
Abstract
OBJECTIVE. We sought to develop and provide preliminary validation for a questionnaire evaluating functioning related to ADHD (i.e., the FX-II) with a particularly underserved group (i.e., Mexican youth). METHOD. 191 Mexican raters completed the FX-II alongside measures of ADHD symptoms, impairment, cultural values, and demographics: 127 raters were caregivers of treatment-naïve youth (i.e., community sample); 32 raters were caregivers and 32 raters were teachers of youth participating in a school-based program for attention/behavior concerns (i.e., clinical sample). RESULTS. We created the 52-item FX-II Scale by adapting a culturally appropriate and psychometrically sound measure of impairment (i.e., the ADHD-FX) to assess functioning most relevant to Spanish-speaking families of children with ADHD (i.e., academic, social/emotional, and familial functioning). The FX-II demonstrated strong reliability, convergent and divergent construct validity, and predictive validity. CONCLUSION. The FX-II appears to be a beneficial tool for evaluating functioning related to ADHD in Mexican children and future validation efforts in broader populations are warranted.
ADHD is considered an “equal opportunity condition” affecting 5% to 10% of youth across the globe (American Psychiatric Association [APA], 2013; Faraone et al., 2015; Faraone, Sergeant, Gillberg, & Biederman, 2003; Hinshaw & Scheffler, 2014; Willcutt, 2012). To substantiate an ADHD diagnosis, a child must demonstrate evidence of inattention and/or hyperactivity-impulsivity symptoms interfering with and/or reducing the quality of functioning in at least two settings (APA, 2013). Areas commonly affected by childhood ADHD symptoms include academic, social/emotional, and familial functioning (APA, 2013; DuPaul, 2007; Hoza, 2007; Johnston & Mash, 2001; Pelham, William, Fabiano, & Massetti, 2005; Sasser, Schoenfelder, & Stein, 2017).
In addition to serving as diagnostic criteria, difficulties in functioning increase the likelihood that families recognize problems in their children and subsequently seek professional help, especially among ethnic minority populations (Bussing, Zima, Gary, & Garvan, 2003; Power, Eiraldi, Clarke, Mazzuca, & Krain, 2005; Reardon et al., 2017). Thus, experts have called for the development of practical tools to help parents identify child mental health problems and their meaningful impact (Reardon et al., 2017). Use of such tools in outreach and screening efforts could facilitate the help-seeking process for ADHD treatment across diverse groups (Haack & Gerdes, 2011; Reardon et al., 2017).
Furthermore, randomized controlled trials (RCTs) of ADHD treatment consistently demonstrate improvements in academic, social/emotional, and familial functioning (Evans, Owens, & Bunford, 2014; Pfiffner & Haack, 2014), implicating these domains as important in treatment outcome research. Interestingly, ADHD treatment outcome domains appear partially distinct from one another (Karpenko, Owens, Evangelista, & Dodds, 2009), such that a substantial minority of children may show improvement in functioning but not symptoms (Owens, Johannes, & Karpenko, 2009). Thus, investigation of functioning related to ADHD is warranted throughout the ADHD treatment process, spanning the stages of outreach, initial assessment, planning, progress monitoring, and outcome evaluation (Eraldi, Mazzuca, Clarke, & Power, 2006; Owens et al., 2009; Pelham et al., 2005; Sasser et al., 2017).
The evaluation of functioning related to ADHD is important for all families, but it appears particularly relevant when working with culturally diverse families, such as Spanish-speaking Latinos (Haack & Gerdes, 2011). To begin, Latino families often lack exposure to and comfort with psychodiagnostic terminology, such as description of symptomotology (Gerdes, Lawton, Haack, & Schneider, 2014; Haack & Gerdes, 2011; Rothe, 2005). Indeed, research suggests that Latino families may underrecognize ADHD symptoms (especially hyperactivity-impulsivity) as present and/or concerning compared with clinicians or teachers (Arcia & Fernández, 2003; Schmitz & Velez, 2003). In contrast, recognition of impairment in functioning appears less susceptible to cultural bias (Gerdes, Lawton, Haack, & Hurtado, 2013). Thus, guidelines for culturally appropriate ADHD assessment emphasize evaluation of functioning in addition to symptoms (Haack & Gerdes, 2011; Rothe, 2005).
Unfortunately, the availability of culturally appropriate, validated tools measuring ADHD functioning is limited, especially in Spanish (Haack & Gerdes, 2011). This may contribute to the unfortunate disparities in ADHD diagnosis and service utilization for youth of Spanish-speaking families in the United States and Latin America (APA, 2013; De la Peña, Ortiz, & Pérez, 2010; Flores & Tomany-Korman, 2008). In response, Haack, Gerdes, Lawton, and Schneider (2014) created the ADHD-FX: a brief measure designed to assess impairment in academic, social, and familial functioning. The ADHD-FX initially was developed with a specific at-risk and underserved population in mind (i.e., Spanish-speaking Latino parents; Haack et al., 2014). Briefly, Spanish-speaking, Latino parents/caregivers were asked to describe and identify behaviors after viewing a silent video depicting a child with ADHD. Thirty-two items were derived for the ADHD-FX based on the most common parent responses. The ADHD-FX demonstrated good psychometric and cultural properties with a distinct sample of Latino parents, as evidenced by high internal consistency, significant correlations with theoretically related measures of ADHD symptoms and impairment, and insignificant correlations with measures of cultural values (Haack & Gerdes, 2017). Importantly, subsequent validation efforts have suggested that the ADHD-FX is a reliable and valid measure for parents/caregivers and teachers to assess functional impairment related to ADHD in community and clinical populations across cultures (Haack, Gonring, Harris, Gerdes, & Pfiffner, 2016).
Efforts to adapt the ADHD-FX scale for assessment of functioning rather than impairment appear warranted for several reasons. To begin, in 2013, the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) altered ADHD diagnostic criteria from “clear evidence of clinically significant impairment in social, academic, or occupational functioning” to “ . . . clear evidence that the symptoms interfere with, or reduce the quality of, social, academic, or occupational functioning” (APA, 2000, 2013). Thus, assessment of functioning now is necessary to warrant an ADHD diagnosis. Furthermore, items evaluating functioning can be directly translated into positively framed treatment goals. For example, if a child reportedly rarely concentrates on completing schoolwork, “concentrating on completing schoolwork” can be targeted on a daily report card and monitored throughout treatment.
In addition to clinical rationale described above, evaluation of functioning rather than impairment may be preferred for practical and cultural reasons. To begin, impairment questions frequently contain “double-negatives” which can be confusing for raters, especially when questions are in Spanish. For example, a rater may have less difficulty rating how often a child completes schoolwork compared with rating how often a child does not complete schoolwork.
Finally, evaluating functioning rather than impairment may be more acceptable to parents, especially Latinos who tend to display collectivistic values such as simpatia, or the emphasis on pleasant interpersonal relationships and familismo, or the emphasis on family loyalty and interconnectedness (Bauermeister, 2005; Bernal & Domenech Rodríguez, 2009; Flores, 2000; Rothe, 2005). For example, a mother may feel uncomfortable or disrespectful describing that her child usually “does not get along with others” but may feel more comfortable describing that her child sometimes “gets along with others.” Taken together, evaluation of functioning related to ADHD is supported by clinical, practical, and cultural rationale.
Current Study
We sought to develop and provide preliminary validation for a measure assessing domains of functioning typically affected by ADHD (i.e., academic, social/emotional, and familial domains) with a particular underserved group (i.e., Mexican youth). Specifically, we first aimed to adapt an existing culturally appropriate and psychometrically sound measure of functional impairment related to ADHD (i.e., the ADHD-FX; Haack & Gerdes, 2017; Haack et al., 2014; Haack, Villodas, McBurnett, Hinshaw, & Pfiffner, 2016) to focus on functioning. Next, we aimed to provide preliminary validation for the new measure (named the FX-II) with 191 Mexican raters: 127 raters were parents/caregivers of treatment-naïve youth (i.e., community sample); 32 raters were parents/caregivers and 32 raters were teachers of youth participating in a school-based service program for attention/behavior concerns (i.e., clinical sample). We predicted that each theoretical subscale and the overall FX-II would demonstrate:
Reliability, as evidenced by internal consistency via Cronbach’s alpha values >.70;
Convergent construct validity, as evidenced via significant correlations with theoretically related ADHD measures completed by parents/caregivers and teachers (i.e., the Child Symptom Inventory [CSI; Gadow & Sprafkin, 1997], the Behavior Rating Inventory of Executive Function [BRIEF; Gioia, Isquith, Guy, & Kenworthy, 2000], and the ADHD-FX [Haack & Gerdes, 2017; Haack et al., 2014; Haack et al., 2016]);
Divergent construct validity, as evidenced by insignificant correlations with measures of cultural values (i.e., Mexican American Cultural Values Scale for Adolescents and Adults [MACV; Knight et al., 2010]) and demographic factors completed by parents/caregivers and teachers; and
Predictive validity, as evidenced by significant discriminant analyses of FX-II ratings differentiating community versus clinical group status.
Method
Participants
Community sample
The community sample participants in this study included parents/caregivers of mental health treatment naïve children recruited from four public elementary schools in Culiacán, Sinaloa, Mexico (n = 127). Briefly, raters primarily included women (91%) with varied socioeconomic backgrounds; mean age was 35.28 years (SD = 7.63). Children were predominantly boys (63%) in first to second grade (range = 1st through 6th grade). See Table 1 for more complete demographic information.
Demographic Information.
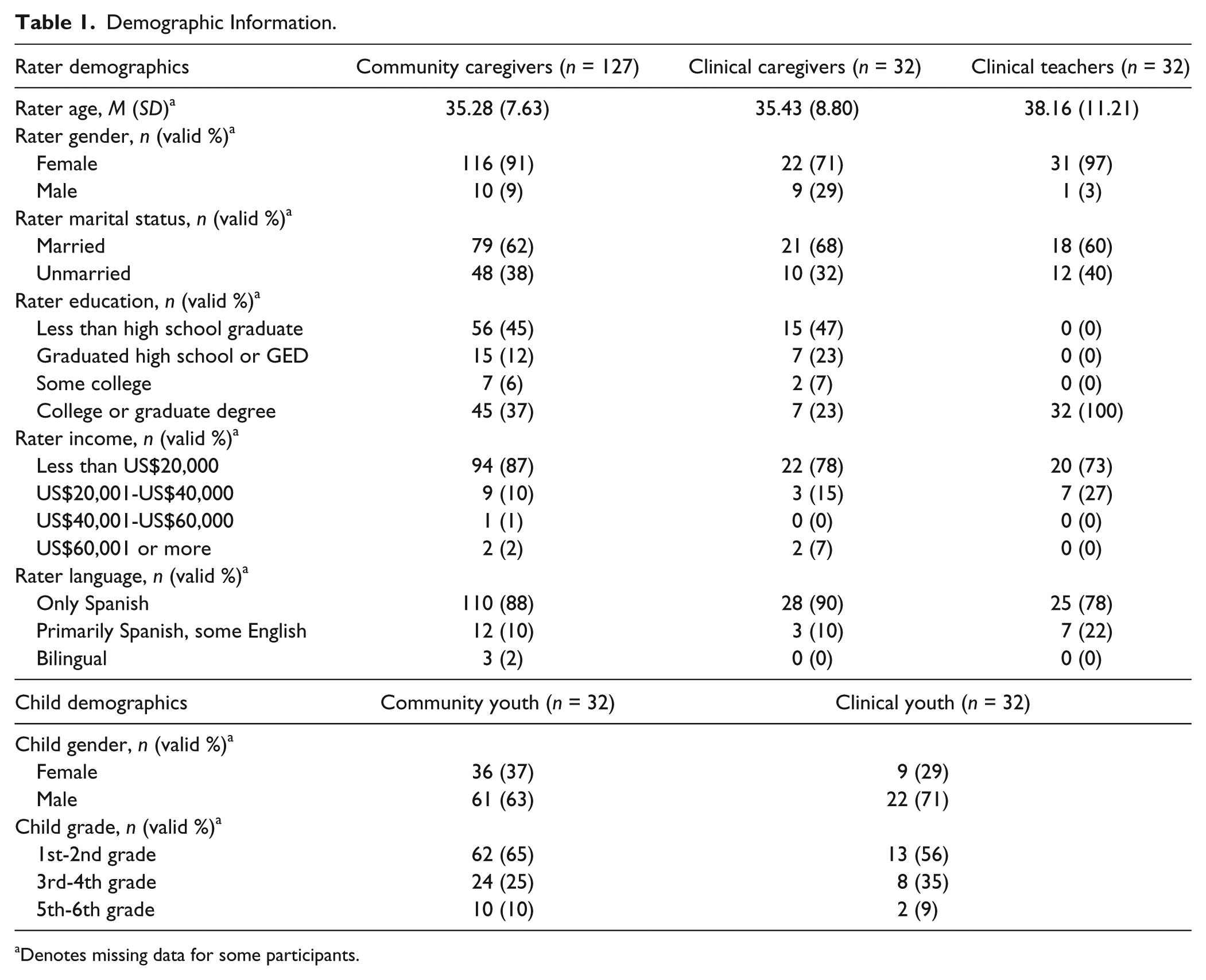
Denotes missing data for some participants.
Clinical sample
The community sample participants included parents/caregivers and teachers of 32 children at each of the four elementary schools participating in a trial of school-based treatment for attention and behavior concerns (n = 32 parents/caregivers and n = 32 teachers; N = 64 total; Haack, Araujo, & Pfiffner, 2017). To be included in the study, parents/caregivers or teachers of youth needed to identify at least six symptoms of inattention and/or hyperactivity-impulsivity on the CSI (Gadow & Sprafkin, 1997) as occurring often or very often (i.e., 2 or 3 on the 4-point, 0-3 scale) and at least one impairment item on the Impairment Rating Scale (IRS; Fabiano et al., 2006) as 3 or higher on a 7-point scale. Briefly, parents/caregivers primarily included women (71%) with varied socioeconomic backgrounds; mean age was 35.43 years (SD = 8.80). All but one teacher was female; mean age was 38.16 (SD = 11.21). Children were predominantly boys (71%) in first to second grade (range = 1st to 5th grade). See Table 1 for more complete demographic information regarding the raters and youth in the clinical and community samples.
Procedure
Community sample
Approximately 1 week before data collection, parents/caregivers in the participating elementary schools received a flyer inviting them to meet the clinical research team and participate in a research study about help seeking for attention and behavior concerns. Meetings occurred at the school and lasted approximately 2 hrs. After the informed consent process (approved by ethics boards at SOURCE MASKED FOR BLIND REVIEW), participants viewed a silent video depicting a child with attention and behavior concerns (i.e., the Behavioral Impairment Video [BIV]; Haack et al., 2014). Next, participants completed a series of paper-and-pencil questionnaires about the child in the video. Relevant to the current study, participants were instructed to select one of their own children between the ages of five and 12 to serve as the subject for subsequently completed child behavior questionnaires. Finally, participants completed measures about their own cultural values and demographic history. Participants also were informed about an RCT of school-based treatment for child attention and behavior problems occurring at their school; they were encouraged to speak to the clinical research staff if they desired more information about participating in the trial.
Clinical sample
As part of the initial trial screening procedure, parents/caregivers and teachers completed a series of questionnaires assessing child behavior and family functioning. If parents/caregivers had already participated in the community sample procedure, their data were removed from the community sample and they were asked to complete the measures of child behavior again to ensure a recent assessment of functioning.
Measures
Child Symptom Inventory (CSI-4)
This measure completed by parents/caregivers and teachers contains items corresponding to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) symptoms rated on a 4-point scale (0 = never to 3 = very often; Gadow & Sprafkin, 1994). Symptoms are considered to be present when they are rated as occurring often or very often (i.e., 2 or 3 on the 4-point, 0-3 scale). The English and Spanish versions of the CSI-4 have normative data, acceptable test–retest reliability, and acceptable predictive validity for categorical diagnosis of ADHD and ODD (Gadow & Sprafkin, 1997).
BRIEF
This measure completed by parents/caregivers and teachers contains 86 items assessing executive function in children and adolescents between 5 and 18 years old (Gioia et al., 2000). It rated on a 3-point scale (1 = never to 3 = often). The items form eight clinical scales (Inhibition, Shift, Emotional Control, Initiate, Working Memory, Plan/Organize, Organization of Materials, and Monitor), two validity scales, and all of them form three broader indexes (Conduct Regulation, Metacognition, and a Global Executive Composite). High scores on any index indicate poor executive functioning. The BRIEF demonstrates strong psychometric properties in English and Spanish (García Fernández, González-Pienda, Rodríguez Pérez, Álvarez García, & Álvarez Pérez, 2014; Gioia et al., 2000).
ADHD-FX
This measure completed by parents/caregivers and teachers contains 32 items assessing academic, social, and home impairment rated on a 4-point scale (0 = not at all to 3 = a lot; Haack et al., 2014). The ADHD-FX has demonstrated high levels of internal consistency, test–retest reliability, convergent construct validity, and universal cultural properties (Haack & Gerdes, 2017; Haack et al., 2016). The internal consistency of the ADHD-FX for the current study was good (Cronbach’s alpha values ranging from .96 to .98).
MACV
This measure completed by parents/caregivers and teachers is a 50-item self-report questionnaire used to measure cultural value orientations in terms of Mexican values and mainstream American values, which is available in Spanish and English (Knight et al., 2010). Items are rated as not at all (1) to completely believe (5). The Mexican values scale is made up of several subscales, including Familism, Respect, Religion, and Traditional Gender Roles. The American values scale is made up of three subscales including Material Success, Independence/Self-Reliance, and Competition/Personal Achievement. Strong internal consistency reliability coefficients have been established for the Mexican values scale (.88), the American values scale (.81-.84), as well as the individual subscales (.50-.86). The MACV also has been shown to have good construct validity and to discriminate between immigrant and nonimmigrant Latinos (Knight et al., 2010).
Demographic Form
Demographic history was obtained about participating parents/caregivers and teachers and chosen children from the Demographic Form. Questions regarding the parent/caregiver include occupation, education level, and household income. Questions regarding the child include age, gender, grade, and mental health diagnosis and treatment history.
Results
Development of FX-II Scale
We developed the FX-II scale in a multistep procedure. First, we redesigned the 32 ADHD-FX items to focus on functioning rather than impairment. Specifically, instead of asking how much negative behaviors affect the child (i.e., 0 = not at all, 1 = a little, 2 = quite a bit, and 3 = a lot), the FX-II items ask how often a child displays positive behaviors (i.e., 0 = rarely, 1 = sometimes, 2 = usually, and 3 = almost always). We avoided double-negative phrasing in the development of FX-II items. For example, instead of asking how much the behavior “doesn’t express and/or show his/her feelings in an appropriate way” affects the child, the FX-II inquires how often the child “use(s) self-control to manage and express feelings effectively and appropriately.”
Next, we developed six new functioning items based on problems and improvements commonly identified in prior qualitative research with Spanish-speaking Latino families receiving school-based services for attention and behavior concerns (Haack & Pfiffner, 2016; Haack, Araujo, Beaulieu, & Pfiffner, 2017). For example, given that “child is behind academically/low grades” was a commonly identified problem by Latino parents/caregivers, an item inquiring if the child “perform(s) at grade level and keep(s) up with the rest of the class (in reading, writing, and/or lecture)” was created. In addition, given that “child responds to Daily Report Card classroom behavior system” was a commonly identified improvement by Latino parents/caregivers, the item “stay(s) motivated to follow expectations in order to achieve a result (e.g., praise, points, and/or rewards)” was developed.
Prior qualitative research with Latino parents/caregivers receiving school-based services for attention and behavior concerns (Haack & Pfiffner, 2016; Haack, Araujo, Beaulieu, & Pfiffner, 2017) also identified that improvement in parent/caregiver and teacher ADHD management strategies, as well as others’ acceptance and support of the child, contributed to improvement in child functioning. Subsequently, we developed nine items for the FX-II assessing how often parents/caregivers/teachers support the child and four items assessing how often others support the child. For example, given that “effectively provides rewards to child” was a commonly identified improvement by Latino parents/caregivers receiving services, the item “praise(s) or reward(s) this child for following through on rules and expectations” was developed. These items could be particularly beneficial in treatment outcome research investigating mechanisms of change, as improvements in parenting mediate child outcomes in psychosocial treatment for ADHD (Chronis-Tuscano et al., 2011; Haack, Villodas, McBurnett, Hinshaw, & Pfiffner, 2017; Hinshaw, Owens, & Wells, 2000).
Finally, given that etiological beliefs are particularly salient for ADHD problem recognition in ethnic minority families, such as Latinos (Eraldi et al., 2006; Reardon et al., 2017), one item regarding beliefs about causes was created. Specifically, raters are asked to identify beliefs about physical/biological/genetic causes, causes related to the family, causes related to the school, causes related to the child’s personality or characteristics, causes related to American culture or adjusting to a new culture, causes related to the environment or disharmony with nature, causes related to the influence of the child’s friends, spiritual or religious causes, causes related to trauma, causes related to relationships and interactions, or other causes.
The final FX-II contains 52 items assessing academic, social-emotional, and familial functioning, as well as caregiver/teacher and other’s support of the child, and the rater’s etiological beliefs. Items 1 to 24 make up the Academic Functioning subscale. Items 3, 5, 7, 8, 12, 14, 16, 18, 20, and 22 make up the Social/Emotional Functioning subscale. Items 25 to 38 make up the Familial Functioning subscale. Items 40 to 48 make up the Caregiver/Teacher Support subscale, and Items 49 to 52 make up the Other Support subscale. The Functioning and Support subscale items are rated on a 0 to 3 Likert-type scale (0 = rarely, 1 = sometimes, 2 = usually, and 3 = almost always). Item ratings can be averaged for a Total Functioning mean score, Functioning Subscale mean scores, and Support Subscale mean scores, with higher mean scores indicating better functioning/support. Item 39 represents the Etiology subscale, which can be used to examine a frequency and valid percentage of raters endorsing each cause; note that each rater can endorse multiple causes.
Preliminary Analyses
We present descriptive statistics for the FX-II Total Functioning, Functioning subscales, and Support Subscales in Table 2. We also present the frequency and valid percentage of raters endorsing each cause on the Etiology subscale item. Mean scores for the FX-II Total Functioning and Academic, Social/Emotional, and Familial Functioning subscales ranged between 2.15 and 2.22 out of “3” when rated by community sample parents/caregivers, between 1.40 and 1.56 out of “3” when rated by clinical sample parents/caregivers, and between 0.85 and 1.27 out of “3” when rated by clinical sample teachers. Mean scores for the FX-II Caregiver/Teacher Support and Other Support subscales ranged between 2.08 and 2.50 out of 3 across samples. The most common Etiology subscale item endorsements were “causes related to the family” (endorsed by 71% of community sample parents/caregivers, 63% of clinical sample parents/caregivers, and 67% of clinical sample teachers), “causes related to the child’s personality or characteristics” (endorsed by 56% of community sample parents/caregivers, 63% of clinical sample parents/caregivers, and 77% of clinical sample teachers), followed by “physical/biological/genetic causes” (endorsed by 43% of community sample parents/caregivers, 52% of clinical sample parents/caregivers, and 43% of clinical sample teachers) and “causes related to the school” (endorsed by 40% of community sample parents/caregivers, 37% of clinical sample parents/caregivers, and 16% of clinical sample teachers).
Descriptive Statistics and Internal Consistency of FX-II Scale and Subscale Ratings Across Samples.
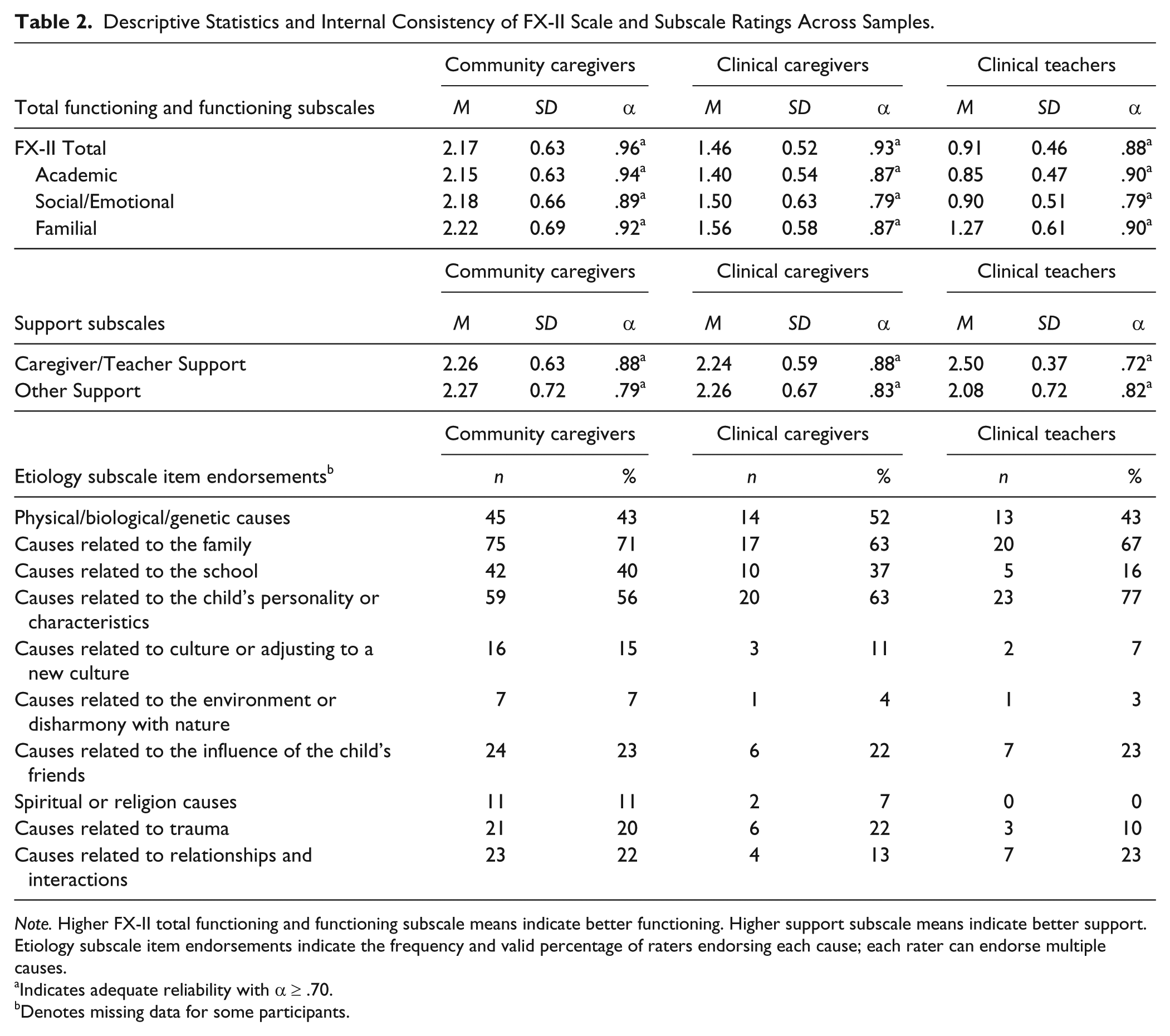
Note. Higher FX-II total functioning and functioning subscale means indicate better functioning. Higher support subscale means indicate better support. Etiology subscale item endorsements indicate the frequency and valid percentage of raters endorsing each cause; each rater can endorse multiple causes.
Indicates adequate reliability with α ≥ .70.
Denotes missing data for some participants.
Reliability
We predicted the overall FX-II Total scale and functioning/support subscales would demonstrate reliability via internal consistency (i.e., Cronbach’s alpha values ≥.70). All functioning/support subscales and the overall FX-II revealed adequate internal consistency levels with Cronbach’s alpha values ranging from .72 to .96 (see Table 2). Examination of item-total statistics did not suggest that deleting any individual items would improve the internal consistency of the overall measure or subscales.
Convergent Construct Validity
We predicted the overall FX-II and functioning/support subscales would demonstrate convergent construct validity via correlations with theoretically related measures completed by parents/caregivers and teachers (i.e., CSI; Gadow & Sprafkin, 1997, BRIEF; Gioia et al., 2000, and ADHD-FX; Haack & Gerdes, 2014; Haack et al., 2014; Haack et al., 2016). All functioning/support subscales (with the exception of the Caregiver/Teacher Support subscale) and the overall FX-II revealed adequate convergent construct validity with correlation values ranging from .16 to .79 (see Table 3).
FX-II Scale and Subscale Convergent Construct Validity.
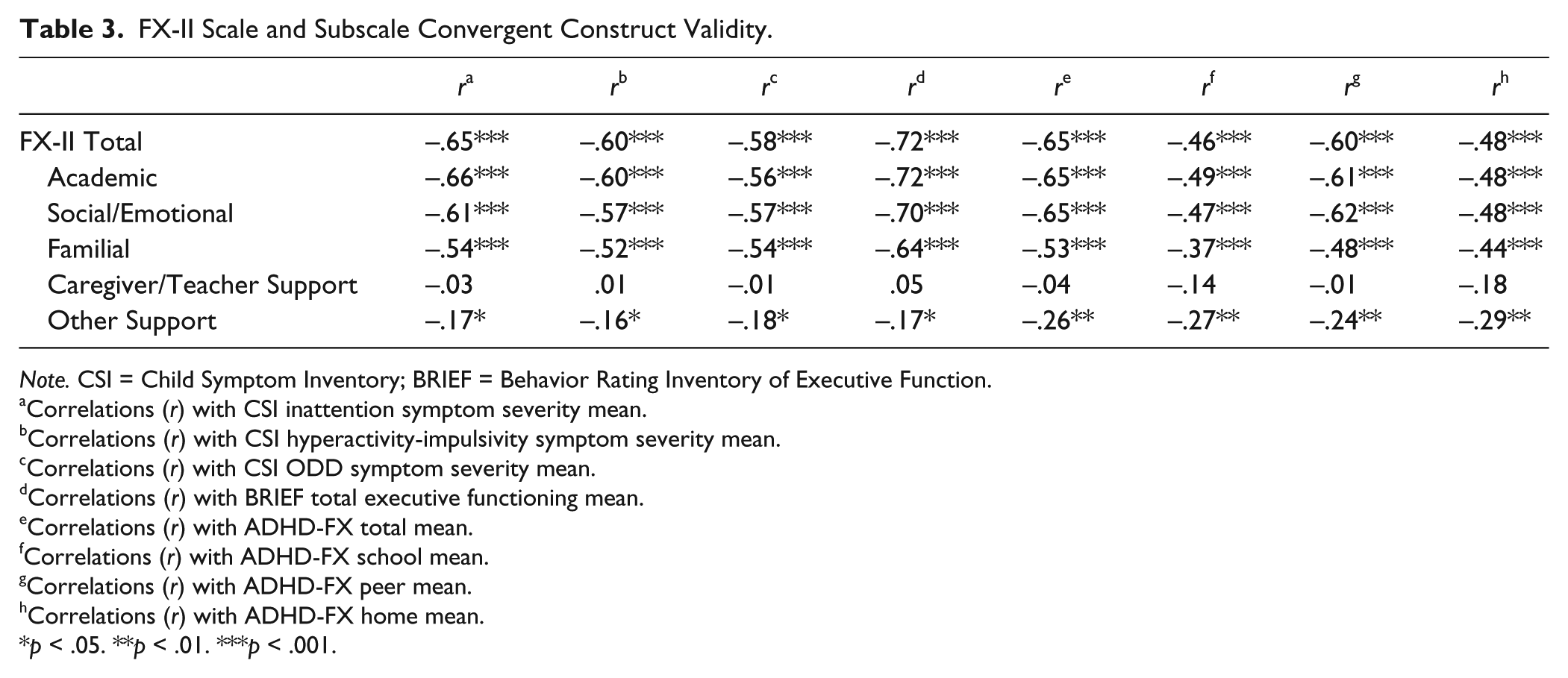
Note. CSI = Child Symptom Inventory; BRIEF = Behavior Rating Inventory of Executive Function.
Correlations (r) with CSI inattention symptom severity mean.
Correlations (r) with CSI hyperactivity-impulsivity symptom severity mean.
Correlations (r) with CSI ODD symptom severity mean.
Correlations (r) with BRIEF total executive functioning mean.
Correlations (r) with ADHD-FX total mean.
Correlations (r) with ADHD-FX school mean.
Correlations (r) with ADHD-FX peer mean.
Correlations (r) with ADHD-FX home mean.
p < .05. **p < .01. ***p < .001.
Divergent Construct Validity
We predicted the overall FX-II and each functioning/support subscale would demonstrate divergent construct validity via correlations between the FX-II scale with measures of cultural values (i.e., the MACV; Knight et al., 2010) and demographic factors completed by parents/caregivers and teachers. As seen in Table 4, correlations failed to reach significance with few exceptions. Specifically, the total FX-II and FX-II Academic Functioning subscale were negatively associated with rater income. In addition, the FX-II Caregiver/Teacher Support subscale was positively associated with rater education.
FX-II Scale and Subscale Divergent Construct Validity.
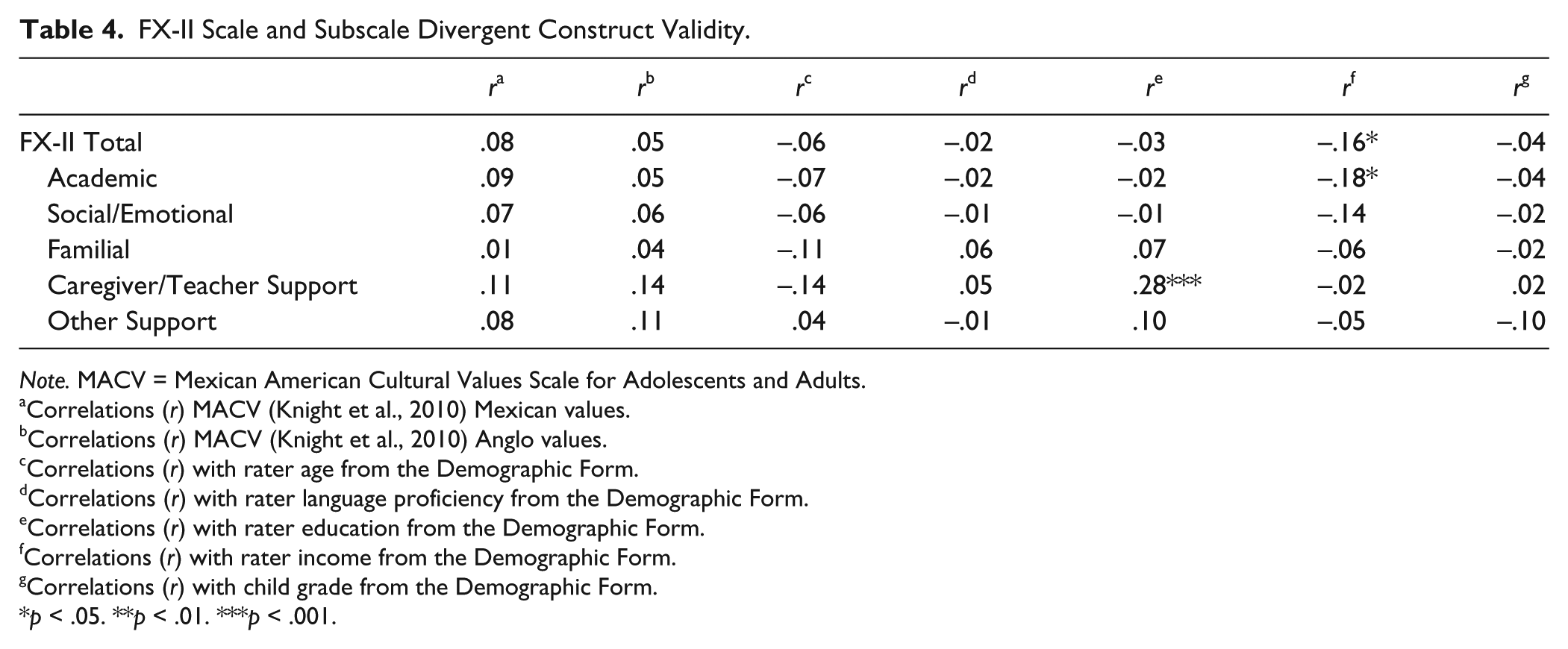
Note. MACV = Mexican American Cultural Values Scale for Adolescents and Adults.
Correlations (r) MACV (Knight et al., 2010) Mexican values.
Correlations (r) MACV (Knight et al., 2010) Anglo values.
Correlations (r) with rater age from the Demographic Form.
Correlations (r) with rater language proficiency from the Demographic Form.
Correlations (r) with rater education from the Demographic Form.
Correlations (r) with rater income from the Demographic Form.
Correlations (r) with child grade from the Demographic Form.
p < .05. **p < .01. ***p < .001.
Predictive Validity
We predicted the overall FX-II and each functioning/support subscale would demonstrate predictive validity via discriminant analysis differentiating youth membership in the community versus clinical sample. When comparing the community sample with the clinical sample caregiver ratings, the discriminant function revealed a significant association between clinical sample group membership and FX-II ratings (Wilks’s λ = .67, p < .001), accounting for 57.90% of the between-group variability (see Table 5). Analysis of the structure matrix revealed that the overall FX-II and the FX-II Academic, Social/Emotional, and Familial Functioning subscale means were significant predictors (structure matrix values > 0.30). The cross-validated classification showed that overall 84.90% of children were correctly classified by the FX-II when rated by community sample parents/caregivers and clinical sample parents/caregivers. When comparing the community sample with the clinical sample teacher ratings, the discriminant function revealed a significant association between clinical sample group membership and FX-II ratings (Wilks’s λ = .47, p < .001), accounting for 73.0% of the between-group variability (see Table 6). Analysis of the structure matrix revealed that the overall FX-II and the FX-II Academic, Social/Emotional, and Familial Functioning subscale means were significant predictors (structure matrix values > 0.30). The cross-validated classification showed that overall 92.4% of children were correctly classified by the FX-II when rated by community sample parents/caregivers and clinical sample teachers.
Predictive Validity via Discriminant Analysis of Community Versus Clinical Sample–Clinical Caregiver Ratings.
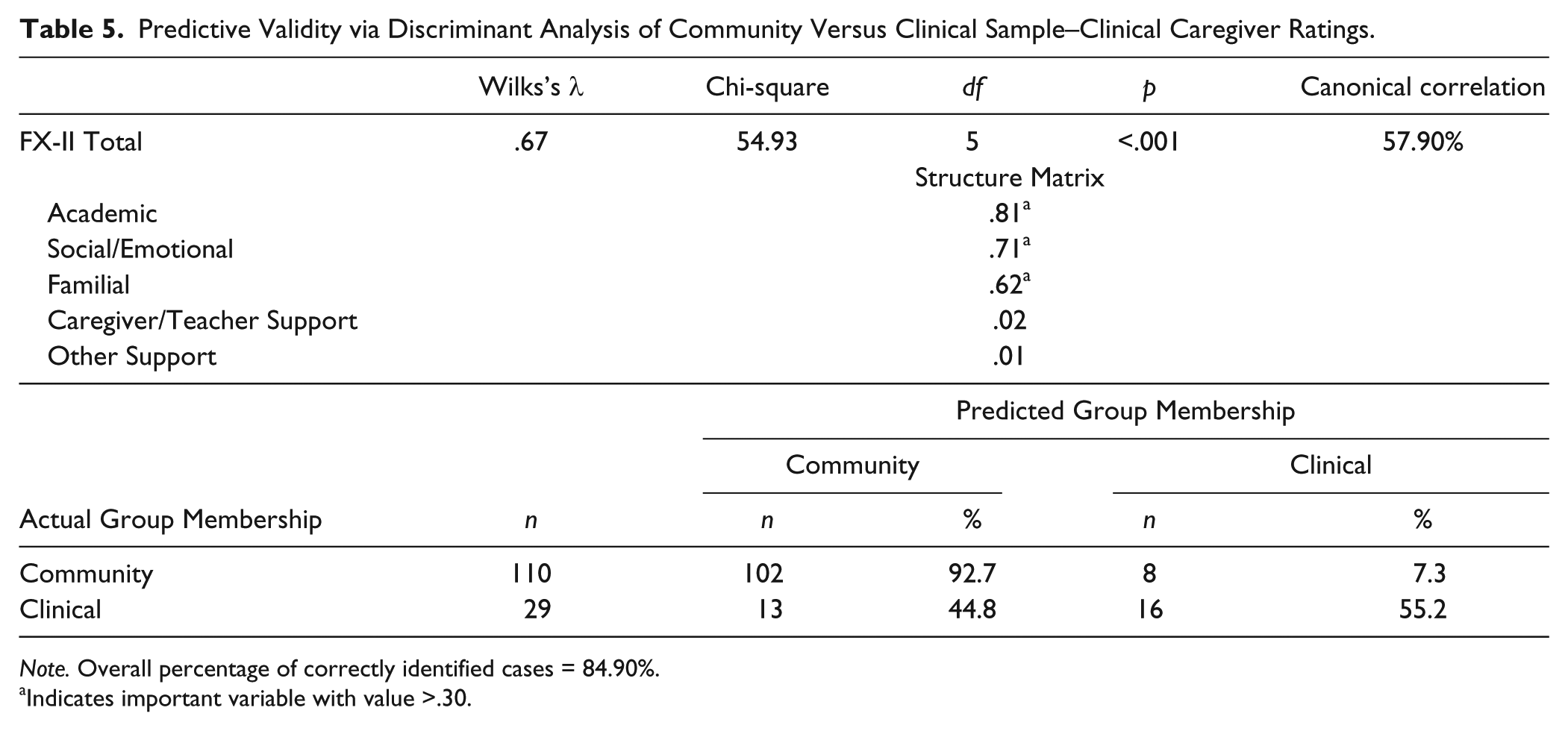
Note. Overall percentage of correctly identified cases = 84.90%.
Indicates important variable with value >.30.
Predictive Validity via Discriminant Analysis of Community Versus Clinical Sample–Clinical Teacher Ratings.
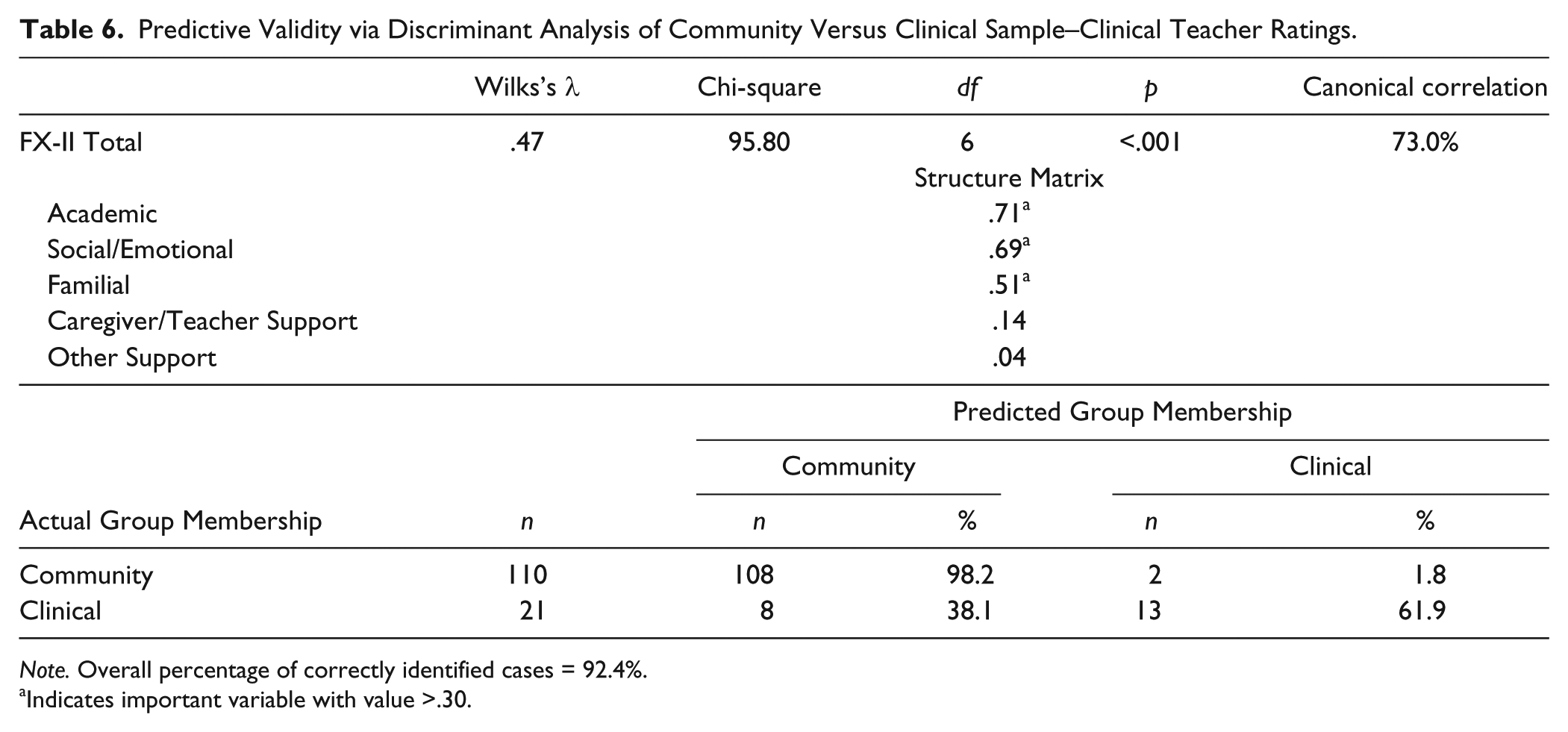
Note. Overall percentage of correctly identified cases = 92.4%.
Indicates important variable with value >.30.
Discussion
Our team developed the FX-II scale by adapting a measure of impairment related to ADHD (i.e., the ADHD-FX scale) to focus on functioning most relevant to Latino youth of Spanish-speaking families. The overall FX-II scale and the Academic, Social/Emotional, and Family Functioning subscales demonstrated strong reliability, construct validity, and predictive validity when completed in Spanish by Mexican parents/caregivers and teachers of school-aged children in community and clinical samples. Thus, preliminary validation results suggest the FX-II scale may be a psychometrically sound and culturally appropriate tool when assessing functioning related to ADHD in Mexican youth and future validation efforts in broader populations are warranted.
The FX-II development process resulted in a 52-item scale assessing academic, social-emotional, and familial functioning, as well as caregiver/teacher and other’s support of the child, and the rater’s etiological beliefs. The scale can be administered to parents/caregivers and teachers in Spanish or English (see Appendix for full scale in English). The brief, comprehensive scale is supported by literature suggesting that ADHD measures of functioning must balance between being easy to administer and providing rich, domain-specific information (Haack & Gerdes, 2011; Sasser et al., 2017).
Examination of preliminary descriptive statistics reveal that the FX-II Total Functioning mean score and the Academic, Social/Emotional, and Familial Functioning subscale mean scores average above “2” out of “3” for youth rated by parents/caregivers in the community sample, compared with less than “2” out of “3” for youth rated by parents/caregivers and teachers in the clinical sample. These findings provide initial evidence for potential clinical cutoff scores to evaluate in future FX-II psychometric studies. In contrast, the FX-II Caregiver/Teacher Support and Other Support subscale mean scores averaged above “2” out of “3” for all youth in the study regardless of the sample. Etiology subscale items endorsed by the majority of raters across samples were “causes related to the family” and “causes related to the child’s personality or characteristics.” The endorsement of “physical/biological/genetic causes” and “causes related to the school” was less common yet still prominent. Interestingly, these findings parallel previous mixed-method research with Spanish-speaking samples in the United States suggesting that many Latino parents identify ADHD etiology related to the family and/or the child’s personality/psychological characteristics, whereas a smaller but substantial portion of Latino parents identify ADHD etiology related to biology/genetics and/or the school (Gerdes et al., 2014; Haack & Pfiffner, 2016).
As predicted, all subscales and the overall FX-II demonstrated adequate reliability with high levels of internal consistency. In addition, all subscales and the overall FX-II (with the exception of the Caregiver/Teacher Support subscale) demonstrated adequate convergent construct validity by significantly correlating with all theoretically related subscales of ADHD completed by parents/caregivers and teachers (i.e., symptoms, executive functioning difficulties, as well as impairment at school, home, and with peers). There are several potential reasons why the FX-II Caregiver/Teacher Support subscale did not correlate with theoretically related measures of ADHD. To begin, examination of subscale mean scores indicates limited variability in the Caregiver/Teacher Support subscale ratings, such that raters in both the community and clinical samples reported high levels of caregiver/teacher support compared with the other subscales of functioning and support. Thus, range-restriction could have limited the ability to detect associations between the Caregiver/Teacher Support subscale with other measures. In addition, it may be that raters are less accurate reporters of their own behavior compared with the behavior of others due to self-protective or social desirability effects. The lack of construct validity documented for the FX-II Caregiver/Teacher Support subscale items warrants future efforts to evaluate and potentially improve this subscale.
With few exceptions, all subscales and the overall FX-II demonstrated divergent construct validity by failing to correlate with cultural and demographic factors (i.e., Mexican cultural values, Anglo cultural values, rater age, language proficiency, education, income, and child grade) completed by parents/caregivers and teachers. It is unclear why the total FX-II and Academic Functioning subscale ratings appear negatively associated with rater income and the Caregiver/Teacher Support subscale ratings appear positively associated with rater education. Given the overwhelmingly positive initial psychometric properties emerging for the FX-II, it is possible that the few significant correlations between ratings and demographic factors are spurious and do not actually represent rater trends. Overall, the strong preliminary reliability and validity results emerging for the FX-II are consistent with previous research suggesting that measures of functional impairment related to ADHD emerge as psychometrically sound when given to Spanish-speaking Latino parents (e.g., Haack et al., 2010; Haack et al., 2014; Haack et al., 2016; Solis & Abidin, 1991).
The FX-II also demonstrated adequate predictive validity via discriminant analyses with the Academic, Social/Emotional, and Familial Functioning subscales emerging as important predictors. The overwhelming majority of youth were correctly classified as belonging in the community versus clinical sample based on FX-II ratings (i.e., over 84% via community and clinical sample caregiver ratings; over 92% via ratings from community sample parents/caregivers and clinical sample teachers). Findings are consistent with previous research suggesting that measures of functional impairment related to ADHD are useful in distinguishing between children whom do and do not exhibit clinically significant attention and behavior concerns when given to Spanish-speaking Latino parents (e.g., Haack et al., 2011; Solis & Abidin, 1991).
Conclusions, Limitations, and Future Directions
The current study extends previous research on culturally appropriate ADHD assessment in diverse youth by developing a novel evaluation tool and establishing initial psychometric properties in a particularly underserved group (i.e., Mexican youth). The FX-II fills a crucial gap in available tools to evaluate functioning related to ADHD, especially given recent DSM-V criteria requiring ADHD symptoms to interfere with functioning (APA, 2013). This tool may be particularly beneficial for assessing ADHD in Latino youth, as it avoids psychodiagnostic terminology and double-negative phrasing which can be unfamiliar and uncomfortable to Spanish-speaking raters. Future research should examine the diagnostic utility of the FX-II in English and Spanish utilized in conjunction with ADHD symptom inventories and structured clinical interviews. The relative brevity but comprehensive coverage of functioning provided by the FX-II suggest it could be a feasible evaluation tool before, during, and following ADHD treatment. Given that academic, social, and familial functioning often are the most salient concerns for families presenting for ADHD services (Pelham & Fabiano, 2001; Pelham et al., 2005; Pelhem, 2002), future research should examine the use of FX-II items to inform treatment planning and guide individual treatment goal setting.
Several limitations of the current study should be noted. First, the current study provides initial evidence for psychometric properties and predictive validity when the FX-II is completed in Spanish by Mexican parents/caregivers or teachers of school-aged youth. Future FX-II validation efforts should utilize samples with more diverse ethnicities, languages, and socioeconomic levels represented. Second, the current sample size did not allow for fully powered factor analyses. A future area of direction includes examining the empirical subscales of the FX-II via factor analyses. In addition, the current study examined FX-II ratings before the clinical sample had completed the school-based intervention program for youth with attention/behavior concerns. Future research should examine if FX-II ratings are sensitive to clinical intervention, thus suggesting the FX-II could be useful in examination of treatment outcomes. This seems especially important in context of ADHD treatment outcome research documenting that improvement in symptoms do not always coincide with improvement in functioning (Karpenko et al., 2009).
Employment of evaluation tools designed for and validated with diverse populations, such as the FX-II, has the potential to encourage ADHD problem recognition and help seeking for at-risk and underserved youth (Eraldi et al., 2006; Haack & Gerdes, 2011; Reardon et al., 2017; Rothe, 2005). The widespread impact and longstanding consequences of untreated ADHD make this a pressing area of concern for researchers and clinicians worldwide. Over time, the use of culturally competent ADHD services (including culturally sensitive evaluation) could reduce unfortunate disparities in ADHD diagnosis and service utilization for vulnerable populations, such as Spanish-speaking families in the United States and Latin America.
Footnotes
Appendix
FX-II
Acknowledgements
We thank our research team at the Universidad Autonoma de Sinaloa (UAS), and specifically Ambrocio Mojardin, Dulce Karely Alcaraz Beltran, Mariana Aldana Castro, María Elena Urquídez Valdez, Brianda Lizeth Borboa Montoya & María Fernanda Arriaga Guerrero.
We also thank the Secretaria de Educacion Publica (SEP) in Culiacán, Sinaloa, and particularly the four participating schools, along with the school principals and the teams of Unidad de Servicios de Apoyo a la Educación Regular, del Departamento de Educación Especial.
Thank you to the original ADHD-FX development team, including Drs. Alyson Gerdes, Brian Schneider, Kathryn Lawton, Kelsey Gonring, and Linda Pfiffner.
Thank you also to our participating families and teachers!
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by NIH Research Training Grant # R25 TW009343 obtained by Dr. Lauren Haack funded by the Fogarty International Center and the National Institute of Mental Health, as well as the University of California Global Health Institute (UCGHI).