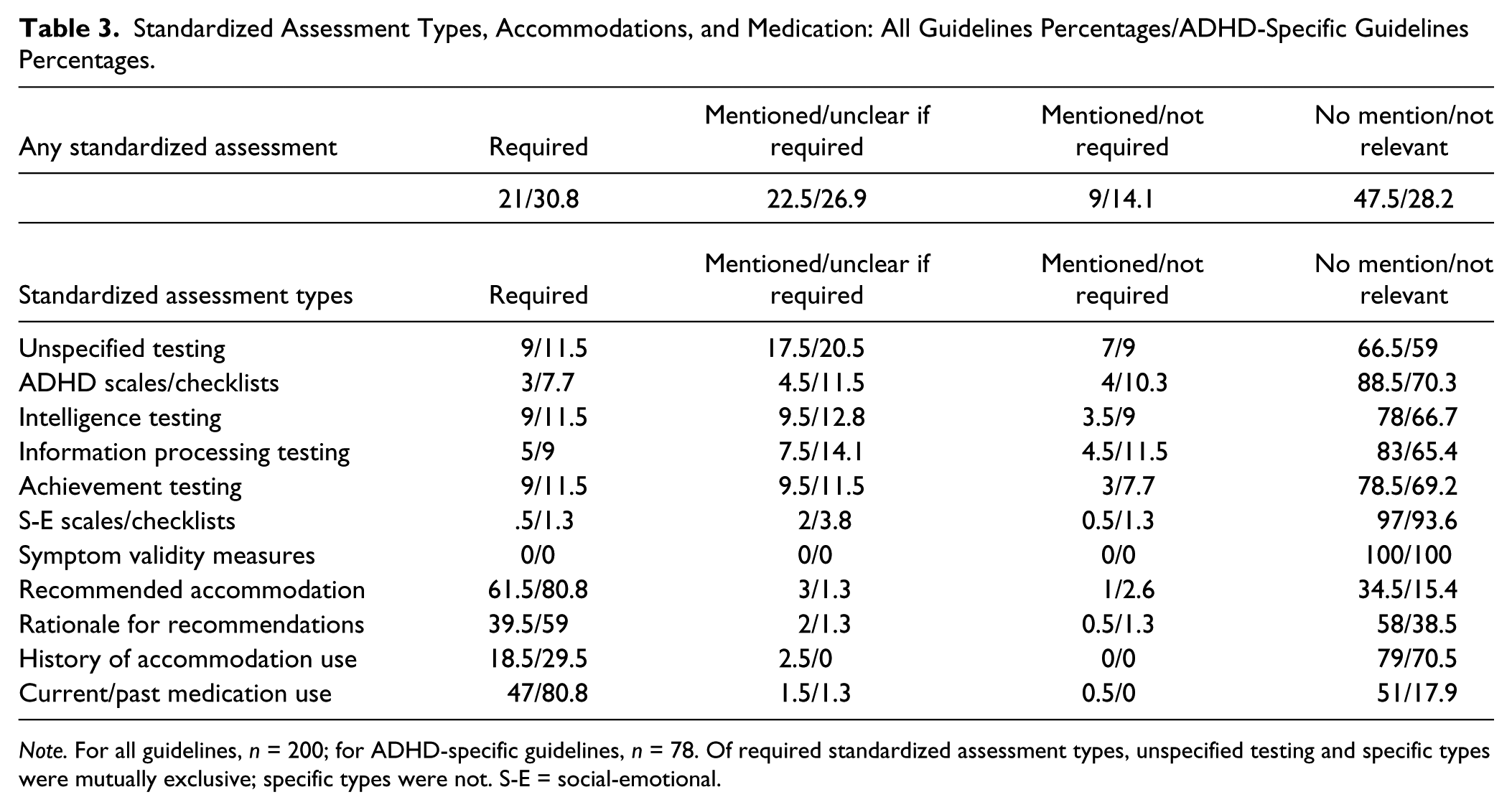
Note. For all guidelines, n = 200; for ADHD-specific guidelines, n = 78. Of required standardized assessment types, unspecified testing and specific types were mutually exclusive; specific types were not. S-E = social-emotional.
Diagnostic Criteria and the Substantial Limitation: All Guidelines Percentages/ADHD-Specific Guidelines Percentages.
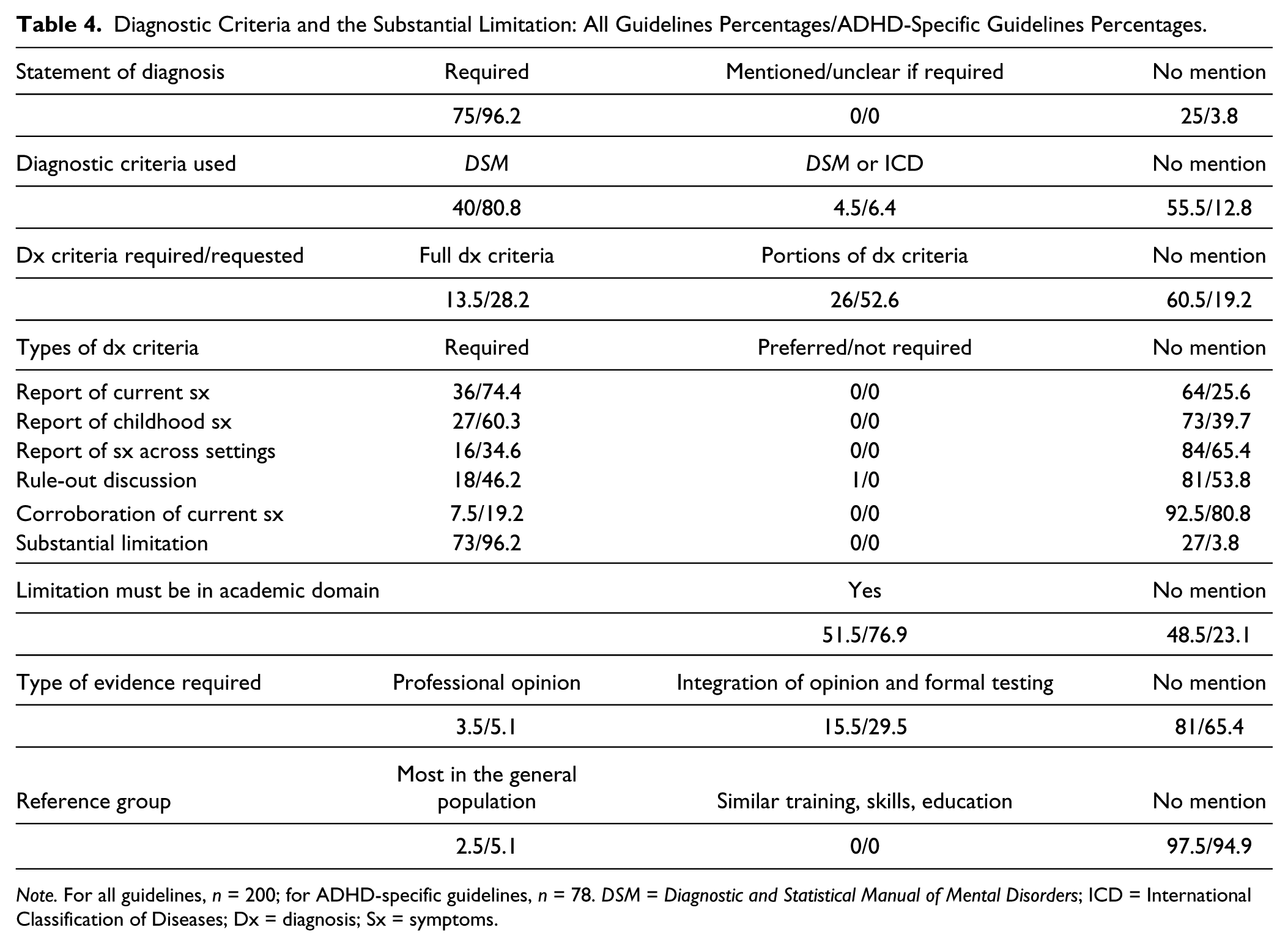
Note. For all guidelines, n = 200; for ADHD-specific guidelines, n = 78. DSM = Diagnostic and Statistical Manual of Mental Disorders; ICD = International Classification of Diseases; Dx = diagnosis; Sx = symptoms.
Reports of current symptoms, childhood symptoms, and symptoms across settings, as well as a rule-out discussion, were used to represent ADHD diagnostic criteria (see Table 4). Nearly two thirds of institutions did not mention diagnostic criteria; only 13.5% required documentation of full criteria. Small percentages requested documentation of specific criteria, the largest being current symptoms (36%). Requests for corroboration of symptoms were rare (7.5%).
Data related to the substantial limitation can be found in Table 4. Nearly 75% required that a clinically significant impairment, functional impairment, or substantial limitation in a major life activity be specified in the documentation. However, the majority provided no guidance regarding the required evidence type (81%) or the appropriate reference group (97.5%).
The most common requirements regarding how recent documentation needed to be included the following: within 3 years (39%), recent/current (24%), and no mention (24.5%). Less frequent recency requirements included the following: within 1 year (1.5%), within 2 years (2%), within 4 years (1%), within 5 years (6%), and others (2%). Of all guidelines, 24.5% included recency exceptions; 74% did not mention exceptions.
ADHD-Specific Guidelines
In the second group of analyses, institutions using general and ADHD + LD guidelines were removed, allowing evaluation of ADHD-specific guidelines (n = 78). These data are listed in the second column for each variable for each of the above-mentioned tables. Most large changes (i.e., an increase of >25% of institutions) were in predictable areas. ADHD-specific guidelines were more likely to require the use of DSM diagnostic criteria, a report of all or portions of diagnostic criteria met, and past/present medication use. They were more likely to give specific guidance regarding provider types. Less predictably, they were more likely to require that substantial limitations occur in the academic environment.
The most common recency requirements included the following: within 3 years (46.2%), recent/current (28.2%), and no mention (6.4%). Less frequent recency requirements included the following: within 1 year (3.8%), within 2 years (1.3%), within 4 years (1.3%), within 5 years (7.7%), and others (5.1%). Of ADHD-specific guidelines, 34.6% included recency exceptions; 62.8% did not mention exceptions.
Discussion
The study investigated the documentation guidelines used by postsecondary institutions to verify ADHD as a disability. Documentation was required by virtually all (99%) institutions. Consistent with previous investigations of LD guidelines (e.g., Madaus et al., 2010), required variables most often included a qualified evaluator (80%), diagnostic statement (75%), and identification of substantial limitations (73%).
Some expectations were confirmed, though with lower proportions of institutions than expected. Psychological/psychoeducational/neuropsychological evaluations were the most frequently requested documentation type, yet were mentioned by less than one third of institutions. As in LD documentation studies (Gormley et al., 2005; Hatzes et al., 2002; Madaus et al., 2010), “within the past 3 years” (39%) and “recently” (24%) were the most frequently used recency criteria, though nearly a quarter of institutions did not mention recency requirements at all (24.5%). Physicians and psychologists were the most frequently required/requested professional evaluators, but each was named in fewer than 50% of institutions. Few institutions requested/required full diagnostic criteria (13.5%), standardized assessment (43.5%), or verification of the substantial limitation (19%). The reference group for determining the substantial limitation was rarely mentioned (2.5%). No institutions mentioned use of symptom validity assessment.
The survey revealed extreme variability in documentation requirements across institutions. Only five variables were found to be required by at least 50% of guidelines reviewed. These included the use of a qualified evaluator, statements of (a) diagnosis, (b) substantial limitation, and (c) academic limitation, and accommodation recommendations. Supportive data such as diagnostic criteria, standardized assessment results, and rationale for accommodations were rarely required. In the following sections, we discuss the degree to which current ADHD documentation practices are consistent with research related to postsecondary disability determinations.
Documentation Practices and Empirical Literature
Whereas there was great variation among the guidelines reviewed, the majority required little to verify ADHD as a disability. In many ways, use of nominal documentation requirements could be construed as consistent with new regulation specifications mandating that documentation requirements be “reasonable and limited” (Title III, 2010, p. 49). However, recent literature has suggested that many documentation practices promoted by the new regulations are not supported by empirical research (Lovett, 2014). For example, the trust placed in the disability-related decision making of Individualized Education Program (IEP) teams and clinical professionals by the regulations was found to be unsupported. Regarding the current study, the question remained whether nominal components would be sufficient for determining disability service eligibility and informing accommodation recommendations. Within the context of the ADHD literature, regulation guidance appeared to overly trust evaluators, disregard the limitations of self-report, and disempower disability service providers (DSPs).
Overly trusting evaluators
To ensure valid disability determinations despite minimal documentation, the majority of institutions required the use of a qualified evaluator. The reasonable assumption is that qualified evaluator statements of diagnosis and disability would be supported by empirically sound practices. However, findings suggest that less than 35% of pediatricians, 15% of family practitioners, and 16% of psychologists adhere to best practice approaches when diagnosing ADHD (Handler & DuPaul, 2005; Rushton, Fant, & Clark, 2004). Reviews of documentation generated by qualified evaluators have revealed large percentages that failed to meet basic diagnostic standards (Harrison, Nichols, & Larochette, 2008; Joy, Julius, Akter, & Baron, 2010). In addition, concern exists that clinicians focus on the nonspecific diagnostic symptoms of ADHD, neglecting the clinically significant impairment criterion required for diagnosis (Lewandowski, Lovett, & Gordon, 2009). Finally, evaluators have been found to be poorly informed regarding the ADA. For instance, over one third of qualified evaluators did not know that the reference group when determining a substantial limitation is “most people in the general population,” a critical lapse when making postsecondary disability determinations (Gordon, Lewandowski, Murphy, & Dempsey, 2002). As this reference group was specified in only 2.5% of guidelines reviewed, the likelihood of high levels of false-positive disability classifications appeared to be great. Experts have lamented the poor documentation provided by evaluators (Murphy, 2012; Wolforth, 2012), with one commenting that many qualified evaluators generate documentation ranging from “incomplete to woefully inadequate” (Murphy, 2012).
Excessive reliance on self-report
According to our findings, most institutions did not require supportive or collaborative information such as standardized assessment results, collateral reports of symptoms, reports of difficulties across settings, or evidence of substantial limitation beyond professional opinion. In the absence of such sources, self-report remained as the foundation for decision making.
Whereas self-report plays an important role in ADHD assessment, it is insufficient and problematic when used in isolation for diagnosis and disability determination. Self-report of ADHD symptoms is common in non-ADHD postsecondary students (DuPaul et al., 2001; Lewandowski et al., 2008), and self-report of childhood ADHD symptoms is common in non-ADHD adults (Murphy, Gordon, & Barkley, 2000). Furthermore, self-reported academic struggles (e.g., needing to reread information to understand it, difficulty finishing timed tests) are common experiences for college students and not specific to disability (Lewandowski et al., 2008). Finally, documented rates of ADHD symptom exaggeration demand increased attention (Harrison & Edwards, 2010; Sullivan et al., 2007). Standardized self-report instruments of ADHD symptoms are particularly susceptible to symptom exaggeration and intentional distortion, with up to 93% of college students being able to successfully endorse the necessary number and pattern of symptoms on such instruments to meet ADHD criteria (Fisher & Watkins, 2008). In the current study, no guidelines mentioned symptom validity assessment. As trained clinicians are not capable of identifying invalid data due to poor effort or symptom exaggeration (Heaton, Smith, Lehman, & Vogt, 1978), calls for inclusion of symptom validity assessment during postsecondary ADHD evaluations should be heeded (Frazier et al., 2008; Harrison, 2006).
Disempowering DSPs
DSPs rely on documentation content when making informed decisions regarding disability authenticity and the appropriateness of accommodations (Gormley et al., 2005). This is especially the case for ADHD when the limitations of self-report must be considered. Although accommodation recommendations are valuable, it is rare that evaluators can anticipate all situations for which a student might need accommodations. DSPs benefit from thorough documentation that can inform decisions in unexpected situations. Nominal documentation forces DSPs to rely on evaluator recommendations which may have little support and leaves DSPs to navigate unanticipated situations with minimal data to guide decision making.
Implications
Given substandard diagnostic practices, the limitations of self-report, high rates of simulation/symptom exaggeration, and poor evaluator awareness of relevant law, sound ADHD approaches require rigorous, detailed guidelines. The best practice approach to ADHD diagnosis employs multiple methods across multiple settings and sources to evaluate DSM symptom existence, chronicity, and pervasiveness (Handler & DuPaul, 2005). Recommended components include interviews with the student, parent, and/or significant other; standardized rating scales completed by the student and a collateral informant; record review; and observations (Handler & DuPaul, 2005). Norm-referenced cognitive, achievement, and social-emotional measures help to rule out other disorders (Gregg, 2009). Symptom validity should be assessed using measures with adequate psychometric properties for suspected postsecondary ADHD (Harrison, 2006).
Because not all cases of ADHD result in impairment relative to most people, the substantial limitation must be assessed and documented. A simple statement that the individual is substantially limited should not suffice. In the current study, we found that approximately 80% of institutions did not mention the type of evidence required to support the possibility of substantial limitation. Recommended methods include self-reported history, corroborative reports, and record review (Barkley et al., 2008; Gregg, 2009). Given the limitations of self-report (Lewandowski et al., 2008), objective and/or verifiable evidence is preferable. Norm-referenced tests with nationally representative samples provide direct comparisons to “most people in the general population” at the student’s age (Lewandowski et al., 2009). Given the evidence of sensitivity to ADHD, achievement tests can be useful (Frazier, Youngstrom, Glutting, & Watkins, 2007). Because ADHD manifests in cross-temporal difficulties, ratings reflecting functioning over longer periods have been recommended (Barkley, 2011). Grade point averages and transcripts, though lacking the precision of norm-referenced measures, provide verifiable indices of functioning (Lewandowski et al., 2009).
Opportunities for Burden Reduction While Maintaining Valid Decision Making
Whereas the comprehensive approach is recommended for valid disability determinations and accommodation decisions (Gregg, 2009), reducing burdens on SWDs is a worthy objective. Because most individuals with ADHD are diagnosed prior to matriculation, opportunities to reduce burden include adjustments to recency requirements, consideration of documentation updates, and willingness to integrate data from multiple sources.
Recency
ADHD symptoms and impairment often attenuate during early adulthood (APA, 2000; Barkley et al., 2008), a pattern acknowledged by the DSM-IV-TR inclusion of an ADHD “in partial remission” specifier. Of extant longitudinal studies, the largest estimations of persistence through adulthood were less than 70% (see Barkley et al., 2008). For those who continue to experience an impairing disorder, manifestations usually change over time. Early adulthood trends include decreasing hyperactivity, increasing executive dysfunction, and persistent inattention (Barkley, 2010). Documentation should be as recent as possible to best inform DSPs how to serve the student’s current needs and environmental challenges (Madaus et al., 2010).
Institutions, however, should maintain a reasonable stance on documentation recency based on “recognized and accepted practices in the relevant field” (Heyward, 2011). Given the developmental nature of ADHD, most frequently used guidelines (i.e., within 3 years, recent/current, and within 5 years) do not appear unreasonable. Rigid cutoffs with no exceptions could be seen as burdensome to those that narrowly miss a recency criterion. In the study, 74% of reviewed guidelines made no comment regarding recency exceptions.
Documentation updates
Updates provide an option to reduce burdens for individuals with sufficient documentation that is not considered reflective of current functioning (e.g., see Educational Testing Service, 2011). Given an established history, a brief, focused evaluation by a qualified evaluator using select measures could be used to verify that historical difficulties remain substantially limiting relative to most people, and appropriate accommodations could be determined based on current limitations, environments, and task demands.
Integration
According to regulations, institutions should consider “a variety of types of information submitted by students” (Title III, 2010, p. 152). Professionals may be able to integrate disparate information to meet verification standards. Sources could include recommendations of qualified professionals, evaluation results, diagnostic history, IEP, 504, and Summary of Performance records, educator observations, and past accommodations (Title III, 2010). The integrated approach is challenging. When relying on historical records, professionals should be aware that the validity of some special education and 504 classifications may be poor (Gresham, MacMillan, & Bocian, 1998). Furthermore, clinical diagnoses and Individuals With Disabilities Education Act (IDEA) classifications (i.e., Other Health Impaired) are not always equivalent to ADA disabilities, neither defining a metric or reference group for determining limitation magnitude. The regulations acknowledge the difficulty of this flexible approach, encouraging a high level of training. According to Title III Guidance and Section-by-Section Analysis (2010), documentation reviews should be “conducted by qualified professionals with similarly relevant expertise” as those who generated the documentation (p. 153), suggesting DSPs should have training equivalent to the qualified professionals making the diagnoses and disability determinations.
Limitations
The most notable limitation to the current study was the dependence on website information. The extent to which all necessary information was posted on websites for all 200 institutions is unknown. Whereas we limited ourselves to collecting data from websites, students and evaluators may also contact disability service offices for clarification. Documentation demands may decrease or increase following interaction with disability service personnel. Second, we encountered some variables during data collection that we were not prepared to code. Some guidelines accepted a “team diagnostic approach” as an acceptable evaluator. To enforce a recency requirement, some institutions required only the use of adult measures. A final limitation related to the challenging nature of the data collection. Despite adjusting the collection instrument and implementing coding rules, the ambiguity and nuanced language of some guidelines occasionally required raters to use judgment when coding.
Recommendations
When developing ADHD guidelines, institutions must be informed regarding what is necessary to verify ADHD as a disability, as well as the limitations of self-report, historical documentation, and common ADHD practices. Institutions will want to weigh the benefits and risks associated with guidelines that are more rigorous (e.g., increased classification accuracy and data for DSPs but increased student burden) and less rigorous (e.g., decreased student burden but decreased classification accuracy and data for DSPs) as they seek an acceptable balance. Institutions are encouraged to follow the flexible documentation approach advocated by the amended ADA and its regulations to the extent that can be supported by empirical evidence. Setting reasonable guidelines for recency, instituting options for updates, and allowing students to integrate pieces of documentation are potential options. Considering the challenges of more flexible approaches, institutions will want to ensure adequate DSP training. Finally, institutions should make guidelines clear and post them in a single, obvious location.
Future Directions
With 11 years since Gordon, Lewandowski, Murphy, and Dempsey’s (2002) study regarding evaluator ADA knowledge and amendments and new regulations now available, a replication would be useful. A similar investigation with DSPs could inform training needs. Investigations into DSP training, skill, and knowledge could determine readiness to perform tasks requiring greater professional judgment. Norm-referenced measures of ADHD-related impairment are needed to reduce reliance on self-report, clinical judgment, and history. Symptom validity measures with improved sensitivity to simulated ADHD are also needed (Musso & Gouvier, 2014). Legally, it will be important to determine how emerging case law operationalizes the vague aspects of the regulations, such as “reasonable” and “burdensome” types of documentation (Title III, 2010). Given that testing agencies, admission panels, and licensing boards may have more demanding guidelines than those of postsecondary institutions, investigations into the rigor of ADHD guidelines across such organizations, as well as with guidelines of postsecondary institutions, could be useful to evaluators, students, and those developing policies. Finally, similar investigations of requirements for other disorders are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.