
Abstract
Keywords
Introduction
A growing consensus holds that ADHD is a developmental disorder, associated with impaired executive function (EF; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). EF can be understood as an umbrella term that incorporates a collection of higher-order cognitive functions such as inhibition, working memory, and cognitive flexibility (Miyake et al., 2000). Recent studies suggest that up to 50% of children and adolescents with ADHD perform within the normal range on EF tests (Egeland, 2010; Nigg, Willcutt, Doyle, & Sonuga-Barke, 2005). As proposed by Sonuga-Barke (2005), EF impairments more often appear in complex everyday situations where affective and motivational processes interact with EF processes (hot EF; Sonuga-Barke, 2005). These hot EF processes have been shown to activate areas of the brain that control emotions and the brain’s reward systems (e.g., orbito–frontal cortex, ventral striatum, and the limbic system). In contrast, traditional EF tests with less pronounced emotional salience (cold EF) activate the dorsolateral parts of the prefrontal cortex (Castellanos, Sonuga-Barke, Milham, & Tannock, 2006). Deficits in hot and cold EF may constitute independent routes to ADHD symptoms (Sonuga-Barke, 2005) and may have different developmental outcomes (Anderson, 2002; Smith, Xiao, & Bechara, 2012). Several studies have examined the longitudinal course of cold EF in boys and girls with ADHD (Seidman, 2006). By comparison, longitudinal studies of hot EF in boys and girls with ADHD have been largely absent. Thus, in the present study we wanted to investigate the longitudinal course and the impact of gender on hot and cold executive processes in children and adolescents with ADHD over 2 years.
One of the challenges for research on EF in children and adolescents is that these skills develop and change rapidly throughout childhood in typically developing (TD) children (Anderson, 2002; Best & Miller, 2010). Furthermore, it appears that various EF components demonstrate different developmental trajectories: age-related improvements seem to emerge later and more gradually for hot EF components than for cold EF components (Anderson, 2002; Prencipe et al., 2011; Smith et al., 2012). Despite improved cold EF performance through development in children with ADHD, these functions seem to remain significantly impaired also in adolescence and adulthood (Miyake & Friedman, 2012; Seidman, 2006).
On decision-making tasks, which is one way of investigating hot EF in a laboratory test situation, impairment has been found to be more evident in adolescents with ADHD than in children with ADHD (Geurts, van der Oord, & Crone, 2006; Hobson, Scott, & Rubia, 2011; Lambek et al., 2010; Skogli, Egeland, Andersen, Hovik, & Øie, 2013; Toplak, Jain, & Tannock, 2005). One reason for these findings may be that hot EF are relatively immature in young children (<12 years; Best & Miller, 2010). Thus, hot EF impairments in children with ADHD will be more pronounced in older children (>12 years). As hot decision-making performance improves with age in TD adolescents, adolescents with ADHD may remain impaired (Crone & van der Molen, 2004; Overman, 2004; Van Duijvenvoorde, Jansen, Bredman, & Huizenga, 2012). The outcome on decision-making tasks like the Iowa Gambling Task (IGT) and the Hungry Donkey Task (HDT) have been associated with emotionally based processes like anticipatory skin conductance and heart rate (Bechara, Tranel, Damasio, & Damasio, 1996; Crone & van der Molen, 2007). The development of these somatic markers during the task are interpreted as warning signals that gradually guide decision-making away from disadvantageous choices and toward advantageous choices (Bechara, Damasio, Tranel, & Damasio, 1997).
Growing evidence indicates that male and female brains develop and mature at different rates in TD children (Lenroot et al., 2007; Thompson et al., 2005). Magnetic resonance imaging studies have reported that frontal lobes involved in EF processes mature 1 to 3 years earlier in TD girls compared with TD boys (Giedd et al., 2009). However, when investigating the impact of gender on cold EF deficits with neuropsychological measures, previous studies have yielded more similarities than differences between males and females with ADHD in childhood and adolescence (Rucklidge, 2010; Seidman et al., 2005; Skogli, Teicher, Andersen, Hovik, & Oie, 2013). By comparison, a growing number of studies have reported sex-related differences in hot EF (decision-making), with males outperforming females in TD children and adults (see van den Bos, Homberg, & de Visser, 2013). van den Bos and colleagues (2013) reported that males in general focus on overall outcome on decision-making tests, while females to a greater extent focus on both win and loss frequencies as well as overall outcome. As a consequence, females are reported to be more risk averse and need more trials to reach the same level of performance as males (van den Bos et al., 2013). Few studies have investigated the impact of gender on decision-making in ADHD populations, but Miller, Sheridan, Cardoos, and Hinshaw (2013) found impaired decision-making performance in young adult females with ADHD compared with TD females. Despite the lack of between-sex comparisons in the study by Miller et al. (2013), results indicate that young adult females with ADHD exhibit impaired decision-making compared with male counterparts (Hobson et al., 2011; Toplak et al., 2005).
To the best of our knowledge, no studies have investigated both hot and cold EF longitudinally in children and adolescents with ADHD. Knowledge about the developmental course of hot and cold EF will be of importance for understanding the etiology of ADHD as well as intervention planning. The aim of the present study was to investigate the longitudinal course and impact of gender on hot and cold executive processes in children and adolescents with ADHD over 2 years. First, we hypothesized that children with ADHD would show improved cold EF performance across time, relative to baseline assessment. Second, we expected that cold EF would remain significantly impaired across time in the ADHD group relative to the TD group. Third, we expected to see improved hot EF performance across time in the TD, but not in the ADHD group, relative to baseline. Fourth, children and adolescents with ADHD were expected to show impaired hot EF performance relative to TD children. Finally, boys were expected to outperform girls on a decision-making test (hot EF) in both groups. As the level of co-existing symptoms and ADHD symptom dimensions are likely to change across time, this may blur findings regarding a true developmental effect in EF (Willcutt et al., 2012). Thus, associations between improved EF performance across time, and altered levels of ADHD symptom dimensions and co-existing problems were also explored.
Method
Procedure and Participants
Detailed recruitment strategy and diagnostic assessment are described in detail in separate publications (Hovik, Plessen, Skogli, Andersen, & Oie, 2013; Skogli, Egeland, et al., 2013) and only a short presentation will be given here. Demographic characteristics are presented in Table 1. The subjects were recruited as consecutive referrals for assessment of ADHD, from child and adolescent outpatient mental health centers in Norway. Diagnoses were considered positive, if, based on a comprehensive evaluation of Kiddie-Schedule for Affective Disorders and Schizophrenia (Kiddie-SADS), teacher information and rating scales Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria were met (ADHD Rating Scale IV [ARS-IV], DuPaul, Power, Anastoupolous, & Reid, 1998; Child Behavior Checklist [CBCL]). The participants were part of a larger research project investigating cognitive and emotional functioning in children and adolescents with neuropsychiatric disorders. The age span in this part of the project with focus on development has been restricted to 9 to 16 years instead of 8 to 17 to get larger age homogeneity.
Demographic Characteristics: Means and Standard Deviations by Group and Assessment Time.
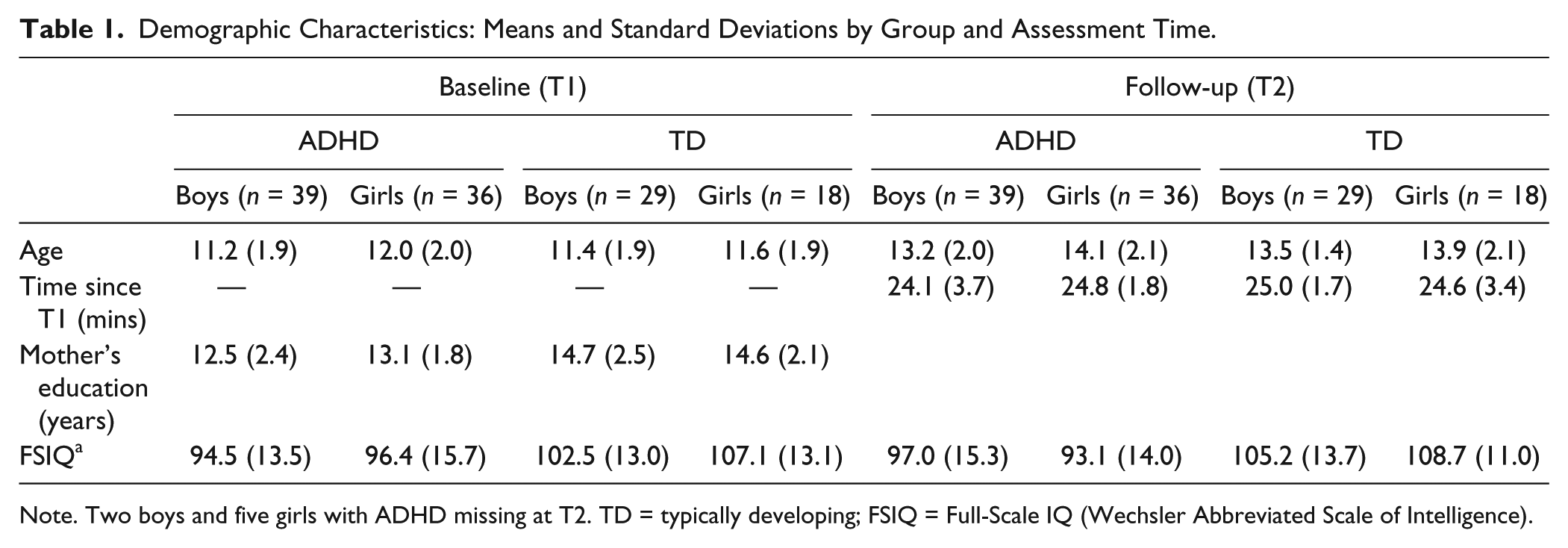
Note. Two boys and five girls with ADHD missing at T2. TD = typically developing; FSIQ = Full-Scale IQ (Wechsler Abbreviated Scale of Intelligence).
Exclusion criteria for all participants included prematurity (<36 weeks), IQ below 70, a history of stimulant treatment, or any disease affecting the central nervous system. All TD children were screened for mental disorders in separate Kiddie-SADS interviews for children/adolescents and parents. The TD children were recruited from local schools and were given a small compensation for participating. The TD children could not have been treated for a mental disorder, have a psychiatric diagnosis, have had a head injury (with loss of consciousness), or have known dyslexia. The study was approved by the Regional Committee for Medical Research Ethics in Eastern Norway (REK-Øst), and by the Privacy protection ombudsman for research at Innlandet Hospital Trust. The study was conducted in accordance with the Helsinki Declaration of the World Medical Association Assembly.
At baseline (T1), 39 males with ADHD (M = 11.2 years), 36 females with ADHD (M = 12.0 years), 29 TD males (M = 11.4 years), and 18 TD females (M = 11.9 years) between 9 and 16 years were included in the study. The four groups (ADHD/males, ADHD/females, TD/males, TD/females) did not differ significantly with regard to age and gender distribution. The groups differed significantly with regard to IQ (The Wechsler Abbreviated Scale of Intelligence; Wechsler, 1999), F(3, 118) = 4.36, p = .006, η2 = .10. Bonferroni post hoc analyses showed that boys in the ADHD group scored below TD females. On average, mothers of children in the TD group had 1.8 years more education than mothers of children with ADHD, F(3, 118) = 7.01, p < 0.001. None of the participants were prescribed psychopharmaca at T1. One boy with ADHD was prescribed Zoloft 10 mg at T2.
Follow-up (T2) assessment was conducted approximately 24 months following baseline assessment. The same procedure was followed in both assessments. Seventy-five subjects with ADHD from the baseline sample of 78 were available for reassessment at T2 (96%). Three boys with ADHD refused to participate at T2. In four cases where the participants were unable to meet at the clinic for reassessment, telephone interviews were performed with the parents/caregivers. Of the 75 subjects with ADHD available for reassessment at T2, 2 boys and 2 girls were symptom-free and received no diagnosis at T2. Due to fatigue or refusal to perform some of the tests, a complete neuropsychological re-assessment was not possible in all cases. In one case, computer failure precluded full data collection (i.e., the HDT).
After inclusion at T1, participants in the ADHD group received standard psychological and/or medical treatment for ADHD-related problems. At T2, a majority of the participants with ADHD had completed their clinical treatment, and were no longer patients at the Innlandet Hospital Trust. The participants receiving stimulant medication at T2 (n = 42; Equasym, Concerta, and Ritalin) were tested after medication was discontinued for at least 24 hr before re-assessment. One female participant forgot to discontinue stimulant medication prior to testing at T2. There were no significant differences in age and IQ (p > .05) between the children with ADHD available for re-assessment and those three lost to follow-up. All TD children were available for reassessment at T2 (n = 47), and none of the participants (ADHD and TD) were excluded at T2 due to neurological or somatic illness known to influence neurocognitive function. Participants with ADHD and TD children did not differ significantly with regard to age and gender distribution at T2 (p < .05).
Measures
Cold EF tests
Miyake and colleagues (2000) suggest that working memory, inhibition, and cognitive flexibility are three central aspects of EF. Based on this, we decided to assess cold EF with the Letter–Number Sequencing Test (LN) measuring working memory (Wechsler, 2004), the Colour–Word Interference Test, condition 3 (CW 3) measuring inhibition (Delis, Kaplan, & Kramer, 2001), and the Trail Making Test, Condition 4 (TMT 4) measuring cognitive flexibility (Delis et al., 2001). These three cold EF tests have demonstrated good psychometric properties, and reflect reasonably well the three EF aspects outlined by Miyake and Friedman. See Skogli, Egeland, et al. (2013) for additional descriptions of EF measures.
Working memory: The LN Sequencing Test (a subtest from the Wechsler Intelligence Scale for Children - Fourth Edition; Wechsler, 2004). Total correct recalled trials were examined. Lower raw scores indicated difficulties with the task. Improvement on the LN test between T1 and T2 was calculated by subtracting raw scores at T2 from T1.
Inhibition: The CW3 Interference Test (Delis et al., 2001; Stroop, 1935). Completion time in seconds was examined. Higher raw scores indicated difficulties with the task. Improvement on the CW 3 test between T1 and T2 was calculated by subtracting raw scores at T2 from T1.
Cognitive flexibility: The TMT 4 (Delis et al., 2001). Time to complete task was examined. Higher raw scores indicated difficulties with the task. Improvement on the TMT 4 test between T1 and T2 was calculated by subtracting raw scores at T2 from T1.
Hot EF test
The computer-based HDT (Crone & van der Molen, 2004) is a children’s version of the IGT (Bechara, Damasio, Damasio, & Anderson, 1994). The children were asked to help a donkey collect as many apples as possible by choosing one of four doors (A, B, C, and D). The amount of wins and losses varied between choices, and overall gains/losses were displayed with a red/green bar at the bottom of the screen. Doors A and B represented disadvantageous choices (resulting in overall loss), and doors C and D represented advantageous choices (resulting in overall gain). The task ended after completion of 150 trials. Net difference scores were calculated by subtracting the amount of disadvantageous choices (A + B) from the number of advantageous choices (C + D; for example, Bechara et al., 1994). Higher net scores indicated better performance on the task. Improvement on the HDT between T1 and T2 was calculated by subtracting net difference scores at T2 from T1. In early phases of decision-making tasks, risk parameters are uncertain. The decision-making process can thus be considered first as decision-making under ambiguity and later as decision-making under risk (Brand, Recknor, Grabenhorst, & Bechara, 2007). Consequently, internal consistency was calculated for odd and even blocks on the HDT (net scores calculated for 10 blocks of 15 trials). Pearson correlation between odd and even blocks revealed adequate internal consistency at T1 (.690) and T2 (.628) on the task in our sample. The change from card gambling into a pro-social game where participants are invited to assist a hungry donkey to win as many apples as possible is considered to be more meaningful for children by stirring their involvement—“you cannot let a hungry donkey down” (Crone & van der Molen, 2004, p. 254). Thus, although the basic format of the IGT is retained, the HDT is considered to be a more appropriate decision-making task in children (Crone & van der Molen, 2004). For a detailed account of the HDT, see Crone & van der Molen (2004).
Measures of symptomatology
The CBCL (Achenbach & Rescorla, 2001) was completed by one or both parents. The CBCL is a widely used scale containing 120 items that provide information on several subscales regarding child/adolescent psychopathology. Internalizing and externalizing symptom scales were used in the current study. Elevated T-scores indicate a higher degree of co-existing internalizing and externalizing problems. Acceptable reliability and validity of the Norwegian version of the CBCL are reported by Nøvik (1999, 2000). Symptom change from T1 to T2 was calculated by subtracting CBCL scores at T2 from T1.
The ARS-IV (DuPaul et al., 1998) was completed by the parents. The ARS-IV is an 18-item scale, with each item corresponding to one of the 18 DSM-IV-TR diagnostic criteria. Inattention symptoms are designated as odd-numbered items and hyperactivity/impulsivity symptoms are displayed as even-numbered items. Elevated scores indicate a higher degree of ADHD-related problems. Symptom change from T1 to T2 was calculated by subtracting ARS-IV scores at T2 from T1.
Data Analyses
Data analyses were conducted using the statistical package SPSS for Windows, version 19.0 (IBM, SPSS, Inc., Chicago, IL). Demographic characteristics were investigated using the chi-square test for independence (nominal variables) and one-way analysis of variance (ANOVA; continuous variables) followed up by Bonferroni post hoc test for group comparisons. Mixed between–within subjects ANOVAs (mixed ANOVA) were conducted for each dependent variable to estimate the effect of group and gender on EF performance across time. Because of multiple comparisons, Bonferroni-Holm corrections were used to control for chance findings by reducing the global alpha level (α = .05) proportionately to the number of comparisons being performed (Holm, 1979). To control for the possible confounding effect of IQ, mixed ANOVAs for all dependent measures with IQ as a covariate were conducted. All significant hot and cold EF test results were re-analyzed without the one participant taking stimulant medication prior to testing at T2. Correlation analyses (Pearson) were used to investigate associations between improvement in EF performance between T1 and T2, and the amount of change in co-existing problems and ADHD symptomatology. Missing data are specified in the Notes in Tables 1, 2, and 3, and Figure 1.
Executive Function Tests (Raw-Scores): Means and Standard Deviations by Group and Assessment Time, and Results From Mixed ANOVAs.
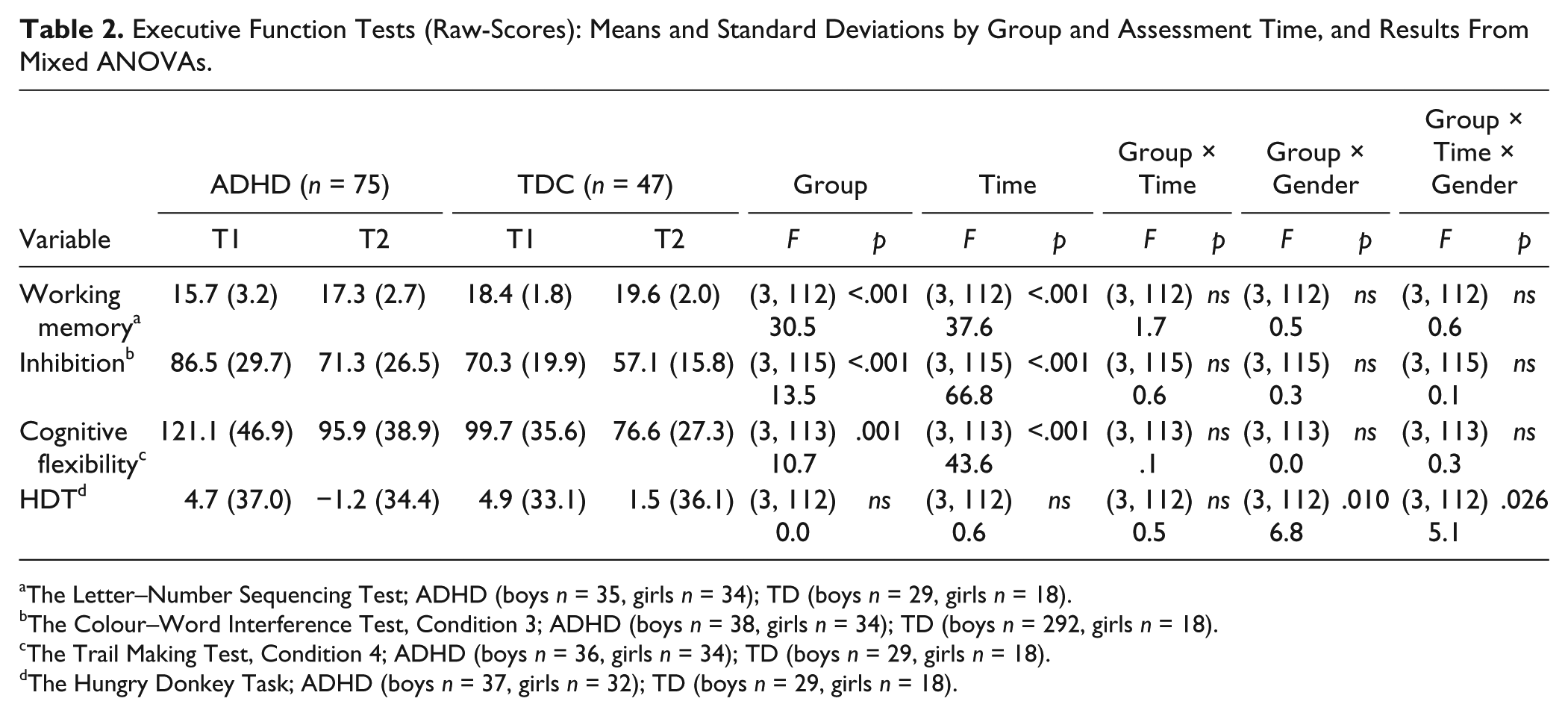
The Letter–Number Sequencing Test; ADHD (boys n = 35, girls n = 34); TD (boys n = 29, girls n = 18).
The Colour–Word Interference Test, Condition 3; ADHD (boys n = 38, girls n = 34); TD (boys n = 292, girls n = 18).
The Trail Making Test, Condition 4; ADHD (boys n = 36, girls n = 34); TD (boys n = 29, girls n = 18).
The Hungry Donkey Task; ADHD (boys n = 37, girls n = 32); TD (boys n = 29, girls n = 18).
Symptom Change: Means and Standard Deviations by Group and Assessment Time.
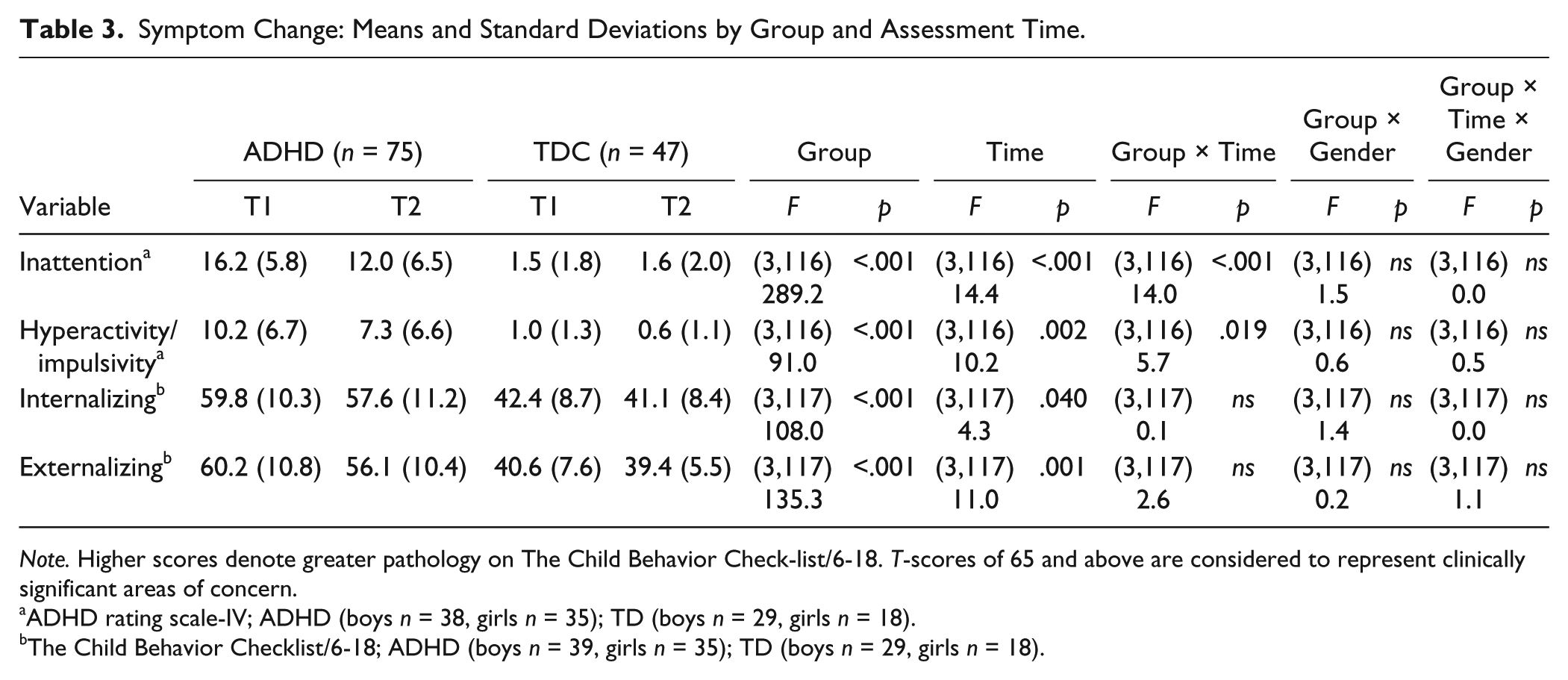
Note. Higher scores denote greater pathology on The Child Behavior Check-list/6-18. T-scores of 65 and above are considered to represent clinically significant areas of concern.
ADHD rating scale-IV; ADHD (boys n = 38, girls n = 35); TD (boys n = 29, girls n = 18).
The Child Behavior Checklist/6-18; ADHD (boys n = 39, girls n = 35); TD (boys n = 29, girls n = 18).
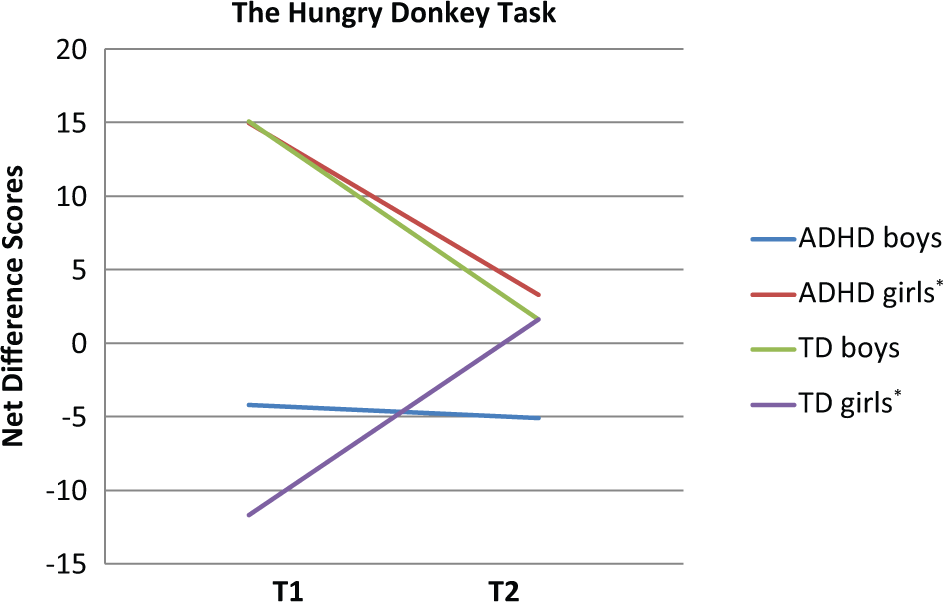
The Hungry Donkey Task: Net difference scores (advantageous choices–disadvantageous choices) at baseline (T1) and follow-up (T2).
Results
Cold Neuropsychological EF Tests
The results are shown in Table 2. There were no significant interaction effects of Group × Time nor Group × Time × Gender on working memory, cognitive flexibility, or inhibition. There was a main effect of time on working memory, F(3, 112) = 37.61, p < .01,
There were no significant interaction effects of Group × Gender on working memory, cognitive flexibility, or inhibition. There was a main effect of group on working memory, F(3, 112) = 30.49, p < .01,
Hot Decision-Making EF Test
There was one significant interaction effect of Time × Group × Gender, F(3, 112) = 5.06, p = .026,
Measures of Symptomatology
The results are shown in Table 3. Significant Group × Time interactions for ARS-IV inattention symptoms, F(1, 116) = 13.93, p < .001,
Associations Between Symptom Change and EF
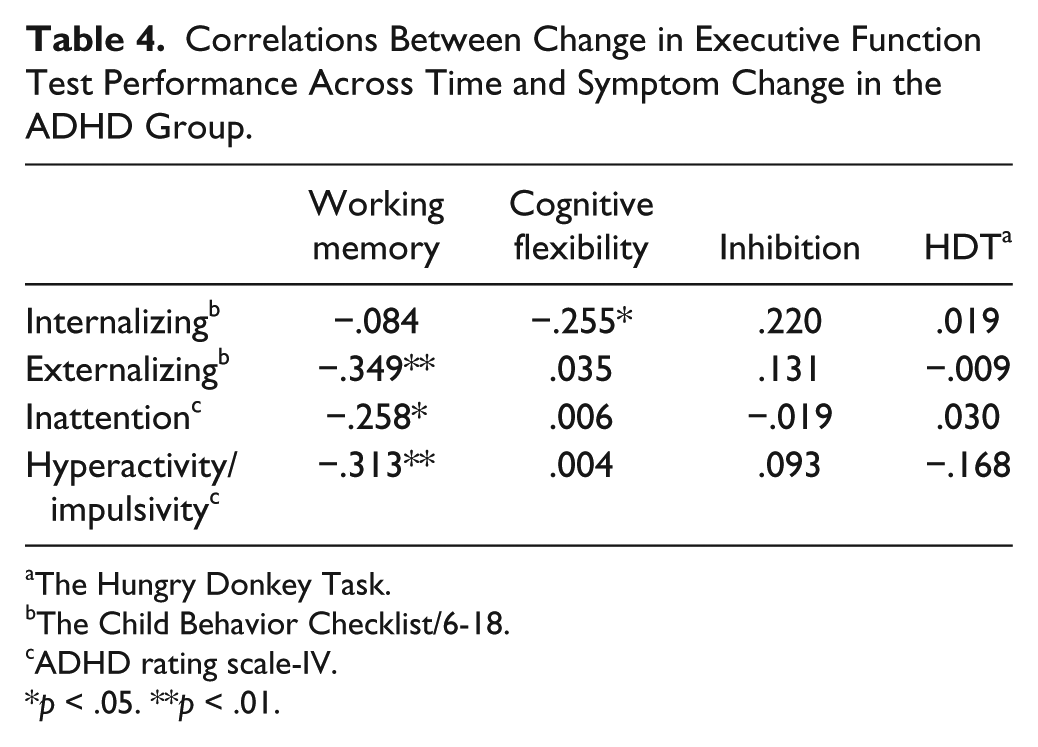
Correlations between symptom change across time and improvement on EF measures between T1 and T2 are reported in Table 4. Improved outcome on the working memory task showed significant correlations with a decline in CBCL externalizing symptoms (r = .35, p < .01), ARS-IV inattention symptoms (r = .26, p < .05), and ARS-IV hyperactivity/impulsivity symptoms (r = .31, p < .05) in the ADHD group. Improved outcome on cognitive flexibility showed a significant correlation with a decline in CBCL internalizing symptoms (r = .26, p < .05). Neither a decrease in CBCL internalizing or CBCL externalizing symptoms, nor a decline in ADHD symptomatology (ARS-IV) correlated with improvement in any other EF measure. When correcting for multiple comparisons with the Bonferroni–Holm procedure, none of the correlations remained significant.
Correlations Between Change in Executive Function Test Performance Across Time and Symptom Change in the ADHD Group.
The Hungry Donkey Task.
The Child Behavior Checklist/6-18.
ADHD rating scale-IV.
p < .05. **p < .01.
Discussion
As expected, we found that both children with ADHD and TD children improved performance on cold EF tests across time. Despite 2 years of maturation, treatment, and significant improvement regarding parent-rated symptoms, children and adolescents with ADHD remained impaired on all cold EF tests relative to the TD group. Our findings are consistent with previous studies reporting persistent impairment in cold EF in children and adolescents with ADHD despite considerable maturation in childhood (Seidman, 2006). In our sample, we observed a decline in parent-rated co-existing internalizing and externalizing problems across time. This decline in co-existing symptoms may be due to the benefits of psychological and/or medical treatment. In particular, the beneficial effect of stimulant medication on behavioral problems in children and adolescents with ADHD is well documented (Abikoff et al., 2004; Van der Oord, Prins, Oosterlaan, & Emmelkamp, 2008). However, it is interesting to note that cold EF impairments seem to persist, despite a decline in co-existing symptoms. Even though a relationship between improved cold EF and a reduction in co-existing symptoms was revealed, most correlations were non-significant. Furthermore, the correlations were small to medium and did not withstand corrections for multiple comparisons. Thus, enduring cold EF impairments despite a decline in symptomatology across time may indicate that these dysfunctions are mainly trait-dependent rather than state-dependent phenotypes in children and adolescents with ADHD (Biederman et al., 2009).
We also observed a decline in ARS-IV ratings of inattention and hyperactivity/impulsivity problems across time in children with ADHD. An association between a decline in ADHD symptomatology and improved cold EF outcome were only found for the working memory measure. Even though previous studies have reported that inattention symptoms are more closely related to EF than hyperactivity/impulsivity symptoms, the two ADHD symptom dimensions did not have differential roles for cold EF outcome in our sample (Sonuga-Barke, 2005; Willcutt et al., 2012). Based on the findings by Willcutt and colleagues (2012) reporting greater decline in hyperactive/impulsive symptoms than inattention symptoms across development, one potential explanation is that cold EF and hyperactive/impulsive symptoms will be less closely related later in development when hyperactive/impulsive symptoms are less salient.
Consistent with previous findings, we did not find support for any effect of gender on impairment or development of cold EF (Rucklidge, 2010; Seidman et al., 2005).
As expected, children and adolescents with ADHD did not improve on hot EF performance (decision-making) across time. Surprisingly, hot decision-making performance did not improve across time in the TD group either. These results support previous findings that hot and cold EF seem to mature at different rates in TD children (Crone & van der Molen, 2004; Prencipe et al., 2011) as well as in children with ADHD (da Mata et al., 2011). Contrary to our expectations, there were no between-group differences on the hot decision-making task across time. No between-group differences on hot decision-making performance have previously been reported in TD children and children with ADHD (10-12 years; Geurts et al., 2006; Lambek et al., 2010; Masunami, Okazaki, & Maekawa, 2009; Skogli, Egeland, et al., 2013). Toplak et al. (2005) found impaired decision-making in adolescents (15 years) with ADHD relative to TD adolescents. These data may support the possibility that between-group differences may become more apparent in adolescents than in children.
Our data did not provide evidence of superior hot decision-making performance across time in boys compared with girls as hypothesized. However, partial support for one effect of gender on the hot decision-making task is supported by significant Group × Gender interactions. Interestingly, females in the ADHD group displayed deteriorating decision-making performance across time, while females in the TD group displayed improved decision-making performance across time. When females with ADHD displayed superior mean scores at T1 relative to females in the TD group, it is notable that HDT (hot EF) results are comparable at T2. It is well documented that TD boys outperform TD girls on decision-making tasks (Crone, Bunge, Latenstein, & van der Molen, 2005; Garon & Moore, 2007; Overman, 2004). Thus, our results with ADHD girls outperforming TD girls at T1 could be caused by a similar effect where girls with ADHD follow decision-making strategies comparable with TD boys. Similar to TD boys, girls with ADHD may focus on overall gain. In contrast, TD girls may to a greater extent focus on both win and loss frequencies as well as overall gain. The more detailed-oriented decision-making strategy may cause TD girls to need more trials to reach the same level of performance as girls with ADHD. Decreasing decision-making performance in girls with ADHD may indicate a developmental delay, or even a regression in hot EF processes as previously reported by Anderson (2002) and Smith and colleagues (2012).
When investigating decision-making with the IGT in TD children and adolescents from 8 to 17 years, Smith et al. (2012) found a curvilinear effect of age. The youngest participants failed to develop a preference for any of the doors, but outperformed the more reward-driven participants in early adolescence (10-13 years). Decision-making improved again from 14 years and peaked at the age of 17. Thus, a potential interpretation in line with the findings reported by Smith and colleagues may be that girls with ADHD outperformed TD girls at T1 because they were less cognitively developed, and, as such, less sensitive to the high reward doors (causing overall loss). With increasing age, however, decision-making performance declines in girls with ADHD as activation in the nucleus accumbens reward system increases, and they become more sensitive to the large payoffs on the hot EF task (Ernst et al., 2005; Galvan et al., 2006). Although not significant, it is interesting to note that performance was deteriorating from T1 to T2 in TD boys as well. These results indicating a similar decline in performance between TD boys and girls with ADHD may potentially be caused by comparable decision-making strategies in TD boys and girls with ADHD.
Another aspect likely to influence decision-making performance is co-morbidity. As hot decision-making tests appear to activate prefrontal processes distinct from cold EF, decision-making performance may have emotional and social, rather than cognitive, underpinnings. Depression and negative mood have been reported to have a negative impact on IGT performance in adult populations (Cella, Dymond, & Cooper, 2010; Suhr & Tsanadis, 2007). In contrast, Mueller, Nguyen, Ray, and Borkovec (2010) found better decision-making performance in groups with higher levels of anxiety. When examining decision-making in children with ADHD, Garon, Moore, and Waschbusch (2006) found that the group with higher levels of internalizing symptoms (anxiety and depression) performed better than children with ADHD and low levels of internalizing symptoms. Garon and colleagues speculated that co-existing internalizing symptoms in children and adolescents with ADHD could have a protective effect by causing a stronger response to loss on decision-making tasks. Likewise, elevated levels of internalizing symptoms in females with ADHD relative to TD girls in our sample (see Table 3) could have caused a similar protective effect in females with ADHD as described by Garon and colleagues.
A longitudinal design with few drop outs (4%) constitutes a major strength of this study. Longitudinal studies make it possible to observe developmental trajectories of different EF components, instead of drawing interpretations out of cross-sectional observations. An additional strength is the assessment of EF with a comprehensive test battery incorporating both hot and cold EF. The large age span (9-16 years at T1) might represent a limitation, but small standard deviations in age reflect the fact that most participants were around mean age at T1 (M = 11.5, SD = 2.0). Another potential limitation is that the sample was drawn from a clinical population, and represents those who are willing to seek help in a mental health clinic. Although we were able to control for the effect of stimulant treatment, we did not have the possibility to control for type and duration of psychological intervention between T1 and T2.
The development of hot EF in children and adolescents with ADHD is an understudied topic, and future longitudinal studies should take the distinction between implicit and explicit hot EF tasks into consideration. Whereas the so-called implicit hot EF tasks (i.e., IGT/HDT) to a greater extent reflect emotional and affective responses to the options of choice, the so-called explicit hot EF tasks (i.e., Cambridge Gambling Task) are more determined by cognitive and rational processes (Groen, Gaastra, Lewis-Evans, & Tucha, 2013). The use of implicit and explicit hot EF test measures may as a consequence reflect different cognitive skills potentially causing inconsistent findings. Furthermore, the developmental outcome of hot EF in the translation from childhood to adulthood, in subjects with ADHD is largely unexplored. In particular, the persistence in cold EF deficits may have implications for hot EF when subjects with ADHD are required to take more control over reward-seeking tendencies in adolescence and early adulthood.
Conclusion
Our findings show that cold EF impairments persist, despite a considerable improvement across time in boys and girls with ADHD. A decline in co-existing problems and ADHD symptomatology showed few associations with improved cold EF performance across time. Thus, enduring cold EF impairments in the ADHD group may reflect that this disability is a stable endophenotypic trait. Clearly, as EF deficits are strongly associated with poor behavioral, social, educational, and occupational outcomes in ADHD populations, impairment level needs to be considered also when ADHD symptoms are remitting (Barkley & Murphy, 2010; Biederman et al., 2004; Biederman et al., 2006). Deteriorating decision-making performance across time in girls with ADHD, but improved performance in TD girls, indicates divergent developmental trajectories of hot EF in girls with ADHD relative to TD counterparts. A possible clinical implication may be that interventions targeting positive reinforcement of desirable behavior may be more effective than strategies emphasizing the costs of undesirable behavior in adolescent females with ADHD.
Footnotes
Authors’ Note
Parts of this article were presented as a poster at the 4th World Congress on ADHD in Milan 6 to 9 June 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project has received financial support from Innlandet Hospital Trust (grant number 150186) and the Regional Resource Center for Autism, ADHD, Tourette syndrome and Narcolepsy, Oslo University Hospital (Grant 150182).