
Abstract
There has recently been increased interest in the study of sluggish cognitive tempo (SCT) in children and adults (see Becker, Marshall, & McBurnett, 2014). Characterized by problems with daydreaming, staring, mental fogginess, confusion, hypoactivity, sluggishness, lethargy, and drowsiness, recent research has converged in demonstrating SCT symptoms to be an important construct in psychology and psychiatry (see Barkley, 2014; Becker, 2013; Becker, Marshall, & McBurnett, 2014). Although some research suggests that SCT may be important for identifying individuals who show problems in attention but few or no symptoms of hyperactivity (Carlson & Mann, 2002; Marshall, Evans, Eiraldi, Becker, & Power, 2014; cf. Willcutt et al., 2014), it has more recently been suggested that SCT represents a disorder that is distinct from, but highly related to, ADHD (see Barkley, 2014). In line with the latter hypothesis, more than a dozen studies conducted with children (Becker, Luebbe, Fite, Stoppelbein, & Greening, 2014; Burns, Servera, Bernad, Carrillo, & Cardo, 2013; Lee, Burns, Snell, & McBurnett, 2014; McBurnett et al., 2014; Willcutt et al., 2014) and adults (Barkley, 2012; Becker, Langberg, Luebbe, Dvorsky, & Flannery, 2013) have shown SCT to be statistically distinct from symptoms of ADHD. As such, research has moved to examining external correlates of SCT, with a clear need for studies to also examine potential moderators and mediators of these associations.
SCT and Social Functioning
Multiple studies conducted with children and adolescents demonstrate SCT symptoms also to be associated with social impairment (Bauermeister, Barkley, Bauermeister, Martínez, & McBurnett, 2012; Becker, 2014; Becker & Langberg, 2013; Becker, Luebbe, et al., 2014; Burns et al., 2013; Lee et al., 2014; Marshall et al., 2014). For example, recent research indicates that 75% of school-aged children with high levels of SCT are rated by their teachers as functionally impaired in the peer domain, in contrast to only 8% of children with low levels of SCT (Becker, 2014). More specifically, Willcutt et al. (2014) found SCT symptoms to be significantly associated with social isolation and social withdrawal after controlling for symptoms of ADHD and other psychopathologies. However, despite the established link between SCT and youths’ social functioning, no studies have examined the association between SCT and social impairment in young adults.
SCT and Emotion Dysregulation
Far fewer studies have examined SCT in relation to emotion, but extant research suggests that SCT is associated with problems in emotional functioning or, specifically, difficulties with emotion regulation. Emotion regulation is a multidimensional construct involving (a) awareness, understanding, and acceptance of emotions; (b) an ability to engage in goal-directed behaviors—and also refrain from impulsive behaviors—when experiencing negative emotions; (c) use of conditionally appropriate strategies to modulate the intensity and/or duration of emotional responses; and (d) an ability to recognize negative emotions as part of pursuing meaningful activities in life (Gratz & Gunderson, 2006; Gratz & Roemer, 2004).
With these definitional considerations in mind, why might we hypothesize there to be an association between SCT and difficulties with emotion regulation? First, it is clear that SCT is significantly associated with internalizing symptoms of anxiety and depression (Bauermeister et al., 2012; Becker & Langberg, 2013; Becker, Langberg, et al., 2014; Becker, Luebbe, et al., 2014; Penny, Waschbusch, Klein, Corkum, & Eskes, 2009; Willcutt et al., 2014), and it is well established that internalizing symptoms are themselves linked to problems with experienced emotions as well as cognitive and behavioral regulation of negative emotions (Erk et al., 2010; Gross, 2003; Gross & Muñoz, 1995; Mennin, Heimberg, Turk, & Fresco, 2005; Salters-Pedneault, Roemer, Tull, Rucker, & Mennin, 2006). As emerging work suggests that SCT may be more closely aligned with overarching internalizing versus externalizing psychopathology domains (Becker,et al., 2013), it is reasonable to expect SCT to likewise be associated with emotion regulation difficulties.
Individuals with ADHD often experience emotion dysregulation as well. For example, Sjöwall, Roth, Lindqvist, and Thorell (2012) identified deficits in emotional functioning (e.g., parent-reported ability to calm the self when feeling anger, sadness, or fear; errors in recognition of emotions expressed on pictures of faces) as an important component for distinguishing between children diagnosed with ADHD and children without ADHD. Surman et al. (2012) found that 55% of adults with ADHD reported extreme deficiency of emotional self-regulation as measured by self-reported over-reactivity to negative emotions. Furthermore, such deficits were rated as more severe than 95% of the control participants without ADHD. Given the strong association between SCT and ADHD (co-occurring among both children and adults in approximately 50% of cases of each; Barkley, 2012, 2013), it is reasonable to also expect SCT to be associated with problems in emotional functioning.
Finally, there is some direct evidence suggestive of a link between SCT and emotion dysregulation. In a nationally representative sample of adults, Barkley (2012) found that SCT symptoms, ADHD-inattention symptoms, and ADHD-hyperactive-impulsive symptoms each contributed unique variance in predicting adults’ self-ratings of deficits in the self-regulation of emotion (i.e., over-reacting emotionally to environmental cues). However, SCT explained far more variance in predicting emotion self-regulation deficits (44.5% of the variance) than either ADHD-inattention or ADHD-hyperactivity-impulsivity (1.4% and 7.7%, respectively). Similarly, Jiménez, Ballabriga, Martin, Arrufat, and Giacobo (2015) found SCT to be significantly associated with poorer emotional control in a sample of youth with ADHD, even after controlling for both ADHD-inattention and ADHD-hyperactivity-impulsivity. However, neither of these studies considered (or controlled for) internalizing symptoms, which, as described above, are themselves consistently and strongly associated with emotion dysregulation.
Emotion Dysregulation as a Mediator of the Association Between SCT and Social Impairment
Emotion regulation supports positive social functioning and development (Cole, Michel, & Teti, 1994), and, in turn, emotion dysregulation is associated with social impairment in childhood (e.g., Denham et al., 2003; Eisenberg, Fabes, Guthrie, & Reiser, 2000). As emotion dysregulation is characterized by difficulties in perceiving, experiencing, and expressing emotions, it is not surprising that such difficulties would interfere with adaptive functions such as communication in close relationships and successful problem solving (Cole et al., 1994; Keenan, 2000).
In comparison with research conducted with children and adolescents, fewer studies have examined emotion dysregulation (broadly construed) and social impairment in adulthood. Nonetheless, extant studies demonstrate an association between emotion regulation and college students’ social adjustment. For example, research conducted with college students demonstrates that greater ability in managing emotions (as assessed by a vignette measure in which participants identify the most adaptive way to regulate their feelings in a given context) is positively related to quality of social interactions with friends and individuals of the opposite sex (Lopes et al., 2004). Using the same methodology as the study just reviewed, emotion regulation abilities have also been positively associated with both self-reports and peer nominations of interpersonal sensitivity and prosocial tendencies in college students (Lopes, Salovey, Beers, & Côté, 2005). Thus, as expected, emotion regulation is linked to college students’ overall social adjustment.
Although previous research offers strong support for hypothesizing SCT to be related to social impairment, mechanisms of this association have yet to be uncovered. As SCT appears to be associated with emotion regulation (Barkley, 2012; Jiménez et al., 2015) and emotion regulation difficulties are also associated with social impairment (Cole et al., 1994; Denham et al., 2003; Eisenberg et al., 2000), it is plausible to hypothesize that the link between SCT and social impairment may be, at least in part, due to difficulties in the self-regulation of emotion. Willcutt et al. (2014) found SCT to be uniquely associated with increased social isolation and withdrawal in a large sample of children with and without ADHD. In discussing this finding, they speculated that “individuals with SCT may become overwhelmed by the rapid flow of complex information that must be processed continuously to successfully navigate social interactions, which may then lead to avoidance of social situations and subsequent isolation” (Willcutt et al., 2014, pp. 32-33). In essence, Willcutt and colleagues proposed that regulation—including emotion regulation—is a potential reason for the link between SCT and social impairment, and we sought to directly test this hypothesis in the present study.
Study Hypotheses
In sum, the aims of the present study were to (a) examine SCT in relation to college students’ social functioning as a way to replicate previous research almost exclusively conducted with children and adolescents; (b) test if SCT is significantly associated with deficits in emotion regulation over and above both ADHD and internalizing symptoms; and (c) test the hypothesis that emotion dysregulation mediates the association between SCT symptoms and social impairment. Given the literature reviewed above, we expected SCT to be uniquely related both to poorer social functioning and to greater difficulties with emotion regulation over and above other forms of pathology. We consider our third aim to be an exploratory first step given that the data we present are cross-sectional. As the first study to directly test this hypothesis, however, such analyses seemed warranted, and we expected emotion dysregulation to partially account for the relation of SCT to poorer social functioning.
Method
Participants
Participants were 158 undergraduate students enrolled at a public university in the Midwestern United States. Participants were recruited from two sources: (a) introductory psychology courses (n = 132) and (b) a previous study of SCT and college student functioning that recruited students in an introductory psychology course during the prior semester (n = 26). Importantly, neither differences on demographic characteristics nor any study variable were found between these two groups (all ps > .05). In total, participants ranged in age from 18 to 23 years (M = 19.05, SD = 1.00) and approximately two thirds were female (64%, n = 101). The majority (84%) of participants self-identified as Caucasian; the remaining participants self-identified either as Asian/Asian American (7%), African American (5%), or Multiracial (3%). Most participants (n = 101) were in their first year of college; the remaining participants were in their second (n = 38), third (n = 13), fourth (n = 5), or sixth (n = 1) year of college.
Procedure
This study was approved by the university Institutional Review Board (IRB). Interested participants were given individual time-slots, and after providing informed consent, completed the study measures on a computer in a university laboratory. Participants enrolled in an introductory psychology course at the time of their participation in the study received course credit for their participation; participants recruited from the previous semester’s study received US$10 in compensation for their time.
Measures
SCT and ADHD symptoms
Symptoms of SCT and ADHD were assessed using the Barkley Adult ADHD Rating Scale–IV (BAARS-IV; Barkley, 2011a), an adult self-report measure that includes 18 items corresponding to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) symptoms of ADHD that have been updated in their wording to also reflect DSM-5 (5th ed.; APA, 2013) changes made to the ADHD symptom definitions. The BAARS-IV also includes nine symptoms of SCT (e.g., “I don’t seem to process information as quickly or as accurately as others,” “prone to daydreaming when I should be concentrating on something or working,” “spacey or ‘in a fog’”). Participants respond to each item using a 4-point scale (1 = not at all, 4 = very often). The four-factor structure of this measure consisting of separate SCT, inattention, hyperactivity, and impulsivity dimensions was established in a nationally representative sample of adults (Barkley, 2011a) and has been replicated in a large sample of college students (Becker, Langberg, et al., 2014). The subscales of the BAARS-IV demonstrate satisfactory internal consistency and test–retest reliability over a 2- to 3-week time period (Barkley, 2011a). Internal consistencies in the present study were as follows: SCT α = .88, ADHD-inattention α = .87, ADHD-hyperactivity α = .68, and ADHD-impulsivity α = .83.
Depressive symptoms
The Center for Epidemiologic Studies Depression Scale–Short Form (CES-D-S; Radloff, 1977) was used as a continuous measure of depressive symptoms. The CES-D-S is a shortened 10-item self-report version of the 20-item CES-D. Participants use a 4-point scale (0 = rarely or none of the time [less than 1 day], 3 = most or all of the time [5-7 days]) to indicate how frequently they experienced each item (e.g., “I felt that I could not shake off the blues even with the help from my friends or family”) in the past week. The shortened form has been widely accepted as a comparable tool to the CES-D, as it correlates highly with the longer version and demonstrates comparable accuracy to the CES-D in classifying participants with depressive symptoms (Zhang et al., 2012). In the present study, CES-D-S α = .80.
Anxious symptoms
The 7-item anxiety subscale of the Depression Anxiety Stress Scales–21 (DASS-21; Antony, Bieling, Cox, Enns, & Swinson, 1998; Lovibond & Lovibond, 1995) was used as a continuous measure of anxious symptoms. Like the CES-D-S, participants respond to each item (e.g., “I was aware of dryness in my mouth”) in reference to the past week using a 4-point scale (1 = did not apply to me at all, 4 = applied to me very much or most of the time). The DASS-21 and its subscales are widely accepted as being valid for use with college-aged participants and demonstrate high reliability (Antony et al., 1998; Sinclair et al., 2011). In the present study, anxiety α = .83.
Social impairment
The Behavior Assessment System for Children, 2nd edition, Self-Report of Personality–College Version (BASC-2-SRP-CV; Reynolds & Kamphaus, 2004) and the Barkley Functional Impairment Scale (BFIS; Barkley, 2011b) were used to measure participants’ social functioning. Two measures of social functioning were used because the BASC-2-SRP-CV measures one’s own perception of general social competence, whereas the BFIS is specific to functional impairment. The combination allowed for an examination of general perceptions of interpersonal adjustment as well as impairment within the social domain.
The BASC-2-SRP-CV is a multidimensional self-report survey of behavior and personality among college students. The nine-item Interpersonal Relations subscale was used in the present study. Items on this scale vary in format. First, participants responded to a single true/false item as either being generally true (coded as 2) or generally false (scored as 0) of themselves (i.e., “Other people don’t like me”). Participants then rated eight additional statements (e.g., “I feel that nobody likes me,” “people think that I am fun to be with”) on a 4-point scale (0 = never, 3 = always). After reverse-coding the negatively phrased items, a total score is computed as the sum of all items such that higher scores indicate better interpersonal functioning. Although a clinical T-score can be computed, the total raw score was used in the current study. The BASC-2-SRP-CV has shown to be a consistent and reliable measure, and has shown good test–retest reliability over a 5-week period (Nowinski, Furlong, Rahban, & Smith, 2008). In the present study, α = .87 for the Interpersonal Relations subscale.
The BFIS (Barkley, 2011b) is a 15-question self-report measure of functional impairment in 15 major domains of adult psychosocial functioning. Using a 10-point scale (0 = not at all, 9 = severe) as well as a “does not apply” option, participants rate how much difficulty they have functioning effectively in 15 major life activities (e.g., in your home life with your immediate family, in your work or occupation). The BFIS has previously demonstrated adequate validity, high internal consistency, and test–retest reliability over a 2- to 3-week interval (Barkley, 2011b). For the present study, a two-item composite of items pertaining to social interactions was computed such that higher scores indicated greater social impairment. Specifically, the two domains assessed included difficulty in functioning effectively: (a) in social interactions with strangers and acquaintances, and (b) in relationships with friends. A mean-item score was used for this composite (α = .85). One participant did not complete this measure and so analyses using this measure utilize a sample of 157 participants.
Emotion dysregulation
The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) was used to measure participants’ emotion dysregulation. The DERS is a 41-item multidimensional scale that consists of six subscales measuring difficulties in one’s awareness and understanding of emotions, acceptance of emotions, and the ability to engage in goal-directed behavior (and refrain from impulsive behavior) when experiencing negative emotions. Respondents rate each item on a 5-point scale (1 = almost never; 5 = almost always), with items coded so that higher scores indicate greater difficulties in emotion regulation. The DERS is a widely accepted scale and has shown high internal consistency and good test–retest reliability over a period ranging from 4 to 8 weeks (Gratz & Roemer, 2004). Given high correlations among subscales, and little theoretical work to suggest differential relations between constructs of interest and specific subscales on the DERS, the total DERS score (α = .94) was used for analyses.
Results
Preliminary Analyses Examining Participants With High SCT
For purposes of describing the sample, we examined the percentage of participants meeting Barkley’s (2012) two criteria for having elevated SCT: (a) endorsing ≥5 symptoms of SCT on the BAARS-IV (Barkley, 2011a) at clinically significant levels (i.e., a score of “3” or “4”) and (b) being impaired in at least one BFIS domain based on the nationally representative sample validating the BFIS (Barkley, 2011b). In the current sample (recall that the BFIS was completed by 157 participants), 36 participants (23%) met the SCT symptom level criterion and 50 participants (32%) met the impairment criterion. Nineteen participants (12%) met both criteria and were thus classified as having high SCT. Independent-samples t tests indicated that, after applying a Bonferonni correction for multiple comparisons (.05/7 = .007), high SCT participants had higher BAARS-IV inattention, BAARS-IV hyperactivity-impulsivity, CES-D depression, DASS-21 anxiety, DERS emotion dysregulation, and BFIS social impairment scores, as well as lower BASC Interpersonal Relations scores, than participants without elevated SCT (all ps ≤ .001).
Correlation Analyses
For all study variables, the absolute values of skewness and kurtosis were below 2.0. Variable means, standard deviations, and intercorrelations are displayed in Table 1. Correlations were examined to determine which independent variables (i.e., SCT, ADHD-inattentive, ADHD-hyperactivity, ADHD-impulsivity, anxiety, and depression) and demographic variables (i.e., sex, age, and race) were associated with the dependent variables of interest (i.e., social functioning, difficulties in emotion regulation) and thus retained for inclusion in the regression analyses.
Means, Standard Deviations, and Intercorrelations of Study Variables.
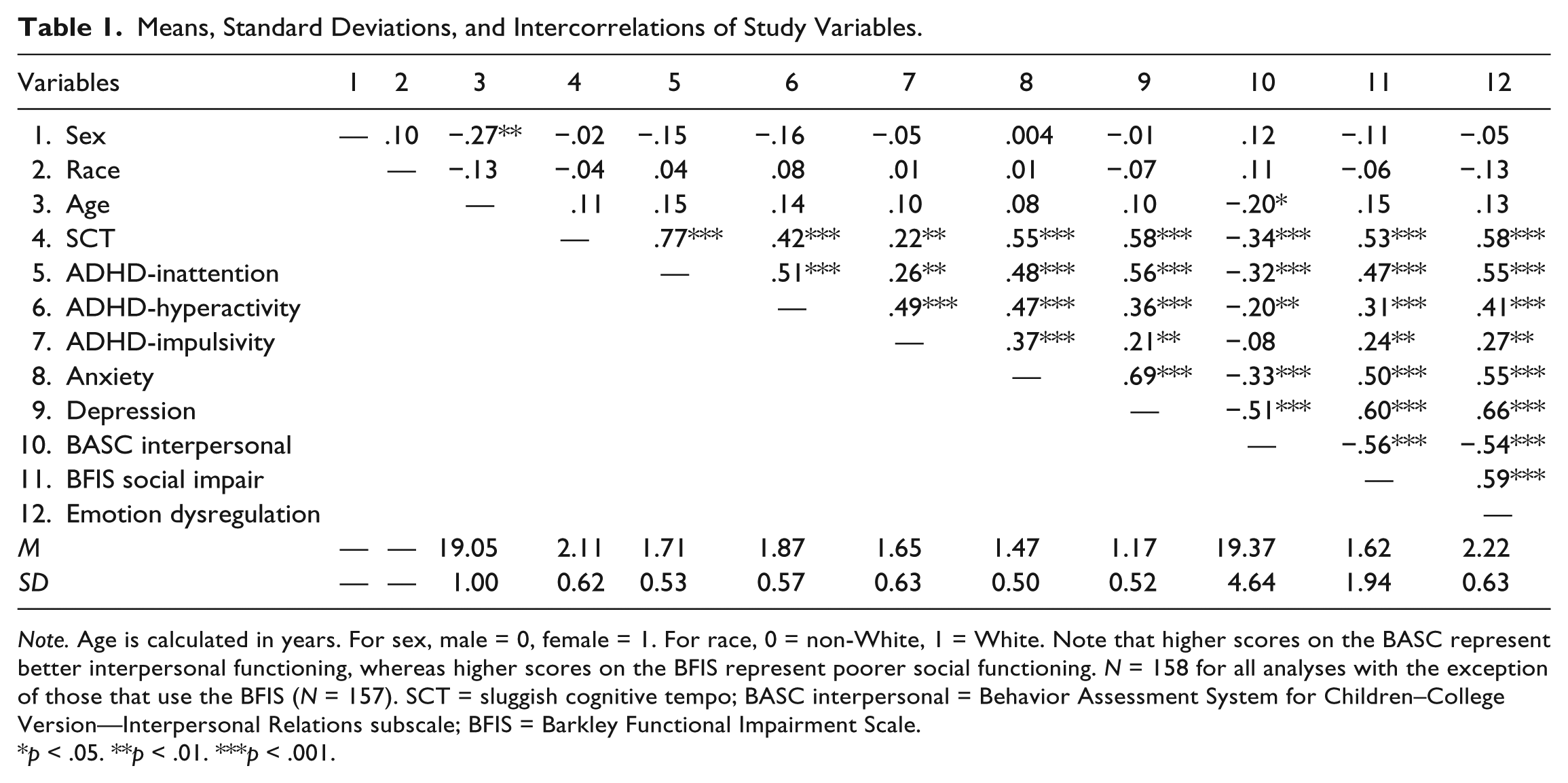
Note. Age is calculated in years. For sex, male = 0, female = 1. For race, 0 = non-White, 1 = White. Note that higher scores on the BASC represent better interpersonal functioning, whereas higher scores on the BFIS represent poorer social functioning. N = 158 for all analyses with the exception of those that use the BFIS (N = 157). SCT = sluggish cognitive tempo; BASC interpersonal = Behavior Assessment System for Children–College Version—Interpersonal Relations subscale; BFIS = Barkley Functional Impairment Scale.
p < .05. **p < .01. ***p < .001.
As displayed in Table 1, age was significantly negatively correlated with BASC Interpersonal Relations (r = −.20, p = .01) and so was included as a covariate in all subsequent models. In addition, each of the psychopathology dimensions (i.e., SCT, ADHD-inattention, ADHD-hyperactivity, ADHD-impulsivity, anxiety, and depression) was significantly associated with poorer social functioning as measured by both the BASC Interpersonal Relations and the BFIS Social Impairment variables, with the exception that anxious symptoms were not significantly correlated with the BASC Interpersonal Relations domain.
Likewise, each of the psychopathology dimensions was significantly positively associated with difficulties in emotion regulation, ranging from a correlation of .27 for the correlation between ADHD-impulsivity and emotion dysregulation to .66 for the correlation between depressive symptoms and emotion dysregulation. SCT, ADHD-inattention, and anxiety were also strongly associated with emotion dysregulation (rs = .55-.58, all ps = .001).
Regression Analyses
Next, hierarchical regression analyses were conducted to examine whether SCT symptoms were associated with difficulties in social functioning and emotion regulation after controlling for ADHD, anxious, and depressive symptoms. Across all regression analyses, no variance inflation factor (VIF) values were above 3 (values >10 are typically considered problematic) and no tolerance values were below .30 (values <.10 are typically considered problematic; Cohen, Cohen, West, & Aiken, 2002), suggesting that our regression models did not suffer from problems with multicollinearity. As displayed in Table 2 (top panel), age and depressive symptoms were significantly negatively associated with social functioning as measured by the BASC Interpersonal Relations domain. When SCT was added to the model in Step 2, it did not emerge as a significant predictor of social functioning as measured by the BASC. Contrasting results were found when examining social impairment as measured by the BFIS. As summarized in Table 2 (bottom panel), both ADHD-inattentive and depressive symptoms were significantly positively associated with greater social impairment as measured by the BFIS Social Impairment domain, but when SCT was added to the model in Step 2, the association between ADHD-inattention and social impairment was reduced to nonsignificance and SCT emerged as a significant positive predictor of participants’ social impairment.
Hierarchical Regression Models of Psychopathology Dimensions in Relation to Social Functioning.
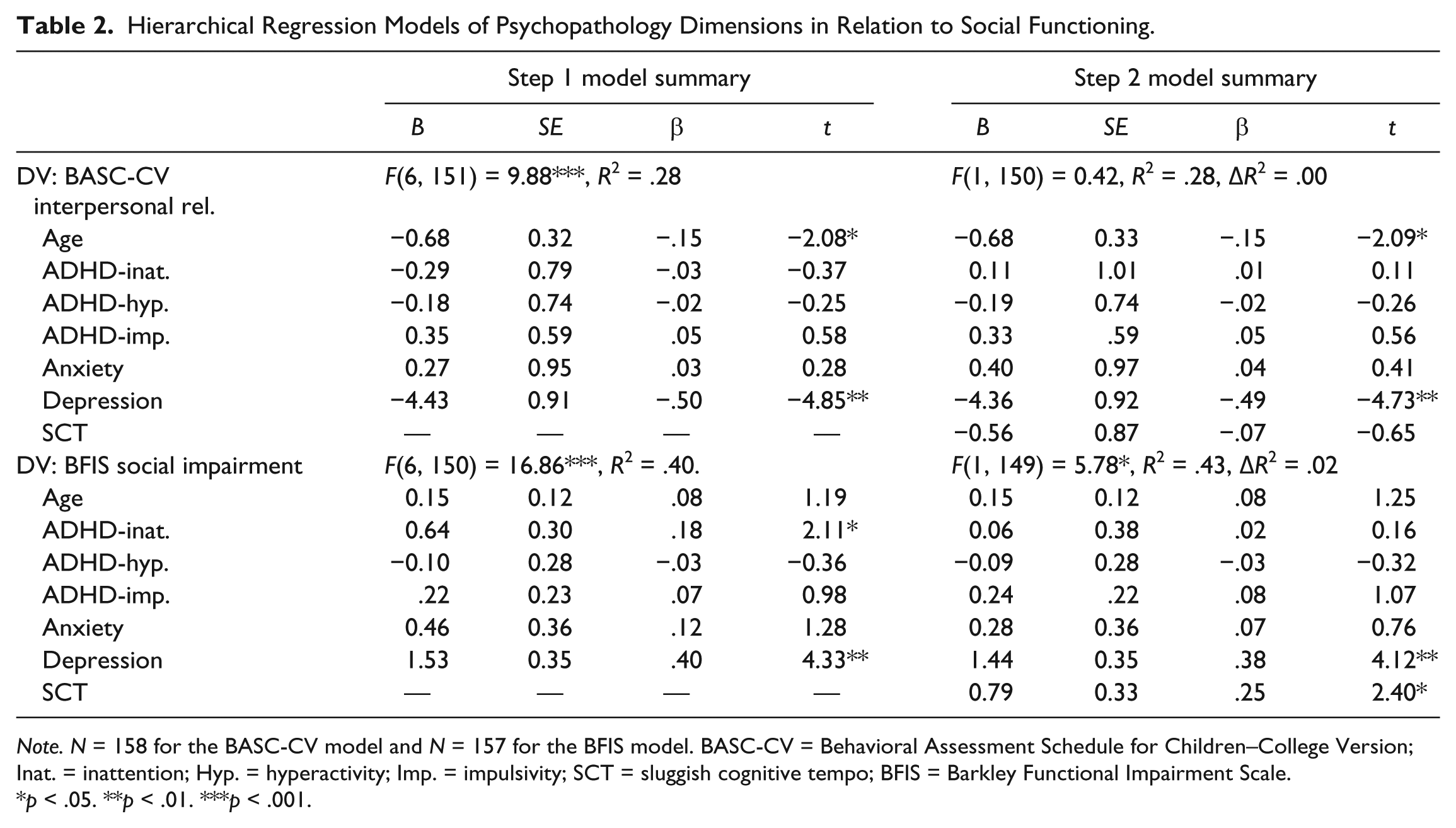
Note. N = 158 for the BASC-CV model and N = 157 for the BFIS model. BASC-CV = Behavioral Assessment Schedule for Children–College Version; Inat. = inattention; Hyp. = hyperactivity; Imp. = impulsivity; SCT = sluggish cognitive tempo; BFIS = Barkley Functional Impairment Scale.
p < .05. **p < .01. ***p < .001.
A similar model was conducted with emotion dysregulation as the outcome variable. As shown in Table 3, ADHD-inattentive and depressive symptoms were significantly positively associated with difficulties in emotion regulation in Step 1. However, when SCT was added to the model in Step 2, ADHD-inattention was no longer associated with emotion dysregulation and SCT was significantly positively associated with difficulties in emotion regulation. In sum, although SCT was no longer associated with social functioning as measured by the BASC Interpersonal Relations scale when other psychopathologies were included in the model, SCT remained significantly associated with both emotion dysregulation and social impairment after controlling for participants’ age and ADHD, depressive, and anxious symptomatology.
Hierarchical Regression Models of Psychopathology Dimensions in Relation to Emotion Dysregulation (N = 158).
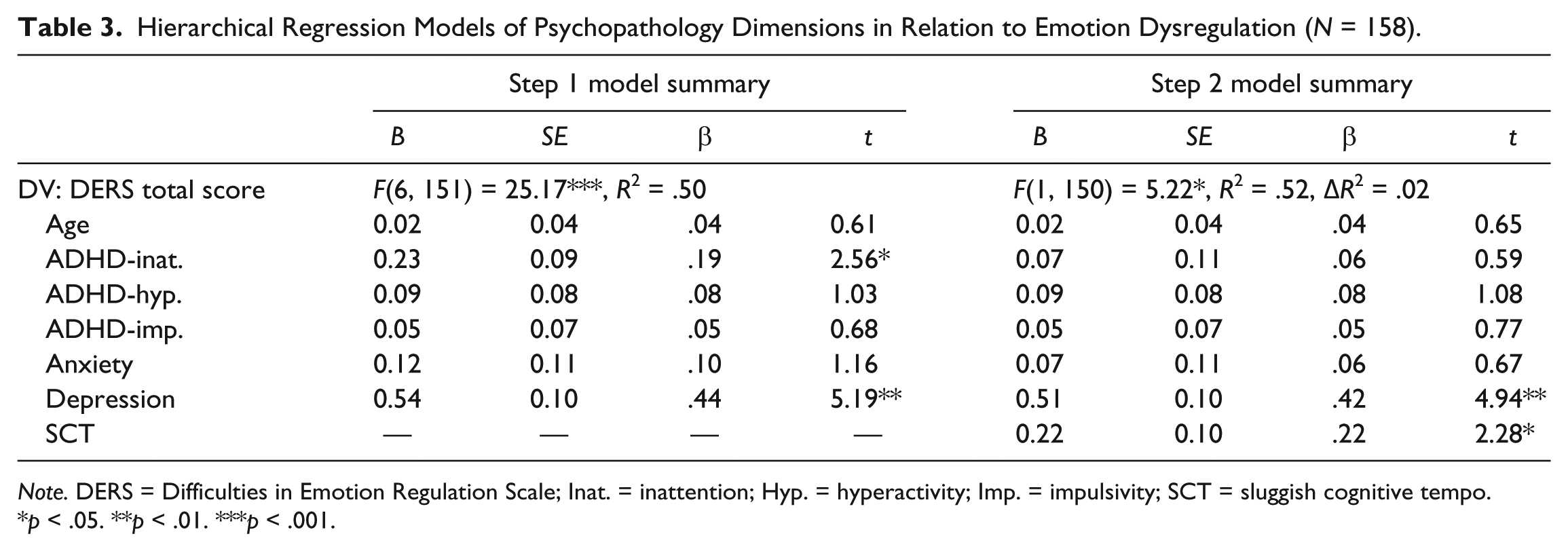
Note. DERS = Difficulties in Emotion Regulation Scale; Inat. = inattention; Hyp. = hyperactivity; Imp. = impulsivity; SCT = sluggish cognitive tempo.
p < .05. **p < .01. ***p < .001.
Mediation Analyses
The PROCESS macro (Hayes, 2013) was used to test whether SCT was indirectly (and uniquely) related to social functioning outcomes via its effect on emotion regulation difficulties. Unlike older recommendations for tests of mediation (Baron & Kenny, 1986), new guidelines suggest that indirect effects (denoted as ab below) may exist via a particular mediating variable even in the absence of a direct effect of an independent variable on a dependent variable (e.g., Preacher, Rucker, & Hayes, 2007). As such, the indirect effect of SCT on each social functioning variable was examined, despite the lack of a unique relation between SCT and the BASC Interpersonal Relations subscale in the initial regression analyses. Furthermore, bias-corrected bootstrapped estimates of the confidence intervals (CIs) for indirect effects were calculated (n = 10,000 replications) given that this approach does not assume normality of the distribution of sampled indirect effects like the Sobel test does (Preacher et al., 2007). For these analyses, 95% CIs are considered significant if they do not encapsulate 0. All analyses controlled for age, depression, anxiety, ADHD-inattention, ADHD-hyperactivity, and ADHD-impulsivity scores. For both social functioning variables, a significant indirect effect emerged from SCT via emotion regulation difficulties. Specifically, predicting BASC Interpersonal Relations scores, there was a significant indirect effect from SCT via DERS scores (SCT → DERS → BASC ab = −.63, SE = 0.34, 95% CI = [−1.48, −0.12]) over and above all covariates in the model. Likewise, predicting the three-item BFIS Social Impairment composite, there was a significant indirect effect from SCT via DERS scores (SCT → DERS → BFIS ab = .18, SE = 0.10, 95% CI = [0.03, 0.44]). Recall that higher BASC scores represent more adaptive functioning, whereas higher BFIS scores represent maladaptive functioning. Full models predicting BASC (top panel) and BFIS (bottom panel), including total and direct effects, are shown in Figure 1.
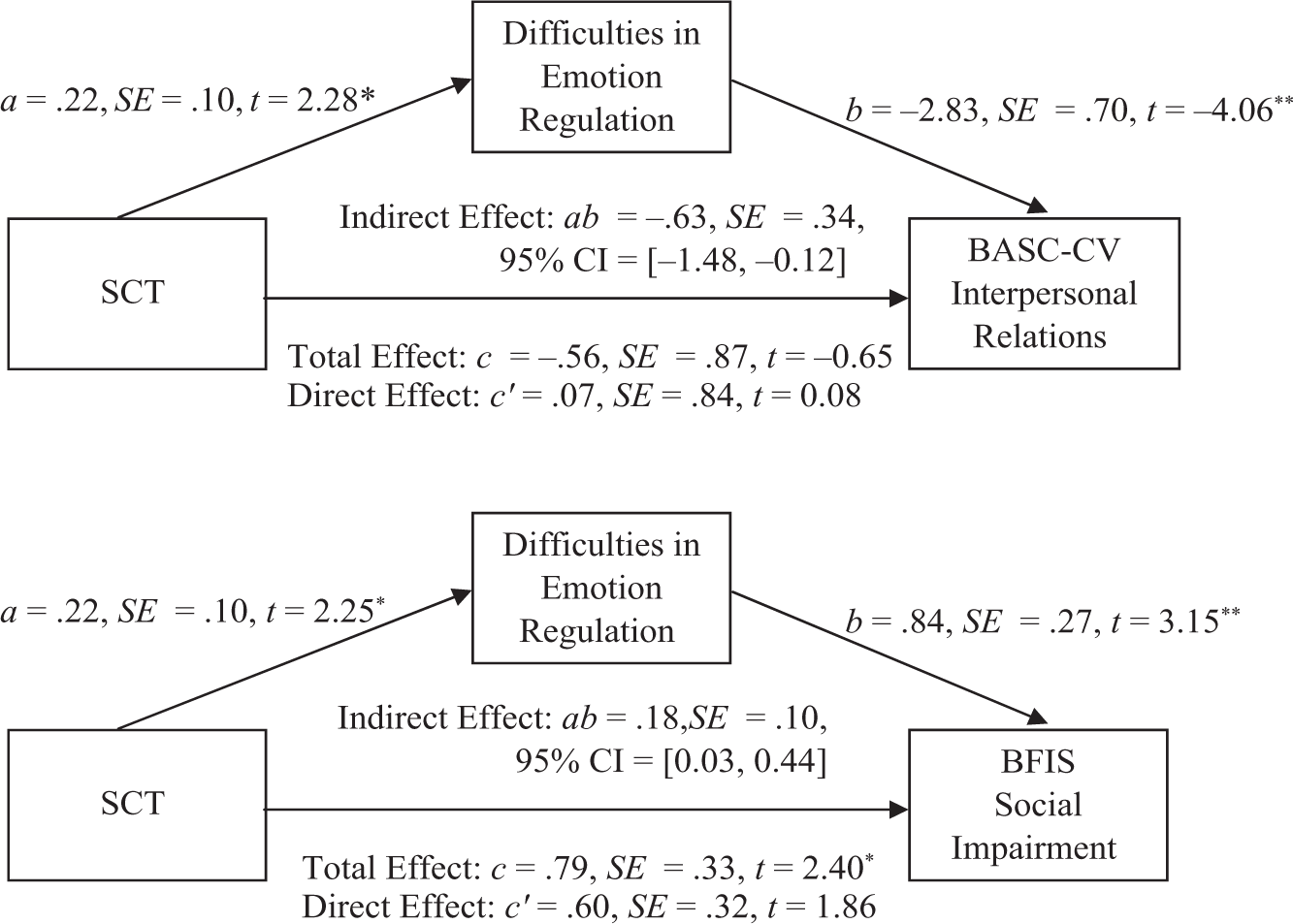
Indirect effects models of SCT predicting college student social functioning via difficulties in emotion regulation.
Discussion
The goals of the present study were to examine SCT’s unique relation to college students’ impairment in social functioning and difficulties with emotion regulation, and to test if emotion dysregulation might be the mechanism linking SCT symptoms to social impairment. The current investigation adds to extant research regarding both SCT and emotion regulation in important ways. First, we partially replicated the finding (primarily found in youth samples) that SCT is uniquely associated with social functioning. Second, the current study is the first to show that SCT is uniquely related to emotion regulation difficulties in young adults, over and above the effect of internalizing and ADHD symptoms. Finally, although emotion regulation had been proposed as a potential mechanism explaining the link between SCT and social impairment (Willcutt et al., 2014), the present study is the first to directly test this relationship, finding a significant indirect effect of SCT on social impairment via emotion dysregulation.
As hypothesized, SCT was related to social impairment in college students at the bivariate level. The present study provided mixed evidence, however, that SCT predicted social impairment over and above other psychopathology symptoms. Specifically, whereas SCT was uniquely related to social functioning impairment as measured by the BFIS, it was unrelated to the BASC Interpersonal Relations measure in the regression analyses. Why exactly these divergent results emerged is unclear, especially given extensive past work linking SCT uniquely to a host of social difficulties including poorer social skills and elevated social isolation, social withdrawal, and general social problems (Bauermeister et al., 2012; Becker, 2014; Becker & Langberg, 2013; Becker, Luebbe, et al., 2014; Burns et al., 2013; Lee et al., 2014; Willcutt et al., 2014). Differences in what these two measures of social impairment actually assess may help explain divergent findings. In particular, the BFIS measures perceived difficulties in social interactions with friends, acquaintances, and strangers. In contrast, the BASC has items that assess broader perceptions of social worth (e.g., “I am liked by others,” “people think I am fun to be with”). SCT symptoms like excessive daydreaming, staring, and mental fogginess may impair interpersonal skills more than perceptions of one’s own value in social situations.
Similarly, an alternate explanation for this mixed finding is that it reflects differences in relations between covariates and outcomes rather than SCT and outcomes. Unsurprisingly, depression was the strongest predictor of social impairment regardless of the outcome measure used. Given that feelings of worthlessness and low self-efficacy are extremely common features of depression (APA, 2013), and that the BASC taps perceptions of social worth, the strong relation between depression and BASC scores in our data may have obfuscated any relation between SCT and this particular measure of social impairment. Indeed, even in the model using the BFIS, it is important to acknowledge that SCT only contributed an additional 2% of the variance in outcomes over and above the significant effects of depression and ADHD-inattention. Regardless of the reason, our data do partially replicate the finding that SCT is uniquely related to social impairment in certain domains. Of note, ADHD-inattentive symptoms no longer predicted social impairment (as measured by the BFIS) once SCT was included in our model.
As a unique contribution to the literature, in the current study SCT was associated with difficulties in emotion regulation beyond symptoms of other forms of psychopathology. Expanding upon the research of Willcutt et al. (2014) and the speculation of several other authors (Barkley, 2012; Jiménez et al., 2015), our results explicitly demonstrated that SCT was associated with emotion dysregulation above and beyond symptoms of ADHD, anxiety, and depression. It is possible that individuals with SCT may be overwhelmed with the rapid influx of complex emotional information in a given context (e.g., Willcutt et al., 2014). As a result, these individuals may have trouble regulating their emotions in a situationally appropriate manner and also have trouble creating an awareness and understanding of their emotions.
Similar to social impairment, the amount of variance in emotion dysregulation explained in our full model by SCT was relatively small (~2%) owing in large part to the strong and expected association between depressive symptoms and emotion dysregulation (e.g., Joormann & Gotlib, 2010). Although most studies to date, including the current study, find considerable overlap between SCT and depression, the two are repeatedly found to be statistically distinct syndromes (Becker, Luebbe, et al., 2014; Lee et al., 2014; Willcutt et al., 2014). Our data provide further validity for considering SCT as a construct distinct from depression given the unique association found with an important outcome like emotion dysregulation. Furthermore, as occurred in one of our models with social impairment, when SCT was included in the model, the previously significant association between ADHD-inattentive symptoms and emotion dysregulation became nonsignificant. Taken together, these results point to the potential of SCT to emerge as a distinct and important syndrome with regard to the social and emotional functioning of young adults.
The final contribution of the current study was our test of emotion dysregulation as a potential mechanism explaining why individuals with high levels of SCT might experience difficulties in their social relationships. As hypothesized, there was a significant indirect effect from SCT to social impairment via greater difficulties in regulating emotions. Notably, this indirect effect emerged for both social impairment outcomes and while controlling for other forms of psychopathology and relevant demographics. As an aside, our use of modern techniques for mediation analyses (i.e., Hayes, 2013) allowed us to find an indirect effect from SCT to BASC Interpersonal Relations scores despite a lack of a significant direct effect in earlier regression analyses. Past recommendations for mediation (Baron & Kenny, 1986) would have suggested that mediation was not possible without evidence of the direct effect.
Although more often studied in youth populations (e.g., Cole et al., 1994; Denham et al., 2003; Eisenberg et al., 2000), the link between emotion regulation difficulties and impaired social relations has been demonstrated in college-aged populations (e.g., Lopes et al., 2004; Lopes et al., 2005). Our data suggest that high levels of SCT may affect an individual’s ability to regulate their negative emotions, which in turn leads to feelings of low social worth and difficulties in a broad array of relationships from those with friends to those with strangers. Other authors have proposed self-regulation as a potential mechanism explaining the oft-replicated link between SCT and social difficulties (Willcutt et al., 2014). We argue, and the current data support, that difficulties in the regulation of negative emotions in particular may be that piece of self-regulation disrupted in individuals with SCT and which have especially pernicious effects for social functioning. Indeed, the bivariate relations between emotion dysregulation and social functioning in the current study were some of the largest of all relations examined. Of course, these results should be interpreted cautiously given our cross-sectional data. It is equally plausible that if SCT is associated with social skills deficits that result in social isolation and withdrawal, this could in turn lead to a lack of understanding emotional cues in social situations or the adoption of maladaptive regulation strategies (e.g., avoidance of negative emotions). Clearly, longitudinal work is needed to unpack the exploratory mediation results presented herein. As a first step, however, the findings of significant indirect effects, unique to SCT over and above other forms of psychopathology, appear to warrant future investigation of the interplay of SCT, emotion regulation abilities, and social functioning in young adults.
Finally, descriptive statistics indicated that 12% of participants in the present study had elevated SCT based on Barkley’s (2012) criteria of endorsing five or more SCT symptoms as well as impairment in at least one domain of functioning. Although not the primary purpose of our study, it should be noted that this rate of 12% is more than twice as high as Barkley’s rate of 5.1% based on a nationally representative sample of adults aged 18 to 96. The reason for this discrepancy is not clear, but given that both the BAARS-IV (Barkley, 2011a) and BFIS (Barkley, 2011b) are newer measures and other studies have not examined how to best classify or “diagnose” elevated SCT, more research attention should be devoted to this area. In addition, our sample size was relatively small and drawn from a single university and is thus clearly not representative of adults or even college students broadly. As such, our rate of 12% should be viewed cautiously and considered preliminary in nature. In any event, participants in the present study who were classified with high SCT did report greater psychopathology symptoms (i.e., ADHD-inattentive, ADHD-hyperactive-impulsive, depressive, anxious) and poorer emotion regulation and social functioning in comparison with participants without high SCT.
The current findings should be considered in light of several limitations. First, as noted above, the cross-sectional nature of this study precludes drawing causal conclusions, and there is a critical need for longitudinal studies of SCT and its effects on development and adjustment. In addition, as noted above, our study was limited to primarily non-Hispanic White college students from a single university. A third limitation of the present study is sole reliance on self-reported psychopathology, emotion regulation, and social functioning. In addition to the mediating hypotheses discussed above, it will also be important for future research to incorporate additional measures (e.g., other co-occurring psychopathologies) and informants (e.g., parents, peers) to more fully test the hypothesis that emotion dysregulation mediates the association between SCT and social adjustment. Similarly, our measure of emotion dysregulation only assesses for difficulties with managing negative emotions. Whether similar deficits with regulating positive emotions are also related to SCT is unknown. Despite these limitations, this study offers an important first step in elucidating potential pathways by which SCT is linked to psychosocial impairment and points to the need for additional research in this area.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Miami University Doctoral-Undergraduate Opportunities for Scholarship (DUOS) award fostering research collaboration between undergraduate (Mr. Flannery) and graduate (Mr. Becker) students, with this project conducted under Dr. Luebbe’s faculty oversight and mentorship.