
Abstract
Extensive research demonstrates that negative body image and depression are related and together contribute to eating disorder symptoms (Spoor et al., 2006; Stice & Bearman, 2001). Other research shows that ADHD symptoms place adolescents and young adults at risk for depression symptoms (Bagwell, Molina, Pelham, & Hoza, 2001; Barkley, Fischer, Smallish, & Fletcher, 2002; Biederman et al., 2008). However, little to no research has identified how ADHD symptoms relate to body image or eating disorders. Negative body image may contribute to the positive association of depression symptoms with ADHD symptoms. Further, improving understanding of how ADHD symptoms, body image, and depression symptoms relate may inform future research on how ADHD symptoms relate to eating disorders. The present study examined the role of body image in the association between ADHD and depression symptoms among young adult college students.
ADHD and Body Image
Understanding how ADHD symptoms relate to body image is important given the close association between negative body image and eating disorders (Stice & Bearman, 2001; Stice & Shaw, 1994). Only two studies have included body image constructs when assessing outcomes associated with ADHD symptoms. This research suggests that, as youth with ADHD symptoms enter adolescence, they experience greater body dissatisfaction than their counterparts without ADHD symptoms (Mikami et al., 2010; Mikami, Hinshaw, Patterson, & Lee, 2008). Such findings are cause for concern given that negative body image is a notable risk factor for depression symptoms and eating disorders (Markowitz, Friedman, & Arnet, 2008; Stice, 2002) and that adolescence is the highest risk developmental period for onset of eating disorders and depression symptoms (Kessler et al., 2012; Swanson, Crow, Le Grange, Swendsen, & Merikangas, 2011). Importantly, although existing research has focused on adolescence, findings relating body image and ADHD symptoms may hold true for emerging adults, as they also experience risk for developing eating disorder and depressive symptoms. However, no research has identified if these associations have emerged among young adults. Further, little research has identified at any age the degree to which ADHD symptoms affect body image constructs other than body dissatisfaction, such as evaluation of one’s appearance, the value one places on physical appearance, preoccupation with weight and shape, and comparison of one’s body weight and size with peers.
Very little research has specifically evaluated rates of binge-eating or anorexia nervosa among adolescents or young adults with ADHD (Cortese, Isnard, Bernardino, & Mouren, 2007). Some studies indicate that bulimia does not occur at significantly higher rates among adolescents and young adults with ADHD (Surman, Randall, & Biederman, 2006). Other studies with prospective designs demonstrate higher rates of bulimia among adolescents with childhood diagnoses of ADHD (Biederman et al., 2007; Mikami et al., 2010; Mikami et al., 2008), with one study showing a 5.6-fold increase in prevalence of bulimia symptoms among adolescents with ADHD (Biederman et al., 2007). Given the crucial role that body image plays in eating pathology, understanding how ADHD symptoms relate to body image may shed light on inconsistent findings and demonstrate future research approaches to investigate the links between ADHD symptoms and eating disorders.
ADHD and Depression
The association between ADHD and depression has been demonstrated across a variety of samples (see Bagwell et al., 2001; Barkley, 2002; Biederman et al., 2008). Several studies indicate that ADHD increases risk for depression in adolescence and young adulthood (Bagwell et al., 2001; Barkley et al., 2002). Comorbidity between ADHD and depression is estimated to be 20% to 30% with some researchers indicating that adolescents with ADHD experience 5.5 times greater risk of having a depressive disorder than adolescents without ADHD (Costello, Mustillo, Erkanli, Keeler, & Angold, 2003). Chronis-Tuscano et al. (2010) found that children diagnosed with ADHD during childhood were significantly more likely to receive a depression diagnosis, report experiencing suicidal ideation, or have attempted suicide during adolescence. Van Eck, Ballard, et al. (2014) showed that risk for depression symptoms and suicidal ideation was heightened among young adult college students with ADHD symptoms as well. These studies demonstrate the close association between depression and ADHD symptoms during adolescence and young adulthood. Clarifying what factors contribute to increased risk for depression among youth with ADHD symptoms is an important undertaking for identifying effective prevention and intervention strategies for this population.
Body Image and Depression
Extensive research links negative body image to depression symptoms (Carpenter, Hasin, Allison, & Faith, 2000; Dong, Sanchez, & Price, 2004; Markowitz et al., 2008; Onyike, Crum, Lee, Lyketsos, & Eaton, 2003; Simon et al., 2006). It is crucial to understand how body image relates to depression symptoms given evidence suggesting that, together, depression symptoms and negative body image predict the maintenance of eating pathology (Stice & Bearman, 2001). Research has found that normal weight adolescent boys who view themselves as under- or overweight reported higher levels of depressive symptoms as compared with boys who viewed themselves as average weight (Blashill & Wilhelm, 2014). Further, research with both male and female adolescents found that body dissatisfaction was associated with increased depressive symptoms, especially among individuals who expressed a desire to be thinner or a distortion between their perceived and desired physical figure (Almeida, Severo, Araújo, Lopes, & Ramos, 2012). Because the literature suggests a strong association between body image and depression, it is important to understand how body image may affect the link between ADHD and comorbid depressive symptoms.
The Present Study
Given the links between depression, negative body image, and ADHD, the purpose of the current study was to evaluate the degree to which body image contributed to the association between depression and ADHD symptoms. Specifically, analyses assessed the mediating role of body image in the link between depression and ADHD symptoms. Based on the existing research, we expected that as ADHD symptoms increased, college students would evaluate their bodies less positively, demonstrate more orientation to their appearance, experience less satisfaction with their body, more preoccupation with their weight, and perceive themselves to be more overweight. We hypothesized that these negative body image tendencies would partially mediate the association between ADHD and depression symptoms for college students.
We included participant gender, minority race/ethnicity, mother’s education, and household income during childhood as covariates in analyses. We added these covariates given research findings indicating that these variables affect ADHD symptoms, depression symptoms, or body image. Young adult males are more likely than young adult women to display ADHD symptoms (Murphy & Barkley, 1996), whereas young adult women tend to display higher depression symptoms than young adult men (Lopez et al., 2014). Different cultural norms related to ideal body shape and size may affect body image constructs (George & Franko, 2010). Finally, research on the epidemiology of depression symptoms demonstrates that the socioeconomic status of a young adult’s childhood inversely affects depression symptoms (Quesnel-Vallée & Taylor, 2012). With the inclusion of these covariates, we will be able to state that this study’s findings exist despite the confounding influence of these included covariates.
Method
Participants and Procedure
Participants were 627 college students aged 18 to 25 years (M = 20.23 years, SD = 1.40 years, 60% female), many of whom were freshmen (43%); 47% identified as European American, 12% as African American, 3% as Asian, and 3% as Latino. About 31% identified as multiracial; 4% did not specify race/ethnicity. Childhood household income was ≤US$40,000/year for 14% of participants and ≥US100,000 for 48%; 41% of participants’ mothers had completed some college coursework. Recruitment occurred through class announcements in undergraduate psychology courses. Participants consented online and completed an Internet-based survey (M = 52 min, range = 18-162 min). No significant inconsistencies were apparent between items with similar content, and response time on the survey was unrelated to study variables. Participants received extra course credit for participation and provided consent prior to completing the survey; the university’s Institutional Review Board approved all procedures.
Measures
ADHD symptoms
The Current Symptoms Scale, Self-Report Form (CSS; Barkley & Murphy, 2006) assesses continuous ADHD symptoms with 36 items that have a 4-point scale (0 = never or rarely to 3 = very often) and correspond to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) criteria for ADHD. Eighteen items asked about current symptoms, and another 18 items assessed childhood symptoms. Validity concerns about retrospective self-report (Mannuzza, Klein, & Moulton, 2002) led us to use only current symptoms. Items were summed for a total scale score, given the multicollinearity between inattention and hyperactivity (r = .78, p < .05). Reliability was strong (α = .92). Prior research indicates sensitivity to symptom change (Safren et al., 2005), and self-report is correlated with parent and spousal report (Barkley, Knouse, & Murphy, 2011; Barkley, Murphy, & Fischer, 2008). Sixty-one participants (9%) scored in the clinical range (i.e., symptoms ≥ CSS clinical cutoff for ADHD; Barkley & Murphy, 2006), which is slightly higher than ADHD prevalence rates among other studies of college students (2%-8%; DuPaul, Weyandt, O’Dell, & Varejao, 2009; Heiligenstein, Conyers, Berns, & Smith, 1998).
Depression symptoms
The Brief Symptoms Inventory (BSI; Derogatis & Coons, 1993) has 53 self-reported items that measure constructs related to psychological adjustment using a 5-point scale (1 = almost never to 5 = almost always). Analyses included only the depressive symptoms subscale (7 items). Reliability for this scale was strong (α = .89) with responses ranging from 7 to 29. The depression subscale has strong construct validity (Schwannauer & Chetwynd, 2007) and discriminates between those with and without Major Depression Disorder (Johnson, Chipp, Brems, & Neal, 2008). About 96 participants (15%) had symptoms in the clinical range, which is slightly above the typical prevalence rate of depression found among college students (8.4%; Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality, 2012).
The Multidimensional Body-Self Relations Questionnaire–Appearance Scale (MBSRQ-AS; Cash, 2000; Cash, Winstead, & Janda, 1986) is comprised of 34 self-report items measuring five components of body image: Appearance Evaluation, Appearance Orientation, Overweight Preoccupation, Self-Classified Weight, and the Body Areas Satisfaction Scale (BASS) on a 5-point Likert-type scale (1 = definitely disagree to 5 = definitely agree). Higher scores on the 7-item Appearance Evaluation scale (α = .90) refer to more negative feelings or more problems related to physical attractiveness and satisfaction with one’s looks. Higher scores on the 12-item Appearance Orientation scale (α = .83) indicate placing greater value on one’s appearance, paying more attention to appearance, and spending more time grooming. Higher scores on the 4-item Overweight Preoccupation scale (α = .80) indicate increased experience of weight anxiety and vigilance, dieting, and eating restraint. Higher scores on the 9-item BASS (α = .86) correspond with greater dissatisfaction with discrete aspects of one’s appearance and specific parts of one’s body. Higher scores on the 2-item Self-Classified Weight scale (α = .79) indicate appraisal of one’s self as being more overweight.
Analytic Procedures
We evaluated the effect of ADHD symptoms on depression symptoms through body image constructs and the degree to which each body image construct mediated these relations. That is, ADHD symptoms were linked in the model to body image, which was linked to depression symptoms; ADHD symptoms were also directly linked to depression symptoms. Independent models were estimated for each body image construct given the multicollinearity among these constructs. Covariates included participant sex (0 = female, 1 = male), race/ethnicity (0 = European American, 1 = non-European American), mother’s education, and household income during childhood.
We estimated all paths of each mediation model simultaneously using maximum likelihood estimation and bootstrapping with 5,000 generated samples, where 95% confidence intervals represented the possible range of the reported point estimates (Preacher & Hayes, 2008). Fully saturated models were assessed obviating fit statistics.
The only missing data were for 29 participants who did not disclose their racial/ethnic background (4.4% of data). List-wise deletion was used to manage missing data, which was appropriate given the small proportion of data missing and their lack of association with variables of interest.
Results
Descriptive Statistics
Descriptive statistics and correlations were assessed for continuous variables (see Table 1). Only depression symptoms demonstrated skew outside of the accepted range. However, skew did not change significantly when depression symptoms were log transformed and results were similar between models with and without depression symptoms log transformed. Thus, depression was retained without the transformation.
Correlations Among Continuous Variables and Descriptive Statistics (N = 627).
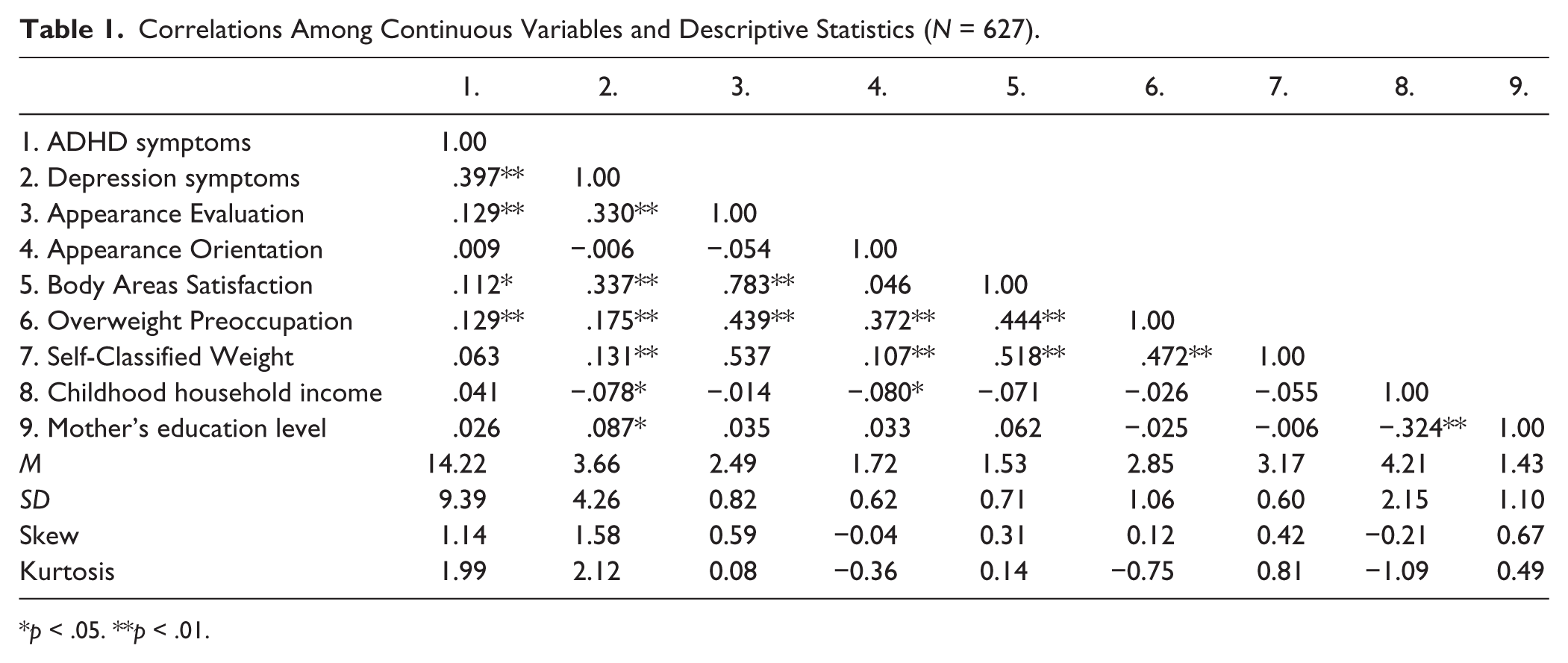
p < .05. **p < .01.
ADHD symptoms displayed a moderate correlation with depression symptoms and small positive correlations with Appearance Evaluation, Body Areas Satisfaction, and Overweight Preoccupation. Depression symptoms shared moderate, positive associations with Appearance Evaluation and Body Areas Satisfaction and small, positive correlations with Overweight Preoccupation and Self-Classified Weight. These results supported pursuit of mediation models assessing the degree to which body image constructs contribute to the association between ADHD and depression symptoms. Furthermore, all body image constructs shared a moderate or large correlation with at least one other body image construct, supporting evaluation of the effect of body image constructs in separate mediation models.
Depression symptoms also shared a very small negative association with childhood household income and a very small positive association with mother’s education level. These results supported inclusion of childhood household income and mother’s education level as covariates in mediation models.
Mediation Analyses
Appearance Evaluation
ADHD symptoms were associated with an indirect increase in depression symptoms through Appearance Evaluation (B = .017, SE = .007; see Table 2), as 95% confidence limits did not include zero (lower confidence limit [LCL] = .005, upper confidence limit [UCL] = .031). ADHD symptoms were also directly related to increases in depression symptoms (B = .192, SE = .025, t = 2.283, p = .022). The total effect of ADHD symptoms on depression symptoms, which represented the combined effect of the indirect and direct effect, was also significant and positive (B = .209, SE = .025, t = 2.819, p = .005).
Direct and Indirect Effects.
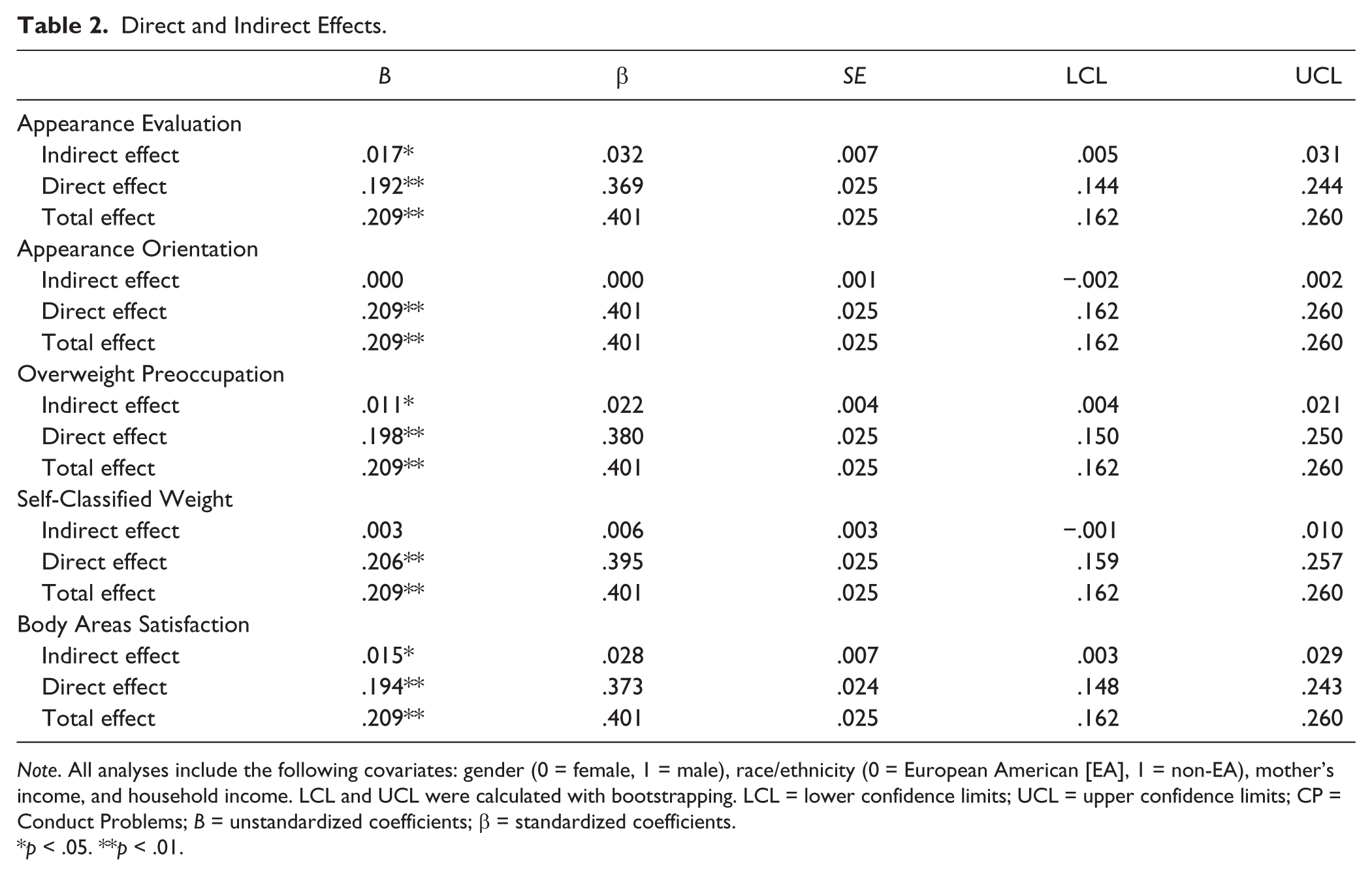
Note. All analyses include the following covariates: gender (0 = female, 1 = male), race/ethnicity (0 = European American [EA], 1 = non-EA), mother’s income, and household income. LCL and UCL were calculated with bootstrapping. LCL = lower confidence limits; UCL = upper confidence limits; CP = Conduct Problems; B = unstandardized coefficients; β = standardized coefficients.
p < .05. **p < .01.
According to MacKinnon (2008), the proportion mediated indicates how the size of the indirect effect compares with the total effect. It is calculated by dividing the indirect effect by the total effect. Given that the proportion mediated is not necessarily bounded by 0, caution is suggested in interpreting the proportion mediated as a strict proportion ranging from 0 to 1.0 (Preacher & Kelley, 2011). The proportion of the association between ADHD and depression symptoms that Appearance Evaluation mediated was .081. This finding indicates that Appearance Evaluation mediated approximately 8.1% of the variance in the total effect of ADHD symptoms on depression symptoms.
The standardized effect size of the indirect effect provides an indication of the proportion of variance that the indirect effect can account for in the outcome variable (MacKinnon, 2008). The standardized value of the indirect effect of ADHD symptoms on depression symptoms was 0.032, indicating that as the indirect effect of ADHD symptoms increased, depression symptoms increased by 0.032 standard deviations.
Consideration of the individual paths provides an indication of the contribution of a and b paths to the mediated effect (see Table 3 for regression coefficients for model paths). Standardized regression coefficients can serve as effect sizes for individual paths (MacKinnon, 2008). Standardized regression coefficients are bounded between 0 and 1.0; thus, effect size parameters for correlations apply. The a path for ADHD symptoms to Appearance Evaluation was negative and significant (a = .010, SE = .004, t = 2.824, p = .005) and had a standardized regression coefficient of .117. The b path for Appearance Evaluation to depression symptoms was negative and significant (b = 1.651, SE = .254, t = 6.506, p < .001) with a standardized regression coefficient of .275.
Path Coefficients for Mediation Models.
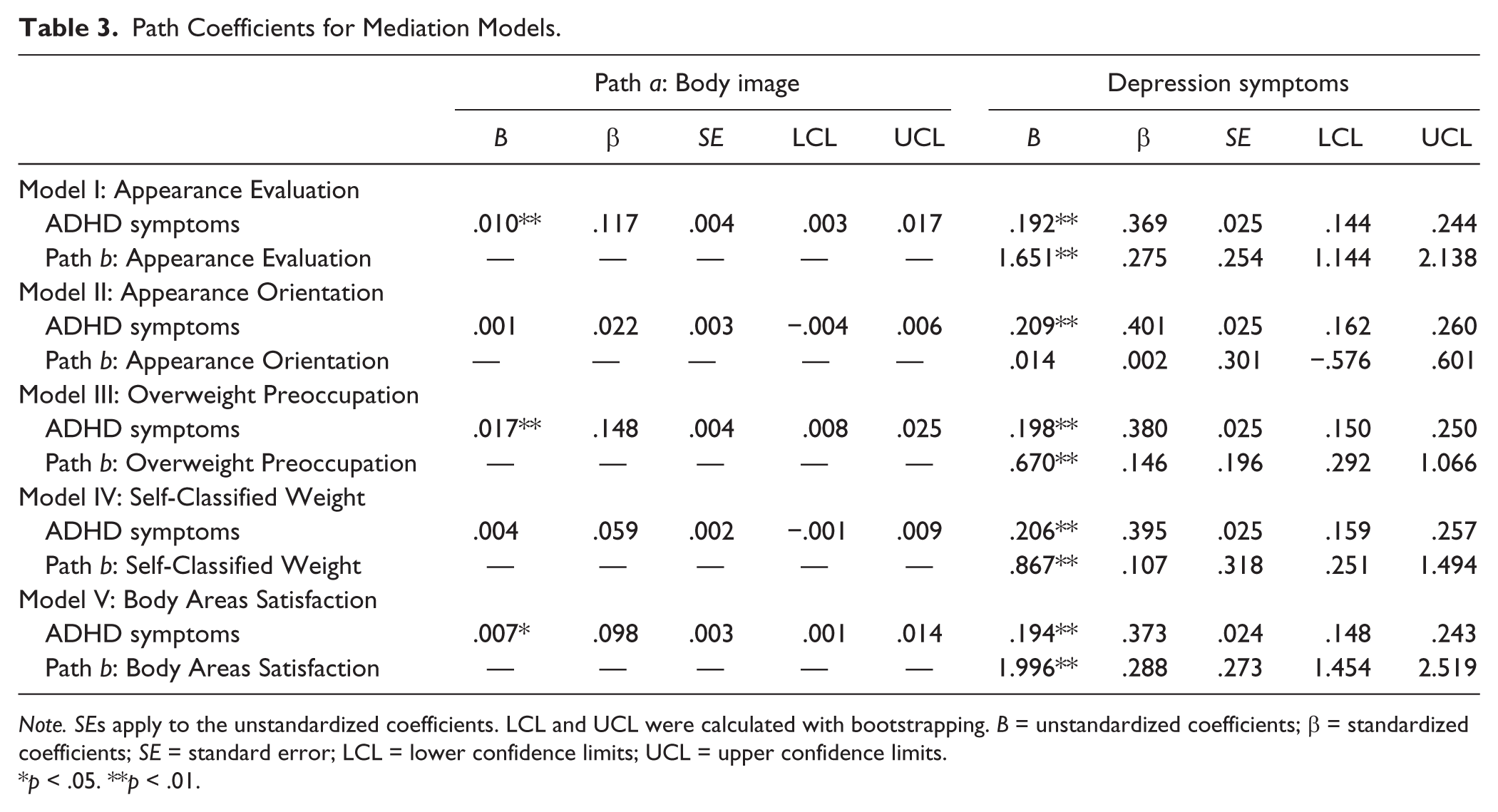
Note. SEs apply to the unstandardized coefficients. LCL and UCL were calculated with bootstrapping. B = unstandardized coefficients; β = standardized coefficients; SE = standard error; LCL = lower confidence limits; UCL = upper confidence limits.
p < .05. **p < .01.
Appearance Orientation
ADHD symptoms were not related to Appearance Orientation (B = .001, SE = .003, t = 0.559, p = .576), and Appearance Orientation was not related to depression symptoms (B = .014, SE = .301, t = 0.048, p = .962). The indirect effect of ADHD symptoms on depression symptoms through Appearance Orientation was not significant, with confidence intervals including zero (LCL = −.002, UCL = .002). However, the strong association between ADHD and depression symptoms remained (B = .209, SE = .025, t = 8.344, p < .001).
Body Areas Satisfaction
ADHD symptoms were associated with an indirect increase in depression symptoms through Body Areas Satisfaction (B = .015, SE = .007; see Table 2), as 95% confidence limits did not include zero (LCL = .003, UCL = .029). ADHD symptoms were also directly related to increases in depression symptoms (B = .194, SE = .024, t = 8.023, p < .001). The total effect of ADHD symptoms on depression symptoms was also significant and positive (B = .209, SE = .078, t = 8.350, p < .001).
The proportion of the association between ADHD and depression symptoms that Body Areas Satisfaction mediated was .072. This finding indicates that Body Areas Satisfaction mediated approximately 7.2% of the variance in the total effect of ADHD symptoms on depression symptoms. The standardized value of the indirect effect of ADHD symptoms on depression symptoms was .028.
The a path for ADHD symptoms to Body Areas Satisfaction was negative and significant (a = .007, SE = .003, t = 2.308, p = .021) and had a standardized regression coefficient of .003. The b path for Body Areas Satisfaction to depression symptoms was negative and significant (b = 1.996, SE = .273, t = 7.314, p < .001) with a standardized regression coefficient of .288.
Overweight Preoccupation
ADHD symptoms were associated with an indirect increase in depression symptoms through Overweight Preoccupation (B = .011, SE = .004; see Table 2), as 95% confidence limits did not include zero (LCL = .004, UCL = .021). ADHD symptoms were also directly related to increases in depression symptoms (B = .198, SE = .025, t = 7.806, p < .001). The total effect of ADHD symptoms on depression symptoms was also significant and positive (B = .209, SE = .025, t = 8.349, p < .001).
The proportion of the association between ADHD and depression symptoms that Overweight Preoccupation mediated was .053. This finding indicates that Overweight Preoccupation mediated approximately 5.3% of the variance in the total effect of ADHD symptoms on depression symptoms. The standardized value of the indirect effect of ADHD symptoms on depression symptoms was .022.
The a path for ADHD symptoms to Overweight Preoccupation was positive and significant (a = .017, SE = .004, t = 3.779, p < .001) and had a standardized regression coefficient of .148. The b path for Overweight Preoccupation to depression symptoms was positive and significant (b = 0.670, SE = .196, t = 3.425, p = .001) with a standardized regression coefficient of .146.
Self-Classified Weight
Although Self-Classified Weight was related to increases in depression symptoms (B = .004, SE = .002, t = 2.728, p = .006), ADHD symptoms were not related to Self-Classified Weight (B = .867, SE = .318, t = 1.541, p = .123). Thus, the indirect effect of ADHD symptoms on depression symptoms through Self-Classified Weight was not significant with confidence intervals including zero (LCL = −.001; UCL = .010). ADHD and depression symptoms remained related (B = −.206, SE = .025, t = 8.247, p < .001).
Covariates
Gender differences were present in all mediation models (see Table 4). Although ADHD and depression symptoms were not significantly different in any of the models, women reported significantly more negative body image on all constructs compared with men. Compared with men, women evaluated their appearance more negatively (B = −.214, p = .002), placed more value on their appearance (B = −.329, p < .001), reported more problems being preoccupied with being overweight (B = −.765, p < .001), identified themselves as being more overweight than men (B = −.219, p < .001), and were less satisfied with their body (B = −.179, p = .004). Given the strong gender differences in body image, follow-up analyses were conducted where gender was included as a moderator of the link between ADHD and body image. None of these models supported the moderating effect of gender.
Effect of Covariates on Variables of Interest.
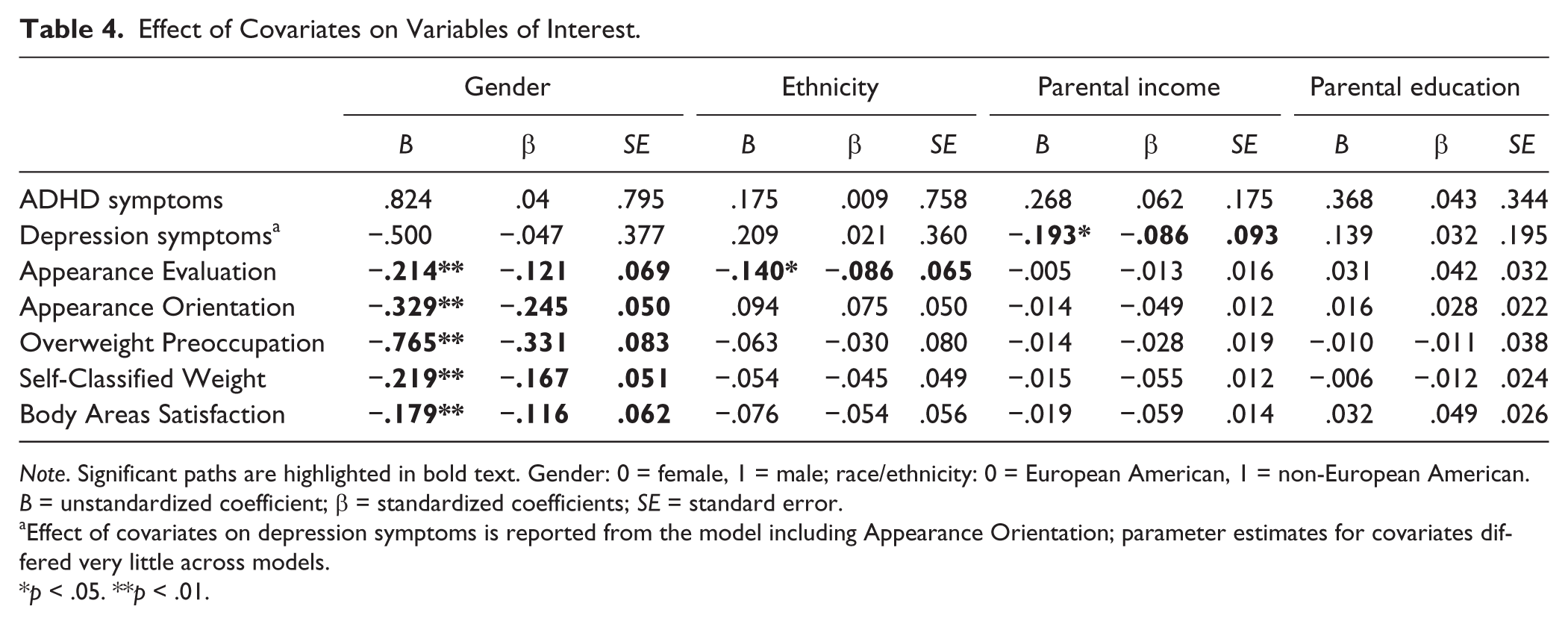
Note. Significant paths are highlighted in bold text. Gender: 0 = female, 1 = male; race/ethnicity: 0 = European American, 1 = non-European American. B = unstandardized coefficient; β = standardized coefficients; SE = standard error.
Effect of covariates on depression symptoms is reported from the model including Appearance Orientation; parameter estimates for covariates differed very little across models.
p < .05. **p < .01.
Ethnicity was significantly related to Appearance Evaluation, where European Americans reported more negative evaluation of their appearance than non-European Americans (B = −.140, p = .031). Also, young adults from families with less parental income reported higher depression symptoms (B = −.193, p < .001).
Additional analyses
We tested the assumption that the mediators did not function better as moderators (MacKinnon, 2008; VanderWeele & Vansteelandt, 2010) by adding the interaction of ADHD symptoms with each body image construct serving as a mediator in predicting the depression symptoms. None of the interaction terms were significant, and no meaningful changes in results were found.
We also tested identical models where ADHD symptoms and depression symptoms were dichotomized above and below the diagnostic threshold. The effect sizes and statistical significance of these models were similar to the reported results where continuous variables of ADHD and depression symptoms were used.
Discussion
The current study identified that body image plays a significant role in increased risk for depression symptoms as ADHD symptoms increase. College students evaluated their physical appearance more poorly, experienced more concern about being overweight, and were less satisfied with their body as ADHD symptoms increased. As college students expressed less positivity about their body image, depression symptoms increased. Negative body image accounted for a small but significant proportion of the link between ADHD and depression symptoms for college students.
These findings are important given that only two other studies to date have assessed how body image relates to ADHD symptoms. Findings from the current study demonstrated some consistencies with Mikami and colleagues (2008, Mikami et al., 2010) in that we identified a significant association between ADHD symptoms and body dissatisfaction. We extended these findings by demonstrating that preoccupation with being overweight and evaluating one’s body negatively were also associated with ADHD symptoms and all three body image constructs contributed to the increased rate of depression symptoms associated with ADHD symptoms. These findings are consistent with research demonstrating that depression symptoms are closely associated with negative body image (Markowitz et al., 2008; Stice, 2002).
Given extensive literature demonstrating that body image and depression symptoms together contribute to the onset and maintenance of eating disorders (Spoor et al., 2006; Stice & Bearman, 2001), future research should evaluate the role that body image plays in the association between ADHD symptoms and eating disorders. Current research suggests that ADHD symptoms increase risk for bulimia (Biederman et al., 2007; Mikami et al., 2010; Mikami et al., 2008) and ADHD symptoms may increase binge-eating disorders as well. The combined effect of both ADHD and depression symptoms on binge-eating and bulimia behaviors remains unexplored. Furthermore, the role of body image related to depression symptoms specifically for youth with ADHD symptoms also remains unevaluated.
Body image and depression symptoms may place youth with ADHD symptoms at risk for disordered eating through engagement in dietary restraint as youth pursue the cultural ideal of a thin physique (Stice & Shaw, 1994). Body dissatisfaction, negative evaluation of one’s physique, and preoccupation with being overweight are strong risk factors for dietary restraint (Stice & Shaw, 1994). Unfortunately, reducing caloric intake can reduce serotonin levels (Attenburrow et al., 2003). Given that release of serotonin in the hypothalamus triggers satiety and de-motivates food intake, lower levels of serotonin may leave an individual with physical fatigue and weakened interoceptive cues to stop eating, contributing to binge-eating behavior (Chandler-Laney et al., 2007). This cycle may occur in addition to the increased risk for binge-eating from impulsive behavior that characterizes ADHD symptoms. In addition to researching degree to which ADHD symptoms are related to dietary restraint, further research should identify the function that body image serves in depression symptoms, dietary restraint, and eating disorders symptoms for youth with ADHD symptoms.
Although women demonstrated higher rates of negative body image, gender did not interact with body image or ADHD symptoms in any of the mediation models. These findings suggest that female as well as male college students experience susceptibility for negative body image as ADHD symptoms increase. Furthermore, body image appears to influence depression symptoms for both male and female college students. These results are consistent with research demonstrating that adolescent and young adult men demonstrate concerns with body image regarding weight and shape (Cafri, Olivardia, & Thompson, 2008; Olivardia, Pope, Borowiecki, & Cohane, 2004) and that these concerns contribute to depression symptoms for young adult men just as they do for women (Cafri et al., 2008; Cash, Theriault, & Annis, 2004). Young men may have specific concerns about their upper body muscularity (Olivardia et al., 2004), which this study did not assess. Future research should provide enhanced description of specific body image concerns that young men with ADHD symptoms may experience. Importantly, this study demonstrated that even at a general level, young men with ADHD symptoms experience increased body image concerns that are associated with depression symptoms.
Future research should evaluate gender differences in the function of body image in increasing risk for depression symptoms and eating disorder behavior for young adults with ADHD symptoms. Although negative body image may lead young women with ADHD symptoms to engage in dieting and dietary restraint behaviors, young men with ADHD symptoms may engage in body building or overindulge in exercise in pursuit of cultural ideals of male attractiveness.
Other covariates also played an interesting role in the analyses. The finding that non-European Americans had higher Appearance Evaluation is consistent with some previous research findings (Fitzsimmons-Craft & Bardone-Cone, 2012). Also consistent with previous research, decreases in childhood household income were associated with increased depression symptoms (Quesnel-Vallée & Taylor, 2012).
Strengths and Limitations
Despite the strengths of this study, limitations were present. First, our sample was cross-sectional, which limits evaluation of directional associations (MacKinnon, 2008; Maxwell & Cole, 2007). For example, depression symptoms could have preceded body image and led to increased negative perceptions and evaluations of one’s physicality. However, little to no research has evaluated body image for young adults with ADHD symptoms and the relation between depression symptoms and body image at different levels of ADHD symptoms. Thus, cross-sectional analyses provide an opportunity to consider a potentially important explanation for factors that contribute to and maintain depression symptoms for this population.
Second, ADHD symptoms were measured continuously rather than with diagnosis. Although examining symptoms on a continuum may capture some individuals with transient attention problems unrelated to ADHD, measuring ADHD dimensionally has many advantages. Evidence supports that ADHD symptoms are best represented on a continuum of symptom severity rather than with discrete diagnosis (Marcus & Barry, 2011). Dichotomized continuous variables have well-known methodological shortcomings that would have limited the statistical validity of our findings (MacCallum, Zhang, Preacher, & Rucker, 2002). Subthreshold ADHD symptom severity may also affect problems with body image and depression symptoms in ways that would not be visible if diagnosis rather than symptom severity was used.
Third, this study used all self-reported measures, which is a frequently-used measurement approach in research on ADHD, depression, and body image. Self-report of ADHD symptoms corresponds closely with parent and spousal report for young adults (Barkley et al., 2011; Barkley et al., 2008). Furthermore, disclosure of sensitive thoughts and behaviors in general is highest when self-report is used and when it is collected in an anonymous, confidential online format rather than a face-to-face interview (Kobak et al., 1997; Tourangeau & Smith, 1996), as done in this study.
Summary and Clinical Implications
Little research has addressed how body image relates to ADHD symptoms or the potential role that body image may play in depression symptoms for young adults with ADHD symptoms. Despite the cross-sectional design of this study, these results indicate that negative body image is associated with increased depression symptoms for young adults with ADHD symptoms. These findings suggest that young adults with both ADHD and depression symptoms may benefit from working with their clinicians to evaluate their perceptions of body image. These youth may also benefit from prevention and intervention programs that target healthy attitudes about one’s physique, appearance, eating habits, and physical activity habits. Clinicians working with young adults with ADHD symptoms should aid youth in building accurate and positive perceptions regarding their physical appearance. Youth with ADHD symptoms may also experience enhanced susceptibility to peer and media influences on behavioral and appearance-related expectations (e.g., see Van Eck, Markle, Dattilo, & Flory, 2014). As youth work with their clinicians to improve accuracy in assessing their own physical appearance, they may also benefit from considering how external feedback influences their perceptions of themselves. For example, a dissonance prevention approach, where youth participate in activities designed to challenge the value and healthfulness of maintaining a thin physique, was designed to engender discomfort regarding dietary restraint and body dissatisfaction (see Stice, Marti, Spoor, Presnell, & Shaw, 2008). This approach has shown effectiveness in helping youth to reduce dieting behavior and eating disorder symptoms, as well as to improve body image up to 3 years following intervention exposure (Stice, Rohde, Gau, & Shaw, 2009). Given the findings of this study, young adults with ADHD symptoms may also benefit from such a program and future research should explore this possibility.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.