
Abstract
Introduction
Prisoners are typically a disadvantaged group with high rates of unemployment, low levels of education, and frequent unstable accommodation (Australian Institute of Health and Welfare [AIHW], 2011). Australian and international research studies have consistently identified high levels of mental disorder among prisoners (Fazel & Danesh, 2002). Moreover, rates of mental disorder among prisoners have been found to be significantly elevated compared to the general population, even after accounting for demographic differences (Butler et al., 2006). Butler and colleagues (2006) found that 80% of prisoners had at least one psychiatric disorder in the preceding 12 months compared with 31% of the community sample. Substance use disorders (SUD) were particularly elevated, with the prevalence among prisoners exceeding that of the community by 11 times (Butler et al., 2006).
ADHD is a neurodevelopmental disorder and is associated with age-inappropriate problems with inattention and/or hyperactivity/impulsive behavior (Konstenius et al., 2015; Wilens, Faraone, & Biederman, 2004). While ADHD has typically been seen as a childhood disorder, recent longitudinal studies suggest persistence into adulthood (Barkley, Fischer, Smallish, & Fletcher, 2002), and adult ADHD is now recognized in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000). Using epidemiological data from different study designs, a recent meta-analysis found that the pooled prevalence of adult ADHD was 2.5% (Simon, Czobor, Balint, Meszaros, & Bitter, 2009). Research has also found that ADHD commonly co-occurs with other psychiatric disorders (particularly SUD; Biederman et al., 1993), and is associated with socioeconomic and functional impairments (e.g., lower educational attainment, unemployment, divorce, arrest history; Biederman et al., 2006).
Given the elevated rates of psychiatric disorders identified among prisoners, particularly SUD, it is not surprising that research has identified a disproportionately high prevalence of individuals with ADHD within the criminal justice system (Young & Thome, 2011). International studies (from the United States, Canada, Sweden, Germany, Finland, and Norway) suggest that half of the adult prisoners will report symptoms of childhood ADHD, with an elevated rate identified among juvenile offender samples (71%; Young & Thome, 2011). Studies utilizing clinical assessments to identify persistent ADHD symptoms in adult prisoners have identified prevalence rates of 20% to 30% (Konstenius et al., 2015; Westmoreland et al., 2010; Young & Thome, 2011). Rosler, Retz, Yaqoobi, Burg, and Retz-Junginger (2009) identified slightly lower rates of persistent ADHD among female prisoners (10%), but others have found nonsignificant gender differences (Westmoreland et al., 2010).
Recent studies exploring the clinical characteristics associated with the diagnosis of ADHD among prisoners have identified higher rates of psychiatric comorbidity (i.e., substance use, mood, anxiety, psychotic, and personality disorders; Konstenius et al., 2015; Rosler et al., 2009; Westmoreland et al., 2010). For example, Rosler and colleagues (2009) found that females with ADHD had a significantly higher number of Axis I diagnoses compared with females without ADHD (3.6 vs. 2.3). Similarly, Konstenius and colleagues (2015) found that among prisoners with ADHD, 71% had illicit drug dependence, compared with 31% among prisoners without ADHD. Difficulties in emotional and social functioning, as well as suicide risk, also appear to be higher among prisoners with ADHD (Westmoreland et al., 2010). A diagnosis of ADHD among prisoners is complex, given that symptoms like impulsivity are common among illicit drug users and individuals with a personality disorder. In addition, the treatment and management of ADHD in this group will be complicated by other co-occurring psychiatric disorders.
The current study utilizes the ADHD Self-Rating Scale (ASRS) as a screening instrument (Kessler, et al., 2005). The short six-item version of this instrument has been shown to be valid and reliable in predicting the diagnosis of ADHD in the general population (Kessler, et al., 2005), among individuals with SUD (Elkins, McGue, & Iacono, 2007; Gau et al., 2007), and recently, in a Swedish study of female prisoners (Konstenius et al., 2015). Replication of these results is required in other jurisdictions, and in samples with male offenders. To our knowledge, there are no prior Australian studies examining adult ADHD among prisoners or the validity of the ASRS among adult offenders. Given that half of all New South Wales (NSW) prisoners report ever receiving a psychiatric assessment and/or treatment (Indig et al., 2010), it is likely that ADHD is elevated compared with the general population. Moreover, 84% of NSW prisoners have used illicit drugs, and 44% report regular illicit drug use prior to prison (Indig et al., 2010). Further, 60% have been incarcerated as an adult on at least one previous occasion (Indig et al., 2010). Better identification of individuals with untreated ADHD and associated clinical characteristics may assist in preventing recidivism and developing better integrated treatment programs.
Given the paucity of research among prisoners, particularly in Australia, the current study aimed:
to examine the prevalence of adult ADHD among prisoners in NSW;
to examine clinical characteristics associated with ADHD including substance use and lifetime comorbid psychiatric disorders; and
to examine the validity of the ASRS as a screening tool among prisoners in an Australian context.
Method
Study Design
The study was conducted between January 2011 and June 2012 at four NSW correctional facilities (two male and two female centers). Participants initially completed a screening assessment, which included the ASRS. The screening assessment was conducted by trained research officers, and took approximately 30 to 45 min to complete. Participants were classified as either screening positive or negative for ADHD, and 46% (n = 92) were randomized to complete a more comprehensive assessment of ADHD and other psychiatric morbidity (full assessment). The full assessment was conducted by registered clinical psychologists, took 1 to 2 hr to complete, and was conducted over multiple visits for some participants due to correctional center access restrictions. Where possible, the screening and full assessments were conducted on the same day to minimize risk of participant loss due to prison transfer. Participants were reimbursed $10 for each interview.
The study received ethics approval from the Justice Health Human Research and Ethics Committee, the Corrective Services NSW Ethics Committee, and the Aboriginal Health and Medical Research Council Ethics Committee.
Sample
A random sample of inmates from each correctional facility was generated routinely using SPSS statistics package version 19 (IBM, 2010). If the approached participant refused, then the next randomly selected person on the list was invited to participate. A total of 241 inmates were approached to participate in the study, with 200 participants (75% male) completing the screening assessment and 41 refusals, equating to an 83% response rate. In addition, 77 participants were transferred/released prior to being approached by research staff. This group was not included in the response rate as we were unable to determine if they would or would not have participated if directly approached. Eighty-eight participants (76% male) completed the full assessment.
To determine the validity of the ASRS, the study initially intended to randomly allocate 50% of participants who screened positive and 50% of participants who screened negative for ADHD (using the ASRS) to the full assessment. However, toward the end of recruitment, the study design was amended as a lower proportion of ADHD-positive participants were being randomly allocated to the full assessment. For the last 20 female and the last 50 male participants, all those who screened positive on the ASRS proceeded to the full assessment, and the full assessment was not conducted on individuals who screened negative. There were no significant demographic differences (i.e., gender, age, Aboriginality, employment, martial status, education, previous incarceration) for individuals who completed the screening assessment only, compared to those who completed the full assessment.
Measures
Screening assessment
Sociodemographic variables included gender, age, indigenous status, employment prior to prison, homeless or living in unsettled accommodation prior to prison, education, ever placed in care prior to age 16, and parental history of incarceration (during the respondents childhood). To determine psychiatric history, participants were asked whether a health professional ever told them they had a mental health or behavioral problem as a child and/or as an adult (coded separately for anxiety, depression, bipolar disorder, schizophrenia/other psychotic disorder, oppositional defiant disorder, ADHD, conduct disorder). Use of prescribed and diverted ADHD medication was also assessed. Substance use variables included current tobacco smoker, daily risky alcohol use (≥6 drinks per occasion), ever used illicit drugs, and ever injected illicit drugs. Self-reported offending behaviors, that is, ever being in juvenile detention, incarceration in an adult facility, and types of offenses committed, were also collected.
The 18-item adult ASRS was used to assess ADHD symptomatology (Kessler, et al., 2005). The ASRS consists of 9 items assessing symptoms of inattention, and 9 items assessing symptoms of hyperactivity/impulsivity. Each item is rated on a 4-point scale (from never to very often) in terms of how often the symptom occurred during the past 6 months. For screening purposes, the first 6 items can be used to generate a positive screen for adult ADHD, 4 inattention items and 2 hyperactivity/impulsivity items (Kessler, et al., 2005). A participant screens positive for adult ADHD if four or more of their answers occur within predefined ranges (i.e., “sometimes” to “very often” on the first 3 items, and “often” to “very often” on the next 3 items). The performance of the short-form (6-item) ASRS has been found to be superior to 18-item version on sensitivity, specificity, and total classification accuracy (Kessler, et al., 2005).
Full assessment
The full assessment collected a more comprehensive assessment of psychiatric illness. The Personality Disorder Diagnostic Questionnaire for the DSM-IV (PDQ-4; Hyler, 1994) was used to assess avoidant and dependent personality disorders, while borderline personality disorder (BPD) was assessed using the Structured Clinical Interview for DSM-IV (SCID-II; Taylor, James, Bobadilla, & Reeves, 2008). The Mini-International Neuropsychiatric Interview (M.I.N.I. Plus) was used to assess childhood ADHD, adult ADHD, major depressive episode, hypomanic/manic episode, social phobia, generalized anxiety disorder, conduct disorder, antisocial personality disorder (ASPD), alcohol abuse and dependence, and nonalcohol psychoactive substance use disorders (Sheehan et al., 1997). The full assessment also assessed suicidal thoughts, suicide attempts and episodes of self-harm (defined as distinct from suicidal behaviors). Meeting criteria for a diagnosis of posttraumatic stress disorder (PTSD) was also generated using the 17-item self-report PTSD Checklist–Civilian Version (PCL-C; Weathers, Litz, Herman, Huska, & Keane, 1993).
Data Analysis
Data were analyzed using SPSS statistics package version 19 (IBM, 2010). Characteristics of the sample by ADHD diagnosis (yes/no) were compared using chi-square analyses. Correlates of ADHD diagnosis were identified using univariate logistic regression; those significant at p < .05 were entered into a multivariable logistic regression model to identify independent correlates of ADHD while adjusting for significant sociodemographic characteristics (i.e., current age, Aboriginality, history of parental incarceration, age of first contact with the criminal justice system). Unadjusted and adjusted odds ratios (OR, AOR) with 95% confidence intervals (95% CI) are reported. The validity of the ASRS was examined with sensitivity, specificity, area under the ROC curve, Kappa value, and positive and negative predictive values reported. Where appropriate, given the relatively small sample size, 95% confidence intervals for the proportions are reported.
Results
Sample Characteristics
Eighty-eight prisoners completed the full assessment. The majority were male (76%), with a mean age of 41 years (SD = 13 years; range = 18-72), and a third identified as Aboriginal and/or Torres Strait Islander. Half the sample (53%) reported that they completed less than 10 years of schooling, 41% had been placed in care as a child, 21% had a parental history of imprisonment, and 32% had a history of juvenile detention. Under half (47%) were single, 63% were unemployed, and 5% reported living in unsettled accommodation prior to prison. Forty-five percent reported three or more episodes of incarceration in an adult facility, and the mean age of first contact with the criminal justice system was 21 years (SD = 12 years; range = 5-71).
Males were significantly more likely to report ever being in juvenile detention (37.3% vs. 14.3%, p < .05), and to be younger at first admission into the criminal justice system (19.4 years old vs. 26.4 years old, p < .05). Female participants were significantly more likely to report being unemployed prior to prison, compared with males (81.0% vs. 56.7%, p < .05).
Prevalence of ADHD and Associated Symptomatology
Thirty-five percent of the sample (N = 200) screened positive for ADHD using the six-item ASRS (Table 1). In the full assessment, 17% of the sample (N = 88) was diagnosed with adult ADHD according to the M.I.N.I. Plus. There were no gender differences in either screening positive for ADHD or being diagnosed with adult ADHD. Aboriginal prisoners were significantly more likely to be diagnosed with adult ADHD (31% vs. 10%), compared with non-Aboriginal prisoners.
Prevalence of ADHD.

p < .05. **p < .001.
Of those who screened positive for ADHD on the six-item ASRS (n = 70), a quarter reported ever being diagnosed with childhood ADHD (26%), ever receiving a diagnosis of adult ADHD (24%), and/or ever being prescribed medication for ADHD (26%). Moreover, of those who were not diagnosed with adult ADHD on the M.I.N.I. Plus (n = 73), 41% met criteria for childhood ADHD.
Table 2 describes the proportion of individuals who endorsed each of the ASRS items at a severity level indicative of ADHD symptomatology in the total sample (n = 200), and in the full assessment sample (n = 88). Item 1 (i.e., difficulties finalizing a project) and item 3 (i.e., problems remembering appointments) were the most frequently endorsed items on the “inattention” dimension, while Item 5 (i.e., inability to sit still) was most frequently endorsed from the “hyperactivity/impulsivity” dimension. Figure 1 highlights the number of items endorsed for each ASRS dimension in the total sample. The majority of the sample (75%) endorsed at least one item on the “inattention” dimension, and half the sample (54%) endorsed at least one “hyperactivity/impulsivity” item. Nineteen percent of the total sample endorsed both items on the “inattention” dimension, and 22% endorsed both items on the “hyperactivity/impulsivity” dimension.
Prevalence of ASRS Items Endorsed at a Severity Level a Indicative of ADHD Symptomatology.
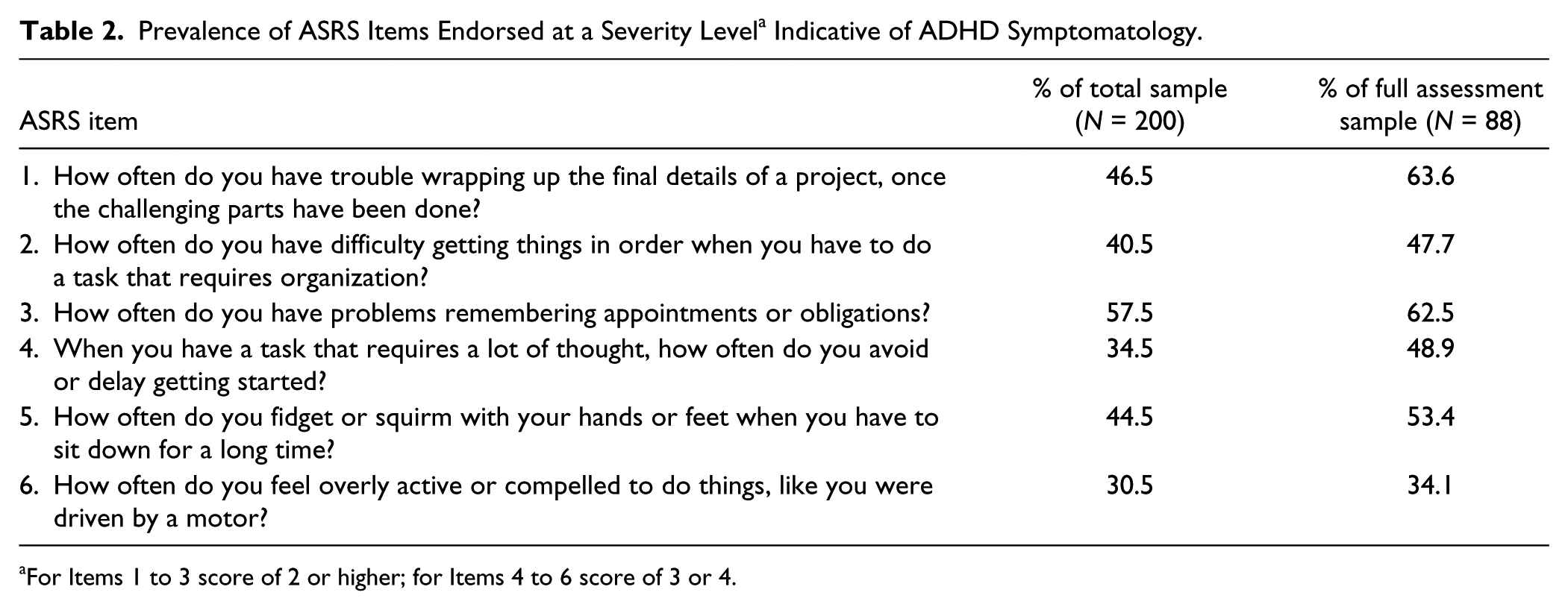
For Items 1 to 3 score of 2 or higher; for Items 4 to 6 score of 3 or 4.
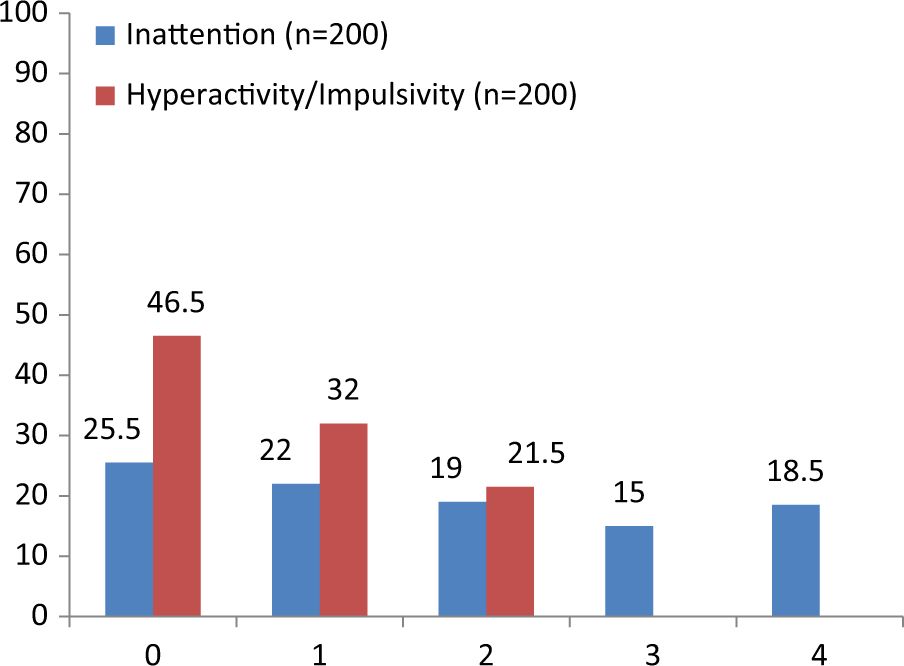
Total number of inattention and hyperactivity/impulsivity items endorsed on ASRS at a severity level indicative of ADHD symptomatology among whole sample (n = 200).
Correlates of ADHD
Prisoners diagnosed with ADHD in the full assessment were significantly (all p < .05) more likely to be younger (M = 34 years, SD = 9 years vs. M = 42 years, SD = 13 years), identify as Aboriginal and/or Torres Strait Islander (60% vs. 27%), report a parental history of incarceration (40% vs. 16%), and report a younger age at first contact with the criminal justice system (M = 15 years, SD = 5 years vs. M = 22 years, SD = 13 years) than prisoners without ADHD.
Table 3 shows the unadjusted and adjusted results for correlates (substance use and psychiatric comorbidity) for ADHD. After adjustment for the significant sociodemographic correlates (i.e., age, Aboriginality, parental history of incarceration, age at first contact with the criminal justice system), benzodiazepine dependence, BPD, social phobia, ASPD, and a number of lifetime psychological disorders remained significantly and independently associated with a diagnosis of ADHD.
Substance Use and Psychological Comorbidity With Adult ADHD (yes/no).
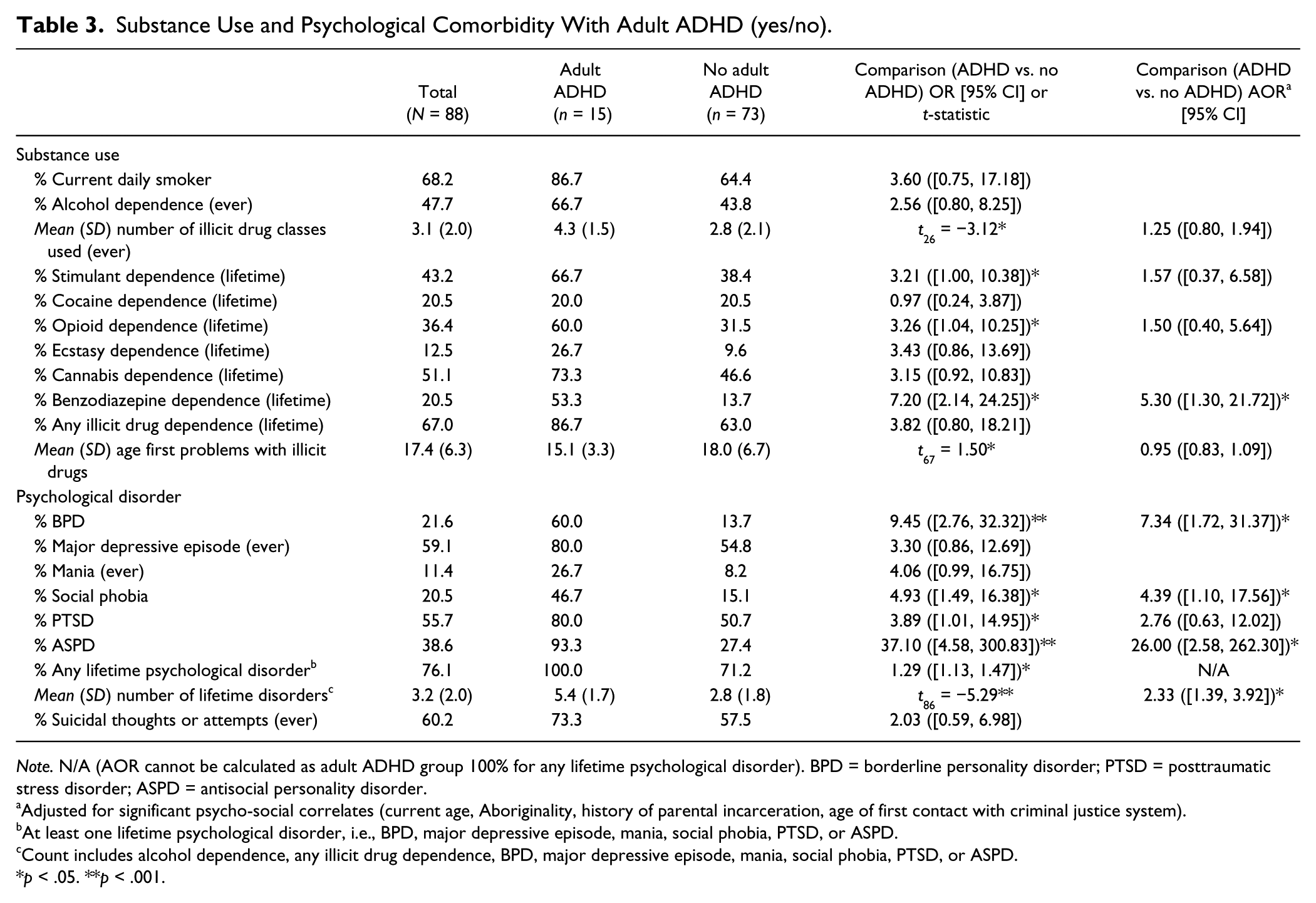
Note. N/A (AOR cannot be calculated as adult ADHD group 100% for any lifetime psychological disorder). BPD = borderline personality disorder; PTSD = posttraumatic stress disorder; ASPD = antisocial personality disorder.
Adjusted for significant psycho-social correlates (current age, Aboriginality, history of parental incarceration, age of first contact with criminal justice system).
At least one lifetime psychological disorder, i.e., BPD, major depressive episode, mania, social phobia, PTSD, or ASPD.
Count includes alcohol dependence, any illicit drug dependence, BPD, major depressive episode, mania, social phobia, PTSD, or ASPD.
p < .05. **p < .001.
Validity of the ASRS
The validity of the ASRS was assessed by investigating how well it performed at identifying individuals with adult ADHD from the M.I.N.I. Plus diagnostic assessment (Table 4). The six-item ASRS using the standard threshold score of ≥4 produced a sensitivity of 80% and a specificity of 55%. Lowering the threshold to ≥3 increased the sensitivity to 93%, at the expense of specificity (47%). Whereas increasing the threshold to ≥5 reduced the sensitivity to 67%, but increased the specificity of the instrument to 78%. The area under the ROC curve found a threshold of ≥5 produced the most accurate test with a value of 0.72.
Validity of the ASRS Screener in Predicting ADHD Diagnosis on M.I.N.I. Plus (n = 88).
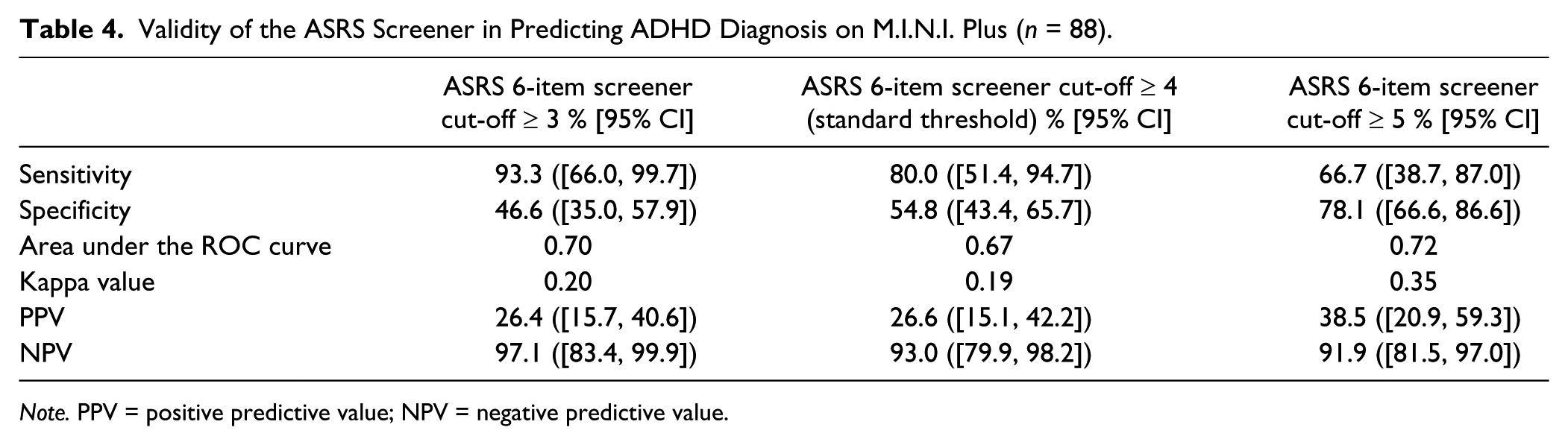
Note. PPV = positive predictive value; NPV = negative predictive value.
Discussion
A third (35%) of the prisoner sample screened positive for ADHD and, upon further diagnostic assessment, 17% met criteria for adult ADHD. The prevalence of adult ADHD among this prison sample is considerably higher (17%) than estimates in the general population (2%-3%; Simon et al., 2009), but is consistent with previous research among prisoners and individuals with SUDs (10%-29%; Daigre et al., 2009; Konstenius et al., 2015; Rosler et al., 2009; Westmoreland et al., 2010). Considering the lack of research on adult ADHD among prisoners, particularly in Australia, the current study makes an important contribution to the evidence base. Variations in the prevalence of adult ADHD across studies are likely to be due, at least in part, to methodological differences including sample size, demographics of the sample (i.e., sampling women or men only), or the type of clinical interview used to assess DSM-IV criteria (i.e., M.I.N.I-Plus vs. the ADHD Diagnostic Checklist vs. the Connors’ Adult ADHD Diagnostic Interview; Konstenius et al., 2015; Rosler et al., 2009).
The current study found no significant gender differences in the prevalence of adult ADHD. While this is supported by a larger study of prisoners in the United States (Westmoreland et al., 2010), other studies among offender samples report conflicting evidence (Robertson, Dill, Husain, & Undesser, 2004; Rosler et al., 2009; Teplin, Abram, McClelland, Dulcan, & Mericle, 2002). Prisoners identifying as Aboriginal were found to be significantly more likely to have a diagnosis of adult ADHD in the current study. Research on ADHD among indigenous people worldwide is scarce, and to our knowledge, there are no previous Australian studies. The findings reported by Azevedo and Caixeta (2009) from in-depth clinical interviews with Brazilian indigenous children provide some support for the existence of core ADHD symptoms (i.e., inattention, hyperactivity, and impulsiveness) as well as associated difficulties with family and school environments. Similarly, a Canadian study found a high prevalence of ADHD in Aboriginal children, but the authors suggest that unique learning styles among Aboriginal children may incorrectly lead to an ADHD diagnosis (Baydala, Sherman, Rasmussen, Wikman, & Janzen, 2006). Given the lack of research, the validity of the ADHD diagnosis among indigenous Australians is questionable, and more work in this area is clearly needed (Azevedo & Caixeta, 2009).
Inattention symptoms of ADHD were more prevalent than symptoms on the hyperactivity/impulsivity dimension, which is consistent with prior research with offender and SUD samples (Kaye, Darke, & Torok, 2013; Konstenius et al., 2015) as well as with findings from a longitudinal study which found symptoms of hyperactivity/impulsivity declined at a higher rate than symptoms of inattention (Biederman, Mick, & Faraone, 2000). Symptoms of inattention typically reflect an individual’s usual behavior, whereas symptoms of hyperactivity/impulsivity are more likely to be influenced by transient factors such as substance use or the prison environment (Kaye et al., 2013). These findings suggest that offenders have the ability to reflect on their usual behavior (as instructed) when questioned using the ASRS (Kaye et al., 2013).
The majority of those who screened positive for ADHD had never been diagnosed with ADHD (either in childhood or as an adult), which is consistent with other research (Faraone, Spencer, Montano, & Biederman, 2004; Kaye et al., 2013; McAweeney, Rodgers, Huddleston, Moore, & Gentile, 2010). It is possible, given the average age of the inmates was 41 years, that some childhood-onset ADHD diagnoses were overlooked given a change in knowledge and awareness of ADHD over the last two decades (Faraone et al., 2004; Kaye et al., 2013). In fact, adult ADHD was not recognized in the Diagnostic and Statistical Manual for Mental Disorders until the most recent edition (DSM-IV-TR; APA, 2000). It has also been suggested that ADHD is commonly undiagnosed in individuals presenting with other psychiatric disorders, even in patients who express concerns about symptoms typical of ADHD, or that ADHD symptoms escalate in adulthood when individuals are faced with challenges of independent living (Faraone et al., 2004). Moreover, there is a belief among some mental health clinicians that ADHD among adults is not a true disorder, particularly given that some symptoms associated with ADHD are common among illicit drug users (who may or may not have ADHD; e.g., impulsivity), particularly in the context of comorbid personality disorders (Kalbag & Levin, 2005). Integrated treatment for substance misuse and psychiatric disorders is clearly needed, but many services are not equipped with resources to deal with this need (McAweeney et al., 2010). In particular, there is a need for adult ADHD to be accepted as a mental health disorder and for treatment to be offered without prejudice, and without the assumption that those who have a history of illicit drug use are drug seeking or will misuse their medication.
A number of sociodemographic correlates were found to be higher among individuals with a diagnosis of adult ADHD compared to those without ADHD including younger age of first contact with the criminal justice system, substance dependence, and comorbid psychiatric disorders. Despite a paucity of research on ADHD among prisoners, Rosler and colleagues (2009) found that female prisoners with ADHD were significantly younger at their first conviction, compared to females without ADHD. Substance use and misuse have been associated with ADHD in numerous prior studies. In studies with offenders, substance use disorders, particularly stimulant use/dependence, have been identified as significantly higher among individuals with ADHD compared to those with no ADHD (Konstenius et al., 2015; Rosler et al., 2009). Stimulants have a paradoxical effect among people with ADHD, in which they experience a calming effect and an increased ability to focus and concentrate (hence, treatment of the disorder with stimulant medication). Consequently, those who may not have been diagnosed or remain untreated may be self-medicating with nonprescribed or illicit stimulants. A study of illicit psychostimulant users found that those with ADHD had a more extensive drug use history including lifetime polydrug use, which remained significant after adjusting for demographics, drug use, treatment history, and psychopathology (Kaye et al., 2013). As alluded to above, the relationship between ADHD and SUD is complicated by the heterogeneity of symptoms. Research has found that ADHD complicates the course and treatment of SUDs. ADHD has consistently been associated with earlier onset, greater severity and increased chronicity of substance use and dependence and a greater level of impairment particularly in the context of other psychiatric comorbidities (Arias et al., 2008; Carpentier, van Gogh, Knapen, Buitelaar, & De Jong, 2011). Further, SUD among those with ADHD is more difficult to treat, and is associated with lower rates of treatment retention and higher rates of relapse (Upadhyaya, 2007; Wilens, 2007).
While there has been increasing recognition of the comorbidity between ADHD and SUD, there is less recognition of, and no routine screening for, ADHD among prisoners, a clinical population known to have significantly elevated rates of SUD and mental health disorders compared to the general population (Butler et al., 2006). Furthermore, there is no consistent approach to treatment for ADHD among prisoners in NSW. The treatment of ADHD among prisoners is complicated by the large proportion of prisoners who are psychostimulant users (Indig et al., 2010). Recent work suggests that nonstimulant agents, antidepressants, and extended-release or longer-acting stimulants may be preferable treatment as the potential for misuse and diversion is lower (Wilens & Morrison, 2011). Encouragingly, recent research has shown a significant reduction in the criminality rate for a large sample of over 25,000 individuals with ADHD during medication versus nonmedication periods (i.e., a 32% reduction for men; 41% reduction for women; Lichtenstein et al., 2012). While more work is needed among prisoners, the research clearly indicates that identification of undiagnosed and/or untreated ADHD is likely to improve reoffending outcomes.
Consistent with prior research (Konstenius et al., 2015; Rosler et al., 2009; Westmoreland et al., 2010), levels of psychopathology—BPD, social phobia, and ASPD in particular—were significantly higher in participants with adult ADHD, compared to those without adult ADHD. Rosler et al. (2009) also found a diagnosis of BPD to be significantly more likely among ADHD versus non-ADHD female offenders. It is perhaps not surprising that associations have been identified between ADHD and BPD, given that the disorders share some core traits, such as impulsivity, angry outbursts, affective instability, and feelings of boredom (Davids & Gastpar, 2005). This overlap in symptomatology may lead to under-diagnosis of ADHD in prisoners presenting with symptoms thought to be due to a diagnosed personality disorder. These findings suggest that more attention on ADHD and comorbid BPD is warranted. It would be of interest to further review those diagnosed with ADHD and BPD, and perhaps males diagnosed with ASPD and ADHD, to determine whether they do in fact still meet the criteria for the personality disorder in the context of the ADHD diagnosis. Furthermore, differing treatment approaches may need to be considered for prisoners with comorbid ADHD and BPD to address deficits, particularly in affect regulation and impulse control (Davids & Gastpar, 2005).
In the current study, the six-item ASRS screener achieved a sensitivity of 80.0% and a specificity of 54.8% against the diagnostic assessment. The sensitivity and specificity from the current study is lower than that reported from general population studies (68.7% and 99.5%; Kessler, et al., 2005), research among prisoners (100.0% and 66.0%; Konstenius et al., 2015), and substance users (87.5% and 68.8%; Daigre et al., 2009). With the relatively small sample size in the current study, the confidence intervals for sensitivity and specificity fit with prior estimates. Comparisons across studies are difficult, given methodological differences, particularly in the use of varying diagnostic tools. Some prior studies, for example, have assessed the ASRS against the Conners’ Adult ADHD Diagnostic Interview for DSM-IV (CAADID), which is arguably more comprehensive as it collects collateral information from parents and teachers (Daigre et al., 2009; Konstenius et al., 2015).
The results of the validity testing of the ASRS screening instrument against the diagnostic assessment suggest that a lower threshold cut off (≥3 vs. ≥4) warrants further research attention. The lower threshold produced a higher sensitivity but a slightly lower specificity, compared to the standard threshold. These findings are in line with Daigre and colleagues (2009) among individuals with SUDs. Daigre et al. (2009) argued that greater sensitivity is potentially more important at the expense of specificity. A higher sensitivity level would lead to an increase in the identification of false positives requiring a thorough diagnostic assessment, whereas a higher specificity level would lead to a deviation from the original aim of the tool as a screening instrument (Daigre et al., 2009). While the six-item screener appears to be sensitive for identifying possible ADHD cases among a prison sample, further work is required in a larger sample before appropriate conclusions can be drawn.
Results from the current study (i.e., 33% of adult ADHD cases specified an age of onset <7 on ASRS; 75% specified an age of onset ≤ 12 years old) support changes to the age of onset cut-off to <12 years in DSM-V (APA, 2013). This change was based on evidence from numerous studies suggesting that revisions to the ADHD age of onset cut-off could help to minimize false negatives (and improve specificity) when a diagnosis is made later in life due to retrospective recall bias (Kieling et al., 2010; Todd, Huang, & Henderson, 2008). In addition, results from a prospective birth cohort study found that prevalence estimates, correlates, and risk factors for ADHD are not affected if the new diagnostic scheme extends the age-of-onset criterion to age 12 (Polanczyk et al., 2010).
A number of limitations from the current study should be considered in interpreting the results. As described in the methodology, the randomization procedure was changed toward the end of the recruitment to account for a lower proportion of ADHD participants being allocated to the full assessment. Despite the change in the randomization procedure, analyses on the full assessment sample showed an equitable split in the proportion screening positive or negative for ADHD on the ASRS (51.1% vs. 48.9%, respectively). The small sample size in the current study makes it difficult to generalize the results to a larger sample of prisoners. Further, we were unable to compare the characteristics of participants versus individuals who refused to participate. While the small sample size may not necessarily be representative of the NSW prisoner population, the basic demographic characteristics reflect those reported in the 2009 NSW Inmate Health Survey of 996 prisoners (Indig et al., 2010). While an association between ADHD and other psychiatric disorders was clearly evident, the cross-sectional design and assessment of lifetime psychiatric disorders made it impossible to draw causal inferences. In addition, the findings are limited as they are based on self-report and may be subject to retrospective recall bias. The ASRS, however, was designed to be a self-report measure (Kessler, et al., 2005) and has been validated in SUD populations (Daigre et al., 2009), and prisoners (Konstenius et al., 2015). In addition, there is evidence that self-report can be a valid and reliable way of measuring behavior among injecting drug users (Darke, 1998). No differences were found between prisoners with and without ADHD by type of crime ever committed. The questionnaire only included questions on types of crimes committed over the offenders’ lifetime which limited our ability to examine this issue further.
Conclusion
Despite these limitations, the current study found that the proportion of NSW prisoners with adult ADHD was similar to prior research on prisoners and SUD populations. The study also found a higher prevalence of adult ADHD among prisoners with SUD and other psychiatric comorbidities. The results suggest that there is a need among clinicians for greater acceptance of ADHD as a true psychiatric disorder in adults. Recognizing ADHD as a valid disorder among adults, particularly prisoners, also warrants greater effort in diagnosis and providing appropriate treatment options. The study also found that while the ASRS is useful among a NSW prisoner sample, a lower cut-off should be investigated in future research. The findings suggest that appropriate identification of ADHD among adults is likely to result in positive outcomes not only for the individual but also in cost savings to the community through reduced contacts with the criminal justice system.
Footnotes
Acknowledgements
The authors would like to acknowledge that this study was internally funded by Justice and Forensic Mental Health Network. We would like to thank Natasha Sindicich, Julia Rosenfeld and Phe Affleck who assisted with interviewing the participants, and Dr. Libby Topp who was involved in the development of the study. We would also like to thank the Nursing Unit Managers and Corrective Services NSW staff who assisted the research team with gaining access to the participants. Lastly, we would like to thank the participants themselves for taking part.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.