
Abstract
Keywords
Introduction
ADHD is one of the most common neurodevelopmental disorders (Wolraich et al., 2011). ADHD arises in childhood and often persists into adolescence or even adulthood (Faraone, Biederman, & Mick, 2006; Polanczyk, de Lima, Horta, Biederman, & Rohde, 2007); the main persistent symptom is inattention rather than impulsivity/hyperactivity (Kessler et al., 2010; Polanczyk & Jensen, 2008). However, the exact neurobiological mechanisms underlying ADHD symptoms remain poorly understood.
Recently, similar to other psychiatric disorders, ADHD has been considered a disorder of neural networks that can be measured by resting-state functional connectivity (RSFC; Fox & Raichle, 2007). The RSFC measures the synchronization in blood oxygen level–dependent (BOLD) signal fluctuations in different brain regions at rest, which may provide insight into the neurobiological underpinnings of the persistence and remission of ADHD symptoms (Damoiseaux & Greicius, 2009). By examining the human brain as a complex connected network of functionally interacting brain regions, we can obtain a new perspective of large-scale neural communication in the brain (Biswal, Yetkin, Haughton, & Hyde, 1995).
Based on the inattention symptom of ADHD, many studies have focused on the default mode network (DMN), which is thought to be linked to the frontal/parietal attention-related network and to serve as a buffer against the disruption of attentional processes by external stimuli (Smallwood, Brown, Baird, & Schooler, 2012). The DMN consists of the precuneus/posterior cingulate cortex (PCC), the medial prefrontal cortex, and the lateral/inferior parietal cortex (Buckner, Andrewshanna, & Schacter, 2008; Fox et al., 2005). The DMN plays an important role in the cognitive activities in ADHD by regulating the conversion of attention between internal mental activity and external stimulus, and is involved in the bottom-up processing of extraneous attention to redirect attention from unrelated objects (or stimuli; Silberstein, Pipingas, Farrow, Levy, & Stough, 2016). The inattentiveness observed in ADHD may be due to the inadequate suppression of the DMN (Fassbender et al., 2009), which is a causative factor mediating attention deficits in ADHD (Sonuga-Barke & Castellanos, 2007).
Nevertheless, the alterations in the RSFC in the DMN in patients with ADHD remain controversial. Castellanos et al. (2008) reported an ADHD-related decrease in the FC between the precuneus and PCC and between the medial prefrontal cortex and PCC/precuneus cortices in ADHD adults compared with healthy controls (HCs); this decrease was also found in children with ADHD (Fair et al., 2010). Furthermore, Tian et al. (2006) found an increased FC between the DMN and sensory brain regions and between the precuneus and sensory motor regions in adolescents with ADHD compared with HCs (Tian et al., 2008), which was consistent with the results reported by H. Mccarthy et al. (2013). Hence, we aimed to confirm the decreased connectivity within the DMN and increased connectivity between the DMN and the sensory motor regions in children with ADHD.
In addition to the DMN, an altered FC in several other attention-related networks has also been associated with ADHD. The following two partially segregated attention networks have been well established: the dorsal attention network (DAN) and the ventral attention network (VAN; Corbetta & Shulman, 2002). Both networks are key components of the attentional regulatory systems in the brain (Corbetta, Patel, & Shulman, 2008). The DAN is centered in the bilateral intraparietal sulcus (IPS) and the junction of the precentral and superior frontal sulcus (frontal eye fields [FEFs]), and enables the control of spatial attention by selecting sensory stimuli based on internal goals or expectations and linking these goals to the appropriate motor responses (Fox, Corbetta, Snyder, Vincent, & Raichle, 2006). The failure to ignore extraneous stimuli, which is one of the core symptoms of ADHD, is associated with a loss of FC in the DAN (Castellanos & Proal, 2012). The VAN is anchored in the right temporo-parietal junction (TPJ) and the ventral frontal cortex (VFC), and reorients attention to salient behaviorally relevant stimuli (Fox et al., 2006). S. Cortese et al. (2012) performed a comprehensive meta-analysis of 55 functional magnetic resonance imaging (fMRI) studies of ADHD, and revealed a significant ADHD-related hypoactivation in the VAN and DAN compared with that in HCs. In addition to the task-based fMRI studies, resting-state fMRI (rs-fMRI) studies have also revealed hypoconnectivity in the DAN and VAN in a sample of children and adults with ADHD (Corbetta et al., 2008; Fox et al., 2006; Mccarthy et al., 2013). Therefore, hypoconnectivity in the attention networks, including the DAN and VAN, is expected.
Numerous neuroimaging studies investigating ADHD included participants who were treated with psychostimulants and other medications (Cortese et al., 2012; Mccarthy et al., 2013). Thus, whether the results represent the effects of the disease or the effects of the medications remains unknown. Peterson et al. (2009) found that psychostimulants significantly improved the suppression of the DMN in the ventral anterior cingulate cortices and PCCs in adolescents with ADHD (Silberstein et al., 2016). The total white matter volume in drug-naïve children with ADHD was lower than that in medicated children with ADHD, and the cognitive enhancement effects in adults with ADHD are associated with a history of psychostimulant use (Fassbender et al., 2009). Metaregression analysis (Nakao, Radua, Rubia, & Mataix-Cols, 2011) of the effect of stimulant medications revealed that the morphological deficit was associated with the medication status; therefore, studying medication-naïve participants with ADHD can resolve the abovementioned critical issue. Moreover, the exclusion of patients with a history of prior psychotropic medication treatment can improve the ability of our study to definitively attribute the group differences to the underlying psychopathology of ADHD.
In addition, maturational delay has been considered one of the pathological mechanisms of ADHD (El-Sayed et al., 2003; Rubia, 2007; Shaw et al., 2007; Sripada, Kessler, Fang, et al., 2014), and Bos et al. (2017) suggested that increases of RSFC in DMN during childhood in ADHD can be interpreted as a reflection of a delay in development. Therefore, we aimed to also explore the correlation between the altered functional connectivity (FC) and age in the DMN or attention networks in children with ADHD.
In this study, we simultaneously investigated three neural networks (i.e., the DMN, DAN, and VAN) involved in attentional processes to better and more thoroughly understand the alterations in the RSFC in Chinese children with ADHD who have not been previously treated. Based on previous studies, we hypothesized that participants with ADHD may exhibit hypoconnectivity in the attention networks, increased connectivity between attention networks and the DMN, and increased connectivity between the DMN and the sensory motor regions. The altered FC may correlate with age, the results of neuropsychological tests, and clinical symptoms.
Materials and Method
Participants
Approval for this study was granted by the medical ethics committee of the First Affiliated Hospital of Wenzhou Medical University. All participants and their parents were fully informed of the purpose and procedures of this study, and written informed consent was obtained from the parents. The children with ADHD were recruited from the Mental Health Center of the First Affiliated Hospital of Wenzhou Medical University, and the healthy children were recruited from a local primary school and were matched with respect to age, sex, handedness, and intelligence quotient (IQ) level. The participants were recruited between March 2012 and November 2014. Seventy-two children with ADHD and 38 HC participants were included in our study. Among them, 13 children with ADHD and five HC participants did not complete the fMRI scan. Thirteen children with ADHD and two HC participants were excluded because of insufficient fMRI data quality (motion parameters exceeded). Finally, 46 children with ADHD (8.39 ± 1.949 years old) and 31 HC participants (9.23 ± 1.820 years old) were reserved for contrast analysis. There were 22 predominantly inattentive type, three predominantly hyperactive–impulsive type, and 21 combined type among the ADHD participants. All participants were right handed, according to the Annett Hand Preference Questionnaire (Dragovic & Hammond, 2007), and all were Han Chinese.
Prior to the magnetic resonance imaging (MRI) scan, none of the participants with ADHD had ever received any stimulant or other treatment for ADHD; also they had never received any psychotropics for any psychiatric condition. The diagnosis of ADHD was determined independently by two experienced psychiatrists (C.Y. and H.C.) with more than 15 years of experience in clinical psychiatry, according to the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria, a semistructured diagnostic interview, and the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime Version (K-SADS-PL; Kaufman, Birmaher, Brent, Ryan, & Rao, 2000). All parents of children with ADHD completed the self-administered Conner’s Parent Symptom Questionnaire–Chinese, revised version (Conners, 1999). This scale measures the hyperactivity/impulsivity symptoms of ADHD and comorbidities. In particular, 48 items are included that relate to the following six aspects: (a) conduct problems, (b) learning problems, (c) physical and psychological problems, (d) impulsivity–hyperactivity score, (e) anxiety, and (f) hyperactivity index score.
In addition, the participants completed a series of neuropsychological tests, including the Wechsler Intelligence Test and the Wisconsin Card Sorting Test (WCST). The exclusion criteria included the following: (a) left-handedness; (b) a history of using psychostimulants or any other drugs or therapy for the disorders; (c) a full-scale IQ score of less than 90 according to the Wechsler Intelligence Scale for Chinese Children–Revised (Gong & Cai, 1993); (d) a history of head trauma with a loss of consciousness; (e) comorbid neurological disorders or other severe diseases, such as pediatric stroke and seizure disorders; and (f) past or current comorbid psychiatric disorders, including affective disorders, oppositional defiant disorder (ODD; based on previous research, although ADHD is highly comorbid with ODD, ADHD and ODD have different pathological mechanisms—we excluded children with ADHD comorbid ODD and aimed to explore the pathological mechanism of ADHD more purely), Tourette’s syndrome, conduct disorder, or any other Axis I psychiatric disorder. The healthy children were screened by the same psychiatrists, according to the Structured Clinical Interview for DSM-IV, and the exclusion criteria were the same as those applied to the children with ADHD. Table 1 summarizes the demographic and clinical characteristics of the participants.
Demographic and Clinical Characteristics of All the Participants.
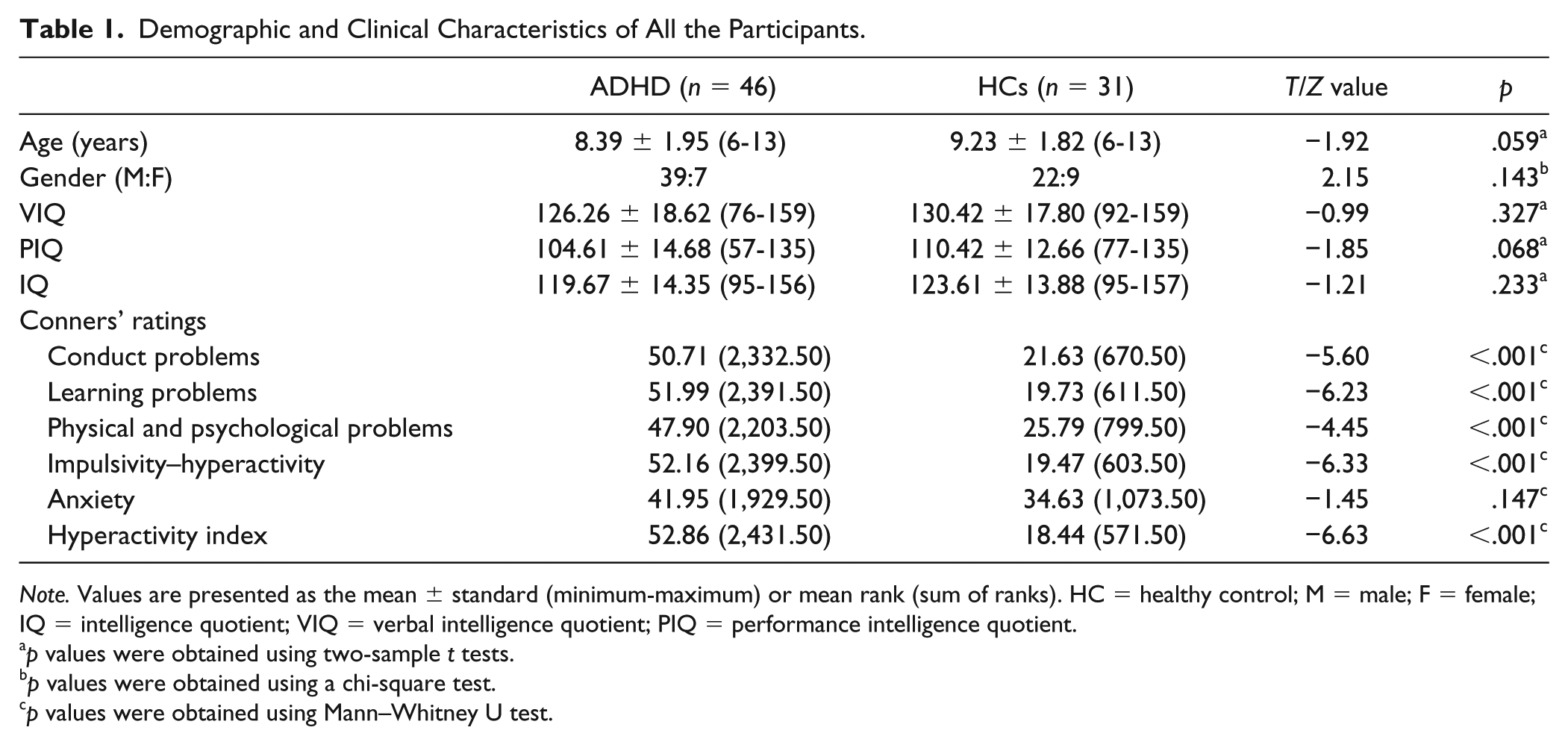
Note. Values are presented as the mean ± standard (minimum-maximum) or mean rank (sum of ranks). HC = healthy control; M = male; F = female; IQ = intelligence quotient; VIQ = verbal intelligence quotient; PIQ = performance intelligence quotient.
p values were obtained using two-sample t tests.
p values were obtained using a chi-square test.
p values were obtained using Mann–Whitney U test.
Image Acquisition
All MRI scans were performed on a 3T MRI scanner (signal HDx, General Electric, Milwaukee, WI, USA) with an eight-channel phased-array head coil. During the entire scanning procedure, all participants were required to lie in a supine position with their heads snugly fixed by foam pads to reduce head movement. Whole-brain rs-fMRI data depicting BOLD contrast were obtained using a gradient-echo echo-planar imaging sequence with the following parameters: 31 axial slices, slice thickness = 4 mm, slice gap = 0.2 mm, repetition time (TR) = 2,000 ms, echo time (TE) = 30 ms, flip angle = 90°, matrix size = 64 × 64, and field of view (FOV) = 192 × 192 mm2. The rs-fMRI contained 240 volumes and ran continuously for 8 min. During scanning, the participants were asked to keep their eyes closed, remain relaxed, and not fall asleep. None of the participants fell asleep during the scan, which was confirmed by self-reports after the scan.
Data Preprocessing
Preprocessing of the rs-fMRI data was performed using the Data Processing Assistant for Resting-State fMRI (DPARSF_V2.3 [Chao-Gan & Yu-Feng, 2010], http://www.restfmri.net/forum/DPARSF). For each participant, the data preprocessing included the conversion of digital imaging and communications in medicine (DICOM) data to neuroimaging informatics technology initiative (NIFTI) images, the removal of the first 10 time points, a slice-timing correction, a realignment to the middle image, a spatial normalization to the Montreal Neurological Institute (MNI) template using echo planar imaging (EPI) templates (previous work has indicated that the normalization of children’s MR images to standard adult templates is acceptable for statistical group comparisons; Burgund et al., 2002; Kang, Burgund, Lugar, Petersen, & Schlaggar, 2003), a resampling of each voxel to 3 × 3 × 3 mm3, and a spatial smoothing using an 8-mm full-width at half-maximum (FWHM) Gaussian kernel. The data were excluded if the motion parameters exceeded 3 mm in any direction or 3.0° of any angular motion during the scan. Because the RSFC could be affected by micromotions from volume to volume, the framewise displacement (FD) values for each participant were computed, and the mean FD value was applied as a covariate in the group comparisons of the RSFC. Several nuisance signals, including the white matter signal, cerebrospinal fluid signal, and 24 head motion parameters, were regressed from each voxel’s time course to reduce the effects of head motion and nonneural BOLD oscillations. Finally, the images underwent a removal of liner trends and temporal bandpass filtering (0.01-0.08 Hz) to exclude the effects of physiological noise, such as the heartbeat and respiratory rhythm.
FC Maps
The RSFC was processed using the REST V1.8 software (Song et al., 2011). Based on previous studies (Mccarthy et al., 2013; Sheline, Price, Yan, & Mintun, 2010), the following seed regions of interest with a 6-mm radius were selected to identify the three different networks: the precuneus (±7, −60, 21) in the DMN, the TPJ (±53, −48, 20) and VFC (±37, −18, 1) in the VAN, and the IPS (±27, −58, 49) and FEF (±24,−13, 51) in the DAN. For each region, the time course from the bilateral spherical region of interest was averaged. Correlation functional analyses were performed by computing the temporal correlation between each seed reference and the rest of the brain in a voxelwise manner. The individual correlation coefficients were normalized to Z scores using Fisher’s Z transformation. Finally, the data of each group were analyzed using a one-sample t test in REST. A statistical map of the significant FC was created for each seed. The significance level was set at p < .05 at the voxel level and was corrected by an Alphasim correction at the cluster level.
Statistical Analysis
We used SPSS (version 16; SPSS Inc.) to calculate the between-group differences in the demographic and clinical variables. Age and IQ were analyzed using two-sample t tests. Furthermore, the gender distribution was compared using the Pearson chi-square test. Conners’ ratings were analyzed using Mann–Whitney U tests. The mean FD derived from Jenkinson, Banister, Brady, and Smith (2002) was analyzed using two-sample t test.
A between-group comparison of the FC maps was performed using two-sample t tests in SPM8 (http://www.fil.ion.ucl.ac.uk/spm/). Specific masks were created by combining the voxels of the children with ADHD and the HCs that were obtained from the one-sample t-test results. Age, gender, and the mean FD derived from Jenkinson et al. (2002) were considered confounding covariates. The statistical significance level was set at p < .01 at the voxel level and p < .05 at the cluster level (false discovery rate [FDR] corrected; Benjamini & Yekutieli, 2001).
Subsequently, the brain–behavior relationships were analyzed in the ADHD and HC groups. Mean FC data were extracted from areas that showed significant differences between ADHD participants and controls. Two-tailed partial correlation (controlling for age) analyses were performed to examine the relationships between the FCs that showed significant group differences and neuropsychological tests (scores on the Digital Span Scale of the Wechsler Intelligence Test, total correct, total errors, categories completed, perseverative errors, and nonperseverative errors of WCST) or clinical symptoms (Conners’ ratings).
Finally, two-tailed Pearson correlation analyses were performed to examine the relationships between age and the FCs that exhibited significant group differences.
Results
Demographic and Clinical Characteristics
As shown in Table 1, the drug-naïve children with ADHD did not significantly differ from the control participants with respect to age, gender, or IQ level.
There were significant group differences in all Conners’ ratings (Table 1).
No significant difference (T = 1.18, p = .241) was found in the mean FD derived from Jenkinson et al. (2002) between the two groups (M ± SD: 0.10 ± 0.06 mm, 0.08 ± 0.05 mm).
Alteration in the Brain Networks in Children With ADHD Compared With the HCs
Altered FC between the DAN and regions of the DMN involved in non–goal-directed processes
Compared with the controls, the participants with ADHD displayed a significantly increased FC between the DAN seeds and regions of the DMN involved in non–goal-directed processes: namely, one region between the right FEF and the right posterior cingulate and another between the left FEF and the precuneus (Table 2, Figure 1a and 1b).
Region of Increased RSFC in ADHD Compared With the HCs.
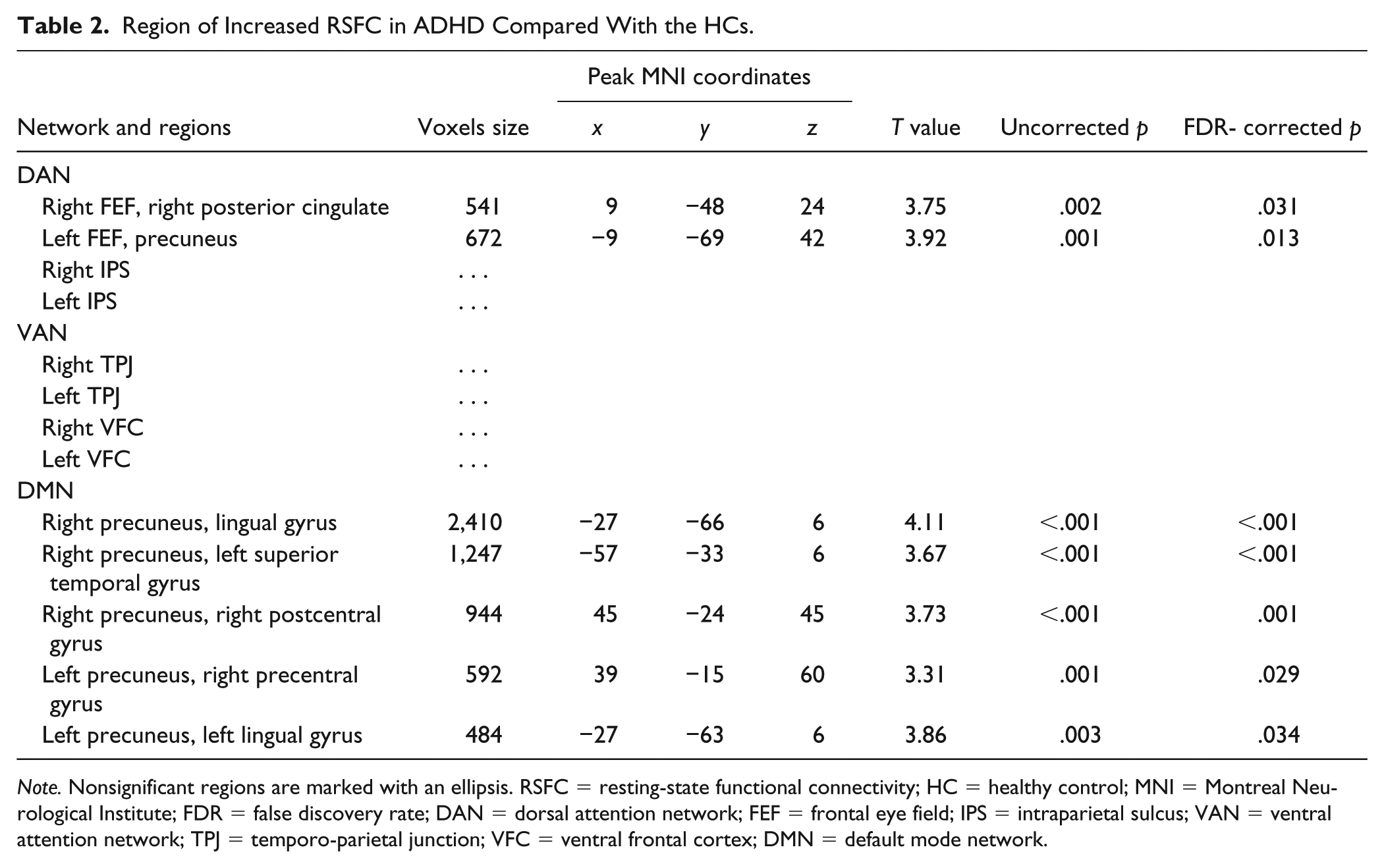
Note. Nonsignificant regions are marked with an ellipsis. RSFC = resting-state functional connectivity; HC = healthy control; MNI = Montreal Neurological Institute; FDR = false discovery rate; DAN = dorsal attention network; FEF = frontal eye field; IPS = intraparietal sulcus; VAN = ventral attention network; TPJ = temporo-parietal junction; VFC = ventral frontal cortex; DMN = default mode network.
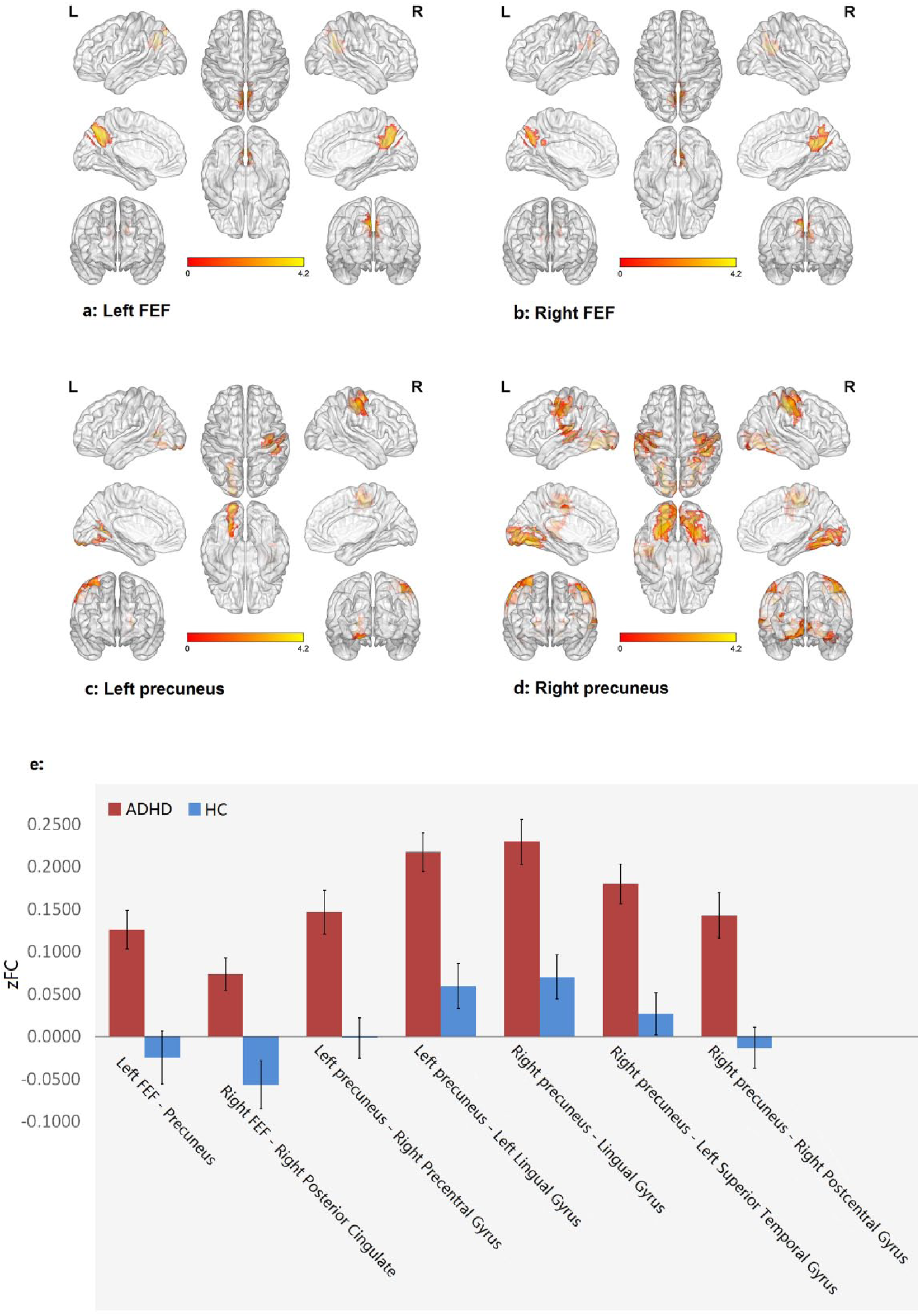
Comparison of connectivity maps.
Altered FC between the DMN and regions of the somatosensory cortex involved in sensory motor information processing
Compared with the controls, the participants with ADHD displayed a significantly increased FC between DMN seeds and regions of somatosensory cortex involved in sensory motor information processing: namely, one region between the right precuneus and the right postcentral gyrus, and another between the left precuneus and the right precentral gyrus (Table 2, Figure 1c and 1d).
Altered FC between the DMN and regions of the visual cortex involved in maintenance of attention
Compared with the controls, the participants with ADHD exhibited a significantly increased FC between DMN seeds and regions of visual cortex involved in the maintenance of attention: namely, between the bilateral precuneus and the left lingual gyrus (Table 2, Figure 1c and 1d).
Altered FC between the DMN and regions of the auditory cortex involved in auditory processing
Compared with the controls, the participants with ADHD displayed a significantly increased FC between DMN seeds and regions of the auditory cortex involved in auditory processing: namely, between the right precuneus and the left superior temporal gyrus (Table 2, Figure 1c and 1d).
No group difference was observed in the FC in the DAN when the IPS was selected as the seed (Table 2). In addition, when the TPJ or the VFC was selected as the seed, no significant difference between the groups was observed for the FC in the VAN (Table 2).
Relationship Between FC and Neuropsychological Tests and Clinical Measures
In the ADHD group, the hyperconnectivity in the DMN was significantly and positively correlated with the scores on the Digital Span Scale of the Wechsler Intelligence Test. In addition, the increased FC in the DMN between the right precuneus and lingual gyrus, between the right precuneus and left superior temporal gyrus, and between the left precuneus and the left lingual gyrus was positively correlated with the total correct scores on the WCST and was negatively correlated with the total error scores on the WCST. However, no significant correlation was found between the altered FC in the DMN and the number of categories completed, the number of nonperseverative errors, or the number of perseverative errors. No significant correlation was found between the altered FC in the DMN and the Conners’ ratings. No significant correlation was found between the altered FC in the DAN and the neuropsychological tests or the Conners’ ratings. (Table 3)
Correlations Between Altered FC and Neuropsychological Tests in the ADHD Group.
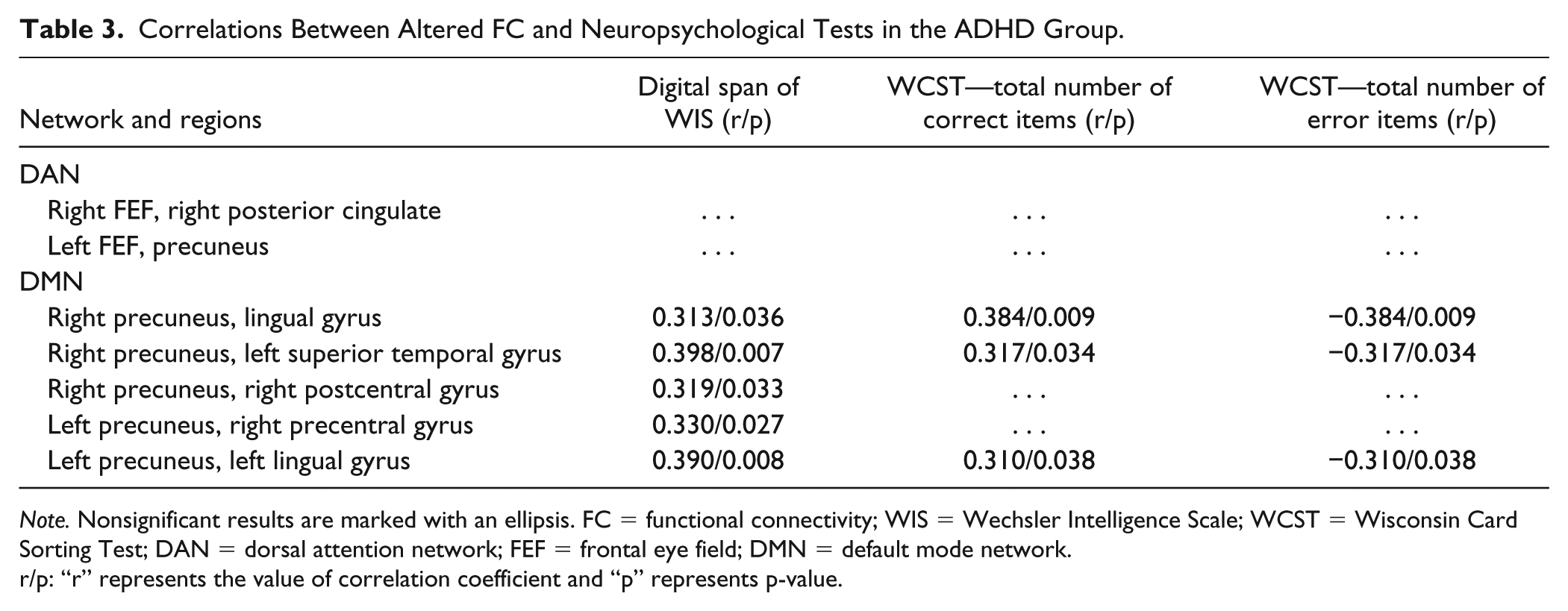
Note. Nonsignificant results are marked with an ellipsis. FC = functional connectivity; WIS = Wechsler Intelligence Scale; WCST = Wisconsin Card Sorting Test; DAN = dorsal attention network; FEF = frontal eye field; DMN = default mode network.
r/p: “r” represents the value of correlation coefficient and “p” represents p-value.
In the HC group, no significant correlation was found between the neuropsychological tests and the FC measurements. The FC in the DMN between the right precuneus and lingual gyrus (r = −.366, p = .047) and between the left precuneus and the left lingual gyrus (r = −.449, p = .013) was negatively correlated with the anxiety score of Conners’ ratings. The FC in the DAN between the right FEF and right posterior cingulate was positively correlated with the impulsivity–hyperactivity score (r = .433, p = .017) and the hyperactivity index score (r = .458, p = .011) of Conners’ ratings.
Relationship Between FC and Age
No significant correlation was found between the FC measurements and age in the ADHD group or in the HCs.
Discussion
To the best of our knowledge, our study is the first to demonstrate attention-related network alterations in drug-naïve children with ADHD using seed-based FC in rs-fMRI studies. The main finding was that children with ADHD showed a significantly increased RSFC in the DAN and DMN, whereas no significant alteration was found in the VAN. The significantly altered RSFC in the DMN was correlated with the subscale in the Wechsler Intelligence Test and WCST.
The hyperconnectivity in the DAN in the children with ADHD was different from that reported in previous studies in which the DAN connectivity was decreased (Cortese et al., 2012; Mccarthy et al., 2013). The hyperconnectivity in these regions can be interpreted as “inefficient” because more energy must be exerted to perform similarly to the HCs. The inefficient top-down deployment of attention by the DAN may account for the symptom of inattention. The PCC and precuneus have been associated with non–goal-directed processes. The highly enhanced activation of the precuneus during task engagement in ADHD has been associated with instances of errors and attention lapses (Castellanos et al., 2008). To the best of our knowledge, previous studies investigating ADHD have reported an alteration in the FC in the DAN, but an alteration in the FC between the FEF and the PCC/precuneus (two hubs of the DMN) has not been reported. ADHD has been considered a disease with abnormal connectivity between networks rather than abnormalities in discrete, isolated brain regions (Sidlauskaite, Sonuga-Barke, Roeyers, & Wiersema, 2016). Therefore, we hypothesize that the aberrant FC between local regions that pertain to the DAN and DMN may be the pathophysiological mechanism of ADHD. Further studies are needed to test the hypothesis that the interaction between the DMN and attentional networks underpins the pathophysiology of ADHD.
Compared with the HCs, we found hyperconnectivity between the DMN seeds and the lingual gyrus, the superior temporal gyrus, the postcentral gyrus, and the precentral gyrus in the children with ADHD, which was similar to previous observations in participants with ADHD (Barber et al., 2015; Cocchi et al., 2012; Cortese et al., 2012; Mostert et al., 2016). The increased FCs may imply compensatory enhancement (Cortese et al., 2012; Fassbender & Schweitzer, 2006; Mccarthy et al., 2013; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005) because this hyperconnectivity was positively correlated with the subscale in the Wechsler Intelligence Test and the total correct scores on the WCST and was negatively correlated with the total error scores on the WCST. The Digital Span Scale of the Wechsler Intelligence Test is considered a measure of attention (Hale, 2002). The number of total errors was reported to be related to frontal executive function (Nyhus & Barceló, 2009). Difficulties with executive function appear to be one important component of the complex neuropsychology of ADHD (Willcutt et al., 2005). However, the correlation with the number of categories completed or the number of perseverative errors on the WCST was not significant, whereas the two measures have been confirmed to be more meaningful in frontal executive function (Nyhus & Barceló, 2009). Therefore, according to our results, we suggest that the strength of FC in the DMN affects the attention status, but the evidence for the impact on executive function is insufficient.
The right postcentral gyrus is the location of the primary somatosensory cortex. The right precentral gyrus is responsible for motor demands, and hyperfunction in this region has been associated with impaired motor inhibition in ADHD (Cortese et al., 2012). Our findings suggest the presence of hyperconnectivity between the precuneus and sensory motor regions in children with ADHD, which is consistent with previous fMRI studies involving ADHD adults and adolescents (Mccarthy et al., 2013; Tian et al., 2008; Tian et al., 2006). The finding that participants with ADHD engage in more sensory motor information processing is consistent with the ADHD symptoms of inattention and hyperactivity. Moreover, our findings may reflect a compensation for the aberrant FC in the attention-related network that typically reconciles with sensorimotor attention (Fassbender & Schweitzer, 2006). This result may be associated with the ADHD symptoms of inattention and hyperactivity. The lingual gyrus is located in the occipital lobe, which directs the processing of visual information, maintenance of attention, and inhibition of indifferent stimuli. The heightened RSFC in the occipital region in ADHD has been associated with a poor inhibition of sensory perception (Cao et al., 2009), whereas dysfunction in the ability to inhibit foreign and indifferent stimuli is a core symptom of ADHD (Buffalo, Fries, Landman, Liang, & Desimone, 2010). The superior temporal gyrus contains the primary auditory cortex, which is involved in auditory processing. The enhanced activity in the superior temporal gyrus indicates an increased aptness to becoming distracted by environmental stimuli. Rubia (2007) found that the delayed cortical development of the superior temporal cortex in patients with ADHD might be related to age-inappropriate deficits in attention.
In addition, many studies have provided evidence for the developmental delay hypothesis of ADHD (Sato, Hoexter, Castellanos, & Rohde, 2012), and some researchers have suggested DMN developmental delay in FC analysis (Bos et al., 2017; Sripada, Kessler, & Angstadt, 2014). However, in the current study, we did not observe a significant correlation between the FCs and age, which may be due to the small sample size, and future studies with longitudinal design will help to clarify this issue.
The FC in the VAN was not significantly altered, and there were discrepancies between our results and those of previous studies. For example, Mccarthy et al. (2013) have reported a decreased RSFC in the VAN in 16 adults with combined-type ADHD, two of whom were medication naïve. Our study samples were different from the abovementioned study with respect to patient age, ADHD subtype, and history of drug therapy. Farrant and Uddin (2015) reported that adults showed greater FC within the VAN than did children. A meta-analysis of 55 fMRI studies (Cortese et al., 2012) investigated various age groups and clinical characteristics, and found voxel hypoactivation (44%; a percentage of the total number of significant voxels) and voxel hyperactivation (23%) within the VAN in ADHD children. However, no voxel hypoactivation or hyperactivation was found within the VAN in adults. These results suggest different functional characteristics in the VAN at different ages in ADHD patients. Disease progression or neurodevelopment with age should be considered. Moreover, Sanefuji et al. (2017) reported increased rs-fMRI connectivity within the right VAN in children and adolescents with predominantly inattentive subtype ADHD compared with the predominantly hyperactive–impulsive subtype. The study proposed differences in RSFC within the VAN between diverse ADHD subtypes. Furthermore, we did not identify any ADHD literature that reported the effect of medication history on FC in the VAN. However, in other brain networks of ADHD studies, the effect of drugs on the FC of networks was clear (Rubia et al., 2009; Silberstein et al., 2016). Thus, the dissimilar results of the aberrant FC in the VAN may be due to diverse patient age, medication status, and phenotypes of ADHD. In addition, neither the VAN nor the DAN control attentional processes in isolation, and the flexible interaction between both systems enables the dynamic control of attention in relation to top-down goals and bottom-up sensory stimulation (Vossel, Geng, & Fink, 2014). The suppression of the VAN is necessary to prevent attentional switching (Corbetta & Shulman, 2002), and its hyperactivation might underpin distractibility, which is one of the cardinal symptoms of ADHD. However, certain studies failed to confirm that the VAN is explicitly involved in ADHD. In contrast, abnormalities in the DAN clearly emerge (Dickstein, Bannon, Castellanos, & Milham, 2006; Rubia, 2011; Stevens, Pearlson, & Kiehl, 2007). Therefore, these inconsistent results regarding the VAN in fMRI studies warrant further investigation.
Notably, many studies suggested different FC patterns with different resting-state conditions (Xu et al., 2014; Yan et al., 2009; Zou et al., 2009). Van et al. have reported reduced FC in DMN and attention networks under the “eyes closed” condition compared with the “eyes open and fixated” condition (Van Dijk et al., 2010). The rs-fMRI data in our study were scanned under the “eyes closed” condition as instructed. Therefore, the significance of our results should be considered under the “eyes closed” condition, and our findings may differ from the findings under other resting-state conditions.
In summary, we found that the dysregulation of networks in children with ADHD was present not only in the DAN and DMN, which contribute to cognitive–behavioral functions, but also in the somatosensory, motor, visual, and auditory networks, which account for sensory and motor processes.
Limitations
There are some limitations in this study as follows: (a) During the recruitment of the participants, patients with ADHD with obvious hyperactive symptoms were excluded due to difficulties undergoing the fMRI scan, which may have increased the selection bias (hyperactive–impulsive type with fewer opportunities for inclusion) to a certain extent, and the results may also lack universality. (b) An increasing number of studies have shown that ADHD is a complex heterogeneous disease using different etiology, pathophysiology, and cognitive models, including different subtypes, and we were unable to perform subtype analysis due to the insufficient sample size. (c) Although we adopted a well-recognized analytical method of fMRI data, as there is no single uniformed pipeline for imaging data processing and especially for the results demonstration, which are highly dependent on the p value, we need to be cautious when interpreting different results. Therefore, a larger sample size including subtype analysis should be investigated in further studies.
Footnotes
Acknowledgements
The authors are grateful to the patients and control participants for their participation in the study, and our colleagues who facilitated the work.
Ethical Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Authors’ Contribution
Haixi Lin and Qingxia Lin contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No. 81671669) and the Natural Science Foundation of Zhejiang Province (Grant No. LY14H090012).