
Abstract
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder affecting approximately 5% to 7% of youths (Polanczyk et al., 2014). The condition is characterized by pervasive symptoms of inattention and/or hyperactivity and impulsivity that are associated with substantial functional impairment. Deficits in social functioning, such as peer relationship difficulties, are especially pronounced in ADHD (Hoza, 2007; Ros & Graziano, 2018) and are predictive of global impairment (Mrug et al., 2012). Although there is recent consensus that ADHD persists into adolescence for a majority of children (Willcutt, 2012), due to historical conceptualizations of ADHD being a disorder of childhood only, interventions to improve social functioning have generally focused on children to the exclusion of adolescents (Storebø et al., 2011, 2019).
Peer Relationships in Adolescence
Adolescence is a period characterized by physical changes (e.g., neurobiological and pubertal), psychological changes (e.g., identity formation and a desire to individuate from parents), and social changes (e.g., the transition to high school, the opportunity to drive, access to alcohol and other drugs, the development of romantic relationships, and gaining employment; Wehmeier et al., 2010). The psychosocial factors unique to adolescence make social impairment a particularly pernicious risk factor for adverse outcomes as peer relationships are the primary setting for skill development in conflict resolution, negotiation, and cooperation, which are essential for competent social functioning across the lifespan (Bukowski et al., 2018). Although social functioning relates to all interpersonal relationships, the focus of this review is on the domain of peer relationships.
Definition of Social Functioning, Competence, and Impairment in Adolescents With ADHD
Social functioning encompasses the continuum from social impairment through to competence. Social competence describes the ability to achieve social goals and meet social demands in a given context through adaptive behavior (Iarocci et al., 2007), and may be indexed by social behavior, social cognition, and social outcomes (Nixon, 2001). Conversely, social impairment denotes deficits in these areas, to a degree that is problematic.
Social behavior includes day-to-day observed skills and can be compromised by deficits in acquisition (absence of knowledge), performance (failure to enact competent behavior in the moment), or fluency (awkward or unpolished enacting of social behaviors, Gresham et al., 2001). The social behaviors most strongly associated with social impairment in adolescent ADHD include the tendency to interrupt, not follow directions, forgetfulness in daily activities (Zoromski et al., 2015), and behavioral dyscontrol, such as aggression or rule-breaking, in the context of strong emotions (Bunford et al., 2018).
At a basic level, social cognition includes abilities such as theory of mind and emotion recognition in which youth with ADHD (age range 8–15 years old) have demonstrated impairments of small to medium effect sizes (Bora & Pantelis, 2016). Adolescents with ADHD exhibit similar social-cognitive deficits apparent in childhood ADHD including difficulties with social comprehension and social problem-solving (Sibley et al., 2010). Furthermore, adolescents with ADHD demonstrate less sensitivity to contextual cues to understand and interpret the emotional responses of others (Bunford et al., 2018; Da Fonseca et al., 2008).
Finally, social functioning can be measured by its outcomes. At the level of peer relationships, two related but distinct outcomes of peer-group acceptance/rejection, and reciprocated friendships can be measured as indicators of impairment in ADHD (Mikami, 2010; Mrug et al., 2012). Similar to well established findings in childhood (Hoza et al., 2005), adolescents with ADHD report fewer close friendships and experience greater peer rejection than their nonADHD peers (Bagwell et al., 2001). ADHD is also associated with peer victimization in adolescent girls (Sciberras et al., 2012).
Etiology of Social Impairment in ADHD
Factors contributing to the prevalence of social impairment in ADHD include the influences of core symptoms, emotional dysregulation, and comorbidities, but may vary across development. The core symptom of inattention is proposed to impede a young person’s opportunity to learn through social observation (Hoza, 2007), whereas impulsivity/hyperactivity may contribute to an overbearing and intrusive style, marked by difficulties with cooperating (Wehmeier et al., 2010). The influence of these core symptoms on impairment in peer relationships is different in adolescence than early or middle childhood. Whereas hyperactivity is implicated in social impairment in childhood, the core symptom of inattention appears to be the more important factor in adolescence (Zoromski et al., 2015). This may reflect the increased social demands of adolescence in which identifying, accurately interpreting, and responding appropriately to more subtle social cues are necessary for competent engagement. For example, although some behaviors are generally more prosocial than others (e.g., smiling), the social effectiveness of a behavior is dependent on how well it is matched to its social context (e.g., in conflict, smiling may be perceived as antagonistic, Dirks et al., 2007). As such, the core symptom of inattention inherent in ADHD can be an impediment to developing social competence.
Compared with community samples, adolescents with ADHD are characterized by emotion dysregulation which involves primary deficits in behavioral inhibition and self-regulation of emotions (Bunford et al., 2018). Although normal adolescent development is marked by more frequent and intense emotional experiences (Larson et al., 1980), it is coupled with increased environmental demands for both affective and behavioral control (Steinberg, 2005). Unsurprisingly, the emotion dysregulation common in ADHD becomes more prominent in adolescence and is associated with social impairment in this age group (Bunford et al., 2018).
Another reason why youth with ADHD may be at risk for difficulties in social functioning are the high rates of comorbidities, such as oppositional defiant disorder (Barkley, 2014; Gillberg et al., 2004). The presence of co-occurring disorders are predictive of worse social skills (Booster et al., 2012), and also contribute to the heterogeneity of social functioning difficulties experienced.
Implications of Social Impairment in ADHD
Remediation of social impairment is particularly important in adolescent ADHD for several reasons. Beyond the risks for adverse outcomes conferred by ADHD alone, social impairment places youth with ADHD at increased risk of developing depression (Eadeh et al., 2017; Feldman et al., 2017), conduct disorder, substance-use disorder (Greene et al., 1997), and eating pathology (Mikami & Hinshaw, 2006), whereas social acceptance may be protective in academic functioning (Dvorsky et al., 2018; Mikami, Ruzek, et al., 2017). A compounding challenge to treating adolescents in particular is that many desist or refuse standard treatments of stimulant medication (Sibley et al., 2014), despite evidence for their continued efficacy on core symptomatology (Chan et al., 2016). Improving social functioning through nonpharmacological interventions may be more acceptable to adolescents, and is in keeping with recommendations to focus on improved functioning over symptom reduction (Pelham et al., 2005).
Interventions to Improve Social Functioning in Youth With ADHD
Traditionally, social skills training (SST) has been the central approach to improving social functioning in ADHD (Mikami et al., 2014). The SST is traditionally delivered by a clinician directly to youths, often in group format, for 60 to 90 min for a prescribed period (e.g., 8–12 weeks). The content typically provides knowledge about and then in-session practice of skills that are thought to be lacking, for example, taking turns, following rules, identifying emotions, and emotion regulation. The SST interventions may vary in their approach, with some emphasizing training of social skills, others on improving social cognition, and still others emphasizing behavioral management by modifying contingencies of rewards or punishment to increase target behaviors. SST can also be delivered through multicomponent behavioral interventions in which social functioning is targeted alongside other domains such as organizational or academic skills. A criticism to the effectiveness of SSTs has been limitations in the generalization of skills to “real-world” situations, and has thus been identified as an important focus for the design of effective interventions (Aduen et al., 2018; Gresham, 1998; Mikami et al., 2014). Although SST has continued to be the primary paradigm for improving social functioning, other approaches have included parent-directed training, more general cognitive-behavioral approaches and classroom-level interventions to improve peer inclusion (Battagliese et al., 2015; Gardner et al., 2019; Mikami et al., 2013).
The majority of research has focused on social functioning interventions for children with ADHD, to the exclusion of adolescent populations. The most comprehensive review to date aimed to identify randomized controlled trials (RCTs) including both children and adolescents, but found no RCTs for adolescents in its original review (Storebø et al., 2011). Recently updated (Storebø et al., 2019), subgroup analyses included one RCT for adolescents (defined as 12–18 years) which utilized a more general cognitive-behavioral curriculum of problem-solving and organizational skills, rather than an explicit focus on SST (Schramm et al., 2016). The review concluded that there was not enough quality evidence to support or refute the efficacy of social skills interventions for children and adolescents with ADHD (Storebø et al., 2019). Although Storebø et al. (2019) is extremely comprehensive, the distinctiveness of adolescence from childhood, as argued in this introduction, provides a rationale for an exclusive focus on this developmental period.
Two other recent reviews explored peer relationships in youth with ADHD and proposed improvements for interventions; however, neither review applied a systematic search or provided a meta-analytic summary of efficacy (Gardner & Gerdes, 2015; Mikami, Smit, & Khalis, 2017). Another recent review focused on stand-alone SST for children and adolescents, but only found one intervention for youth aged >12 years (Willis et al., 2019). Other reviews have evaluated psychosocial interventions to improve overall functioning in adolescents with ADHD, and therefore, conflated outcomes of peer social functioning with other domains of functioning, such as academic performance (Evans, Owens, & Bunford, 2014; Evans et al., 2018) or parent–child conflict (Chan et al., 2016). Evidence for improvements in social functioning specifically cannot be determined from these reviews. As such, this article seeks to clarify the efficacy of interventions that target peer social functioning in adolescents with ADHD.
Method
Preregistration of the systematic review and meta-analytic protocol was submitted to PROSPERO (registration number: CRD42018100874).
Inclusion Criteria
Articles included in this review were trials of interventions to improve social functioning in adolescents with ADHD, according to the following guidelines.
Types of studies
Given the limited research among this age group (Storebø et al., 2011, 2019), the designs of studies eligible for inclusion included randomized, pre–post, multiple base-line, or wait-list control designs. Single case studies were excluded.
Types of participants
This review focused on adolescents with ADHD. We used a broad age range of 10- to 18-year-old youths to capture young people moving into adolescence at a lower age. If a study incorporated ages outside this range (e.g., from eight to 13), the results needed to be reported separately via age bands, so that only the relevant adolescent participants between 10 and 18 could be included for analysis.
Participants were required to have a formal diagnosis of ADHD or hyperkinetic disorder according to criteria described in the major nosological systems (Diagnostic and Statistical Manual of Mental Disorders [DSM] and/or International Statistical Classification of Diseases and Related Health Problems [ICD]). This may have been ascertained through parent- or clinician-report of a retrospective diagnosis or through assessment by a clinician at entry to the study. All subtypes of ADHD were included.
Studies were not excluded based on participants’ medication status, or disorders comorbid with their ADHD, though this was noted. Studies that focused on another mental health disorder in which some participants had comorbid ADHD were only included if outcomes were reported for the subset diagnosed with ADHD.
Types of interventions
Any nonpharmacological intervention which targeted peer social functioning was eligible for inclusion. That is, interventions that sought to improve or remediate, for example, adolescents’ friendships, social status among peers, and social skills relevant for peer interactions. Interventions that targeted other areas of functioning, such as academic achievement, alongside a focus on social functioning were also eligible for inclusion. Young people with ADHD needed to be the recipients of the intervention, and studies that incorporated a parent-directed component alongside the youth-directed component were not excluded. No exclusion criteria pertained to the delivery of intervention, so included interventions could use a variety of modes such as individual therapy, computer-based learning, or group work. When clarification was needed on two occasions, authors were contacted.
Types of outcome measures
Included studies were required to report outcomes related to peer social functioning. Where social outcomes were not specifically reported but were subsumed under a broad measure of “overall impairment,” they were not included given lack of specificity to the target outcome.
Search Strategy
Using EBSCOhost, the following databases were searched from inception until April 18, 2018: Embase via Embase, PsycINFO via EBSCO, CINAHL Complete via EBSCO, ERIC via EBSCO, and MEDLINE Complete via EBSCO. The searches were limited to peer-reviewed articles (to ensure methodological rigor and quality), in English language. Search terms were determined through checking relevant literature for relevant text word terms, and Medical Subject Headings (MeSH) were used (see Table 1).
Search Terms.
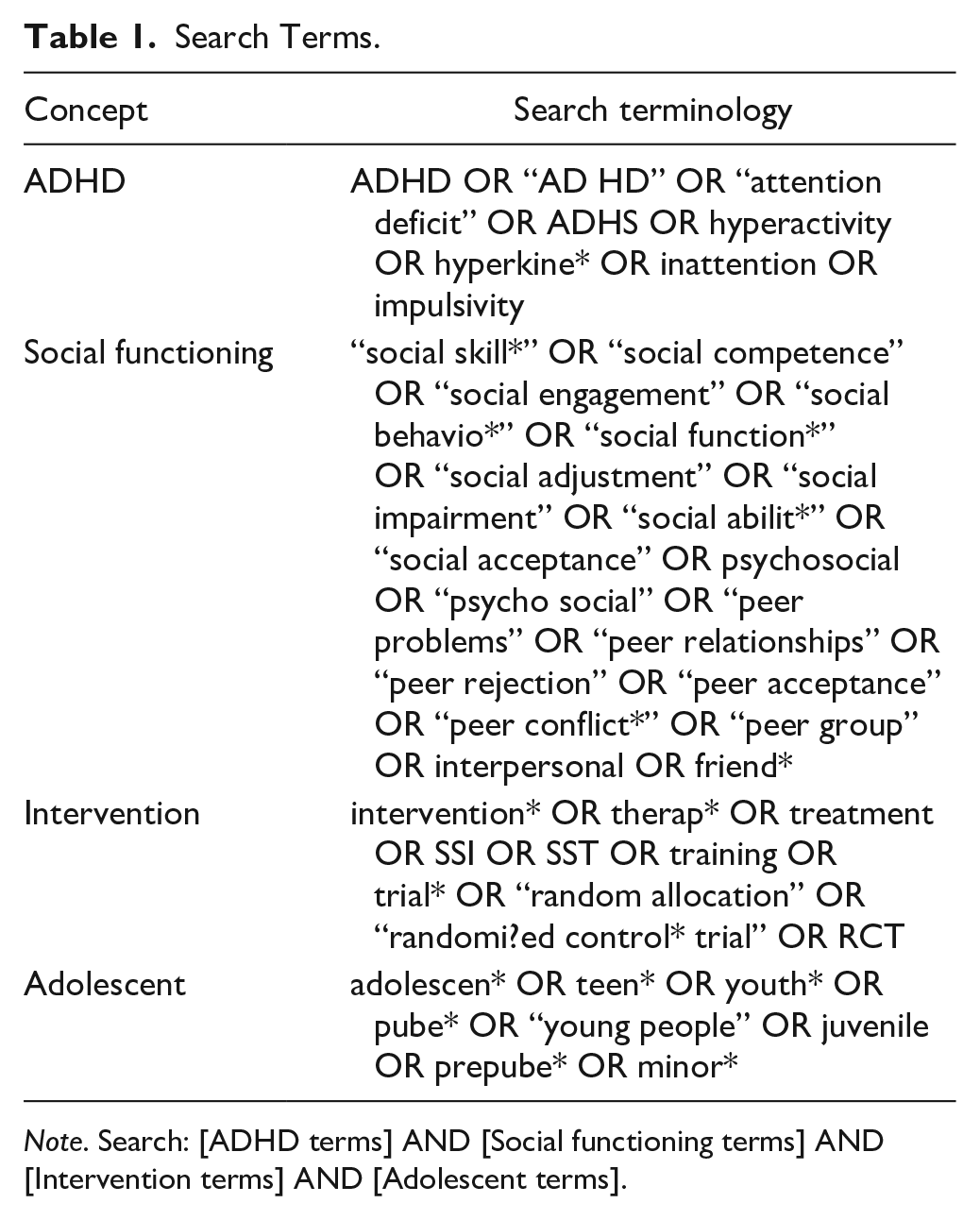
Note. Search: [ADHD terms] AND [Social functioning terms] AND [Intervention terms] AND [Adolescent terms].
Selection of Studies
After removal of duplicates, two review authors (SM, DF) independently screened the titles and abstracts of all identified studies using Rayyan software (Ouzzani et al., 2016) which enables systematic inclusion and exclusion of articles. Discrepancies were discussed in person until consensus was reached. Full-text review was conducted by SM, with consultation of ES.
Supplementary sources
The reference lists of all included studies were hand-searched for nonduplicate articles that may meet inclusion criteria. In addition, an author search on Steven W Evans was conducted via Scopus to identify other articles for inclusion, given that our search results indicated that this author had published many articles on interventions for adolescents with ADHD that incorporated a focus on social functioning.
Duplicate data
Where multiple papers reported outcomes for the same data set, these were reported together.
Data Extraction
Having identified all eligible articles, the designs of each study were identified and categorized as randomized and nonrandomized studies. Data relating to participant characteristics and comparison group, the intervention, and outcomes were extracted for each article by SM and independently checked by DF, see Tables 2 and 3.
Randomized Trials to Evaluate Improvements in Social Functioning in Adolescents With ADHD.
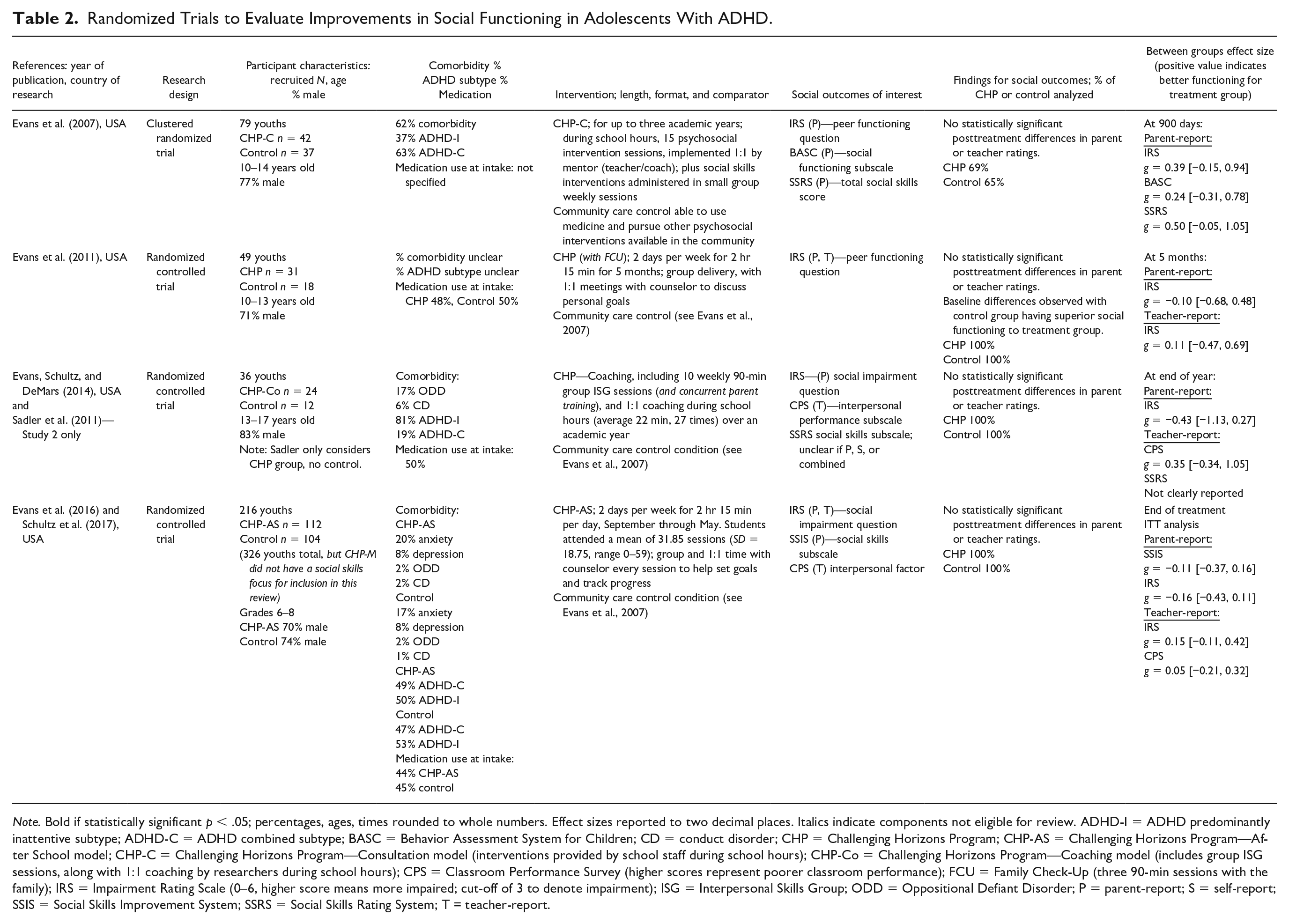
Note. Bold if statistically significant p < .05; percentages, ages, times rounded to whole numbers. Effect sizes reported to two decimal places. Italics indicate components not eligible for review. ADHD-I = ADHD predominantly inattentive subtype; ADHD-C = ADHD combined subtype; BASC = Behavior Assessment System for Children; CD = conduct disorder; CHP = Challenging Horizons Program; CHP-AS = Challenging Horizons Program—After School model; CHP-C = Challenging Horizons Program—Consultation model (interventions provided by school staff during school hours); CHP-Co = Challenging Horizons Program—Coaching model (includes group ISG sessions, along with 1:1 coaching by researchers during school hours); CPS = Classroom Performance Survey (higher scores represent poorer classroom performance); FCU = Family Check-Up (three 90-min sessions with the family); IRS = Impairment Rating Scale (0–6, higher score means more impaired; cut-off of 3 to denote impairment); ISG = Interpersonal Skills Group; ODD = Oppositional Defiant Disorder; P = parent-report; S = self-report; SSIS = Social Skills Improvement System; SSRS = Social Skills Rating System; T = teacher-report.
Nonrandomized Trials to Evaluate Improvements in Social Functioning in Adolescents With ADHD.
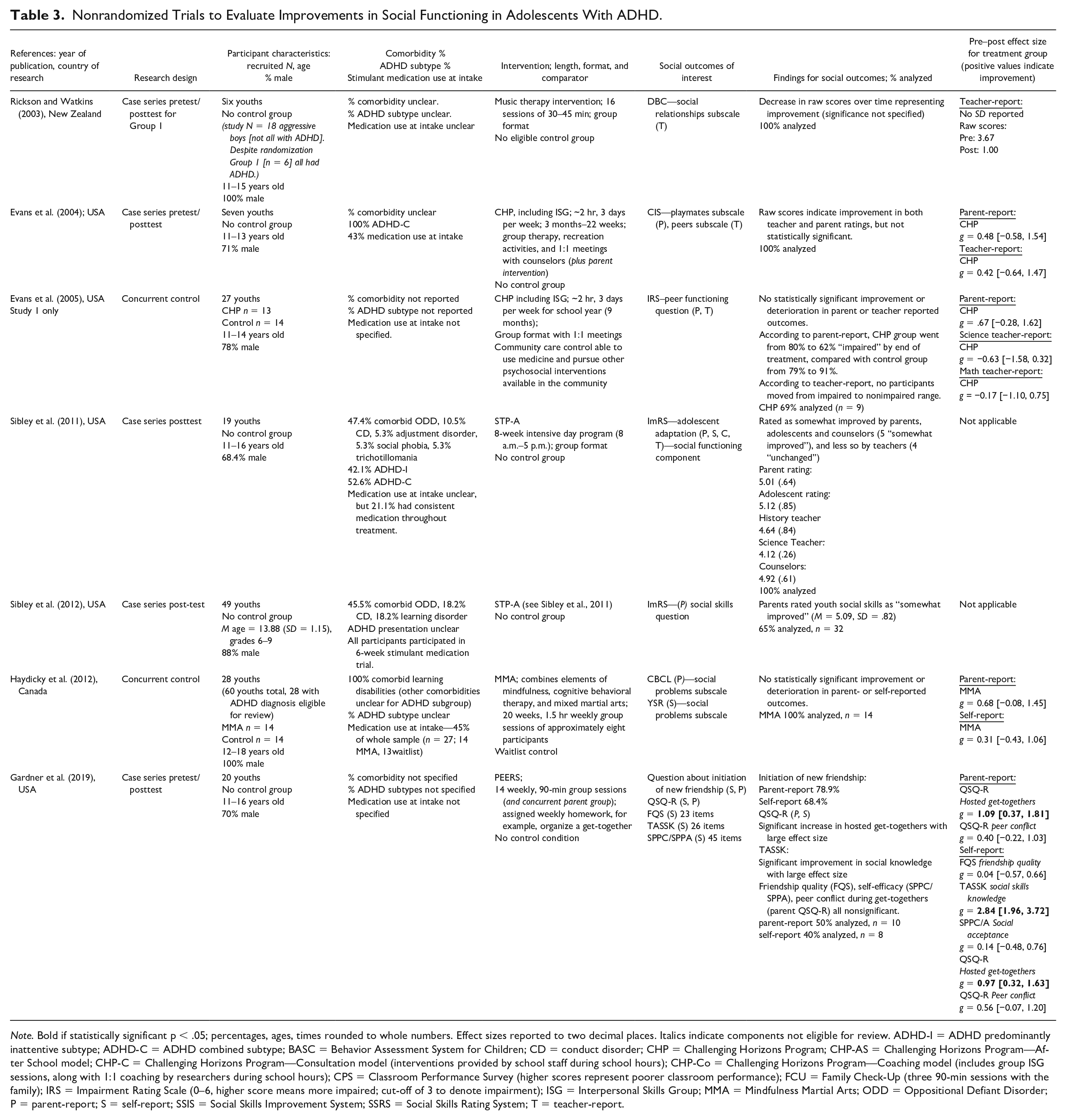
Note. Bold if statistically significant p < .05; percentages, ages, times rounded to whole numbers. Effect sizes reported to two decimal places. Italics indicate components not eligible for review. ADHD-I = ADHD predominantly inattentive subtype; ADHD-C = ADHD combined subtype; BASC = Behavior Assessment System for Children; CD = conduct disorder; CHP = Challenging Horizons Program; CHP-AS = Challenging Horizons Program—After School model; CHP-C = Challenging Horizons Program—Consultation model (interventions provided by school staff during school hours); CHP-Co = Challenging Horizons Program—Coaching model (includes group ISG sessions, along with 1:1 coaching by researchers during school hours); CPS = Classroom Performance Survey (higher scores represent poorer classroom performance); FCU = Family Check-Up (three 90-min sessions with the family); IRS = Impairment Rating Scale (0–6, higher score means more impaired; cut-off of 3 to denote impairment); ISG = Interpersonal Skills Group; MMA = Mindfulness Martial Arts; ODD = Oppositional Defiant Disorder; P = parent-report; S = self-report; SSIS = Social Skills Improvement System; SSRS = Social Skills Rating System; T = teacher-report.
Analysis
Assessment of risk of bias
Study quality was assessed by SM, with 10% independently assessed for rating agreement by DF using the Cochrane Risk of Bias Tool (Higgins et al., 2011, RoB2) for the randomized studies, and Risk Of Bias In Nonrandomized Studies—Interventions (Sterne et al., 2016, ROBINS-I) for the nonrandomized studies.
Effect sizes
Effect of treatment was investigated by considering baseline scores and scores at the end of treatment. Between-group effect sizes were calculated to quantify differences between treatment and control groups at postintervention in the randomized studies. Within-group effect sizes were calculated for pre to postintervention differences in the treatment groups of the nonrandomized studies.
Hedges g was used to calculate effect sizes where possible. It is similar to Cohen’s d, but is recommended when groups have small or unequal sample size, as it provides an unbiased estimate through weighting the pooled standard deviation (Ellis, 2010). The formulae are shown below (Lakens, 2013; Figure 1).
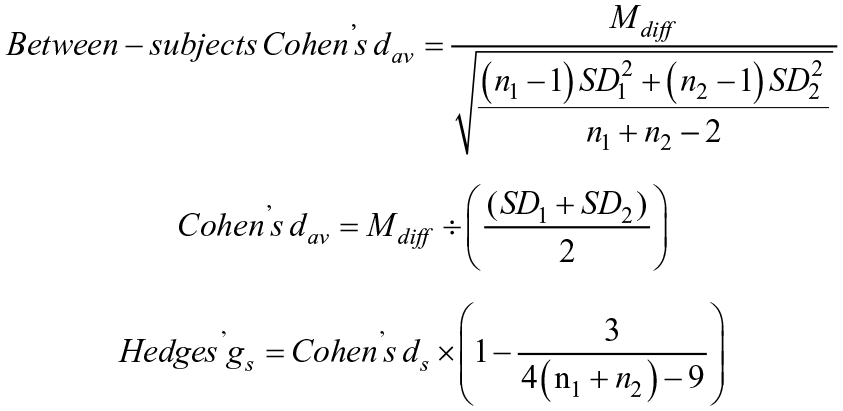
Formulae for calculating effect sizes (Lakens, 2013).
Meta-analysis
Where possible, studies were included in meta-analyses, however, not all studies included pre/ postratings, with some only including a single rating of perceived improvement (Sibley et al., 2011, 2012). As such, an effect size could not be calculated, and they could not be included in the meta-analyses. Meta-analyses were conducted using the metafor package (Viechtbauer, 2010) for R (R Core Team, 2019).
Outcomes were meta-analyzed according to the source of the outcome ratings: parent-, teacher- or self-report, in keeping with theoretical models that emphasize judge-specificity of social functioning ratings (Dirks et al., 2007). Where there was more than one outcome measure to choose from (e.g., five self-report measures in Gardner et al., 2019), we chose the outcome measure based on the following considerations: whether it was the focus outcome for a particular study, its conceptual similarity to other measures in the meta-analysis, and whether it was being used in other meta-analyses of different reporters (i.e., parent or teacher). The outcome measures used in the meta-analyses are listed in Table 4. A meta-analytic summary effect size of posttreatment scores was calculated for parent-reported (k = 4) and teacher-reported (k = 3) social functioning in the randomized studies, and parent-reported (k = 4), teacher-reported (k = 2) and self-reported (k = 2) social functioning in the nonrandomized studies.
Outcome Measures Used for Meta-Analyses.
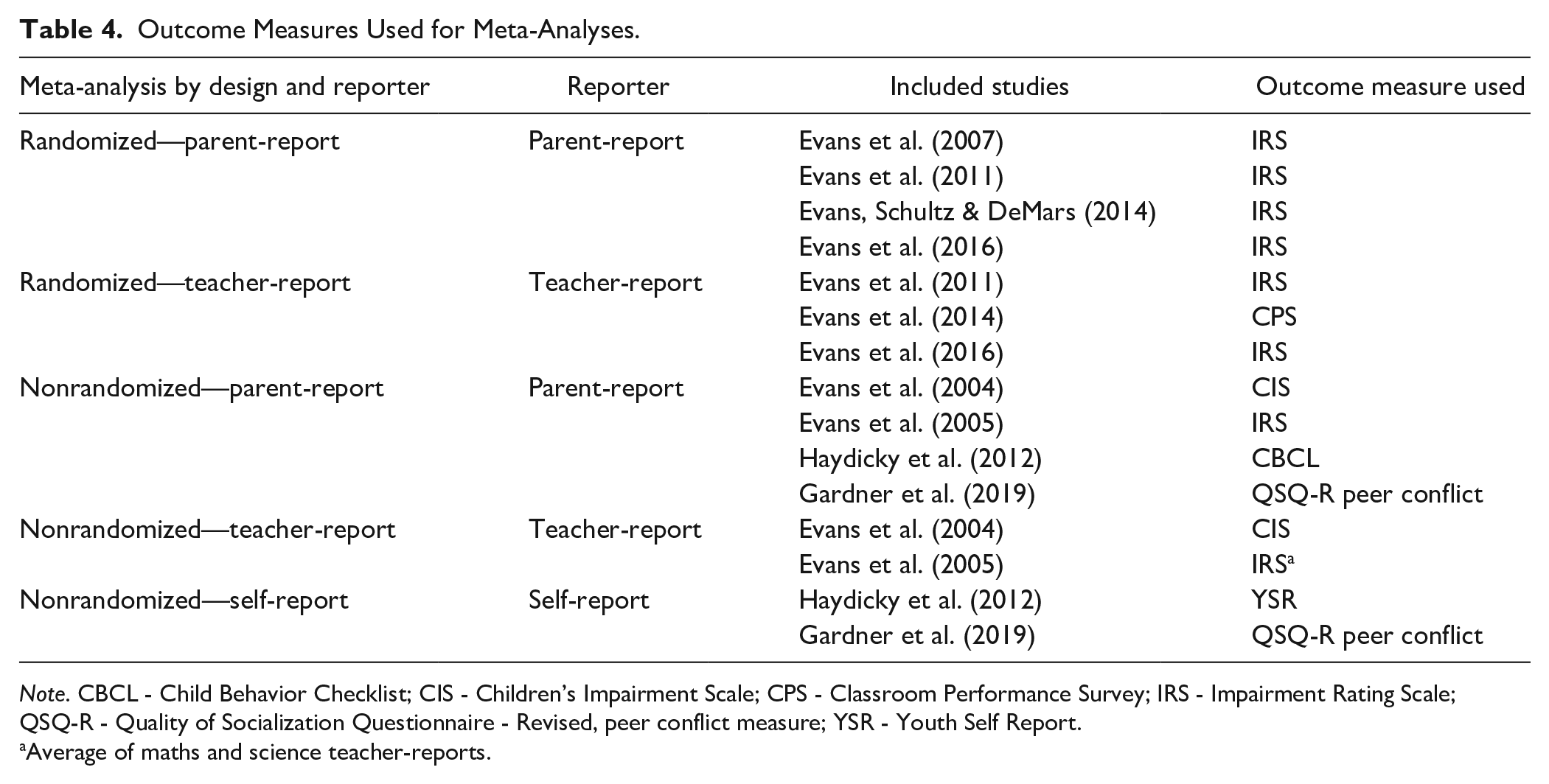
Note. CBCL - Child Behavior Checklist; CIS - Children’s Impairment Scale; CPS - Classroom Performance Survey; IRS - Impairment Rating Scale; QSQ-R - Quality of Socialization Questionnaire - Revised, peer conflict measure; YSR - Youth Self Report.
Average of maths and science teacher-reports.
Results
A summary of the search and screening process is represented in Figure 2. The electronic search yielded 2,683 results, of which 1,599 were nonduplicates. After title and abstract screening, the full text of 69 articles were reviewed resulting in nine trials from 11 reports meeting inclusion criteria. The references of these articles, along with a key author search identified 16 more articles of which two met inclusion criteria. This resulted in 11 trials from 13 records included for review.
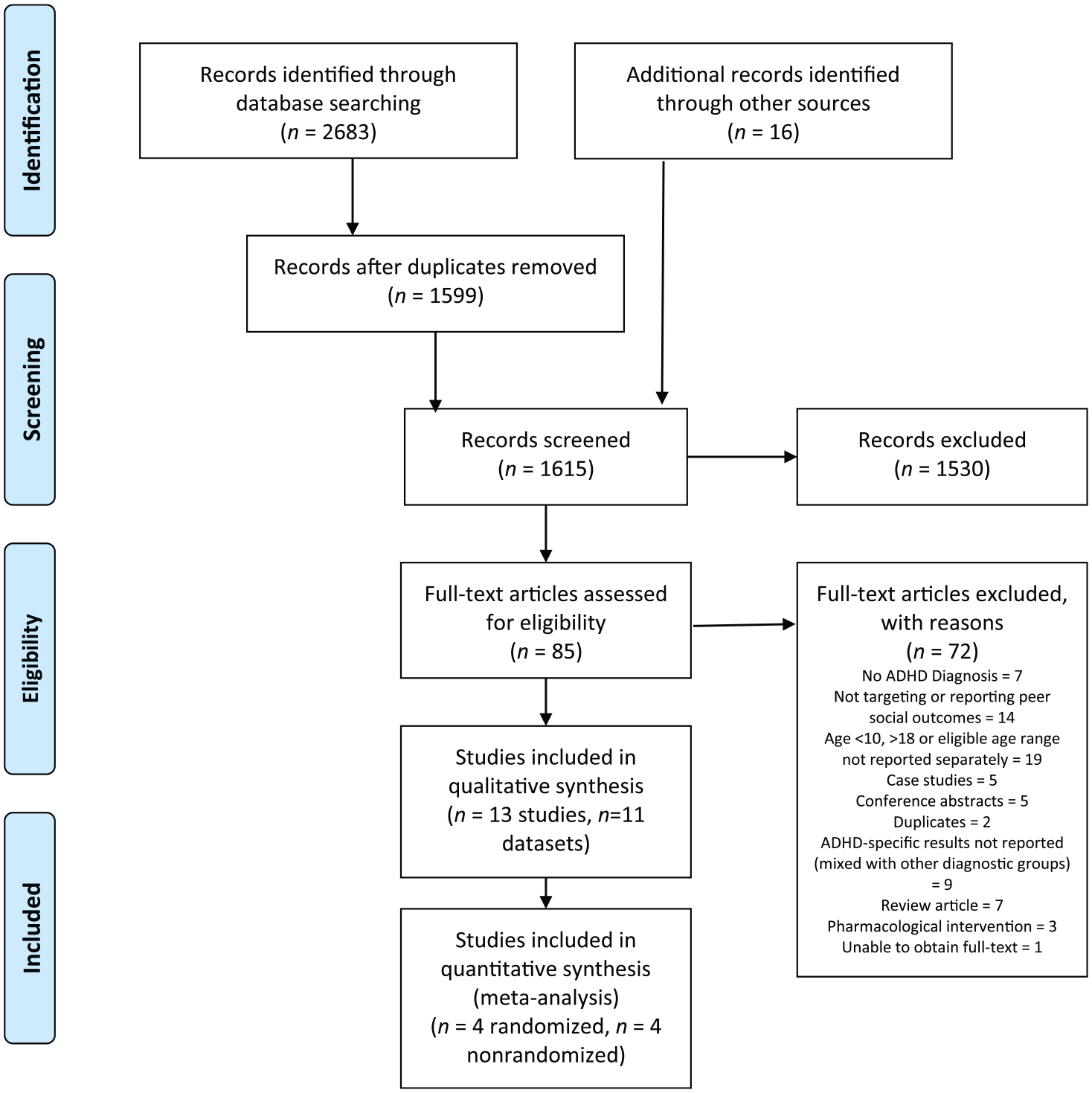
PRISMA flow diagram.
Included Studies
Altogether, four studies presented in six papers were identified as RCTs (see Table 2). Notably, all four studies investigated variations of the same intervention: the Challenging Horizons Program (CHP), which was adapted from the Summer Treatment Program for Children (Pelham et al., 2010). It targets social functioning along with other domains such as academic and organizational functioning., The studies were conducted in Virginia (Evans, Schultz, & DeMars, 2014; Evans et al., 2007, 2011) and the mid-west (Evans et al., 2016) of the United States. ADHD diagnostic status was assessed at entry to study according to semi-structured clinical interview, with social functioning ascertained by parent- or teacher-report on validated rating scales. Sample sizes ranged from 36 to 216 adolescents with ADHD, and the duration and format of the social intervention component was modified over time (see “Intervention” column in Table 2 ).
A further seven nonrandomized studies were identified (see Table 3), of which two also investigated variations of CHP (Evans et al., 2004, 2005). The other five studies investigated music therapy (Rickson & Watkins, 2003), an intensive holiday treatment program (Sibley et al., 2011, 2012, based on the model by Pelham et al., 2010), a mindfulness martial arts program (Haydicky et al., 2012), and a friendship-building intervention (Gardner et al., 2019). ADHD diagnostic status was determined through clinical interview and rating scales at study entry for three of the studies (Evans et al., 2004, 2005; Sibley et al. 2011). The procedure for determining ADHD diagnosis was unclear in one study (Sibley et al., 2012), and for the remaining three studies was via parent-report of a previous diagnosis of ADHD (Gardner et al., 2019; Haydicky et al., 2012; Rickson & Watkins, 2003). Sample sizes ranged from six to 49 adolescents with ADHD.
Participant characteristics
Most studies (64%) used a combination of rating scales, interview, and clinical consensus to ascertain whether participants met criteria for ADHD. Comorbidity, ADHD subtype, and medication status was unclear or unreported in 55% of studies. Although social impairment was a possible reason for participant inclusion, it was a specific and necessary criterion in only one study (Gardner et al., 2019), with the CHP studies typically requiring academic and/or social impairment as defined by a rating of >3 on the Impairment Rating Scale (IRS).
Intervention characteristics
The CHP was investigated in six of the 11 trials. The CHP is a training program, adapted from the Summer Treatment Program (Pelham et al., 2010), to be delivered in the school setting. This intervention targets academic, organizational, and social functioning, and various delivery methods were trialed—such as an after-school group format conducted by the research team, or delivered by school staff during school hours. Evaluations of CHP often incorporated a parent-directed component. An Interpersonal Skills Group (ISG) was typically incorporated into the CHP interventions, and was the primary method of delivering a social skills intervention which focused on improving social cognition (Sadler et al., 2011). Appropriate social behavior was then typically modeled, prompted, and reinforced during the recreational time of the CHP, or during the school day, and may also have been addressed during 1:1 meetings between adolescent participants and a facilitator, with the social intervention component of the CHP being modified in duration and format across different trials (see Tables 2 and 3 for details).
NonCHP interventions included an adolescent adaptation of a summer camp program, music therapy, mindfulness and martial arts, and a friendship building program (see Table 5). Of the various interventions, only one had a singular focus on the social domain, with others also targeting vocational or organizational domains, for example. The curriculum specifically targeting social functioning varied across interventions in its emphasis, from explicit teaching and practicing of social skills (such as group entry/exit skills, Gardner et al., 2019), using feedback and contingencies (i.e., rewards) to reinforce appropriate social behavior (Sibley et al., 2011), through to an emphasis on improving social cognition skills such as perspective-taking (Haydicky et al., 2012; Rickson & Watkins, 2003). All interventions utilized a group-based format as the primary means of training social skills.
Summarized Content of Interventions Targeting Social Functioning.

CHP and other interventions’ sessions varied in length from minutes, through to a whole day, on a daily through to weekly basis, and took place over several weeks to a few years (see Tables 2 and 3). The school setting was the environment in which CHP interventions were delivered, and other interventions sought to mimic natural social environments through a summer camp format (Sibley et al., 2011, 2012), or promote youths’ opportunities for practicing in natural social settings (Gardner et al., 2019) with the rationale of promoting generalization of skills.
Comparator characteristics
The randomized studies of CHP interventions all utilized a community care control in which young people were able to access other psychosocial interventions available in the community, along with the use of medication. In the nonrandomized studies, only two of the seven trials included an eligible control group, which were a waitlist design (Haydicky et al., 2012) and community care (Evans et al., 2005).
Outcome characteristics
Outcomes relating to social functioning were typically measured by parents and teachers, with three studies also including a self-report measure (Gardner et al., 2019; Haydicky et al., 2012; Sibley et al., 2011). The IRS was used in most of the CHP studies, in which peer social functioning is assessed via a single question on a 7-point scale (Fabiano et al., 2006). The parent or teacher is asked to rate the level of impairment from 0, No problem/definitely does not need treatment or special services to 6, Extreme problem/definitely needs treatment or special services with regard to the following statement How this child’s problems affect his or her relationship with other children. Impairment is defined through a cut-off score of 3 or greater.
Risk of Bias
A summary of the risk of bias in each study is presented in Tables 6 and 7. The randomized trials were all evaluated as having a high risk of bias. The overall risk of bias in the nonrandomized trials were serious (i.e., has some important problems) or critical (i.e., the study is too problematic to provide any useful evidence). Although it is recommended in the ROBINS-I tool to exclude papers with a critical risk of bias from synthesis in meta-analyses, given the overall high risk of bias of the nonrandomized trials in this review, it was determined to include the four eligible trials, but consider risk of bias in the interpretation of the meta-analyses.
Risk of Bias for Randomized Trials (RoB2).
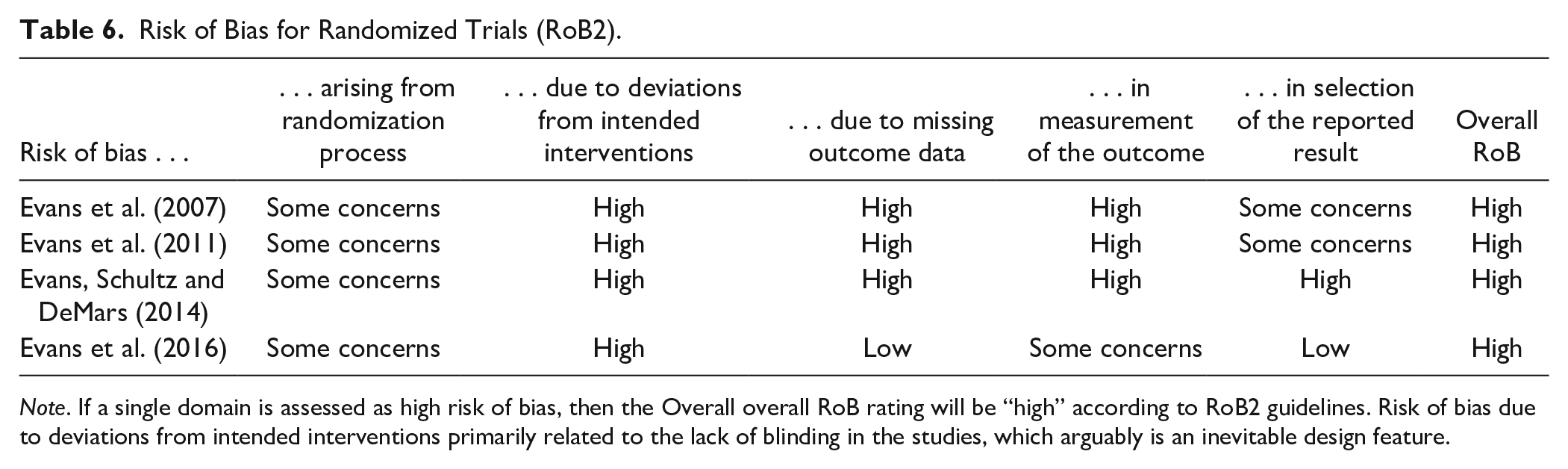
Note. If a single domain is assessed as high risk of bias, then the Overall overall RoB rating will be “high” according to RoB2 guidelines. Risk of bias due to deviations from intended interventions primarily related to the lack of blinding in the studies, which arguably is an inevitable design feature.
Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I).
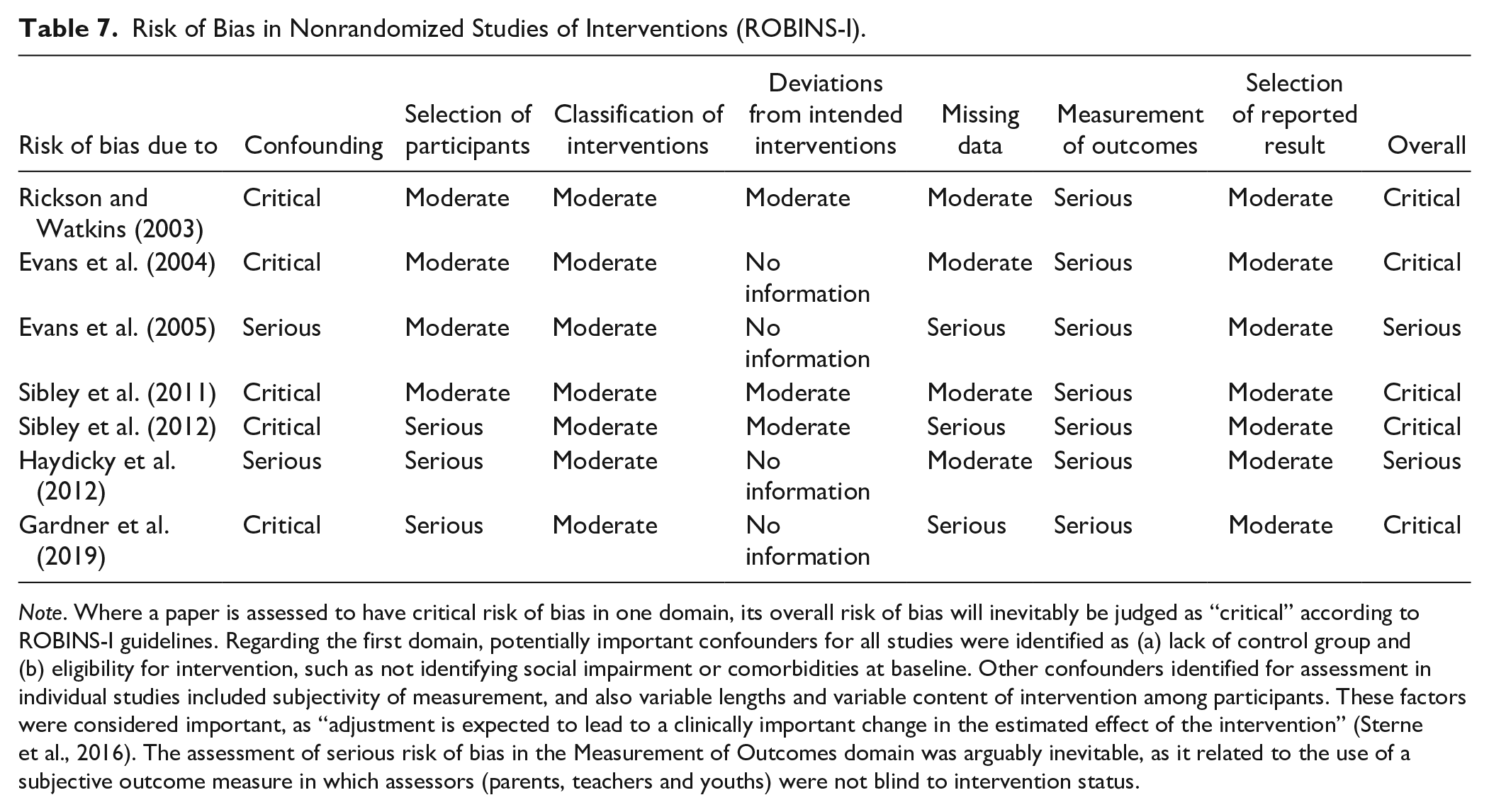
Note. Where a paper is assessed to have critical risk of bias in one domain, its overall risk of bias will inevitably be judged as “critical” according to ROBINS-I guidelines. Regarding the first domain, potentially important confounders for all studies were identified as (a) lack of control group and (b) eligibility for intervention, such as not identifying social impairment or comorbidities at baseline. Other confounders identified for assessment in individual studies included subjectivity of measurement, and also variable lengths and variable content of intervention among participants. These factors were considered important, as “adjustment is expected to lead to a clinically important change in the estimated effect of the intervention” (Sterne et al., 2016). The assessment of serious risk of bias in the Measurement of Outcomes domain was arguably inevitable, as it related to the use of a subjective outcome measure in which assessors (parents, teachers and youths) were not blind to intervention status.
Effects of Interventions—Randomized Studies
None of the randomized studies demonstrated statistically significant differences in social functioning between treatment and control groups by parent- or teacher-report at posttreatment (Table 2). Random effects meta-analyses of randomized studies were conducted and found no statistically significant posttreatment differences between treatment and control groups for either parent-reported (k = 4, N = 354) or teacher-reported (k = 3, N = 301) social functioning, though small to moderate effect sizes were found (see Figures 3 and 4). The tests for heterogeneity of parent- and teacher-reported outcomes were not significant, Q (df = 3) = 4.16, p = .24; Q (df = 2) = 0.32, p = .86, respectively, suggesting there is no variance in the true effect between studies. The I2 statistic indicates the proportion of variance attributable to heterogeneity was I2 = 20.85% for parent-report, and I2 = 0.00% for teacher-report.
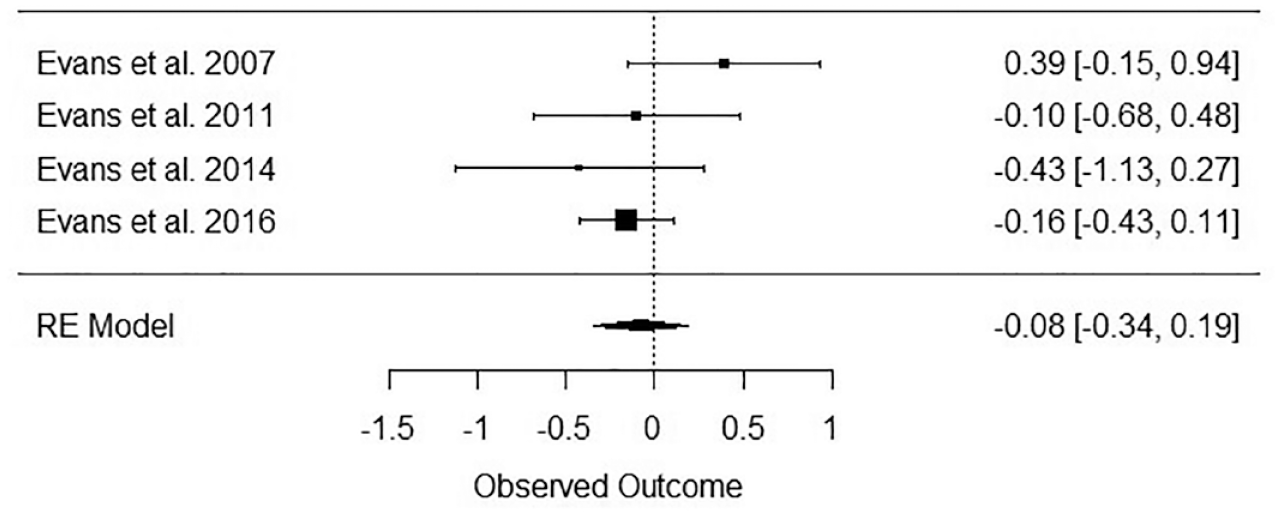
Meta-analysis of effect sizes of randomized studies—Parent-report (N = 354).
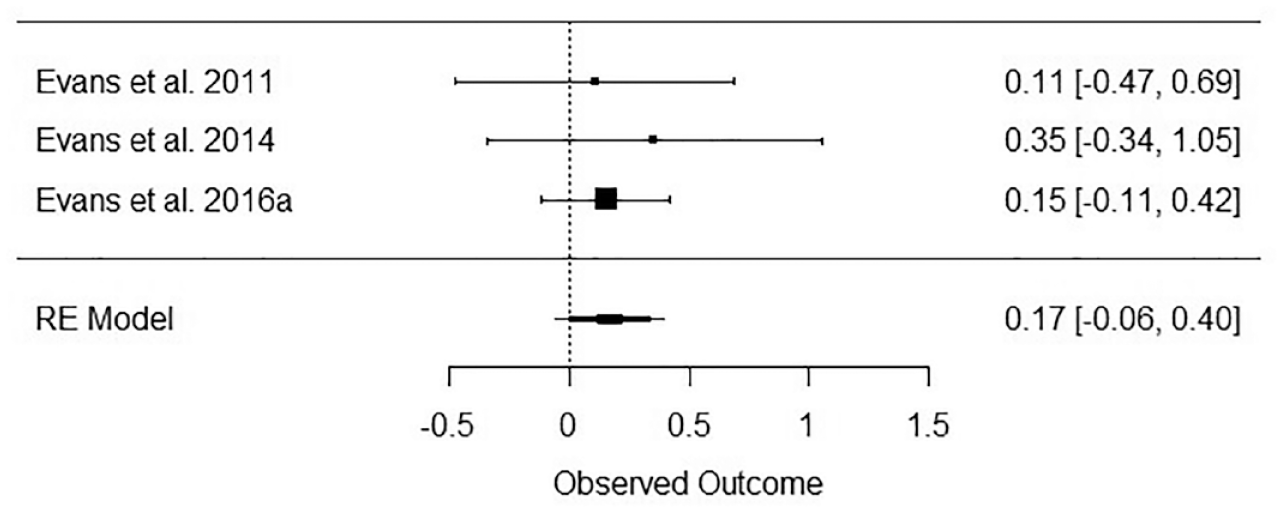
Meta-analysis of effect sizes of randomized studies—Teacher-report (N = 301).
Effects of interventions—Nonrandomized studies
One study demonstrated statistically significant improvement in the number of hosted get-togethers, as well as social skills knowledge from pre–post measurement for the participants, according to parent- and self-report (Gardner et al., 2019, see bold text Table 3). Although small to moderate effect sizes were found in other papers, none were statistically significant. A random effects meta-analysis of pre–post improvement in social functioning according to parent-report supports efficacy of treatment for the participants of these studies, with a large effect size (k = 4, N = 40, Figure 5); however, pre–post improvements were not supported in the meta-analyses including teacher- (k = 2, N = 16, Figure 6), or self-report (k = 2, N = 22, Figure 7). The tests for heterogeneity of parent-, teacher-, and self-reported outcomes were not significant, Q (df = 3) = 0.31, p = .96; Q (df = 1) = 1.04, p = .31; Q (df = 1) = 0.13, p = .71, respectively, suggesting there is no variance in the true effect between studies. The I2 statistic indicates the proportion of variance attributable to heterogeneity was I2 = 0.00% for parent-report, I2 = 4.1% for teacher-report, and I2 = 0.00% for self-report.
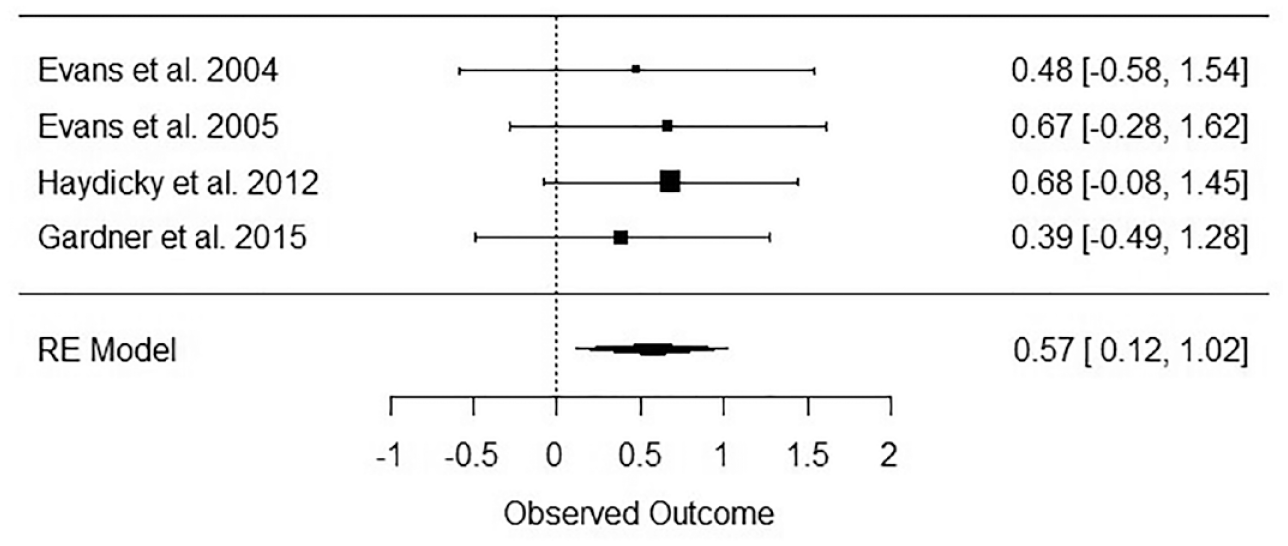
Meta-analysis of effect sizes of nonrandomized studies—Parent-report (N = 40).
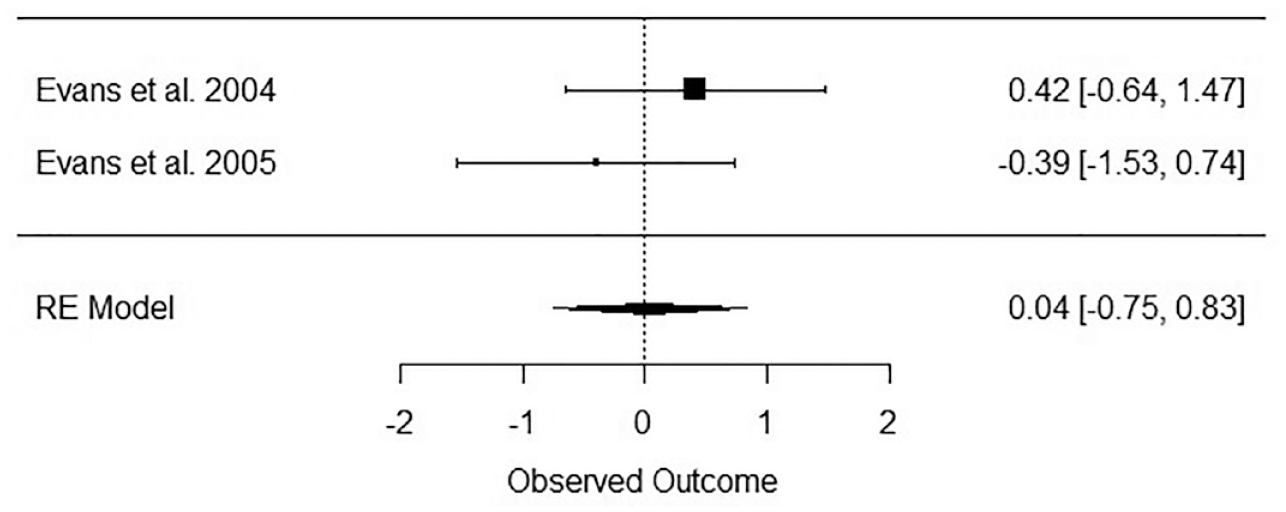
Meta-analysis of effect sizes of nonrandomized studies—Teacher-report (N = 16).
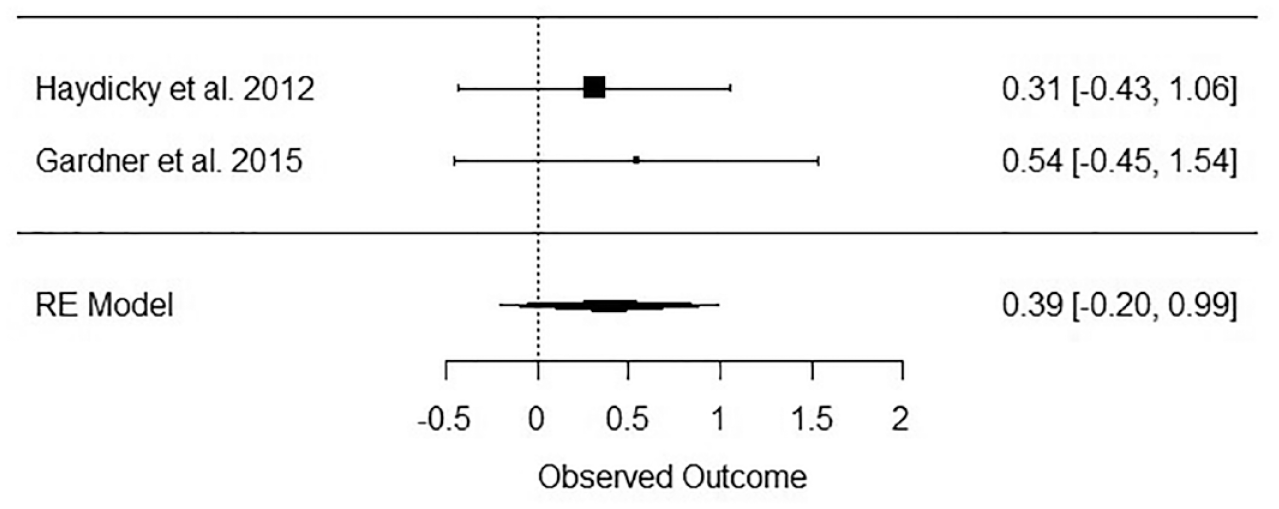
Meta-analysis of effect sizes of nonrandomized studies—Self-report (N = 22).
Discussion
There is a paucity of quality research in youth-directed, nonpharmacological interventions to improve peer social functioning in adolescents with ADHD. Only four randomized trials have been conducted, which all assessed variations of the same intervention (CHP), and a meta-analytic summary does not support efficacy of this treatment in improving parent- or teacher-reported social functioning in adolescents with ADHD. Although a meta-analysis of nonrandomized trials identified that the participants significantly improved in social functioning from their baseline to posttreatment scores with a medium effect size according to parent-report, there was no improvement according to teacher- or self-report. Furthermore, these studies had a much smaller sample size than the randomized studies, had serious/critical risk of bias as they were not compared with a control group, and therefore cannot be interpreted with confidence. As such, the weight of evidence does not support the efficacy of current nonpharmacological interventions to improve peer social functioning in adolescents with ADHD. Furthermore, the dearth of studies in this area highlights the need for more research among this age group.
Baseline Social Impairment
Although social impairment is well documented in adolescents with ADHD (Bagwell et al., 2001; Wehmeier et al., 2010), not all individuals with ADHD display such impairments (DuPaul et al., 2018). The majority of reviewed studies’ inclusion criteria did not necessitate social impairment for enrollment in the study. Investigating the effectiveness of interventions for adolescents without baseline social impairment is unlikely to yield significant results due to ceiling effects. This explanation was proposed by Schultz et al. (2017) to explain the lack of improvement in social functioning in their large RCT, that is, participants did not display mean levels of baseline social impairment (i.e., IRS ≥ 3). Social impairment was subsumed under the inclusion criteria of functional impairment for most CHP trials (64% of all papers included in this review) which meant that not every participant necessarily exhibited social impairments specifically.
Of the remaining four nonCHP papers included in this review, only one included the specific and necessary inclusion criterion of social impairment (Gardner et al., 2019). Notably, it was the only trial included in the review that displayed statistically significant improvement on some outcomes (social skills knowledge, and number of hosted get-togethers according to parent- and self-report).
Choosing Treatment Targets
Given the dearth of studies in this area and the lack of efficacy of current social functioning interventions for adolescents, a reexamination of curriculum and treatment targets is warranted. It is argued that adolescent interventions should not merely adapt child-focused interventions but reflect developmentally relevant features and address causal factors of poor social functioning in adolescent ADHD specifically. Hoza (2007) proposed that the social deficits exhibited in ADHD are performance-related, rather than knowledge-related. For example, youth with ADHD may be able to describe an appropriate response to a given social situation but struggle to enact such a response in the heat of the moment. Several factors may impede the effective remediation of performance deficits if they are missing from social functioning interventions for adolescents, including addressing emotion dysregulation, designing for generalization, and addressing inattention.
Emotional dysregulation appears to be especially impairing for peer relationships in adolescence (Bunford et al., 2018). Behavioral inhibition and self-regulation of emotions in the context of peer relationships should therefore feature in adolescent curriculum, both in experiential and didactic form. Of the interventions included in this review, many included in-session rewards, such as verbal praise, for prosocial behavior (Haydicky et al., 2012), appropriate game play in the Summer Treatment Program (Sibley et al., 2011), and practicing social skills during recreational time in the CHP interventions (e.g., Evans et al., 2011), which may all reflect experiential teaching of emotion regulation. As well as this, didactic teaching of emotion regulation skills may have been reflected in topics such as responding to peer teasing (Gardner et al., 2019), increasing self-control and adaptability (Haydicky et al., 2012), and understanding the link between our behavior and others’ responses (Sadler et al., 2011). However, emotion dysregulation as it relates to peer social functioning was not explicitly identified as a treatment target or outcome measure in any of the included papers, and it may be that the aforementioned examples were not central enough to the interventions to provide remediation of this core deficit. Overt inclusion of curriculum that addresses behavioral inhibition and self-regulation in the context of peer relationships may be important for efficacious intervention design for adolescent populations.
Another important design element to address performance deficits for adolescents is the inclusion of in vivo peer interaction opportunities to promote generalization (Mikami, Smit, & Khalis, 2017). A strength of many of the included papers in this review is the locating of interventions in real-life settings, such as school settings. However, these may not have adequately replicated the real-world social environment of adolescence. For example, the peer-groups within the intervention context all had ADHD, received overt and identical teaching about social norms, and were under a high level of supervision. Generalization of performance-related skills are unlikely to occur unless the context of interventions accurately mimic real-world demands.
Along with this, inattention likely exacerbates ADHD performance deficits, impeding an adolescent’s in the-moment attendance to social cues. Pharmacological treatment generally improves attention and social function in adolescents (Chan et al., 2016; Smith et al., 1998), so motivational interviewing to promote medication adherence may be an important adjunct to social functioning interventions (Chan et al., 2016). However, it is common for adolescents to desist pharmacological treatments (Sibley et al., 2014). Given this trend, exploring developmentally relevant ways to make interventions more inherently rewarding may help to address core symptoms of inattention (Morsink et al., 2017)
A further consideration to improve intervention efficacy is the malleability of the various targets for intervention. Mikami (2010) proposes addressing friendship difficulties, rather than the related but distinct construct of peer rejection. Mikami cites evidence that peer reputations are quickly formed, and relatively fixed, and are therefore more difficult to address than friendship difficulties. Of note, the only intervention with statistically significant results in the social domain was the one that focused on friendship specifically (Gardner et al., 2019). Even so, gains were not found in performance-related domains of friendship quality or reductions in peer conflict. Rather, improvements were identified in social knowledge, and increasing opportunities for friendship (hosting get-togethers). If this social knowledge reflected improvements in the identified deficits of social comprehension and social problem-solving characteristic of adolescent ADHD (Sibley et al., 2010), then this represents an important curriculum focus to replicate in future studies. However, if this social knowledge reflects a decontextualized and theoretical knowledge distinct from performance deficits, then it may be argued that the statistically significant outcomes of the study are inadequate proxies for improvement in the core social impairments of ADHD. This is also the case for the outcome of hosted get-togethers, as adolescents may not be the agents of change in organizing such events. This serves to highlight the unique challenges associated with measuring changes in social functioning for adolescent populations.
Measurement Challenges
Measurement challenges were a central problem in the reviewed studies. For example, one of the most intensive interventions reviewed, the Summer Treatment Program, could not be incorporated into the meta-analyses due to its utilization of a single “improvement” score, rather than baseline and postintervention measurements. Table 5 further identifies the ways in which social competencies that were targeted in the reviewed interventions were not always directly measured. For example, in CHP, social cognitive skills of anticipating others’ reactions and socially skilled behaviors were some of the targeted competencies. However, proximal indices of these competencies were not directly measured, and instead a more distal social outcome measure of impairment in peer relationships was used. This measurement may not have been able to capture smaller, more proximal improvements in participants’ behavior or cognition. Further to this, existing measures may not capture the adolescent’s social experience as effectively as they do for childhood. There are challenges associated with ratings provided by different judges that are unique to adolescence. Whereas teachers are reliable informants of social functioning in elementary aged children, their opportunity to observe adolescent students is reduced due to schooling structures. Self-report also presents challenges in that positive illusory bias (Murray-Close et al., 2010) may mean that participants do not accurately perceive their own social performance. Parents may not have the opportunity to observe peer interactions, and as with all parent-reported outcomes, they are typically not blind to condition, so their responses may be confounded by placebo effects. As such, there are limitations in the sensitivity of outcome measures which may have impeded the identification of intervention effectiveness in the reviewed studies.
Limitations
The risk of bias assessments were conducted using best practice tools of RoB2 and ROBINS-I. Nonetheless, such assessments may have shortcomings when applied to this field of psychology. For example, in utilizing parent-reported measurements, the study design does not allow for blinding to treatment status. In fact, this is a norm in psychology, yet inevitably requires the judgment of a high risk of bias under deviations from intended interventions. As such, ratings of risk of bias should be thoughtfully interpreted, in light of the inherent limitations of the field, rather than being taken as an indiscriminate judgment.
This review chose to include a broad range of studies rather than limiting inclusion to RCTs as other reviews have done (Storebø et al., 2019). We also elected to conduct meta-analyses on nonrandomized trials, which could lead to the erroneous conclusion that the statistically significant result identified in those is comparable with the results of meta-analyses of randomized studies. Nonetheless, we have endeavored to make plain the quality of evidence by categorizing studies according to randomization, and informing readers’ discriminate evaluations of the quality of studies through risk of bias assessments. This review has sought to provide an up-to-date account of the research, but it is a burgeoning field, and there will undoubtedly be many more trials published in the coming months and years.
Conclusion
Despite the prominence of peer social difficulties experienced by adolescents with ADHD and their deleterious consequences, there is a paucity of research in this area, and effective interventions remain elusive. The content of future interventions may be improved by taking into consideration the social profiles of adolescents with ADHD, the features most causally related to social impairment and the malleability of these treatment targets for intervention. Utilizing outcome measures that are sensitive to change may also aid research effectiveness. Given the well established importance of peer social functioning to the mental health and wellbeing of this vulnerable population, further research is essential.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sarah Morris is supported by an Australian Government Research Training Program Scholarship. Emma Sciberras’ position is funded by an NHMRC Career Development Fellowship (1110688: 2016-21) and a veski Inspiring Women’s Fellowship.