
Abstract
Keywords
Behavioral parent training (BPT) is an evidence-based treatment for addressing behavior problems in school-aged children with attention-deficit hyperactivity disorder (ADHD). BPT programs target the behaviors of parents, teaching them positive parenting skills to decrease common behavior problems (e.g., noncompliance, aggression, and temper tantrums) associated with a diagnosis of ADHD and other behavior disorders. Common components of BPT include teaching parents strategies for giving commands effectively, increasing compliance with directions, using contingency management systems, and implementing time out or response-cost consequences (Chronis, Chacko, Fabiano, Wymbs, & Pelham, 2004).
The efficacy of BPT has been demonstrated in numerous studies over the years (Chronis, Jones, & Raggi, 2006; Evans, Owens, & Bunford, 2014; Evans, Owens, Wymbs, & Ray, 2017; Pelham & Fabiano, 2008). However, most efficacy studies involve the use of BPT within the context of controlled clinical research trials. These studies typically include families receiving treatment free of charge, incentives for completing treatment, and regular monitoring and follow-up to encourage attendance and participation. In addition, practitioners in these studies undergo extensive training and are closely monitored on adherence to the treatment manual. These factors are likely to affect participation rates as well as the effectiveness and feasibility of offering BPT in real-world, community-based clinical settings (Cunningham, Bremner, & Secord-Gilbert, 1993; Dulcan, 2005). Effectiveness trials (pragmatic trials) that measure the degree of beneficial effect in real-world clinical settings are critical as poor uptake of evidence-based practices is a major barrier to providing effective mental health care (Novins, Green, Legha, & Aarons, 2013). Furthermore, research also shows that programs developed and tested in the research context may be limited in their applicability and transportability to families of diverse cultural, racial/ethnic, and socioeconomic backgrounds in real-world clinical settings (Williamson, Harrison, Reader, & Tynan, 2016). There are many fewer effectiveness trials for BPT, but fortunately those that exist suggest that BPT can be integrated into routine clinical practice with beneficial outcomes on parenting behaviors, confidence, and stress, child impairment, ADHD and externalizing problems, and child compliance (Gerdes, Haack, & Schneider, 2012; Lauth, Otte, & Heubeck, 2009; Loren, Ciesielski, & Tamm, 2017; Loren et al., 2015; Malik & Tariq, 2014; Shata, Abu-Nazel, Fahmy, & El-Dawaiaty, 2014; Tynan, Schuman, & Lampert, 1999; van den Hoofdakker et al., 2010).
A critical issue for evaluating the efficacy of BPT is which variables are utilized to demonstrate outcomes (Evans et al., 2017). A recent systematic review and meta-analysis found that reductions in frequency or severity ratings of ADHD symptoms were not as robust as would be desired (Sonuga-Barke et al., 2013). In addition to issues related to potential bias (ratings are most often completed by parents who are participating in treatment), the use of ADHD rating scales pose additional challenges for documenting efficacy. For example, these scales often assume a common definition of behaviors, provide ratings only for behavioral symptoms, and collapse these ratings across all situations. However, many of the behaviors or symptoms associated with ADHD may occur situationally or only within certain contexts (Barkley & Edlebrock, 1987), and family environment and other contextual features affect behavioral presentation as well (Breen & Altepeter, 1991; Paidipati & Deatrick, 2015). In fact, Evans and colleagues in reviewing the evidence for BPT argued that impairment produced by ADHD symptoms, and not ADHD symptoms themselves, should be the primary focus of outcome evaluation for BPT (Evans et al., 2017).
There are a few studies that have examined whether BPT is effective at reducing parental reports of child impairment using the Impairment Rating Scale (IRS; Fabiano et al., 2006), which assesses impairment in relationships (with parents, peers, and siblings), academic, and self-esteem domains. These studies have found improvements in parental ratings of child impairment following BPT offered in academic settings (Chacko et al., 2008; Chacko et al., 2009; Fabiano et al., 2009). In addition, Loren and colleagues reported similar improvements in child impairment as rated on the IRS following BPT offered in a clinical community setting (Loren et al., 2017; Loren et al., 2015). Of note, however, is that the IRS does not include situationally specific items, nor does it include impairment in specific areas, such as task completion or bedtime routine. Thus, an important area to focus on is whether and how BPT reduces the impact of the child’s ADHD symptoms in various situations and contexts.
The Home Situations Questionnaire (HSQ; Barkley & Edlebrock, 1987) was developed to allow such an assessment. The HSQ assesses situational variability or pervasiveness of a child’s problems with complying with instructions, commands, or rules. Specifically, the HSQ asks parents to rate whether or not their child has “any problems with compliance to instructions, commands, or rules” in 16 specific situations and, if so, to rate the severity of these problems. Research examining the use of the HSQ to assess the efficacy of BPT has been limited. However, the few studies found have reported significant reductions in both the number and the severity of problematic behaviors at home following the completion of BPT (Lauth et al., 2009; Malik & Tariq, 2014; Shata et al., 2014; Varnado, Williams, & Dahmes, 2014). Another study, which used the HSQ-Revised (DuPaul & Barkley, 1992), did not report significant reductions in the parental report of the number of attentional difficulties in specific situations after completion of BPT (Anastopoulos, Shelton, DuPaul, & Guevremont, 1993). However, the HSQ-Revised asks whether the child has any problems “paying attention or concentrating” in 14 situations, and thus may not be directly comparable with the HSQ, which asks about problems with compliance. Furthermore, it may be important to investigate the specific situations which BPT affects most and least to refine BPT interventions to be more efficacious. This is especially important as these impairments are most often the reason a parent seeks treatment. For example, it is not so much that a child “often makes careless mistakes” (ADHD inattention symptom), but that making careless mistakes is negatively affecting their ability to do school work and homework, thereby affecting their grades and increasing arguments with parents, that may drive a parent to seek treatment.
In fact, despite having levels of symptoms that would be clinically elevated enough to warrant a diagnosis of ADHD or another diagnosis, relatively few parents seek treatment for their children (Angold et al., 1998; Bussing, Zima, Gary, & Garvan, 2003; Teagle, 2002). Parents are more likely to seek treatment when they perceive an increased burden associated with parenting their child (i.e., the behaviors are negatively affecting the family), with Angold et al. (1998) noting that they are three times more likely to seek treatment if their child has symptomatic behaviors associated with a mental health diagnosis and impairment, rather than just symptomatic behaviors alone. In addition, behaviors commonly demonstrated in children with ADHD affect their family unit as a whole, increasing parent distress and decreasing their ability to engage in positive parenting, with the negative impact on family functioning also acting as a driver for seeking treatment (Moen, Hedelin, & Hall-Lord, 2016).
Given that the goal of BPT programs is to teach intervention strategies to be implemented in the home setting by parents, effectiveness may be affected by parental factors such as stress. Numerous studies have provided evidence that parenting a child with ADHD significantly increases parental reports of stress and negative family impact (Breen & Barkley, 1988; Paidipati & Deatrick, 2015; Reader, Stewart, & Johnson, 2009). Mothers of children with ADHD report higher levels of anxiety, depression, and stress than mothers of typically developing children who do not have ADHD (Musa & Shafiee, 2007). Furthermore, parents of children with ADHD reported the highest levels of both perceived problems as well as perceived negative family impact compared with parents of children with other diagnoses (e.g., anxiety, depression, oppositional defiant disorder; Teagle, 2002). This stress can vary by situation, with parents noting increased stress with homework; frequent calls or contacts from teachers; disruptive behaviors at home, in school, with peers, and in public; and a limited effect of punishment and other forms of discipline in changing their child’s behaviors. Increased levels of parental stress limit parents’ ability to effectively implement positive parenting techniques and strategies (Johnson & Reader, 2002). Moreover, parents who report higher levels of stress (including stress resulting from socioeconomic status, being a single parent, and other environmental factors) have a significantly higher rate of attrition from BPT (Lauth et al., 2009; Schneider, Gerdes, Haack, & Lawton, 2013). However, parents who report higher levels of stress prior to treatment report more benefits when completing BPT than parents reporting lower stress levels (Lauth et al., 2009). Thus, assessing the impact of BPT on parental stress related to a child’s disruptive behavior, as well as the interplay between a child’s behavior across various situations and contexts and related parental stress, may also be important to explore.
Present Study
We assessed the impact of BPT for ADHD offered in an outpatient mental health clinic on situational pervasiveness and severity of behavior problems and parental stress ratings. It is particularly important to confirm that BPT interventions offered in real-world settings (i.e., not as part of highly controlled research investigation offered under optimal conditions) have a clinically meaningful impact on the behaviors that lead parents to seek treatment (Lauth et al., 2009; Loren et al., 2017). We hypothesized that after attending BPT, parents would report fewer situations in which problem behavior was observed and less severe behavior problems, as well as reduced parenting stress related to their child’s behavior. Exploratory analyses were also conducted to examine whether reductions in situational pervasiveness and severity of behavior problems were associated with reductions in parental stress ratings.
Method
Participants
Participants were outpatients seeking treatment for their child’s ADHD and were not specifically recruited as research participants; however, all signed an Institutional Review Board approved informed consent to allow their clinical data to be utilized for research purposes. Data were collected from 304 parents of 6- to 12-year-old children who attended BPT groups offered through the Center for ADHD at Cincinnati Children’s Hospital Medical Center in Ohio. Participants came from a variety of sources, including referrals from physicians, psychologists, other parents, and self-referrals. Families interested in participating in the group completed a general background questionnaire that included questions about the child’s demographics, medical and developmental history, homework and compliance, diagnoses, and school and social history, including any accommodations the child currently receives. A psychologist then reviewed the packet to ensure appropriateness for group participation. To participate, the identified child needed to have a parent-reported diagnosis of ADHD without a co-existing diagnosis of autism or intellectual disability. This process was developed using a series of quality assurance trials that demonstrated this method to be sufficient for assessing group eligibility, thereby obviating the need for a diagnostic session with the parents, decreasing the cost to the family, and improving access to patient care. If both of a child’s parents attended group, data were collected from only one (usually the mother). Demographic and clinical characteristics of children whose parents attended BPT and provided complete data on both outcome measures (n = 159) are presented in Table 1. The primary reason for missing data was families not attending the final session of group where outcome measures were collected. Other issues included families leaving early from the final session, families not filling out forms completely, and data not being entered into the repository due to staffing issues. Unfortunately, limited information was documented in the clinical database including diagnostic comorbidities, medication and insurance status, and attendance. Furthermore, no demographic information was available on parents.
Demographic and Clinical Characteristics.
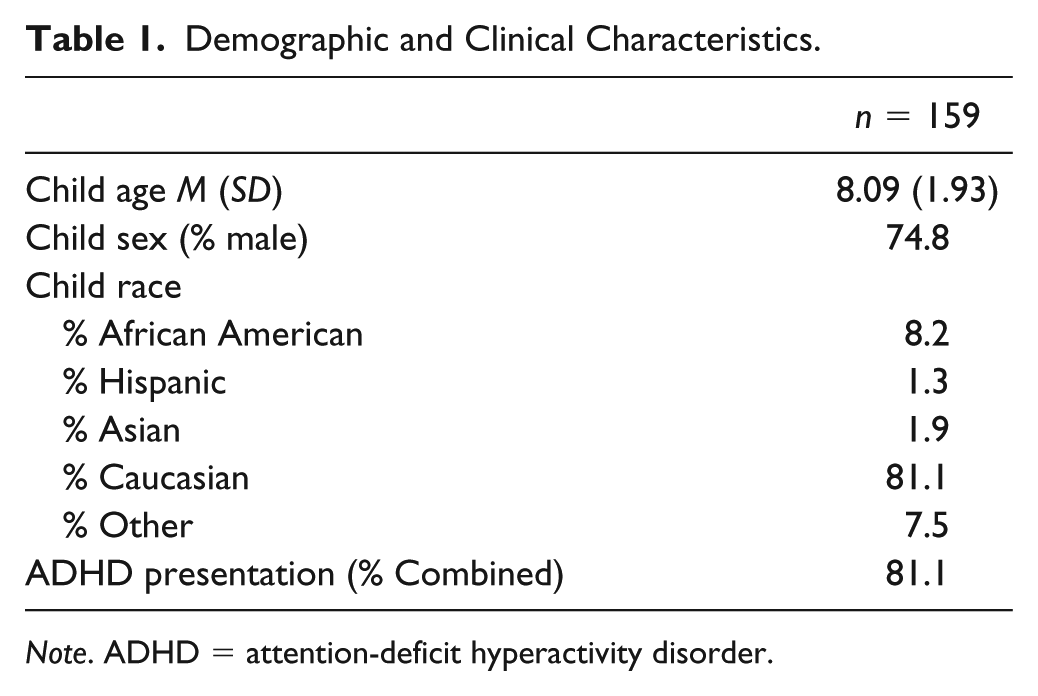
Note. ADHD = attention-deficit hyperactivity disorder.
Procedure
Parents attended an eight-session manualized BPT group focused on ADHD (Loren et al., 2015) which was based on programs developed by Barkley (1987) and the Multimodal Treatment Study of ADHD (MTA; Wells et al., 2000). The group progresses by providing content and examples of new behavioral parenting skills each week beginning with (a) an overview of the diagnosis of ADHD including underlying neurobiology, associated executive function deficits, behavioral difficulties associated with the diagnosis, and evidence-based treatment options, followed by sessions teaching (b) an overview of basic principles of social learning theory and behavior modification (including discussions on antecedents, behaviors, consequences, and their relationships, as well as schedules of reinforcement) and use of descriptive praise, ignoring, and Special Playtime, (c) giving effective commands, (d) creating a contingency management system, (e) homework strategies, (f) Daily Report Cards (DRC), (g) effectively using time out and response cost, and (h) managing behaviors in public places, maintaining improvements, and addressing future problems. Prior to the first session and at the last session of the groups, parents completed the ratings of situational variability and pervasiveness of child behavior problems and ratings of parental stress. The groups were all lead by one of three independent licensed clinical psychologists with at least 3 years of experience in practice postlicensure.
Measures
HSQ
The HSQ consists of 16 situations in which parents commonly observe and manage child behaviors (Barkley & Edlebrock, 1987). Parents rate whether problems with compliance occur in these situations and, if so, the severity on a 1 (mild) to 9 (severe) scale. The HSQ yields total number of problem situations (possible range 0-16), severity of problems in each situation (possible range 1-9 with higher scores indicating greater severity), and a mean severity of problems across settings (possible range of 1-9). In addition, four subscales are derived: Nonfamily Transactions, Custodial Transactions, Task Performance Transactions, and Isolate Play (Breen & Altepeter, 1991). The Nonfamily Transactions subscale assesses social-interpersonal situations in which the child is under public observation or the scrutiny of others. Custodial Transactions refers to situations in which there is an expectation to engage in self-help tasks such as getting dressed or bathing. The Task Performance Transactions subscale refers to situations in which there is a clear expectation to engage in an activity or chore. Finally, the Isolate Play factor refers to situations in which the child is engaged in a solitary activity (e.g., playing alone, watching television). Strong internal consistency and test–retest reliabilities (Altepeter & Breen, 1989; Breen & Altepeter, 1991; Pelletier, Collett, Gimpel, & Crowley, 2006), and good inter-rater agreement and criterion validity (Altepeter & Breen, 1989; Breen & Altepeter, 1991) have been reported for the HSQ. In the current sample, internal consistency was good for the HSQ (number of problems α = .80, severity α = .79). Given that sample sizes vary significantly for the severity items (i.e., if a parent did not endorse problem behavior in a situation then no value was provided for severity), we opted to substitute a 0 value (i.e., no severity rating) for those with missing values allowing us to retain the full sample for analyses of the severity ratings.
Disruptive Behavior Stress Inventory
The Disruptive Behavior Stress Inventory (DBSI) is a parent-rated measure designed to assess the frequency and degree of child behavior–related stress experienced by parents or primary caregivers (Reader et al., 2009). Parents responded to the 40-item measure by first reporting on a dichotomous (yes/no) scale whether they had experienced the stressor and then rating the degree of stress associated with that stressor on a 4-point Likert-type scale ranging from 0 (not at all stressful) to 3 (very stressful). The DBSI yields the Stress Experience Index, based on the sum of the total number of child behavior–related stressors that the parent has experienced, and the Stress Degree Index, based on the sum of stressfulness ratings for each stressor that was endorsed (Reader et al., 2009). The Stress Experience Index and the Stress Degree Index have shown strong internal consistency (Johnson & Reader, 2002). In the current sample, internal consistency was good (Stress Experience α = .89, Stress Degree α = .91).
Analyses
Independent t tests or chi-square comparisons were computed to assess whether demographic or clinical characteristics were different for participants with and without complete data. Paired samples t tests were computed to assess the impact of BPT on HSQ and DBSI ratings. Cohen’s d (Cohen, 1988) effect sizes were computed correcting for dependence between means (Morris & DeShon, 2002). Generally, effect sizes of ≥.2 are considered small, ≥.5 moderate, and ≥.8 large (Cohen, 1988). To further examine whether there was any specificity in the impact of BPT on specific situations listed in the HSQ, we conducted nonparametric McNemar tests investigating whether the proportion of yes responses (i.e., problem behavior was experienced in the situation) differed at pre and post for each item. Paired samples t tests were computed to compare severity ratings for each item. Multiple regressions were used to evaluate whether changes in situational variability and pervasiveness ratings are associated with changes in parental stress ratings. The p values for all analyses reported in Tables 2 to 4 were corrected for multiple comparisons using false discovery rate (FDR) procedures (Benjamini & Hochberg, 1995). Specifically, these procedures are used to reduce the number of false positive findings that may occur by chance [FDR = expected (# false predictions/# total predictions)].
Results of Paired Samples t Test Analyses.
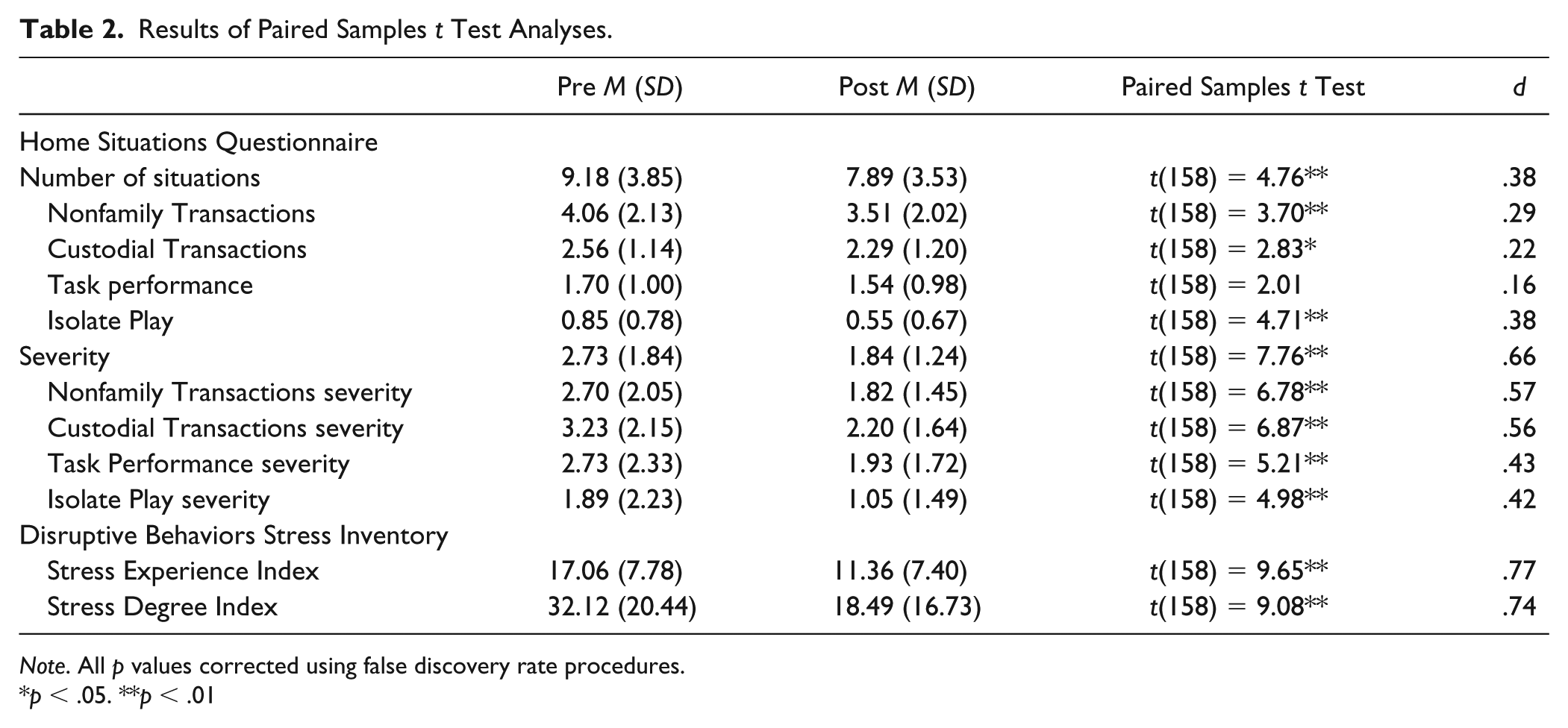
Note. All p values corrected using false discovery rate procedures.
p < .05. **p < .01
Home Situations Questionnaire Item Level Results.
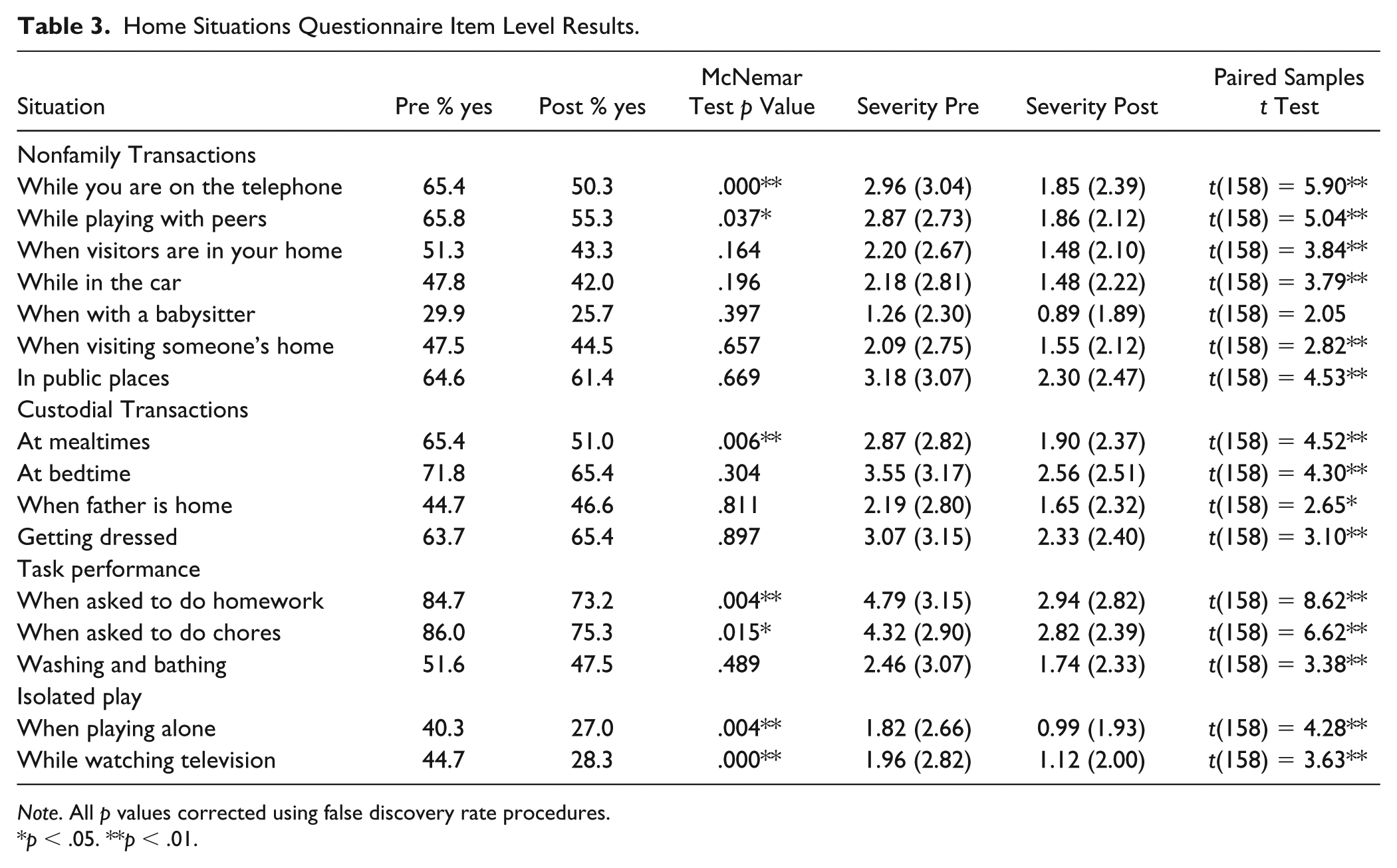
Note. All p values corrected using false discovery rate procedures.
p < .05. **p < .01.
Multiple Regressions Examining Whether Change in Situational Pervasiveness of Behavior Problems Predict Associated With Change in Related Parental Stress.
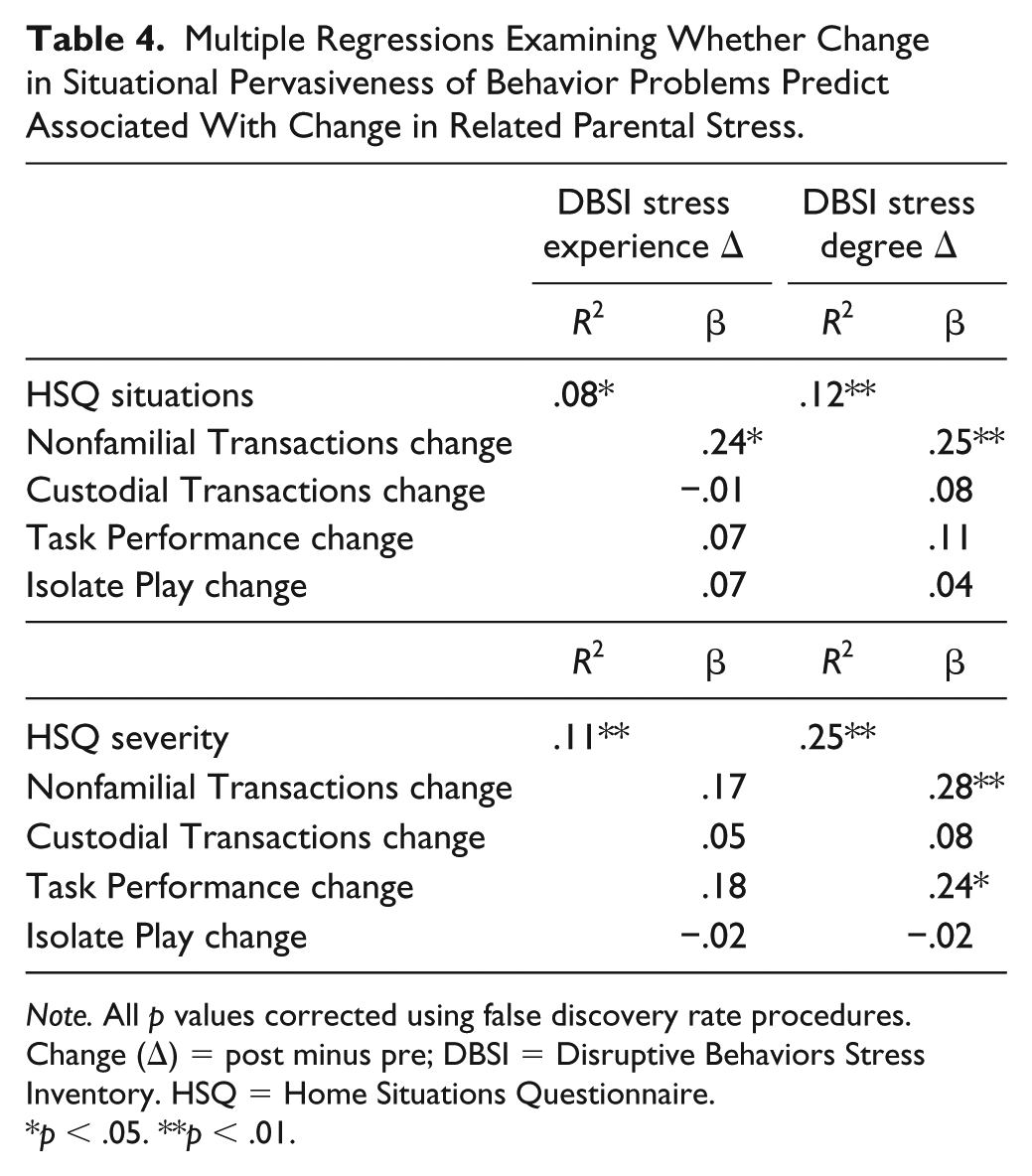
Note. All p values corrected using false discovery rate procedures. Change (Δ) = post minus pre; DBSI = Disruptive Behaviors Stress Inventory. HSQ = Home Situations Questionnaire.
p < .05. **p < .01.
Results
Missing Data Analyses
Approximately 57% of the sample had complete data (i.e., HSQ and DBSI measures at both time points). Those with incomplete data (i.e., HSQ, n = 122; DBSI, n = 114) did not differ in terms of child age (F(276) = 0.12, p = .726), child sex (χ2(1) = 1.23, p = .268), or number of situations reported on the HSQ (F(258) = 1.90, p = .169). There was no difference in DBSI stress experience (F(262) = .092, p = .762) or DBSI stress degree (F(261) = .247, p = .620) for those with and without complete HSQ data.
However, there were significant differences for those with and without complete HSQ data for race (χ2(4) = 10.59, p = .032; more parents of minorities had missing data) and ADHD subtype (χ2(3) = 11.31, p = .010; more children with subthreshold ADHD had missing data). There were also differences for those with and without complete data on the HSQ severity rating such that those reporting less severe problematic behaviors were more likely to have incomplete data (F(279) = 8.86, p = .003).
Primary Analyses
Results of the paired samples t test analyses revealed significant decreases for all subscale ratings on the HSQ except Task Performance after participating in the BPT group with effect sizes ranging from .22 to .38 (small) for number of situations and from .42 to .57 (small to moderate) for severity ratings (see Table 2). Similarly, significant decreases for both DBSI index scores after participating in the BPT group were observed with effect sizes >.7 (moderate; see Table 2).
Item-level analyses show that there were significantly fewer yes responses after BPT for the following situations on the HSQ: playing with peers, while parent is on the phone; at mealtimes, when child is asked to do chores and homework; and while child is playing alone or watching television (see Table 3). Severity ratings were significantly decreased for all situations except for when the child is with a babysitter.
Exploratory Analyses
Results examining the HSQ situation subscales showed that reduced number of problem behaviors in the Nonfamilial Transactions was associated with decreases in both the DBSI Stress Experience and Stress Degree Index ratings. For HSQ severity ratings, a slightly different pattern emerged. Reductions in both HSQ Nonfamilial Transactions and Task Performance severity ratings were associated with decreases in the DBSI Stress Degree Index but not the DBSI Stress Experience Index (see Table 4).
Discussion
In the current study, we investigated whether BPT would affect the situational variability and pervasiveness of behavior problems (noncompliance), as well as parenting stress levels. We also explored whether changes in HSQ subscale ratings were associated with reductions in child behavior–related parenting stress, which is important to document given that parental stress is associated with multiple negative sequelae including poor parenting practices, treatment dropout, and so on. Results showed that after BPT, parents reported fewer and less severe problematic situations related to child noncompliance, particularly for chores, homework, mealtimes, and peer interactions. Parents also reported significantly reduced stress related to parenting a child with ADHD. Improvements in Nonfamilial Transactions and Task Performance were associated with reductions in degree of parental stress.
Although evidence-based practices for mental health problems, including ADHD, have been identified for children, the science of disseminating and implementing these practices into real-world settings has received considerably less attention. In fact, poor uptake of such practices in usual care settings remains one of the major barriers to providing safe, effective, and efficient mental health care (Novins et al., 2013). Demonstrating the effectiveness of BPT in the outpatient setting for improving meaningful outcomes (e.g., reducing functional impairment, parental stress) is critically important to ensure that patients with ADHD receive state-of-the-art treatment addressing the issues that cause parents to seek treatment (Angold et al., 1998). Barkley eloquently argued that it is important to capture the frequency as well as situational variability and pervasiveness of behaviors (i.e., number of situations in which problematic behaviors occur) to fully elucidate the functioning of children with ADHD (Barkley & Edlebrock, 1987).
Our results showed that after completing BPT, parents reported significant reductions in both the frequency and severity of behavior problems across a variety of situations, along with reductions in related parenting stress. The findings of reductions in both the number of problem situations and severity of problem behaviors on the HSQ replicate those reported in previous studies using the HSQ (Lauth et al., 2009; Malik & Tariq, 2014; Shata et al., 2014; Varnado et al., 2014). At the situational level, parents reported seeing significantly fewer problem behaviors during homework, chores, and mealtimes, during play (both alone and with peers) and while parent is on the phone. Importantly, arguments related to homework, chores, and mealtimes are frequently situations that cause family stress and impairment, which are often the reason parents seek treatment for their child’s ADHD. Furthermore, parents reported reduced severity ratings across all situations, including those in which the frequency of problematic behaviors was not significantly reduced. Thus, our findings suggest that BPT is effectively addressing problematic child behaviors across a broad range of situations that cause impairments in daily functioning that parents find stressful. Our findings add to the literature reporting that BPT positively impacts children’s functioning in a number of domains assessed by the IRS (Chacko et al., 2008; Chacko et al., 2009; Fabiano et al., 2009) and, in particular, the impact of the child’s behavior on the family (Loren et al., 2017; Loren et al., 2015).
Although significantly fewer situations in which children exhibited problem behaviors were endorsed at post than pre, effect sizes were relatively small for this outcome compared with reductions in severity and parental stress (Table 2). In addition, there were still a number of situations in which parents reported experiencing behavior problems (Table 3). Nonetheless, the severity of these endorsed problems was reduced with large effect sizes, and parents also reported significantly less stress. These findings suggest that children with ADHD still exhibit noncompliance in various situations, even after their parents receive BPT, but that the impact and stress related to these behaviors are significantly reduced. This may be partly due to parents’ feeling more confident in their ability to manage their children’s problematic behaviors. This hypothesis is consistent with previous findings that BPT results in improvements in parenting confidence for parents of children with ADHD (Loren et al., 2015). The finding of reduced parental stress is critical given the literature showing that parents of children with ADHD report higher levels of stress (Paidipati & Deatrick, 2015), and findings that although parents with higher levels of stress may have higher levels of attrition, those who complete a BPT program also report larger decreases in their parental stress (Lauth et al., 2009). Furthermore, reduced parental stress has previously been associated with better child outcomes (e.g., reduced ratings of child ADHD severity; Anastopoulos et al., 1993), whereas low parenting efficacy is associated with poorer child treatment outcomes (Hoza et al., 2000).
Limitations
There are several limitations to the current study. Because data were derived from a clinical setting and not a formal research study, there is limited information available regarding the sample. For example, no information was available about family income, family composition (e.g., two parent or single parent, number of siblings), parent education, parental psychopathology, parenting style, and so on, which could contribute to treatment outcomes; such information is critical to advance the effectiveness literature given that recent reviews are reporting significant nuance in the BPT efficacy literature with regard to sample characteristics (e.g., diversity and education; Evans et al., 2017). In addition, detailed information regarding who attended BPT sessions (mother, father, or both), the number of sessions attended, or child medication use was not available. Furthermore, there was a high rate of missing data. Thus, our findings may have been biased by the fact that the attendees who were benefiting stayed in treatment and therefore rated positive behavior changes. Relatedly, the fact that it was the parents attending BPT who also completed the rating scales may have also biased findings in a positive direction. The fact that parents knew they were receiving an empirically based intervention may have biased their reports of reductions in problematic child behaviors and parenting stress due to a belief that treatment “should” work.
Parents of children with less severe ADHD and less severe problematic behavior were less likely to have complete HSQ data, perhaps reflecting inconsistent attendance or a higher dropout rate due to parents perceiving treatment was not as necessary for their child. On the contrary, it is potentially a strength that our findings demonstrated the efficacy of BPT on compliance and stress in a more severe population of children. There were also fewer parents of minorities with complete data which is consistent with the literature showing a higher rates of missing data for minorities (Brouwer, Mosack, Wendorf, & Sokolova, 2013; Feskens, Hox, Lensvelt-Mulders, & Schmeets, 2006; Fongwa et al., 2010). Thus, our findings may not generalize to these populations or to less severe cases.
While a strength of our study is that it demonstrates real-world benefits of BPT for families of children with ADHD, the fact that it is based on a sample drawn from parents seeking treatment for their child’s ADHD in a clinical setting introduced other potential weaknesses or limitations. For example, a formal diagnostic evaluation for ADHD that included ratings from both parents and teachers and assessed for comorbidities was not conducted. While this could potentially limit the generalizability of our results, it is also likely to reflect a common reality in real-world clinical settings. Because families were paying for the services they received, a comparison waitlist or placebo treatment control group could not be used to detect possible effects of bias or nonspecific effects of treatment. However, given the large body of research that has demonstrated the efficacy of BPT for children with ADHD, it is reasonable to assume that the findings from this study are a result of the treatment program. A final limitation is the naturalistic medication status of children in the present study, with no consistent tracking of medication use or changes in medication status over the course treatment, which precludes our ability to examine possible moderating effects of medication. We cannot rule out the hypothesis that functional improvements resulted from children either being started on medication or having changes made in their medication dose over the course of BPT. It should be noted, however, that one study reported that medication status did not impact the effectiveness of BPT offered in a mental health outpatient clinic, and, in fact, that study reported that BPT may limit the prescription of poly-pharmaceutical treatment (van den Hoofdakker et al., 2010). Furthermore, the proportion of cases who concurrently started medication and BPT is not expected to be high given there is no systematic referral to a psychiatrist at the same time as the referral to BPT in the clinic, and the intake staff are all trained to suggest BPT as an approach to consider prior to initiating medication. However, this cannot be verified with the available data.
Conclusion
Our findings suggest that in real-world clinical settings, BPT for parents of children with ADHD results in significant reductions in the severity of child noncompliance across a broad range of situations along with milder reductions in the number of situations in which noncompliance occurs, which results in significant reductions in related parenting stress. Because a major reason parents of children with ADHD seek treatment for their child is the negative impacts of their child’s ADHD-related behaviors on daily family life, these findings provide further evidence that BPT is an effective way to reduce the negative impacts of ADHD on the daily lives of children and their families. Our findings also suggest that measures such as the HSQ may be useful in clinical practice as a means of measuring the impact of treatment on the aspects of a child’s behavior that are most likely to lead parents to seek treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.