
Abstract
ADHD has predominantly been viewed as a childhood disorder, and research has started to focus on the characteristics of ADHD in adulthood only in recent years (Rucklidge, Brown, Crawford, & Kaplan, 2007). Studies have revealed that in 40% to 60% of children with ADHD, the disorder continues into adulthood (Davidson, 2008); the prevalence of ADHD in adulthood is estimated to be between 2.5% to 4.7% (de Zwaan et al., 2012; Fayyad et al., 2007; Kessler et al., 2006; Simon, Czobor, Bálint, Mészáros, & Bitter, 2009). Adults with ADHD show impairment in multiple domains of self-regulation, such as academic achievement, cognitive performance, and psychiatric well-being (Biederman, Faraone, Monuteaux, Bober, & Cadogen, 2004; Rucklidge et al., 2007). For instance, they are at risk for cognitive problems (Biederman et al., 2004), impaired physical and psychological functioning (Klein et al., 2012; Ramos Olazagasti et al., 2013), and obesity (Cortese, Faraone, Bernardi, Wang, & Blanco, 2013).
College Students With ADHD
College students with ADHD who have managed to graduate from high school and gain admittance to a postsecondary institution are considered a subpopulation of individuals with ADHD because they are expected to be less impaired by their ADHD symptoms compared with adults with ADHD from the general population (Merkt et al., 2013). Thus, college students with ADHD have experienced more academic success, which may lead to a stronger belief in their abilities (Nelson & Gregg, 2012); they may have a less severe form of the disorder (Nelson & Gregg, 2012); and they are likely to have higher ability levels, greater academic success during primary and secondary school, and better compensatory skills (Frazier, Youngstrom, Glutting, & Watkins, 2007). Although they show less impairment compared with other adults with ADHD, college students with ADHD show more impairment compared with their fellow students without ADHD (Weyandt & DuPaul, 2008). One domain in which impairment has repeatedly been found in adults and college students with ADHD is health.
Health
ADHD in adulthood has been related to various health problems such as sexually transmitted disease, head injury, emergency department admissions (Ramos Olazagasti et al., 2013), overweight (Cortese et al., 2008), a greater prevalence of psychiatric disorders (Kessler et al., 2006; Klein et al., 2012; Ramos Olazagasti et al., 2013), and a diminished health-related quality of life (Gjervan, Hjemdal, & Nordahl, 2012; Gjervan, Torgersen, Rasmussen, & Nordahl, 2014). Findings in college students with ADHD are still sparse. In one recent study, college students with self-reported ADHD displayed more noxious behaviors such as substance and alcohol abuse and smoking initiation (Blase et al., 2009). College students with self-reported ADHD also showed impaired psychological functioning; thus, they gave significantly higher ratings on somatization, obsessive compulsive disorder, interpersonal sensitivity, depression, anxiety, hostility, paranoid ideation, and psychoticism (Richards, Rosen, & Ramirez, 1999). However, to our knowledge, health-related quality of life in college students with ADHD has not been explored yet. A second domain that is strongly related to health issues and in which problems of adults with ADHD have been demonstrated repeatedly but has not been the focus of studies with college students yet is the domain of overweight and dietary habits.
Dietary Habits
ADHD and overweight/obesity seem to be interrelated. Thus, on one hand, in obese populations increased ADHD symptoms can be found, and on the other hand, children with ADHD and men with ADHD showed a higher body mass index (BMI) than would be expected in the general population (Cortese et al., 2008; Cortese, Ramos Olazagasti, et al., 2013). Furthermore, there is a greater likelihood of overweight and obesity in adults with ADHD symptoms (Pagoto et al., 2008). However, an epidemiological study showed that the relation of ADHD diagnosis and obesity in adulthood disappeared when controlling for mood or anxiety disorders (Cortese, Faraone, Bernardi, Wang, & Blanco, 2013). The number of ADHD symptoms before the age of 18 years was still associated with obesity in adulthood even after controlling for comorbid disorders in women but not in men (Cortese, Faraone, et al., 2013). Importantly, there are no studies investigating overweight or dietary habits in college students with ADHD.
Achievement Motivation
Impaired academic achievement in children and in college students with ADHD has been demonstrated repeatedly (Frazier et al., 2007; Weyandt & DuPaul, 2008). However, college students with ADHD managed to graduate from high school and gain admittance to a postsecondary institution. One possible reason for good academic achievement despite ADHD could be a high achievement motivation. Achievement goals are important for academic success and achievement because they can predict academic performance independently from cognitive ability (Harackiewicz, Barron, Tauer, & Elliot, 2002). However, research on achievement goals in ADHD is sparse. Findings so far suggest that children with ADHD show a maladaptive attributional style. Thus, children with ADHD set themselves performance goals rather than learning goals (Dunn & Shapiro, 1999). However, learning goals are important for success in school because they lead to seeking future challenges and increased persistence. Further studies showed that adolescents with ADHD focused on avoiding failure rather than achieving success (Milich & Okazaki, 1991; Olivier & Steenkamp, 2004), and there seems to be a stronger association between achievement motivation and academic performance in children with ADHD compared with children without ADHD (Gut, Heckmann, Meyer, Schmid, & Grob, 2011). Although achievement motivation is vital for academic performance in ADHD, to our knowledge achievement motivation in college students with ADHD has not been previously examined.
Gender Differences
It seems to be important to focus on gender differences in college students with ADHD because two recent studies have revealed such ADHD caused gender differences. However, findings regarding gender differences in children and adults with ADHD are highly heterogeneous (Fedele, Lefler, Hartung, & Canu, 2012; O’Callaghan & Sharma, 2014). Meta-analyses on gender differences in children have repeatedly reported lower levels of hyperactivity and less externalizing behavior in girls with ADHD (Gaub & Carlson, 1997; Gershon, 2002). Furthermore, some studies have demonstrated greater intellectual impairment (Gaub & Carlson, 1997) and more internalizing behavior in girls (Gershon, 2002). Some of these differences were accounted for by moderator variables such as referral source (i.e., clinic vs. community). For example, non-referred samples of girls with ADHD show less impairment than boys with ADHD (Gaub & Carlson, 1997), and among clinic-referred populations, girls and boys with ADHD showed similar levels of impairment (Gaub & Carlson, 1997).
There is even less and more heterogeneous research on gender differences in adult ADHD (Rucklidge et al., 2007). Some studies have found no gender differences (Biederman et al., 2004; Rucklidge et al., 2007) but other studies have (Fedele et al., 2012; O’Callaghan & Sharma, 2014). When gender differences have been recorded in adults with ADHD, greater impairment has been shown in women (Fedele et al., 2012; O’Callaghan & Sharma, 2014). Regarding gender differences in college students with ADHD, most of the existing studies either did not include any females or only included a very small number of females. A review of ADHD in college students did not find gender differences (Weyandt & DuPaul, 2008). However, one study found higher rates of inattention, hyperactivity, and impairment in social life, education, money management, and daily life activities in women (Fedele et al., 2012). A second study found lower ADHD-related quality of life and psychological health in female students compared with male students with ADHD (O’Callaghan & Sharma, 2014). On the basis of these inconsistent findings, we aimed to include a higher number of female college students with ADHD in our sample to explore gender differences in more detail.
Referral Bias as Cause for Gender Differences
It has been discussed whether the gender differences in adults with ADHD are true reflections of the phenotype or may represent diagnostic artifacts or a referral bias (Biederman et al., 2004), which means that boys are referred to receive a diagnosis more often and girls are only referred if they show higher impairment (i.e., more severe ADHD or more comorbid symptoms). Boys received an ADHD diagnosis 4.38 times more than girls. However, when taking symptoms above a clinical cut-off as the criterion, boys were affected only 1.77 times more than girls (Huss, Hölling, Kurth, & Schlack, 2008). Thus, the gender ratio is more unequal (i.e., more boys) in clinical compared with epidemiological samples (i.e., similar numbers of boys and girls; Gaub & Carlson, 1997).
One explanation for this observed low referral rate of girls with ADHD might be the low prevalence of comorbid externalizing problems in girls (Gershon, 2002). Boys with ADHD showed more rule-breaking in school (Abikoff et al., 2002), and teachers, but not parents, reported more problems in boys (Derks, Hudziak, & Boomsma, 2007). Thus, it might be the case that females with ADHD are often not diagnosed because they show less disruptive behavior in childhood (Biederman et al., 2004; Biederman et al., 2005; McGee & Feehan, 1991). However, equal prevalence rates of ADHD in males and females in adulthood have been reported (Biederman et al., 1994; de Zwaan et al., 2012), and it has been suggested that this is due to many women with ADHD seeking psychiatric help as adults and hence receiving their diagnosis of ADHD later (Simon et al., 2009).
The timing of the diagnosis has vivid implications. Adults who did not receive their diagnosis in childhood but in adulthood reported higher rates of depression/anxiety, a more external locus of control, lower self-esteem, and a maladaptive attributional style (Rucklidge et al., 2007; Rucklidge & Kaplan, 1997). Unidentified ADHD can lead to misattributions of blame and thereby to more psychosocial problems (Rucklidge et al., 2007). Therefore, it is possible that unidentified childhood ADHD leads to greater impairment over the life course. Thus, we aimed to examine if gender differences in ADHD were mediated by the timing of the diagnosis.
Present Study
We conducted an online survey using questionnaires to assess psychological functioning, health-related quality of life, dietary habits, and achievement motivation in college students with and without self-reported ADHD diagnosis. We aimed to answer the following research questions: First, do college students with and without self-reported ADHD diagnosis differ in psychological functioning, health-related quality of life, dietary habits, and achievement motivation? On the basis of the current literature, we hypothesized that college students with ADHD would show worse psychological functioning, less health-related quality of life, and more maladaptive dietary habits. Furthermore, we assumed that college students with ADHD would report greater achievement motivation. Our second research question was as follows: Do gender differences exist that are specific to individuals with ADHD? We assumed that female college students with ADHD show even greater impairment in health compared with male students. On the basis of the literature, we did not have a hypothesis regarding gender differences in achievement motivation. Our third research question was: Are gender differences in college students with ADHD mediated by the timing of the ADHD diagnosis? We assumed that women received their diagnosis later than men and that this is related to higher impairment in general.
Method
Participants
Seventy-seven college students with self-reported ADHD (49 women; M = 25.82 years, SD = 4.62) and 120 college students without ADHD (65 women; M = 25.17 years, SD = 5.41) participated in this online survey.
Screening of cognitive abilities
Students completed five subtests of the Wechsler Adult Intelligence Scale (WAIS; von Aster, Neubauer, & Horn, 2006): the picture completion, the arithmetic, the vocabulary, the similarities, and the matrix-reasoning subtests. We chose these subtests as a screening for general cognitive abilities (i.e., IQ) because it is possible to administer them online. A MANOVA by Group × Gender revealed neither significant main effects nor interactions.
Socioeconomic status (SES)
To make sure college students with and those without ADHD did not differ in SES, we assessed the SES of participants by asking questions regarding the educational level, occupation status, and monthly income of themselves and their parents (Table 1). In a demographic questionnaire, participants had to indicate educational level (i.e., 1 = 9 years of education, 2 = 10 years of education, 3 = 12-13 years of education, 4 = university degree), occupation status (i.e., 1 = unemployed, 2 = low-wage employment, 3 = part-time employment, 4 = full-time employment), and monthly income (i.e., 1 = up to 1,500 €, 2 = up to 2,500 €, 3 = up to 4,000 €, 4 = more than 4,000 €). We used the mean of educational level, occupation status, and monthly income as an index for participants’ SES. We computed the mean of parental education (i.e., the educational level of the father if it was higher than the educational level of the mother and vice versa) and family income to form a parental SES index. ANOVAs by Group × Gender for SES did not reveal significant main effects nor any interactions for either participants’ or parents’ SES.
Characteristics of the Sample by Group and Gender.
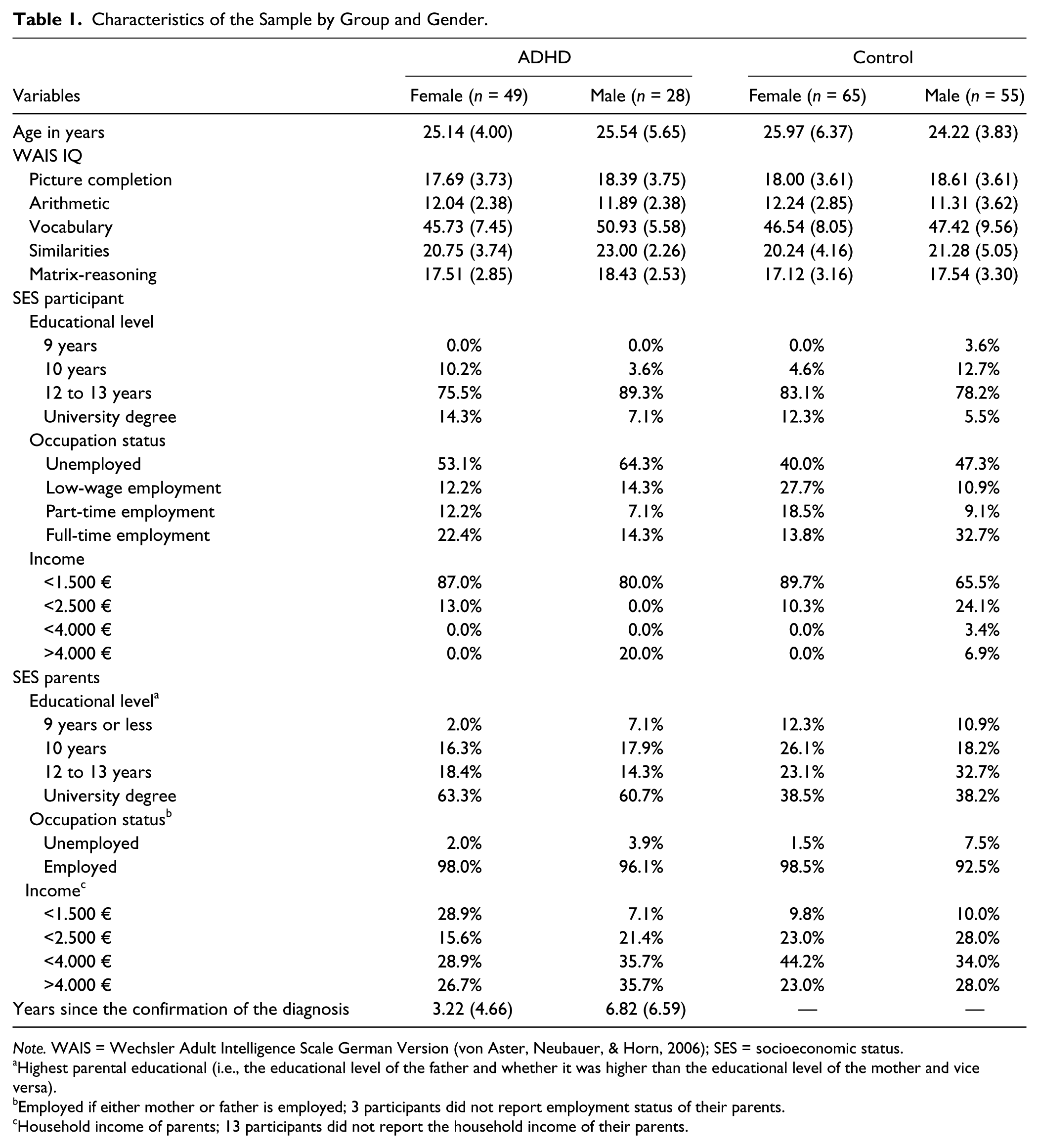
Note. WAIS = Wechsler Adult Intelligence Scale German Version (von Aster, Neubauer, & Horn, 2006); SES = socioeconomic status.
Highest parental educational (i.e., the educational level of the father and whether it was higher than the educational level of the mother and vice versa).
Employed if either mother or father is employed; 3 participants did not report employment status of their parents.
Household income of parents; 13 participants did not report the household income of their parents.
ADHD diagnosis
For the assessment of an ADHD-diagnosis, we asked participants if they had received a clinical diagnosis of ADHD (i.e., “Did you receive a diagnosis of ADD/ADHD?”). Men with ADHD were diagnosed 6.82 years (SD = 6.59) and women 3.22 years (SD = 4.66) before participation in the survey. Diagnoses were given by psychiatrists (57.3 %), medical practitioners (16.0 %), neurologists (13.3 %), pediatricians (8.0 %), and therapists (5.3 %). Fifty-one participants (36 women) in the ADHD group reported taking medication.
Design
The study followed a two-between (Group: ADHD vs. control) × two-between (Gender: female vs. male) design. Dependent variables were psychological functioning, health-related quality of life, dietary habits, and achievement motivation assessed with questionnaires.
Procedure
We conducted a web-based survey because this enabled us to draw a larger, more diverse sample and access a difficult-to-reach population (Gosling, Vazire, Srivastava, & John, 2000). This is important as in the past gender differences in college students with ADHD could often not be explored due to a lack of female participants (Weyandt & DuPaul, 2008). We posted the links for the survey in ADHD and psychology forums on a German social networking website for college students with approximately 15 million members (StudiVZ, http://www.studivz.net), and in forums for college students with ADHD, for female college students with ADHD, for females with ADHD, and students of psychology. Furthermore, we also asked students to share the link. The link directed interested students to the online survey conducted with Unipark (Globalpark AG, 2008). Computer IP addresses were tracked to allow only one entry from the same computer and enable participants to take breaks as often as they wanted. Answering the questions of the survey took participants between 40 and 197 min (M = 86.11, SD = 27.04), which is less than the total completion time that is estimated by the manuals of the respective questionnaires. An ANOVA did not reveal differences in the amount of time taken to complete the survey based on Group or Gender.
Measures
Psychological functioning—Brief Symptom Inventory (BSI)
Because studies in college students have reported poorer psychological functioning in college students with ADHD, we chose to use the BSI (Franke, 2000), which measures self-reported clinically relevant psychological symptoms in adolescents and adults. The BSI is the short version of the Symptom Checklist–Revised-90 (Derogatis, 1994). According to the manual, completion of the BSI requires 8 to 10 min and it consists of 53 items covering nine symptom dimensions: somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism, and three global indices of distress: Global Severity Index (GSI, mean of all items), Positive Symptom Distress Index (PSDI, mean of all non-zero-rated items), and Positive Symptom Total (PST, count of all non-zero items). The global indices measure current or past level of symptomatology, intensity of symptoms, and number of reported symptoms, respectively. The BSI has internal consistencies ranging from α = .63 to α = .85 and retest reliabilities from r = .73 to r = .92.
Health-related quality of life (SF-36)
We used the SF-36-Health Survey (Bullinger & Kirchberger, 1993) to measure health-related quality of life in the domains of physical health (mean of the scales physical functioning, physical role functioning, bodily pain, and general health perceptions) and mental health (mean of the scales vitality, social role functioning, emotional role functioning, and mental health). The SF-36 has 36 items, takes 10 min to complete, and has internal consistencies ranging from r = .57 to r = .94.
Dietary habits (FEV and EVT) and BMI
We assessed dietary habits with the Questionnaire for the Assessment of Eating Behavior (Fragebogen zur Erfassung des Essverhaltens [FEV]; Pudel & Westenhöfer, 1989), which is the German version of the Three Factor Eating Questionnaire (TFEQ, Stunkard & Messick, 1985). The FEV consists of 51 items assessing eating behavior, requires 15 min to complete, and includes three scales: cognitive restraint of eating, disinhibition, and hunger. The FEV has internal consistencies from r = .75 to r = .87 and split-half-reliabilities from r = .74 to r = .86. Furthermore, we used the Eating Behavior Test (Essverhalten-Test [EVT]; Böhm, 1998), which consists of 20 items that are summed up to assess risk for bulimia on the basis of the International Classification of Diseases (ICD) 10 criteria for bulimia. The EVT takes 15 min to complete and has an internal consistency of α = .96. We also asked participants to report their weight and height to compute their BMI.
Achievement motivation inventory (LMI)
We used the LMI to assess several aspects of achievement motivation (Schuler & Prochaska, 2001). The LMI was developed as a comprehensive measure of achievement motivation. It requires about 35 min to answer the 170 items in 17 scales. These scales have been shown to load onto 3 second-order factors (Byrne et al., 2004): independence (mean of the scales confidence in success, dominance, fearlessness, flexibility, eagerness to learn, preference for difficult tasks, and independence), ambition (mean of the scales compensatory effort, competitiveness, engagement, flow, goal setting, pride in productivity, and status orientation), and self-control (mean of the scales persistence, internality, and self-control). The LMI has internal consistencies from α = .68 to α = .86 for the sub-scales and α = .98 for the total scale. The retest-reliabilities for the scales range from r = .66 to r = .82 for the sub-scales and r = .86 for the total scale.
Results
ANOVAs
We conducted ANOVAs by Group (ADHD vs. control) and Gender (female vs. male) for the composite scores of all questionnaires. These are the GSI of the BSI, the physical health and mental health scores from the SF-36, the EVT score, the BMI, and the three factors of the LMI (i.e., independence, ambition, and self-control). Because there is no composite score for the FEV, the three scales (i.e., cognitive restraint of eating, disinhibition, hunger) were analyzed separately. We further explored the results by conducting ANOVAs on all the scales but focus on the report and discussion of the analyses from the composite scores. Means, standard deviations, effect sizes, and results for all ANOVAs are displayed in Table 2. We only report results that reached the Bonferroni corrected alpha level of p ≤ .001 (i.e., .05 divided by 45 ANOVAs). The only differences in the interpretation of results between corrected and uncorrected alpha levels were some main effects of Gender, which were not the focus of our survey, and effects of Group on dietary habits. We checked whether the results changed if we used medication as covariate. To answer our first research question (i.e., group differences between college students with and without self-reported ADHD diagnosis), we focused on the Group main effect. To answer our second research question (i.e., gender differences that are specific for ADHD), we focused on the interactions of Group and Gender.
Means and Standard Deviations and Results of ANOVAs for All Dependent Variables.
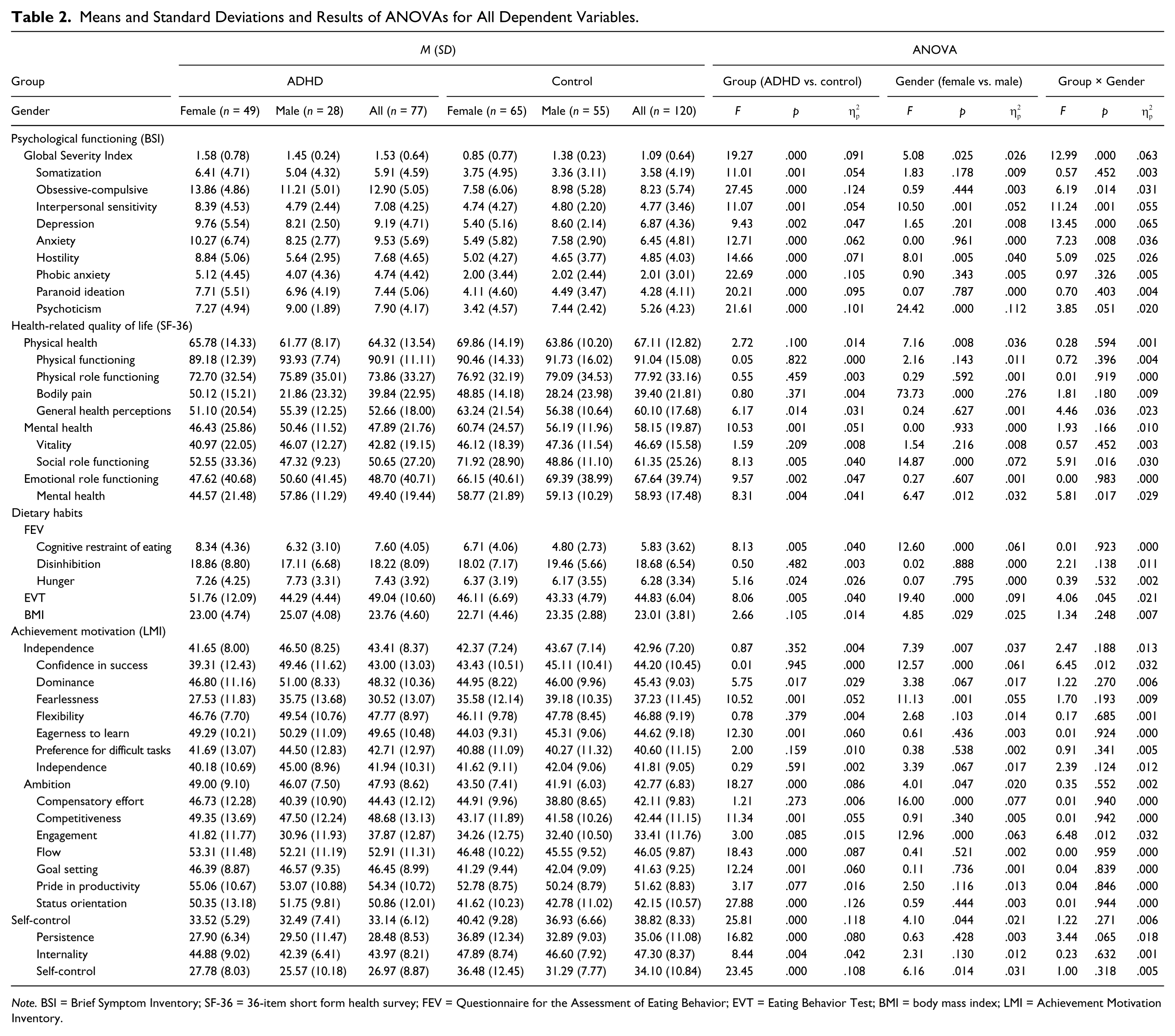
Note. BSI = Brief Symptom Inventory; SF-36 = 36-item short form health survey; FEV = Questionnaire for the Assessment of Eating Behavior; EVT = Eating Behavior Test; BMI = body mass index; LMI = Achievement Motivation Inventory.
Psychological functioning (BSI)
The ANOVA of Group × Gender for GSI, the mean of all items of the BSI revealed a significant main effects for Group, as well as a significant interaction. The exploration of the means displayed that the interaction was caused by the female college students with ADHD who demonstrated as much impairment as male students both with and without ADHD. Female students without ADHD showed less impairment. A closer inspection shows that there were significant or marginally significant group differences for all scales of the BSI. Students with ADHD showed worse psychological functioning on all scales. The Group difference in interpersonal sensitivity and depression was qualified by a Group × Gender interaction, which were caused by the high impairment in women with ADHD compared with women without ADHD in these constructs. Men with and without ADHD did not differ in these constructs.
Health-related quality of life (SF-36)
The ANOVA for physical health did not yield significant main effects nor interactions. However, the ANOVA for mental health showed that college students with ADHD report worse mental health-related quality of life.
Dietary habits (FEV and EVT) and BMI
The only significant effects were main effect of Gender on cognitive restraint of eating and the EVT, indicating that women report more restrained eating and risk for bulimia than men. The group differences in cognitive restraint of eating, hunger, and EVT, as well as the interaction of Group and Gender on the EVT did not reach the Bonferroni corrected significance level. The means indicated that participants with ADHD reported more cognitive restraint of eating and more hunger. Women with ADHD had a higher risk of bulimia compared with all other groups. When medication was used as covariate, the group difference in BMI between participants with and without ADHD became significant on the 5% alpha level, F(1, 190) = 4.28, p = .040, but not on the Bonferroni corrected alpha level of p ≤ .001. However, an ANOVA of Gender (female vs. male) and Medication (yes vs. no) on BMI did not reveal significant main effects or interactions.
Achievement motivation (LMI)
The ANOVA of Group × Gender for independence did not reveal significant main effects nor interactions. However, the ANOVAs for ambition and self-control showed significant main effects for Group. College students with ADHD reported higher ambition but less self-control. The main effect of Group on ambition was not significant anymore if controlled for medication, F(4, 192) = 3.49, p = .063. Participants with ADHD who took medication reported higher ambition (M = 49.88, SD = 8.50) compared with participants who did not take medication (M = 45.75, SD = 8.59), but the difference was not significant, t(75) = 1.61, p = .133.
Mediations
To explore our third research question (i.e., relation of gender differences in ADHD to timing of diagnosis), we performed mediation analyses and report results of the stepwise procedure (Baron & Kenny, 1986) and test the significance of the indirect effect using the PROCESS macro for SPSS by Hayes (Preacher & Hayes, 2004) applying a 95% confidence interval (CI) with bootstrapping procedure with 5,000 resamples (Preacher & Hayes, 2008). Twelve separate mediation analyses were run for all scales that showed significant interaction of Group and Gender on the 5% alpha level (i.e., obsessive compulsive behavior, interpersonal sensitivity, depression, anxiety, hostility, psychoticism, general health perceptions, social role functioning, mental health on the scale not the composite score level, EVT, confidence in success, and engagement) and for all scales that showed significant correlation with the timing of the diagnosis (i.e., compensatory effort, r = −.25, p < .05). Only participants with ADHD were included and Gender was used as predictor. Then, we checked whether the effect was mediated by the timing of the diagnosis.
Only the mediations on obsessive-compulsive behavior and compensatory effort were significant. All other mediations did not meet the criteria of the stepwise procedure (Baron & Kenny, 1986) and did not show a significant indirect effect (Preacher & Hayes, 2004), demonstrating that the relation between Gender and the other outcome variables (i.e., interpersonal sensitivity, depression, anxiety, hostility, psychoticism, general health perceptions, social role functioning, mental health on the scale not the composite score level, bulimia, confidence in success, and engagement) was not significantly influenced by the timing of the diagnosis. Gender predicted timing of the diagnosis, t(73) = −2.75, p < .05, and obsessive-compulsive behavior, t(73) = 2.17, p < .05. In addition, the direct effect of Gender on obsessive-compulsive behavior disappeared, when controlling for timing of the diagnosis, t(72) = 1.66, ns, suggesting a full mediation (Baron & Kenny, 1986). The bias-corrected bootstrap 95% indicated that timing of the diagnosis mediated the relation of Gender and obsessive-compulsive behavior, B = .538, CI = [0.004, 1.561]. The effect size kappa-squared (Preacher & Kelley, 2011) was κ2 = .050, with 95% CI = [0.007, 0.134]; κ2 can be interpreted defining a small, medium, and large effect sizes as .01, .09, and .25, respectively. Gender also predicted compensatory effort, t(73) = 2.22, p < .05. The direct effect of Gender on compensatory effort disappeared, t(72) = 1.63, ns., when controlling for timing of the diagnosis, thus suggesting a full mediation. The bias-corrected bootstrap 95% indicated that timing of the diagnosis mediated the relation of Gender and compensatory effort, B = 1.517, CI = [0.002, 4.742]; κ2 = .058, with 95% CI = [0.007, 0.168].
Discussion
The aims of this study were first, to compare college students with and without self-reported ADHD diagnosis in aspects of psychological functioning, health-related quality of life, dietary habits, and achievement motivation; second, to explore gender differences that are specific to ADHD; and third, to find out whether gender differences are mediated by the timing of the diagnosis.
Group and Gender Differences
Health
College students with ADHD reported greater impaired psychological functioning and mental health compared with college students without ADHD. The results are in line with current findings of impaired psychological functioning in college students with self-reported ADHD (Richards et al., 1999; Weyandt, Rice, Linterman, Mitzlaff, & Emert, 1998). Our survey extends findings of impaired health-related quality of life in adults with ADHD (Gjervan, Hjemdal, & Nordahl, 2012; Gjervan, Torgersen, et al., 2014) showing that impaired health-related quality of life with regards to mental health can also be found in college students with ADHD. The group differences in psychological functioning (GSI), interpersonal sensitivity, and depression were qualified by Group × Gender interactions. Women with ADHD who showed the highest impairment compared with the other groups caused this pattern. This is in line with two recent studies that found higher impairment in female college students as compared with male college students regarding ADHD-related quality of life and psychological health (O’Callaghan & Sharma, 2014) and more inattention, hyperactivity, and impairment in females compared with male students with ADHD (Fedele et al., 2012).
It has been proposed that gender differences—especially more impairment in women—can only be found in clinical samples and not in population-based samples because many females with ADHD do not receive a diagnosis unless they exhibit a strong impairment (i.e., more ADHD symptoms, more comorbid psychiatric problems, worse health; Derks et al., 2007). Our sample only includes cases with a clinical diagnosis of ADHD and our finding of worse health in female college students with ADHD as compared with male college students might be caused by a referral bias. It is possible that women with ADHD with higher psychological functioning did not seek for or receive a diagnosis of ADHD. A second explanations is that males and females do not differ in impairment in childhood, but females are not diagnosed and therefore not treated until adulthood (Biederman et al., 2004), which leads to an accumulation of comorbid symptoms and health problems in females with ADHD in adulthood (Rucklidge et al., 2007). To test this explanation, we checked if gender differences were mediated by the timing of the diagnosis (see Timing of Diagnosis).
Dietary habits
The group differences and the interaction of Group and Gender did not reach the Bonferroni corrected significance level. There is no clear indication that dietary habits in college students with ADHD are impaired like in other adults with ADHD (Cortese, Ramos Olazagasti, et al., 2013). However, the means indicated that college students with ADHD show higher cognitive restraint of eating and more hunger. Furthermore, female college students with ADHD show a higher risk of bulimia compared with all other groups. There is a greater likelihood of overweight and obesity in adults with ADHD symptoms (Pagoto et al., 2008) and suggestions have been made that ADHD symptoms are only related to obesity in adulthood in women but not in men (Cortese, Faraone, et al., 2013). However, we did not find a higher BMI in participants with ADHD compared with participants without ADHD. It is possible that women with ADHD in our sample are more aware of their overeating and therefore conduct counteractive actions as for instance vomiting, or the intake of diuretics, that are not pursued by all women with ADHD.
Achievement motivation
We found group differences in achievement motivation. Lower self-control in college students with ADHD was expected because impaired self-control is an important characteristic of ADHD (i.e., Gawrilow, Gollwitzer, & Oettingen, 2011). College students with ADHD in our sample also displayed higher ambition, but this effect disappeared when medication is used as a covariate. However, participants with ADHD who took medication and those who did not indicated the same level of ambition. Although these results warrant replication, it would be interesting to explain how these effects come about. For instance, there are studies suggesting that a high motivation can help individuals with impairments to enter and succeed in higher education, as college students with learning disabilities were found to have a higher need for achievement compared with students without learning disabilities (Hall, Spruill, & Webster, 2002). In addition, findings suggest that achievement motivation shows a higher relation to actual performance in children with ADHD than in children without ADHD, and that a high motivation or specific volitional strategies of goal stetting can help children with ADHD to perform on the same level of children without ADHD (Gawrilow & Gollwitzer, 2008; Gut et al., 2011). Perhaps the high ambition reported by our sample of college students with ADHD helped them to achieve an academic performance in school that allowed them to enter higher education despite their ADHD.
Timing of Diagnosis
Because gender differences might be caused by referral bias leading to an under diagnosis of girls with ADHD (Biederman et al., 2005), we wanted to explore if timing of the diagnosis mediated the relation between gender and outcome in the ADHD group. The women in our survey were diagnosed on average 3.6 years later than the male participants. It is possible that the later diagnosis led to the assembly of more health-related problems in the women. We found full mediations for obsessive-compulsive behavior and compensatory effort. This suggests that male and female college students with ADHD do not differ in obsessive-compulsive behavior and compensatory effort per se but that differences are driven by the fact that women receive their diagnosis later than men. Obsessive-compulsive behavior and compensatory effort seem to be specific behaviors or strategies that are adopted when individuals with ADHD do not receive their diagnosis early in life. Interestingly, a recent study found higher levels in obsessive-compulsive behavior in a sample of female college students with ADHD that also show a cautious strategy of trading speed for accuracy in a flanker task and therefore produce less errors compared with female students without ADHD (Merkt et al., 2013). Furthermore, academically less successful students with ADHD spend more time using coping mechanisms and this is maladaptive because they have less time to study (Kaminski, Turnock, Rosén, & Laster, 2006). It seems likely that women with ADHD who were not diagnosed and therefore not treated in childhood adopt more maladaptive coping strategies such as being overly cautious, almost obsessive-compulsive, and invest more compensatory effort.
A second possible explanation is that more obsessive-compulsive behavior and compensatory effort lead to the later diagnosis. Maybe being overly cautious to prevent any errors and showing certain obsessive-compulsive behaviors, such as controlling assignments before handing them in, leads to comparably high performance and therefore girls with this behavior are less likely to get a diagnosis. Only when demands get higher, for instance, when entering university the ADHD symptomology cannot be sufficiently compensated by strategies like overly cautious behavior anymore, that women seek help in psychiatric settings.
However, many of the gender differences (i.e., interpersonal sensitivity, depression, anxiety, hostility, psychoticism, general health perceptions, social role functioning, mental health, bulimia, engagement and confidence in success) were not mediated by the timing of the diagnosis. Therefore, we cannot draw the conclusion that women show worse health only because they received the diagnosis later and were not treated before. Maybe even as adults women have to show higher impairment to receive a diagnosis of ADHD.
Implications
College students with ADHD do not only suffer from impaired academic achievement and psychological functioning (Weyandt & DuPaul, 2008), but they are also impaired in other health-related domains as for instance health-related quality of life and these should be targeted in interventions as well. Furthermore, it seems important to note that although ADHD is more frequent in boys in childhood, female college students with ADHD show high health-related impairment and might need interventions that are adapted to their specific needs.
We discuss whether a higher achievement motivation or overly cautious behavior could be a compensatory mechanism in college students with ADHD. However, because academic achievement is not tested with standardized measures in Germany (as, for example, the grade point average), it is difficult to compare students studying different subjects. Hence, we cannot test if the compensatory mechanisms that we assume actually mediate the relationship between ADHD and achievement. Future research might want to use standardized tests to study the effect of achievement motivation and overly cautious behavior on the achievement of college students with ADHD.
If they prove to be helpful for individuals with ADHD, compensatory strategies can be taught in interventions. This has been suggested before (Newark & Stieglitz, 2010). However, we still lack knowledge of which compensation strategies are used by individuals with ADHD, how these strategies were adopted over the life span, and which of these strategies are adaptive and which are maladaptive. The same strategy could be adaptive or maladaptive depending on the frequency of use. For example, a high rate of obsessive-compulsive behavior or a generally higher caution could help college students with ADHD to make fewer errors and therefore pass their exams. However, if this behavior becomes too pronounced, it could become a comorbid condition causing even further impairment in quality of life over and above the ADHD symptoms. If girls with ADHD are under diagnosed due to them adopting specific compensatory mechanisms such as being overly cautious, this should be taken into account when diagnosing ADHD in girls.
Limitations
An important limitation of this survey is that we only assessed the participants’ self-reported diagnosis of ADHD. However, psychosocial functioning of students with self-reported ADHD is very similar to functioning in students with confirmed diagnosis (Richards et al., 1999). Furthermore, all our results are in line and not contradictory with previous findings. Another limitation concerns the online administration of the survey; it is possible that only a preselected sample of college students with and without ADHD decided to participate. However, research on generalizability of online samples shows that they are generally more diverse than samples tested with traditional methods (i.e., paper-and-pencil administration of questionnaires) with respect to gender, SES, geographic location, and age (Gosling et al., 2000). This is because the wide accessibility of web questionnaires makes them available to a large and broad audience (e.g., physically handicapped, shy, and disorganized individuals, Gosling et al., 2000). Furthermore, online surveys take less effort and time to participate compared with studies conducted at a laboratory. Comparisons of online and paper-and-pencil methods of data collections have revealed that results are comparable for questionnaires (Gosling et al., 2000; Weigold, Weigold, & Russell, 2013), achievement tests (Preckel & Thiemann, 2003), and even experiments (McGraw, Tew, & Williams, 2000). Online administration might even be beneficial when it comes to health behavior, because bias of sensitive topics is reduced (Ramo, Hall, & Prochaska, 2011). However, web samples are not randomly drawn and only include volunteers (Gosling et al., 2000). Therefore, we assume that our sample is not representative for participants with and without ADHD in a complete randomly drawn sample—but at least more representative as compared with self-selected samples of college students with and without ADHD that could have been included in laboratory-based studies. Due to time constrains, we did not use a questionnaire to asses ADHD symptoms and therefore, have no continuous measure of ADHD. We cannot test whether females with ADHD display lower level of ADHD symptoms and how this is related to impairment in health or motivation. To really test the influence of the timing of the diagnosis it would be valuable to include men and women with ADHD who have been diagnosed in childhood and in adulthood.
Conclusion
Students with ADHD showed impairment in health and dietary habits, with women with ADHD reporting even worse health compared with men with ADHD. Achievement motivation differed between students with and without ADHD and might indicate compensatory mechanisms in the population of college students with ADHD. The effect of gender on obsessive-compulsive behavior and compensatory effort was fully mediated by the timing of the diagnosis. It seems important to prevent under diagnosis in girls with ADHD, to further explore that individuals with ADHD use compensation strategies, and which of these strategies are adaptive and which are maladaptive. Results could be used to develop effective interventions for adults with ADHD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.