
Abstract
Keywords
Adolescence is marked by an acute risk for elevated depressive symptoms, with the likelihood of depression onset increasing substantially with puberty. An important line of research examines growth in depressive symptoms over time, finding distinct developmental trajectories of depressive symptomatology. This body of work has identified normative growth patterns of depressive symptoms, such that symptoms tend to decrease in prepubescent children and generally increase around ages 13 to 14 (Dekker et al., 2007; Garber, Keiley, & Martin, 2002; Ge, Conger, & Elder, 2001). The developmental patterns observed in the symptom onset and trajectories of depression support a nuanced approach to evaluating risk and/or prognostic factors that influence the onset and course of depressive symptoms in adolescence.
Symptoms of ADHD constitute one such risk factor for the development of depressive symptoms in adolescence. Indeed, a substantial literature suggests that adolescents with ADHD experience significantly more depressive symptoms compared with same-aged peers without ADHD. Findings from prospective longitudinal research indicate that ADHD is associated with higher levels of depressive symptoms (Elia, Ambrosini, & Berrettini, 2008; Lee et al., 2008), and that youth with ADHD are at an increased risk of developing unipolar depressive disorders in adolescence (e.g., Biederman et al., 2008). Strikingly, children with ADHD have been shown to be at 500% greater risk for depression by age 18 relative to typically developing children (Chronis-Tuscano et al., 2010).
Symptoms of ADHD and depression co-occur at rates that far exceed those expected by chance, but the effect of adolescent ADHD on the course of depressive symptoms across adolescence remains largely underexamined. The only known study to examine the intercept (at age 18) and slope (from ages 18-25) of depressive symptoms as a function of ADHD is that of Meinzer and colleagues (2016), who demonstrated that differences in the trajectories of depressive symptoms between ADHD and non-ADHD groups were evident by age 18. Furthermore, a childhood history of ADHD significantly predicted depressive symptoms at age 18, even after controlling for co-occurring psychiatric diagnoses. In light of these findings among young adults with ADHD, an important direction is to investigate the ways in which youth ADHD symptoms shape the development of depressive symptoms across adolescence.
Maternal Emotion Regulation (ER) Difficulties Moderate Depressive Trajectories
Adolescence is considered a critical developmental period for depression risk among youth with ADHD symptomatology, with depressive symptoms likely emerging before age 18 (Meinzer et al., 2016). Despite the fact that ADHD is a risk factor for later depressive symptoms, substantial heterogeneity exists in the relation between ADHD and depression outcomes (Meinzer, Pettit, & Viswesvaran, 2014). Therefore, an important step in better understanding this longitudinal association is to use a dynamic approach to examining adolescent depressive symptoms over time as a function of ADHD symptomatology and the presence of key moderators.
One such moderator may be maternal difficulties in ER, a transdiagnostic correlate of adolescent depression and psychosocial adjustment (Cumsille, Martínez, Rodríguez, & Darling, 2015; Hankin, 2015; Morris, Silk, Steinberg, Myers, & Robinson, 2007). Maternal ER, defined as the ability to monitor, assess, and change emotional responses in service of one’s goals (Thompson, 1994), is thought to affect youth outcomes via its interaction with youth characteristics (Granic, 2005; Katz et al., 2014; Morris et al., 2007). This approach is consistent with an increasing emphasis on understanding the ways in which transdiagnostic predictors, rather than disorder-specific symptoms/behaviors, impact youth development over time (i.e., Klemanski, Curtiss, McLaughlin, & Nolen-Hoeksema, 2017).
Following a developmental-transactional framework of ADHD in families (Johnston & Chronis-Tuscano, 2015), maternal ER may play a crucial role in adolescent depressive symptom trajectories, especially for youth with ADHD. Youth with ADHD often evoke negative responses from individuals within their social contexts and, given their symptoms and impairments, often require significant parental support and scaffolding more generally, but also specifically within the context of learning to manage their emotions and behaviors (Chronis-Tuscano et al., 2016; Mazursky-Horowitz et al., 2018). Adolescents with ADHD are also thought to accrue failure and frustration experiences and may be especially prone to experiencing depressive symptoms with a dysregulated primary caregiver (e.g., mother) who fails to provide emotional scaffolding and support during this tumultuous developmental period. Therefore, it may be especially important for mothers of adolescents with ADHD to be emotionally regulated, thereby mitigating youth depression risk and symptom trajectories over time.
The Current Study
An important direction in unpacking adolescent depression risk is to examine the independent and interactive effects of maternal ER difficulties and adolescent ADHD symptoms on adolescent depressive symptoms. The current study will address notable gaps in the literature on ADHD and depression by examining the role of Oppositional Defiant Disorder/Conduct Disorder (ODD/CD) and including youth with subclinical levels of ADHD and depressive symptomology. Given that ADHD co-occurs with ODD/CD (hazard ratio = 9.54; Yoshimasu et al., 2012), that externalizing disorders more broadly are associated with depressive disorders (Loth, Drabick, Leibenluft, & Hulvershorn, 2014), that youth with ADHD and co-occurring externalizing concerns exhibit higher levels of depression relative to those with ADHD alone (Ostrander, Crystal, & August, 2006), and that ODD/CD are often characterized by negative affectivity/irritability, which is a developmental correlate and/or precursor to internalizing symptoms such as depression (Evans et al., 2017; Nock, Kazdin, Hiripi, & Kessler, 2006), it is important to include externalizing symptoms in models examining ADHD and depression risk, even in a community sample with relatively low base rates of psychopathology such as ours.
Much of the existing research on ADHD and co-occurring depression has examined youth meeting diagnostic criteria for either disorder, despite accumulating evidence of impairment and risk for developing co-occurring mental health difficulties in subthreshold cases (Bussing, Mason, Bell, Porter, & Garvan, 2010; Kats-Gold, Besser, & Priel, 2007; Keenan, Hipwell, Duax, Stouthamer-Loeber, & Loeber, 2004; Keenan et al., 2008; Seymour, Chronis-Tuscano, Iwamoto, Kurdziel, & MacPherson, 2014). In their longitudinal sample of children ages 5 to 11, Bussing et al. (2010) found that children with subthreshold ADHD symptoms were significantly impaired across development, with higher risk for graduation failure and grade retention. Furthermore, those with clinically elevated ADHD symptoms (SD = 1.5 above the mean) evidenced significant differences in comorbid internalizing symptoms. More recently, in a sample of native-born Japanese youth, Kita and Inoue (2017) found that teacher-reported symptoms of inattention predicted low self-esteem with an indirect effect on depressive symptoms, even among subclinical ADHD cases. This study also showed a significant direct effect of ODD symptoms on depression, reinforcing the importance of including externalizing symptomatology in models of ADHD and depression. Finally, in their population-based study, Roy, Oldehinkel, Verhulst, Ormel, and Hartman (2014) found that 36% of children with ADHD, 24% with subthreshold symptoms, and 14% with no ADHD presented with co-occurring depression, supporting elevated risk even in subthreshold ADHD cases.
Taken together, these studies show the complex associations between continuous ADHD symptoms and the development of co-occurring internalizing symptoms, supporting further examinations of the impact of adolescent ADHD symptoms on co-occurring symptom trajectories outside of clinical populations, alone, and including ODD/CD symptoms in models of risk. Consistent with a dimensional approach to measurement, which shows more reliability and validity relative to dichotomous conceptualizations (see Markon, Chmielewski, & Miller, 2011 for a meta-analytic review), the current study aimed to examine the independent and interactive effects of youth ADHD symptoms and maternal ER difficulties on the trajectory of youth depressive symptoms across adolescence. The current study represents secondary data analyses of a community-based longitudinal sample of adolescents (Mage at the current study baseline = 13.06). Youth ADHD symptoms were hypothesized to be positively associated with baseline depressive symptomatology. Maternal ER difficulties were hypothesized to exacerbate the effect of youth ADHD symptoms on youth depression symptoms over time, such that youth with more ADHD symptoms whose mothers reported more total ER difficulties would experience the greatest increases in depressive symptoms across adolescence (Mages 13.06-18.05).
Method
Participants and Procedures
Participants in the current study took part in a larger, 10-year longitudinal project examining the development of risky behaviors (Collado, Felton, MacPherson, & Lejuez, 2014; Cummings et al., 2013). Youth and their parents were recruited from the community with fliers and media outreach in schools, libraries, and youth organizations. Families were evaluated for inclusion based on three criteria: (a) having a child between the ages of 9 and 13 (Mage = 11.00, SDage = 0.81); (b) proficiency in English; and (c) the ability to participate in annual assessments. Data were collected each year in a university-based laboratory setting and youth and their participating caregivers received up to US$40 for each wave of data collection they completed. Participants at the first wave of data collection included N = 277 adolescents and their parents.
Because maternal ER measures were not included until the third wave of data collection, the current analyses utilized data from Waves 3 to 8 (labeled T1-T6 for clarity). Of the original sample of 277 youth, 247 (56% male) participated in Wave 3 (T1). The sample sizes for all subsequent years (T2-T6) were N = 233, N = 213, N = 193, N = 154, and N = 154, respectively. At T1, youth participants were, on average, 13.06 years old (range 11-15, SDage = 0.90) and 18.05 (range 15-20, SDage = .97) at T6. Participating mothers ranged from 28 to 57 years old at T1 (Mage = 44.09, SDage = 6.07). Race/ethnicity reflected the demographic breakdown of the area from which participants were drawn: 52.5% identified as White/Caucasian, 37.7% identified as Black/African American, 1.6% identified as Asian, and 8.2% identified as “Other race/ethnicity.” Annual family incomes, as reported by mothers, ranged from US$0 to US$325,000 (Mincome = US$102,498, SDincome = US$56,350). The sample was relatively well-educated, with approximately 29% having completed college, and 33% completed an advanced degree. Mean levels of depression symptoms (M = 9.46, SD = 8.25, range = 0-45), measured utilizing the Center for Epidemiological Studies–Depression (Radloff, 1977), were consistent with other community-based samples of women (e.g., Knight, Williams, McGee, & Olaman, 1997). Moreover, mothers reported a mean score of 12.11 (SD = 7.66, range = 0-46) on the Conners’ Adult ADHD Rating Scale–Investigator Rated: Screening Version (CAARS-Inv:SV; Conners, Erhardt, & Sparrow, 1999).
Measures
Demographics
Given prior research suggesting important variations in depressive symptoms based on age, race/ethnicity, and sex (Ge, Conger, & Elder, 2001; Van Voorhees, Paunesku, Fogel, & Bell, 2009), mothers were asked to report their child’s demographic information at study visits. Race/ethnicity was dichotomized to represent (1) White/Caucasian and (0) non-White youth.
Depressive symptoms
Children’s self-reported depressive symptoms were assessed using the Depression subscale from the Revised Children’s Anxiety and Depression Scale (RCADS-D; Chorpita, Yim, Moffitt, Umemoto, & Francis, 2000). The RCADS-D is a 10-item subscale that asks participants to rate how often they experience a feeling or behavior, such as “I feel sad or empty” and “nothing is much fun anymore.” Each item is ranked on a 4-point rating scale, ranging from 0 = never to 3 = always. Total scores were computed by adding all items together, with scores ranging from 0 to 30 and higher values representing greater levels of depressive symptoms. The RCADS has been shown to be both reliable and valid, including in late adolescent/emerging adult samples (Bouvard, Denis, & Roulin, 2015; Chorpita, Moffitt, & Gray, 2005; de Ross, Gullone, & Chorpita, 2002; Mathyssek et al., 2013). Coefficient alphas ranged from .80 to .87 across T1 through T6.
Maternal ER difficulties
Participants’ mothers completed the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) to assess maternal ER difficulties at T1. The DERS is a 36-item self-report measure, which asks individuals to respond to questions on a 5-point rating scale, ranging from 1 = almost never to 5 = almost always. Total scores range from 36 to 180 and are created by summing all items. Higher scores reflect greater difficulty regulating one’s emotions. Prior research demonstrated strong reliability and validity in adult samples (Gratz & Roemer, 2004). Coefficient alpha in the current sample was .80 at T1.
Child ADHD and ODD/CD symptoms
Parents reported on youth symptomatology at T1 using the Disruptive Behavior Disorders checklist (DBD: Pelham, Gnagy, Greenslade, & Milich, 1992). From the DBD, two subscales were derived: ADHD and ODD/CD symptoms. Parents rated their children’s behaviors from 0 = not at all to 3 = very much, such as “often interrupts or intrudes on others (e.g., butts into conversations or games)” and “often does not seem to listen when spoken to directly.” Subscale items were summed together to create total scores, with higher scores reflecting greater symptomatology. The DBD has been shown to have excellent psychometric properties (Pelham et al., 1992). In the current study, coefficient alpha was .94 at T1 for ADHD symptoms, .80 for ODD symptoms, and .70 for CD symptoms.
Data Analytic Approach
To evaluate the hypotheses, we examined a series of structural equation models. First, we sought to evaluate change in depressive symptoms over a 6-year period using latent growth modeling (LGM). LGM can model both inter- and intra-individual change over time, as well as predictors of this change. All analyses were conducted using Mplus 6.0 (Muthén & Muthén, 2010) with full information maximum likelihood (FIML) estimation methods. FIML algorithms estimate missing parameters utilizing all available data (Little & Rubin, 1989), meaning that all participants (N = 247) contributed to the estimation of model parameters.
Each model was first evaluated based on model fit criteria. We examined four main indices of fit: the chi-square statistic, the Comparative Fit Index (CFI; Bentler, 1990), Tucker-Lewis Index (TLI; Tucker & Lewis, 1973), and the Root Mean Square Error of Approximation (RMSEA; Steiger, 1990). Model fit criteria suggest that CFI and TLI of .90 are acceptable (Schweizer, 2010) and .95 (Hu & Bentler, 1999) suggest good fit, while RMSEA values below .08 are acceptable (MacCallum et al., 1996) and values below .06 indicate good fit (Hu & Bentler, 1999). While nonsignificant chi-square values indicate good fit, this statistic is influenced by sample size, and significance may reflect nonmeaningful differences between the proposed model and the data in large samples.
We first examined an unconditional growth model. All factors were indicated by the manifest depressive symptom scores at T1 through T6. Initially, an intercept-only model (indicating no change in depressive symptoms) was fit to the data by constraining the regression weights from each manifest variable to the latent intercept factor to be 1.0. If model fit was unacceptable, a latent slope factor (representing linear change over time) was added to the model by constraining the regression weights from T1 through T6 to this factor to be 1.0, 2.0, 3.0, 4.0, 5.0, and 6.0, respectively. Improvement in model fit was evaluated using a chi-square difference test. Subsequent growth parameters were added as needed, to reflect more complicated trends (i.e., quadratic, cubic). The most parsimonious model evidencing the best absolute fit was selected. We then examined the means and variances of the latent intercept and growth factor. A significant mean would suggest the factor is different than zero while a significant variance indicates important individual differences around this estimate, supporting the inclusion of predictors of these differences.
Finally, we examined a conditional LGM, in which we regressed the latent intercept and growth factors onto ADHD symptoms, maternal ER difficulties, and their interaction, controlling for ODD/CD symptomatology. Given the established literature on sex, age, and race/ethnicity differences in rates of depressive symptoms (Ge, Conger, & Elder, 2001; Van Voorhees et al., 2009), these demographic factors were also added to the model.
Results
Preliminary Analyses
Patterns of missingness within the data were examined in two ways. First, we conducted a Little’s missing completely at random (MCAR) test, which indicated the data were MCAR: χ2 (188) = 166.93, p = .863. Next, we looked at correlations between baseline values of key constructs and subsequent retention. Age at baseline had a small correlation with T5 attendance (r = −.18), and sex was associated with T6 attendance (r = .15); no other variable predicted participation in later waves of data. Means, standard deviations, and correlations between key variables are presented in Table 1. Of note, maternal ER difficulties were correlated with child ADHD scores, such that mothers with poorer ER reported that their children had higher levels of ADHD symptoms.
Means, Standard Deviations, and Correlations Between Key Study Variables.
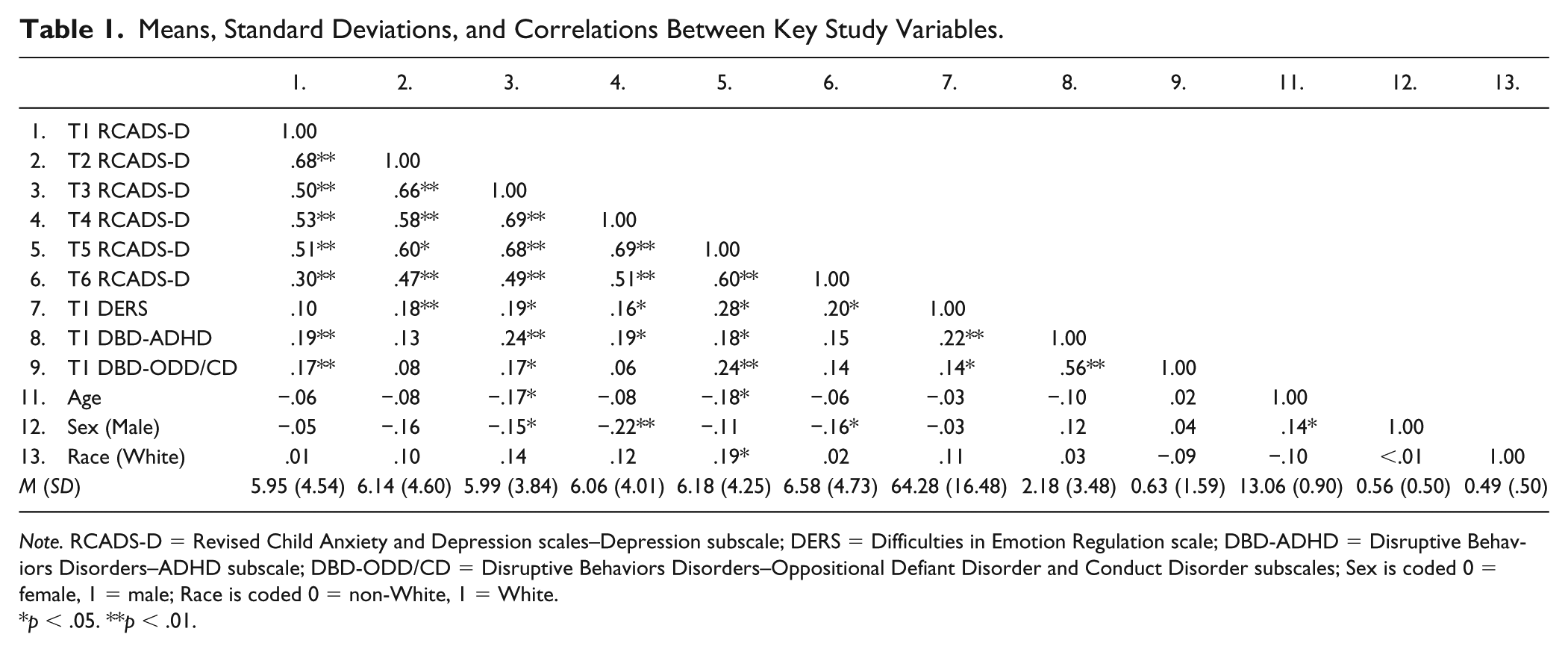
Note. RCADS-D = Revised Child Anxiety and Depression scales–Depression subscale; DERS = Difficulties in Emotion Regulation scale; DBD-ADHD = Disruptive Behaviors Disorders–ADHD subscale; DBD-ODD/CD = Disruptive Behaviors Disorders–Oppositional Defiant Disorder and Conduct Disorder subscales; Sex is coded 0 = female, 1 = male; Race is coded 0 = non-White, 1 = White.
*p < .05. **p < .01.
Unconditional Latent Growth Curve
Next, we examined depressive symptoms using an intercept-only model. This model failed to provide an adequate fit to the data: χ2(df = 19) = 62.43, p < .001; CFI = .93; TLI = .94; RMSEA = .09 (90% CI = [0.07, 0.12]). Adding a linear growth term significantly improved the fit of the data: Δχ2 = 26.24, Δdf = 3, p < .001. The resulting model fit the data well: χ2(df = 16) = 36.19, p = .002; CFI = .97; TLI = .97; RMSEA = .07 (90% CI = [0.04, 0.10]). The mean of the intercept (M = 5.90, SE = 0.27, p < .001) suggested that baseline levels of depressive symptoms were significantly greater than zero. The slope, however, was not significant (M = 0.10, SE = 0.07, p = .117), indicating that youth, on average, do not evidence increased depressive symptoms over time. Both the variances of the intercept (Var. = 13.54, SE = 1.66, p < .001) and the slope (Var. = 0.40, SE = 0.01, p < .001) were significant, indicating individual differences around these parameters and supporting the addition of predictors to the model. Moreover, the mean and slope factor were significantly correlated with one another (r = −.41, p = .005), indicating that youth who started with higher levels of baseline depressive symptoms experienced steeper decreases in depressive symptoms across adolescence.
Conditional Latent Growth Curve
Using a model building approach, we next added the control variables (ODD/CD symptoms, sex, race/ethnicity, and age at baseline) as well as the main effects (youth ADHD symptoms and maternal ER difficulties) as predictors of the latent intercept and slope. This model fit the data well: χ2(df = 40) = 68.84, p = .003; CFI = .95; TLI = .93; RMSEA = .06 (90% CI = [0.03, 0.08]). Only youth ADHD symptoms were a significant predictor of the intercept (std. est. = .20, p = .030), indicating that elevated T1 ADHD symptomatology was associated with higher levels of T1 depressive symptoms. None of the predictors was significantly associated with the slope.
Finally, we added an interaction term between ADHD symptoms and maternal ER difficulties to the model. Again, the model fit the data well: χ2(df = 44) = 74.81, p = .003; CFI = .94; TLI = .93; RMSEA = .06 (90% CI = [0.03, 0.08]). The interaction term was associated with the intercept at trend level (std. est. = −.70, p = .050) and significantly predicted the slope (std. est. = 1.13, p = .029; see Figure 1). To probe this interaction further, we then ran a post hoc multigroup model by splitting the sample at the mean for maternal DERS scores. We examined the relation between ADHD symptoms and the slope of depressive symptoms in both groups, retaining all control variables. Results suggest that the path estimates significantly differed between youth in the low maternal ER difficulties group (std. est. = −2.25) and the high maternal ER difficulties group (std. est. = −.09). In other words, youth with more T1 ADHD symptoms whose mothers evidenced more T1 ER difficulties demonstrated greater increases in depressive symptoms across adolescence relative to their peers with lower ADHD symptoms or youth of mothers with less ER difficulty (see Figure 2).
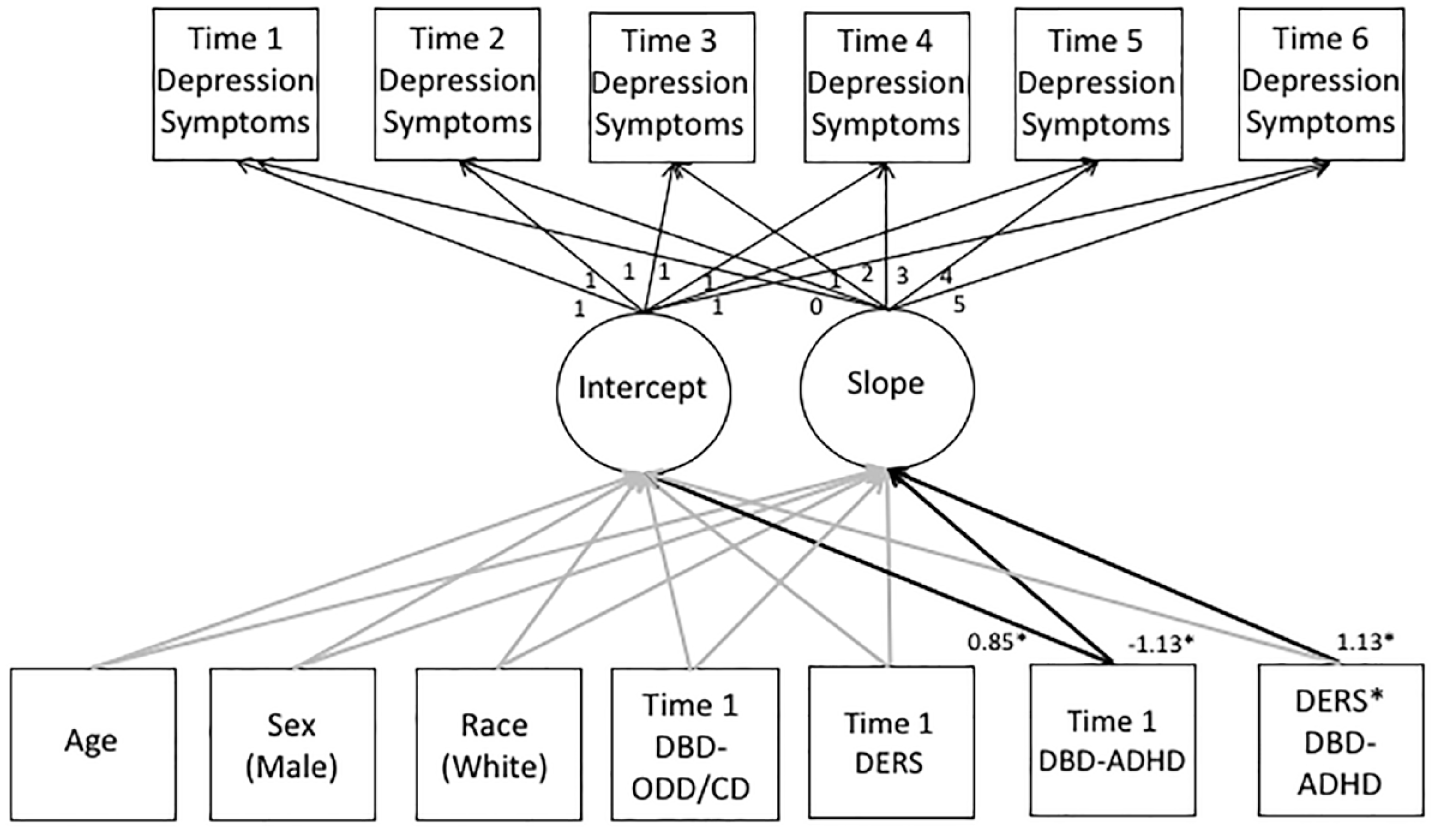
Standardized path estimates for the final growth curve model.
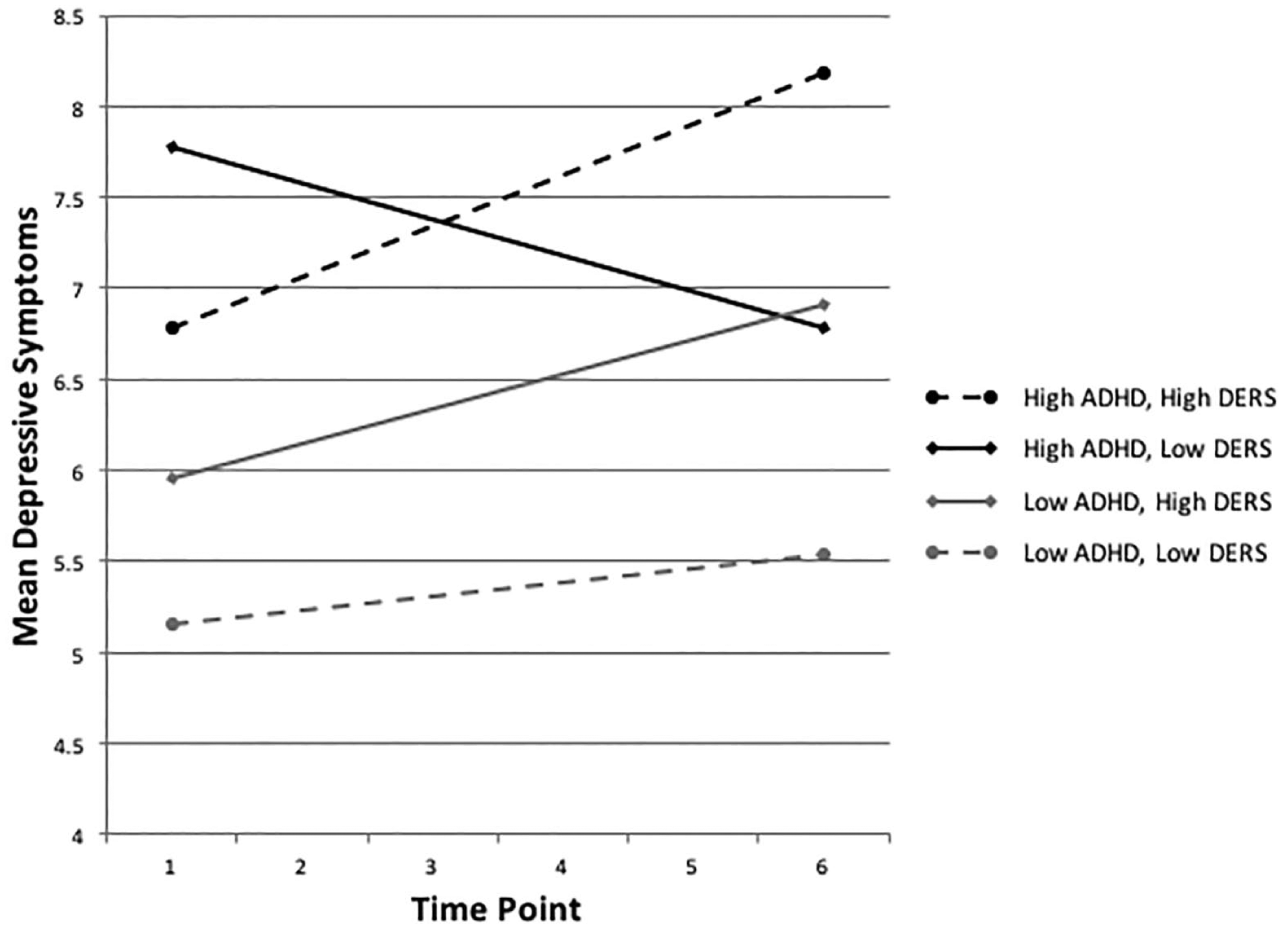
Linear trajectories of depressive symptoms in youth with low and high levels of ADHD symptoms and maternal emotion dysregulation.
Discussion
Adolescent development is marked by an acute risk for depressive symptoms, and youth with ADHD are thought to experience elevated depressive symptoms by the age of 18 (Meinzer et al., 2016). However, significant heterogeneity exists in the longitudinal association between ADHD and depressive symptoms, supporting the presence of moderators. Identification of moderators can inform targets for prevention and treatment of depression among youth with ADHD. Consistent with a developmental psychopathology framework, the current study employed a well-defined, longitudinal community sample of adolescents with varying levels of ADHD and depressive symptoms to evaluate the trajectories of depressive symptoms as a function of the independent and interactive influences of youth ADHD symptoms and maternal ER difficulties across a critical developmental risk period (Johnston & Chronis-Tuscano, 2015; Morris et al., 2007). The present analyses suggest that maternal ER difficulties amplify the trajectory of youth depressive symptoms in the context of higher youth ADHD symptoms, controlling for co-occurring symptoms of ODD/CD. This work promotes a better understanding of the role of maternal ER difficulties in shaping the course of depressive symptoms in adolescents with ADHD symptomatology, with implications for maternal ER as an important intervention target in the context of depression risk among youth with symptoms of ADHD.
The present findings are consistent with individual differences in the trajectories of depressive symptoms over time, supporting the need to examine specific individual characteristics that confer risk across adolescent and young adult development. Results from the conditional latent growth curve model suggest significant associations between ADHD symptomatology, but not maternal ER difficulties, on initial depressive symptoms. Importantly, these results held in the context of controlling for covariates such as ODD/CD symptomatology and support the established link between ADHD, specifically, and concurrent depression symptoms (Meinzer et al., 2014). Moreover, even in a community sample with relatively low rates of ADHD symptoms, the current study found that ADHD symptomatology was significantly and positively associated with adolescent-reported depressive symptoms, controlling for important covariates. This finding adds to the growing research using nonclinical samples of youth and is consistent with the idea that subclinical symptomology, even low levels of ADHD symptoms on average, is an important indicator of risk for experiencing depressive symptoms in adolescence.
ADHD symptoms were associated with the intercept of depressive symptoms, yet neither ADHD symptoms nor maternal ER showed significant main effects on the slope of depressive symptoms across adolescence. That is, in the context of the current study, neither T1 ADHD symptoms nor T1 maternal ER difficulties alone conferred risk for increasing depression trajectories across adolescence. Developmental models of child adjustment propose an interactive effect of maternal ER and youth characteristics on youth outcomes (Beauchaine, 2015; Morris et al., 2007). The present findings, combined with the significant effect of the interaction term on the latent slope of depressive symptoms, align with this transactional hypothesis such that it was the interaction between maternal ER difficulties and youth ADHD symptoms that predicted the unfolding of adolescent depressive symptoms over time. Therefore, it may be the case that adverse youth outcomes such as depression result not from either youth or maternal characteristics alone, but rather the transactional risk of these characteristics over time (Johnston & Chronis-Tuscano, 2015). Interestingly, the interaction term was only marginally related to initial latent depressive symptoms, supporting the possibility that maternal ER difficulties pose an especially salient risk factor for worsening depressive symptoms across adolescence for youth with more ADHD symptoms. This also underscores the importance of targeting maternal ER difficulties in depression prevention for youth with symptoms of ADHD across adolescent development.
Overall, these findings suggest that youth with more ADHD symptoms whose mothers report greater ER difficulties are especially likely to show an increasing trajectory of depressive symptoms across adolescence, highlighting important directions for future work. Future research will be needed to elucidate the processes underlying the effect of maternal ER difficulties and youth ADHD symptoms on the slope of depressive symptoms over time, controlling for key covariates as in the current study. For example, future studies may ask: What are the mechanisms underlying the development of depressive symptoms among youth with ADHD whose mothers experience more ER difficulties? It may be that maternal ER difficulties interfere with effective parenting, leading to increases in depressive symptoms among these youth. Indeed, adolescence represents a time of markedly advancing cognitive and emotional functioning, and caregivers are important agents of promoting health and well-being. Given the symptom constellation of ADHD and associated impairments, adolescents with ADHD may be especially likely to develop depressive symptoms when the ER difficulties of their primary caregivers interfere with responsive parenting (i.e., parental responses to adolescents’ expressions of emotions).
Another direction is to examine whether maternal ER difficulties increase stress and parent-child conflict for youth with ADHD, thereby amplifying depressive symptoms over time. Research shows that parents of adolescents with ADHD report using poorer parenting strategies and show greater levels of hostility and rejection relative to parents of non-ADHD youth (Johnston & Mash, 2001; Lifford, Harold, & Thapar, 2008). The ability to regulate emotions in parenting may compound the effects of such parenting problems (Johnston & Chronis-Tuscano, 2015), thereby increasing parent-child stress and conflict and leading to increases in youth depression symptoms across adolescence. An additional line of research is needed to comprehensively evaluate multiple distinct components of maternal ER difficulties as they interact with youth ADHD symptoms to predict the trajectories of adolescent depressive symptoms. Such results would shed light on the extent to which certain components of maternal ER (e.g., emotional impulsivity) are particularly costly to adolescent well-being.
Future research may also evaluate the simultaneous changes in maternal ER as a function of changes in adolescent depressive symptoms and vice versa over time. In addition, including time-varying disruptive behaviors and other commonly co-occurring difficulties among youth with ADHD symptoms (i.e., substance use) would also provide additional insights into the nature and development of depressive symptoms. Relatedly, future research should consider whether depressive symptoms at T1 (and beyond) predict worsening ADHD symptomatology and/or related impairments (i.e., academics, social), and whether such an effect may be moderated by maternal ER.
Limitations
Although the current study contributes to a better understanding of the trajectories of depressive symptoms as a function of youth ADHD symptoms and maternal ER difficulties, is bolstered by a large sample of community adolescents, and benefits from a prospective longitudinal design, these findings should be considered in the context of its design limitations. A main limitation of the study is the sole focus on maternal self-reported ER difficulties, despite the likelihood that co-parents, siblings, and peers also play important roles in youth depression onset and trajectories (Lunkenheimer, Shields, & Cortina, 2007; Morris et al., 2007; Sheeber, Hops, & Davis, 2001; Yap, Allen, & Sheeber, 2007). In addition, youth ADHD symptoms were assessed using parent-report, although a multi-informant, comprehensive assessment approach (i.e., including teacher reports and diagnostic interviews assessing impairment in addition to symptoms) is considered the gold standard (Pelham, Fabiano, & Massetti, 2005). Similarly, the study did not incorporate multiple converging measures of maternal ER, such as child- or partner-reported maternal ER difficulties, ER tasks, and/or physiology. Therefore, we cannot preclude the possibility that social desirability may have impacted mothers’ reported ER. However, assessments of youth depressive symptoms were conducted at multiple time points, thereby mitigating the likelihood of within-informant biases attributable to variations in maternal mood or other variables. The study also did not include measures of pubertal status or biological development; therefore, we cannot ascertain relations between developmental stage and the variables of interest. Finally, the present findings suggest that even among youth with minimal ADHD symptomatology, maternal ER difficulties confer risk for depressive symptoms, but these findings are not necessarily generalizable to clinical populations, as we do not have data on the diagnostic status of participants.
Conclusion
Adolescents with ADHD symptoms are at risk for elevated depressive symptomatology, yet little is known about the independent and interactive effects of adolescent and maternal characteristics in predicting course characteristics across adolescence. The current study employed latent growth curve modeling to examine the independent and interactive effects of ADHD symptoms and maternal ER difficulties on the trajectory of depressive symptoms across adolescence, consistent with a developmental-transactional model of ADHD. The findings are strengthened by the longitudinal analytic approach to examining the unfolding of depressive symptoms over a critical developmental period and simultaneously evaluating important risk and interaction processes and controlling for key covariates (i.e., youth ODD/CD symptoms). Overall, these results support the interplay of maternal ER difficulties and youth ADHD symptoms on the course of depressive symptoms across adolescence. Future work should further attempt to characterize the nature and development of parental and youth characteristics as they relate to the unfolding of depressive symptomatology over time in the context of youth ADHD symptomatology. Identification of moderators can elucidate depression prevention and intervention targets among youth with ADHD symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a grant from the National Institutes of Health (NIH) 2R01 DA18647 awarded to Carl W. Lejuez.