
Abstract
Keywords
Introduction
ADHD is the most common childhood mental disorder, afflicting approximately 5% to 10% of school-age children (Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007; Skounti, Philalithis, & Galanakis, 2007). Children diagnosed with ADHD vary widely in the types and severity of symptoms that they demonstrate, but the disorder is generally characterized by low levels of attention and concentration, and high levels of activity, distractibility, impulsivity, and the inability to inhibit inappropriate actions (American Psychiatric Association, 2000). Numerous studies using objective, laboratory-based measures of neuropsychological functioning in individuals with ADHD have found deficits in sustained attention, inhibitory control, and target detection (Berwid et al., 2005; Pasini, Paloscia, Alessandrelli, Porfirio, & Curatolo, 2007; Perera et al., 2012; Stern & Shalev, 2013; Tucha et al., 2009; Wang et al., 2011). However, these studies focused primarily on the visual modality, despite the importance of the auditory modality and auditory attention to many areas of learning and functioning.
Attentional mechanism is considered a limited capacity system; there are disparate viewpoints as to the specifications of attentional capacity. One viewpoint assumes central attentional resources that are common to all sensory modalities (Broadbent, 1952). Central capacity theorists argue that tasks draw upon a single pool of attentional resources that can be used flexibly across modalities. However, the possibility of a supramodal attentional system is questionable, as a number of studies have provided counterevidence by using concurrent tasks that tap resources in different modalities (Allport, Antonis, & Reynolds, 1972; Hirst, Spelke, Reaves, Caharack, & Neisser, 1980; Wickens, 1984). In addition, previous studies on auditory and visual information processing in the human brain have suggested that different stimulus features (e.g., pitch, location, color, form) are processed in separate areas of the cerebral cortex (Arnott & Alain, 2011; Cardoso-Leite & Gorea, 2010; Recanzone & Cohen, 2010; Salo, Rinne, Salonen, & Alho, 2013). Based on the difference between primary auditory and visual perceptual systems, it is possible that attention can be modality specific.
Also, the following differences between the visual and auditory modalities are significant. First, information in the auditory channel is primarily temporally sequenced and of short duration, in contrast to visual information, which is richer in spatial organization and often stable for a longer duration (Gomes, Wolfson, & Halperin, 2007). Second, auditory processing transforms the sound-emitting properties of things, while visual processing transforms light reflecting properties (Bregman, 1990). Third, all auditory stimuli impinge on the ears, even if not equally, resulting in a greater need for sorting, weighting, and selecting which auditory information will be further processed (Julesz & Hirsh, 1972). Fourth, unlike the eyes, the ears cannot be closed and can pick up signals in a 360° arc around the body from both visible and occluded sources (Gomes et al., 2007; Julesz & Hirsh, 1972). Given these significant differences between the auditory and visual systems, it is probable that there are modality-specific attentional mechanisms.
Doyle, Biederman, Seidman, Weber, and Faraone (2000) suggested that a combination of visual and auditory tasks would provide more information than adopt only one modality. To date, two investigations (Aylward, Brager, & Harper, 2002; Draeger, Prior, & Sanson, 1986) have explored attentional performance on standardized visual tasks in conjunction with standardized auditory tasks in evaluating ADHD; however, the results of these studies were limited by the recruitment of undiagnosed ADHD samples or the adoption of incompatible visual and auditory attentional tools. Most previous ADHD studies adopted only a single sensory modality (usually vision) to represent attentional problems. It seems that these researchers treated individuals with ADHD as “concordant” for both visual and auditory information processing, meaning these individuals displayed similar deficits in visual and auditory attention.
Although previous studies have demonstrated the utility of visual Continuous Performance Task (CPT) in differentiating children with ADHD from normal controls (Berger, Slobodin, Aboud, Melamed, & Cassuto, 2013; Epstein et al., 2003; Halperin, Trampush, Miller, Marks, & Newcorn, 2008; Johnson et al., 2007; Miranda et al., 2012), little is known about the differences between children with ADHD and their typically developing peers in the performance of auditory attention. No investigation had been executed to explore the differences in the performance of auditory and visual attention in children with ADHD by recruiting qualified ADHD samples and adopting adequate tools. Thus, the differences in the performance of auditory and visual attention in children with ADHD are still unknown.
The current study was conducted to explore the performances of auditory and visual attention in children with ADHD as compared with those of their typically developing peers. Two hypotheses were explored in the present study. First, we explored whether, compared with age- and sex-matched controls, children with ADHD performed more poorly among the dimensions (indexes) of the visual attention tests. Based on previous studies related to visual attention, we hypothesized that in most dimensions of visual attention, children with ADHD might show significant differences from their typically developing peers. Second, based on the viewpoint of modality-specific attentional mechanisms, we hypothesized that the performance of auditory attention would be different from those of visual attention in children with ADHD. In other words, children with ADHD may have a deficit in a specific dimension of one modality but not necessarily in another modality.
Method
Research Design
A randomized, two-period crossover design was used in this study for both children with ADHD and their typically developing peers to balance the order of two test conditions (see Figure 1). The crossover design provides statistical efficiency, as different subjects may respond with wide variation to intervention, whereas variation within the same subjects may be considerably less (Woods, Williams, & Tavel, 1989). Also, all participants in this study had to complete two laboratory-based tests; the crossover design could decrease the impact of learning and fatigue effects in performing these tests.
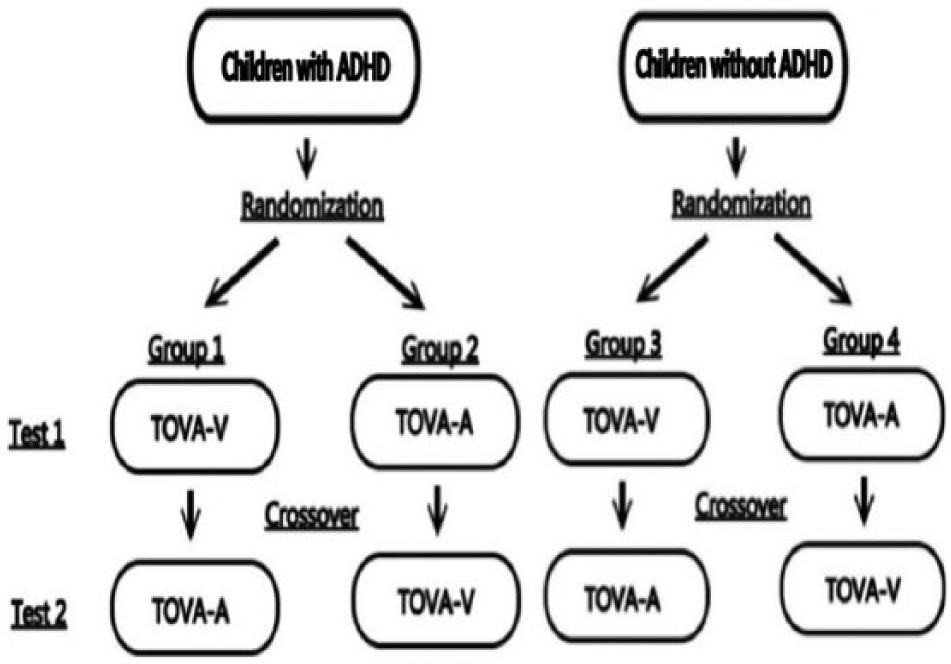
The randomized, two-period crossover design.
Participants
A total of 100 children (aged 6-12) participated in this study. Fifty participants had ADHD, and 50 participants were their typically developing peers without any history of neurological or psychiatric illness. Inclusion criteria for the ADHD participants were as follows: (a) full-scale intelligence quotient (FSIQ) of the Wechsler Intelligence Scale for Children–IV (WISC-IV) above 80; (b) diagnosis of ADHD by qualified neurologists; (c) no diagnosis of neurological disorders other than ADHD; (d) normal or corrected visual ability; (e) normal hearing ability; and (f) normal hand function.
Instrumentation
Test of Various Attention (TOVA)
TOVA is an X-type CPT in that the individual is required to respond as quickly as possible to the target stimulus, while inhibiting response to the nontarget stimulus (Swalwell, Greenberg, & Dupuy, 2011). There are two versions of TOVA. One measures auditory information processing (TOVA-A); the other, visual information processing (TOVA-V). Both versions of TOVA were used in the present study. According to literature, the psychometric data of the TOVA are as follows: The reliability coefficients of all TOVA variables reached significant levels (p < .05), with a range of 0.31 to 0.99 and a mean of 0.81 (Huang, Chao, Wu, Chen, & Chen, 2007; Llorente et al., 2001; Wu et al., 2007). This finding demonstrates an overall satisfactory internal consistency for the TOVA. Also, empirical study showed that ADHD scores correlated significantly with hyperactivity scores on the Child Behavior Checklist (CBCL; r = −.42, p < .05), this finding demonstrates adequate convergent and discriminant validity for the TOVA (Wu et al., 2007).
This study adopted the TOVA as the evaluation tool based on the following advantages. First, the TOVA-A and TOVA-V measure the same variables (indexes) for auditory and visual modalities. Second, the TOVA-A and TOVA-V were developed based on similar design logic, both tests are built upon similar task parameters (simple figures or tones) to measure attention. Finally, all participants in the present study are Taiwanese, so we adopted TOVA, which is a nonlanguage and non-Arabic number based test, to avoid the confounding effects of language and cultural differences. Also, empirical research (Wu et al., 2007) had proved that TOVA can provide objective, reliable, and valid information as well as make a meaningful contribution to the clinical assessment of inattention and impulsivity problems for Taiwanese children, so the testing contents of the TOVA are easy for all participants to understand in the present study.
Four identical indexes of the TOVA-A and TOVA-V were adopted in present study:
Omission Errors (OE)—An index of sustained attention, this score is evaluated as the failure to respond to the target stimulus. Scores of OE are presented as percentages in present study.
Commission Errors (CE)—An index of response inhibition, this score is measured as an inappropriate response to the nontarget stimulus. Scores of CE are presented as percentages in present study.
Response Time (RT)—An index of response speed, this score is determined as the average of the correct RTs. Scores of RT are presented in milliseconds in present study.
RT Variability (RT Variability)—An index of attentional inconsistency, this score is evaluated as the standard deviation (SD) of the mean of correct RTs. Scores of RT Variability are presented in milliseconds in present study.
Procedures
Both participating groups (children with and without ADHD) were randomly assigned to two subgroups for different procedures of taking the TOVA (see Figure 1). Participants assigned to Group 1 (or Group 3) completed the TOVA-V first, after which they took the TOVA-A 30 min later. Participants assigned to Group 2 (or Group 4) completed both versions of the TOVA in the reverse order. Both versions of the TOVA were administered on a personal desktop computer. Before taking each version of the TOVA, all participants completed a 2.5-min practice section. Total test time was approximately 80 min, with two practice sections and one 30-min refreshment break. The experimental setting was located in a specific designated speech therapy room, a quiet test environment with optimal noise insulation equipment. During the test, only the test taker (one at a time) and administrator (the first author) were present in the room. The examiner stood to the rear of the test taker to ensure that the experiment would be carried out smoothly.
Statistical Analyses
The data were analyzed with the statistical software package SPSS, Version 19. Independent-sample t testing was computed to compare the four attentional indexes between the two children groups. Two-tailed p values < .05 were considered statistically significant; Cohen’s d was adopted to calculate the effect size. Effect size is a standardized quantitative index that can represent the magnitude of change that one variable produces in another variable as reflected in the difference between two means, independent of sample size (Cohen, 1988). Interpretation of the effect size d is based on a convention suggested by Cohen, such that 0.20 is considered a small effect size, 0.50 is considered medium, and 0.80 or greater, a large effect size. The statistical significance was sufficient to explain most cases only if the effect size d was considered as large magnitude (d =>.80) in this study.
Results
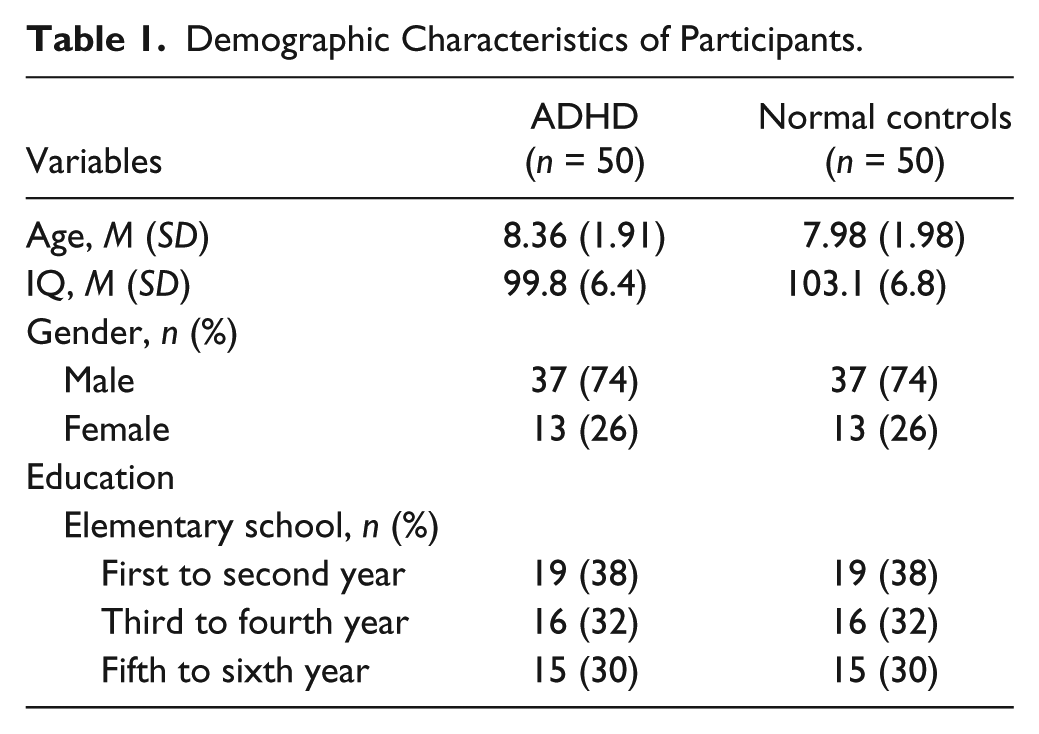
Demographic information for the sample is provided in Table 1. The typically developing children (n = 50) were selected to match the children with ADHD (n = 50) for age and gender.
Demographic Characteristics of Participants.
To evaluate our hypotheses, group means were compared on the four indexes of the TOVA using independent group t tests. Group means (M), SD, t value, p value, and effect sizes (Cohen’s d) are presented in Table 2. According to Table 2, three auditory attentional indexes, including OE (t = 3.20; p < .05), RT (t = 2.84; p < .05), and RT Variability (t = 5.06; p < .05), showed significant differences between the two children groups. For the auditory attentional index of CE, though not showing statistical significance (p = .059), the result may show different if recruiting larger samples, as the p is very close to .05. Only the auditory index of RT Variability was considered to have large effect sizes (d = 1.01). This result suggests that only the problem of high variability of auditory attention is sufficient to explain most cases of ADHD. In addition, the auditory attentional index of CE, though not showing statistical significance (p = .059), could show it with larger samples, as the p is very close to .05.
Comparison of TOVA Results Between Children With and Without ADHD.
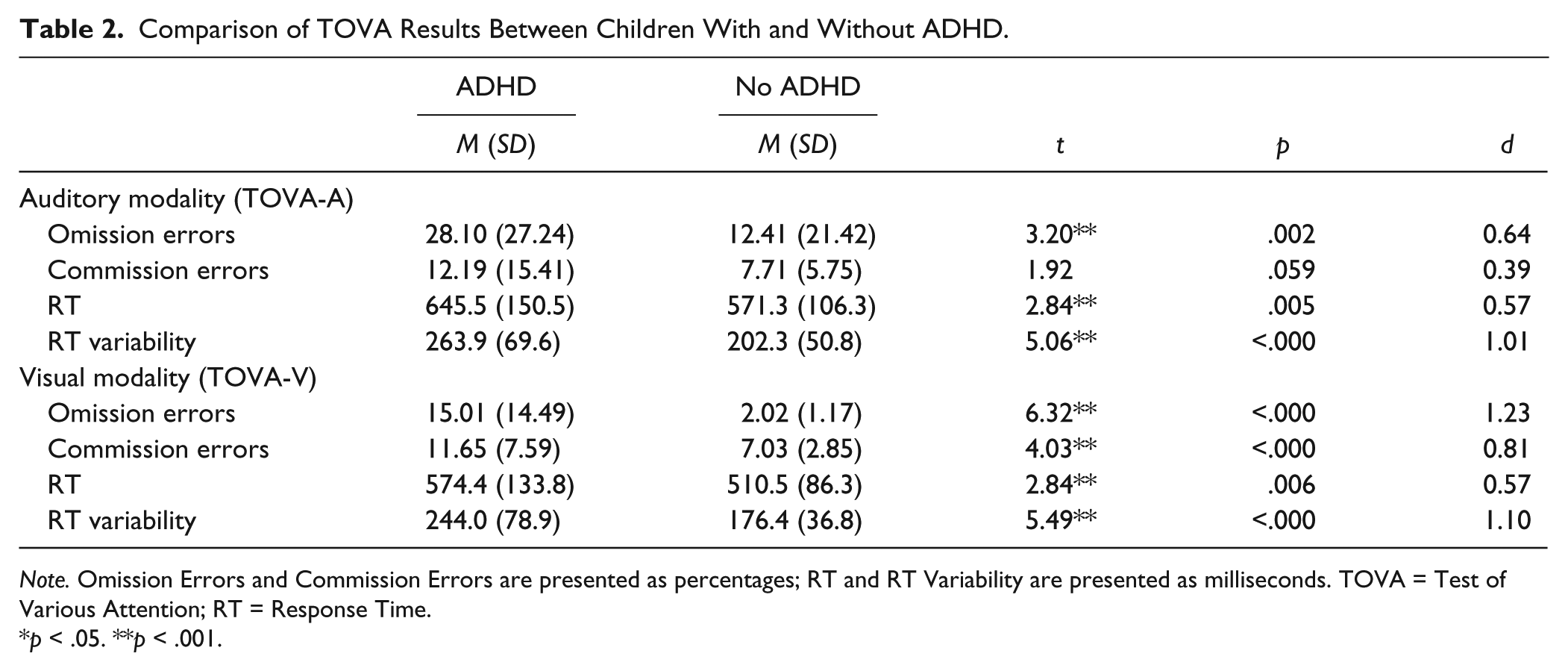
Note. Omission Errors and Commission Errors are presented as percentages; RT and RT Variability are presented as milliseconds. TOVA = Test of Various Attention; RT = Response Time.
p < .05. **p < .001.
All four visual attentional indexes, including OE (t = 6.32; p < .05), CE (t = 4.03; p < .05), RT (t = 2.84; p < .05), and RT Variability (t = 5.49; p < .05), showed significant differences between the two children groups (see Table 2); and three of these indexes, including OE, CE, and RT Variability, were considered to have large effect sizes (d ranging from 0.81 to 1.23). These results suggest that the problems of sustained attention (OE), response inhibition (CE), and attentional inconsistency (RT Variability) are sufficient to explain most cases of ADHD on the visual modality.
Discussion
The present study attempted to address a number of methodological concerns from the existing literature related to attentional testing issues of ADHD. First, a randomized, two-period crossover design was used in this study for both groups of children to balance the order of the two test conditions. This methodology decreased the impact of learning and fatigue effects in performing two sufficiently long laboratory tests based on similar design logic. Such effects (learning and fatigue effects) have not always been considered in previous studies. Second, we recruited participants with a full clinical diagnostic assessment of ADHD identified by qualified neurologists, instead of children with suspected ADHD or those at high risk of ADHD. Third, school-aged children with neurodevelopmental deficits, language deficits, learning disorder, or other externalizing disorders (e.g., oppositional defiant disorder [ODD]) were not included in the present study to avoid possible interference. In past studies, such comorbidities have not always been considered, leaving one to wonder how much of the reported findings could be reliably attributed to the core features of ADHD. Fourth, we employed the TOVA, a packaged computerized laboratory test that includes comparable auditory and visual indexes, as the assessment tool instead of adopting two separate auditory and visual tests based on different theoretical bases or adopting different attentional indexes. Finally, based on the results of empirical studies (Aylward et al., 2002; Hennessey, Stein, Rosengard, Rose, & Clarke, 2010; Mani, Bedwell, & Miller, 2005; Skogli, Teicher, Andersen, Hovik, & Oie, 2013), we recognized that the factors of age and gender truly affect the attentional performance of children with ADHD, so we adopted age- and sex-matched typically developing peers as the normal controls in the present study to decrease the effects of these attributes. Based on these advantages over previous research on related topics, the findings of the present study should be valuable to discussions of the auditory and visual attention of children with ADHD.
Hypothesis 1
The first hypothesis of the present study was that in most dimensions of visual attention, children with ADHD would show significant differences from their typically developing peers, based on the findings of previous studies related to visual attention. The results of present study (see Table 2) support our first hypothesis in that most dimensions, all four visual attentional indexes, showed significant differences between the two children groups. Most visual attentional indexes, including sustained attention (OE), response inhibition (CE), and attentional inconsistency (RT Variability), were considered to have large effect sizes, so the problems of sustained attention, response inhibition, and attentional inconsistency are sufficient to explain most cases of ADHD on the visual modality.
Previous studies has found ADHD patients to have slower overall mean RTs than healthy adults (King, Colla, Brass, Heuser, & von Cramon, 2007; Lundervold et al., 2011), but the medium effect size (d = 0.57) along with the visual index of response speed (RT) suggests that low visual response speed is insufficient to explain most cases of ADHD in the present study. Why is visual RT insufficient to explain most cases of ADHD in the present study? Two large cross-sectional studies may provide a possible answer to this question. In the first (Gualtieri & Johnson, 2006), which examined maturational changes of executive function in ADHD, recently reported impairments in psychomotor speed and reaction times across the investigated age range (10-29 years) in their patient group. Gualtieri and Johnson found that in both normals and in ADHD patients, performance improved with age. However, control group participants improved their performance with shorter reaction times, whereas ADHD patients adopted a less efficient strategy with increased response latencies with age. The second (Berger et al., 2013), which examined whether school-aged ADHD children showed a developmental delay in cognitive performance measured by CPT, found that despite improvement in CPT performance with age, ADHD children continued to demonstrate impaired performance in visual reaction speed as compared with controls, and this delay was most prominent in older children. In the present study, 70% of participants were younger than 10 years (see Table 1); it is possible that not all typically developing children in this age range knew how to adopt more efficient strategies. Also, the children with ADHD in this age range may not have presented serious developmental lag. If this possibility explains why the effect size of the visual response speed was only medium, then recruiting older children may show a larger magnitude on this visual index (RT).
Hypothesis 2
For the processing of auditory information, children with ADHD presented different features of auditory attention from visual attention in at least two aspects as compared with typically developing children (see Table 2). First, children with ADHD showed significant differences from their typically developing peers on the visual index of response inhibition (CE); however, no such difference was shown on auditory modality. Second, most visual attentional indexes were considered to have large effect sizes. However, only the auditory indexes of attentional inconsistency (RT Variability) reached this criterion; the other three auditory attentional indexes, sustained attention (OE), response inhibition (CE), and reaction speed (RT), had only small to medium effect sizes (d ranging from 0.30 to 0.57). These features highlight the potential difference between auditory and visual attention in children with ADHD, so our second hypothesis, that the deficiencies in auditory attention are not necessarily identical to those in visual attention in children with ADHD, is supported.
Reaction Time Variability
Among four attentional indexes, only the index of attentional inconsistency (RT Variability) showed significant group differences (p < .05) and also had large effect sizes in both auditory (d = 1.01) and visual (d = 1.10) modalities (see Table 2). This finding highlights the importance of performance variability in ADHD when both auditory and visual modalities are considered. Previous empirical research and controlled observations suggest that individuals with ADHD are consistently inconsistent across a wide range of tasks, including tasks measuring reaction time on motor speed, choice decision, vigilance, behavioral inhibition, cognitive interference, visual saccade, and visual discrimination (Buzy, Medoff, & Schweitzer, 2009; Kofler, Rapport, & Alderson, 2008; Kofler et al., 2013; Willcutt, Sonuga-Barke, Nigg, & Sergeant, 2008). However, these studies considered only indexes based on visual modality. We further propose that the consistent inconsistency also appeared on tasks measuring reaction time of auditory attention. This result support the finding of a recent study (Díaz-Orueta et al., 2014), which adopt the CPT developing in a virtual setting to explore similar topic, stated the importance of reaction time variability, a measure of consistency of attention, in both auditory and visual attention of children with ADHD.
The Attentional Deficiency of ADHD Is Modality Specific
In the present study, attentional performance was lower in the auditory modality (higher percentage of error, higher reaction time, and higher variability) than in the visual modality of children without ADHD (see Table 2). This finding suggests that the auditory task (TOVA-A) is more difficult than the comparable visual task (TOVA-V). If the auditory attentional task is more difficult than comparable visual task, than why is visual attentional performance shown to be more deficient, including more deficient attentional indexes and larger effect sizes, than auditory attentional performance in children with ADHD? The answer may be related to the developmental lag of ADHD and the different developmental trajectories between the two modalities. We have discussed above that a developmental lag of cognitive functions has long been hypothesized to underlie ADHD. However, only the reason of developmental lag is insufficient to explain why children with ADHD show less deficiency in auditory attentional performance than in visual attention, because children with ADHD suffer developmental lag in both modalities. The auditory and visual systems have different developmental trajectories (Dawes & Bishop, 2008). It is possible that the difference between auditory and visual attentional performance reflects maturational asynchronies; the auditory system starts functioning during the last trimester of gestation, whereas the visual system does not start functioning until after birth (Jusczyk, 1998). As a result, the development of visual system may still lag behind the development of auditory system in early childhood. Combining the two viewpoints, the developmental delay of ADHD and the maturational asynchronism between two modalities, may explain why visual attentional performance shown to be more deficient than auditory attentional performance in children with ADHD.
More specifically, the results of the present study showed that most children with ADHD have a problem with visual inhibition, but not with auditory inhibition. This finding is supported by a previous study, which explored developmental changes in visual and auditory inhibition (Guy, Rogers, & Cornish, 2012). Guy et al. (2012) found a more profound effect of inhibition in terms of accuracy and reaction time in the visual task than in the auditory task. In other words, it was more difficult for their normal preschoolers to inhibit visual stimuli than to inhibit auditory stimuli. Combining the viewpoints of developmental lag, maturational asynchronies, and Guy’s research, it is not hard to imagine the different features of inhibitory function between the two modalities in children with ADHD. These findings provide strong evidence that the attentional deficiency of ADHD is modality specific.
Limitations
Three limitations of the present study need to be considered when interpreting the findings. First, a major methodological limitation of this study is that we recruited only clinical participants with ADHD. The clinic-based sampling limits the generalization of our results, so our findings should not be extrapolated to the general population. Second, because only school-aged children (aged from 6 to 12 years) were included in our study samples, our findings should not be extrapolated to children outside this age group. Third, the subtype of ADHD was not considered in the present study. One of our main purpose of this study was to expanding the number of participants included by recruiting samples of ADHD that were as large as possible in the present study. The balance of each subtype of ADHD was not considered during the period of recruitment, so parts of the participants’ subtypes of ADHD in this study were not identified or distinguished. Although some participants were of identified subtypes (most participants were diagnosed as combined type), analyzing the data was problematic because of the inadequate proportions of these subtypes among these participants.
Future Research
To explain why visual reaction time is insufficient to explain most cases of ADHD in the present study, we propose the possibility that many children in both groups (70%) of the present study were too young to present a difference in adopted strategies to improve their response speed in taking computerized tests. Further research should recruit two different age groups to test the possibility of the above inference. In addition, this study provides strong evidence that the attentional deficiency of ADHD is modality specific; however, based on the limit of CPT assessment tools, only four dimensions (indexes) of attentional performance were explored in the present study. Further studies should adopt different assessment tools or even develop more adequate attentional tests to explore the differences in performance on other attentional dimensions (e.g., selective or shifting attention) between two modalities. Finally, we do realize the importance of analyzing the influence of ADHD subtypes; however, this issue still needs further exploration based on the limitation in the present study. We recruited only clinical participants with ADHD, empirical studies had found that clinic-referred children are more likely to present overtly severe behavioral symptomatology (Staller & Faraone, 2006). Consequently, clinic-referred children may constitute a more homogeneous group than children who have ADHD problems but are not referred for assessment or treatment (Lambek, Trillingsgaard, Kadesjö, Damm, & Thomsen, 2010). This may be the reason that most identified ADHD were belong to the combined type in the present study. Researchers should also consider recruiting community-based ADHD participants to balance each subtype of ADHD in the future research.
Conclusion
In conclusion, our findings highlight the fact that the attentional deficiency in children with ADHD is modality specific, and that the deficiency of visual attention is more serious than that of auditory attention in children with ADHD. In the auditory modality, only the deficit of attentional inconsistency was sufficient to explain most cases of ADHD. In the visual modality, the deficits of sustained attention, response inhibition, and attentional inconsistency were all sufficient to explain most cases of ADHD. In addition, an identical attentional deficit, the performance of attentional inconsistency, in both modalities was also found in the present study. This deficit is sufficient to explain most cases of ADHD in both auditory and visual attentional performance; in other words, the index of attentional inconsistency is the most important indicator for diagnosing and intervening in ADHD when both auditory and visual modalities are considered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.