
Abstract
Objective:
Eveningness diurnal preference is common in psychiatric conditions, including attention-deficit/hyperactivity disorder (ADHD) and internalizing disorders. Little is known about how diurnal preference relates to sluggish cognitive tempo (SCT)—a distinct clinical construct associated with functional impairment—in clinical samples.
Method:
Adult outpatients (n = 65; 43 with ADHD, 22 with internalizing/adjustment disorders) self-reported on SCT symptoms (total symptoms; slow/daydreamy, sleepy/sluggish, and low initiation/persistence factors) and diurnal preference.
Results:
Greater eveningness was associated with overall SCT severity and sleepy/sluggish symptoms in the full sample. Relationships between eveningness and overall SCT severity and slow/daydreamy symptoms were stronger for those with internalizing/adjustment disorders compared to ADHD. The relationship between eveningness and sleepy/sluggish symptoms was uniform across groups.
Conclusion:
Findings suggest a potential role of eveningness preference in adult SCT presentation. Future studies should investigate underlying mechanisms linking these two constructs and the efficacy of circadian interventions in the treatment of SCT among adult outpatients.
Introduction
Sluggish cognitive tempo (SCT) is a constellation of symptoms characterized by daydreaming, mental fogginess, and slowed cognition and behavior (Becker & Barkley, 2018). Although SCT was originally conceptualized as a feature of attention deficit/hyperactivity disorder (ADHD)—particularly the inattentive subtype/presentation—SCT has been shown to be a key clinical construct that is distinct from both internalizing (e.g., mood disorders, anxiety) and externalizing disorders (e.g., ADHD) (Barkley, 2014; Becker, Marshall, & McBurnett, 2014). SCT is also associated with a range of detrimental functional outcomes, including greater stress (Combs et al., 2015), anxiety and depression (Becker et al., 2016), poorer quality of life (Combs et al., 2014), and impaired functioning across home, social, academic, and community domains (Becker et al., 2016; Lunsford-Avery et al., 2018). Although it is unclear whether SCT is best conceptualized as a categorical diagnosis or a dimensional transdiagnostic construct (Becker & Willcutt, 2019), our recent work has shown that SCT can be reliably assessed among adult outpatients using the SCT subscale of the Barkley Adult ADHD Rating Scale-IV (BAARS-IV (Barkley, 2011)) and encompasses three factors: slow/daydreamy, sleepy/sluggish, and low initiation/persistence (Lunsford-Avery et al., 2018).
Given its prevalence and functional impact in clinical samples (Barkley, 2012), it is critical for the field to clarify underlying factors associated with SCT and to develop targeted interventions for individuals who present with this specific pattern of symptoms. One potential contributor to SCT symptoms in clinical populations is sleep disturbance. There is notable overlap in SCT symptoms and correlates of disturbed sleep, including lethargy, slowed information processing, and difficulties with concentration and remaining alert (Becker, 2013; Cortese et al., 2009; Mayes et al., 2009; Willoughby et al., 2008). This correspondence in symptom presentation has generated interest in the potential role of poor sleep in SCT presentations (Becker et al., 2016), and indeed, several aspects of sleep, such as poorer sleep quality, greater sleep disturbances, and daytime sleepiness, have been shown to relate to SCT in adults after controlling for ADHD symptoms (Becker, Luebbe, & Langberg, 2014; Langberg et al., 2014). In the case of daytime sleepiness, it is notable that the sleepiness construct was found to be overlapping with but also statistically distinct from SCT in a college student sample (Langberg et al., 2014).
Less is known about the association of a particularly important component of the sleep/wake cycle with SCT: diurnal preference. Diurnal preference refers to an individual’s preference for the timing of waking activity and sleep, and ranges from extreme preference for morningness (i.e., “morning larks”) to extreme preference for eveningness (i.e., “night owls”). Diurnal preference is strongly related to, but is not synonymous with, an individual’s internal circadian rhythm (Kerkhof, 1985). Eveningness preference is common among adult outpatients who often exhibit SCT symptoms, including those with ADHD (Coogan & McGowan, 2017) and internalizing disorders such as depression (Bauducco et al., 2019).
Eveningness preference shares many clinical facets with SCT, particularly for individuals who have a “mismatch” between their preference for greater activity during the evening/nighttime and their obligation to perform tasks earlier in the day, for example during traditional work hours (Roenneberg et al., 2003). For these individuals, reduced alertness, daytime fatigue and sleepiness, low energy, and difficulties with concentration are frequently evident (Adan et al., 2012; Korman et al., 2019). Thus, there is a critical need for research examining a possible relationship between diurnal preference and SCT in adults. To our knowledge, only one prior population-based study has examined the potential relationship between SCT and diurnal preference. In two independent samples of Romanian adults (a college student sample (n = 301, mean age = 21.82) and a general population sample (n = 250, mean age = 38.61), greater tendency toward eveningness was associated with greater SCT symptoms as measured by the BAARS-IV (Voinescu et al., 2012). However, this topic has yet to be investigated in a clinical sample of adult outpatients.
The current study had two primary aims. The first was to investigate the relationship between diurnal preference and SCT, including overall severity and with the three SCT factors separately, among adult outpatients presenting to an ADHD clinic for evaluation. Based on prior findings in a population sample (Voinescu et al., 2012), we hypothesized that greater eveningness would be related to increased overall SCT symptoms in our full sample. In addition, given the overlap in symptom presentation as well as prior literature linking SCT and daytime sleepiness (Langberg et al., 2014), we hypothesized that SCT would show the greatest association with the sleepy/sluggish factor. Secondly, given the high rates of SCT and eveningness observed in both ADHD and internalizing disorders, we explored how potential relationships between diurnal preference and SCT may differ between adults who received an ADHD diagnosis versus those who received other diagnoses, most commonly internalizing disorders.
Methods
Participants and Procedure
Participants were 65 adults aged 19 to 69 years who were physician- or self-referred to an outpatient specialty clinic at Duke University Medical Center for an ADHD evaluation and provided informed consent to participate in the current study. Participants completed a comprehensive psychiatric evaluation administered or supervised by a licensed doctoral-level clinician, including: the Conners’ Adult ADHD Interview for the DSM (CAADID)—Parts I and II (Epstein et al., 2001); a computerized diagnostic screener for DSM-5 disorders (American Psychiatric Association, 2013); a semi-structured clinical interview; and as available, review of medical/school records and prior psychiatric or psychoeducational assessment reports. Participants also completed self-reported measures of diurnal preference, SCT, and ADHD symptom severity described below.
Measures
Psychiatric diagnoses
The CAADID was used to diagnose ADHD (Epstein et al., 2001). The CAADID Part I is a questionnaire querying information about early development, psychiatric history, and past and current family, academic, occupational, and personal functioning. In this study, participants completed Part I prior to their diagnostic evaluation and it was jointly reviewed with the clinician as part of the assessment. Part II is a clinician-administered semi-structured interview that evaluates the presence, persistence, severity, and age of onset for each of the 18 ADHD symptoms during two developmental periods (childhood and adulthood). ADHD diagnoses derived from the CAADID are associated with satisfactory concurrent validity and interrater reliability (Epstein & Kollins, 2006). Additional psychiatric disorders were assessed using a computerized diagnostic screener adapted from the Mini International Neuropsychiatric Interview (Sheehan et al., 1998) for DSM-5 diagnoses. Participants responded to diagnostic screening items using a tablet, and clinicians followed up using a semi-structured interview format to determine any additional DSM-5 diagnoses (e.g., depression, bipolar, anxiety, substance use, eating disorder modules; APA, 2013).
Barkley Adult ADHD Rating Scale-IV (BAARS-IV) Sluggish Cognitive Tempo Subscale
The 9-item SCT subscale of the BAARS-IV (Barkley, 2011) assessed SCT symptoms. The BAARS-IV has good test-retest reliability and internal consistency in a nationally-representative adult sample (Barkley, 2012). The factor structure of the BAARS-IV, which discriminates SCT from ADHD symptoms, has been confirmed in both nationally representative (Barkley, 2012) and college student (Becker, Langberg, et al., 2014) samples. The SCT subscale of the BAARS-IV assesses the frequency of SCT symptoms over the past 6 months using a four-point scale (1 = “rarely or never”; 2 = “sometimes; 3 = “often”; 4 = “very often”). In our prior publication, we found that the BAARS-IV SCT scale had good internal consistency and convergent validity in an adult clinical sample and yielded three factors: slow/daydreamy (four items), sleepy/sluggish (three items), and low initiation/persistence (two items) (Lunsford-Avery et al., 2018).
Composite Scale of Morningness (CSM)
The 13-item CSM provided a self-report measure of diurnal preference (morningness/eveningness; ME (Smith et al., 1989)). The CSM is a well-validated, reliable, and widely used measure of diurnal preference in adults (Adan et al., 2012; Randler, 2009), including in ADHD samples (Caci et al., 2009; Voinescu et al., 2012). Consistent with research suggesting that ME is a dimensional construct falling along a continuum (Natale & Cicogna, 2002), scores from the CSM range from 13 (extreme eveningness preference) to 55 (extreme morningness preference). Negative relationships between ME and clinical measures suggest that greater eveningness is associated with greater clinical severity.
Conners’ Adult ADHD Rating Scale (CAARS)—Self-report version
The 66-item CAARS assesses DSM ADHD diagnostic criteria as well as related symptoms (Conners et al., 1999). Items are rated on a four-point scale (0 = “not at all, never”; 1 = “just a little, once in a while”; 3 = “pretty much, often”; 4 = “very much, very frequently”). The CAARS is a reliable, valid assessment distinguishing individuals with ADHD from their healthy counterparts (Erhardt et al., 1999).
Data Analysis
For Aim 1, partial correlations controlling for age, sex, comorbidity (i.e., presence of more than one disorder; dummy coded as “not present” = 0, “present” = 1), and severity of self-reported ADHD symptoms (i.e., CAARS DSM Total ADHD Symptoms) evaluated relationships between ME preference (CSM total score) and total BAARS-IV SCT severity as well as the three SCT factors in the full sample. For Aim 2, which explores whether relationships between ME and SCT differ among adults with ADHD versus those with internalizing/adjustment disorders, linear regressions controlling for age, sex, and comorbidity in step 1 assessed the main effects of group (ADHD versus internalizing/adjustment disorders) and ME in step 2 and the group-ME interaction in step 3 on SCT total severity and the SCT factors. In this analysis, the interaction effect was the primary outcome of interest. ADHD severity was not included as a covariate for Aim 2 analyses due to its association with group status.
Results
Participants
Of the 65 participants, 43 met criteria for ADHD, any presentation, and 22 received other DSM-5 primary diagnoses, including depressive disorders, anxiety disorders, or/and adjustment disorders. As might be expected in a clinically-referred adult sample, comorbidity rates were high, with 35 (81%) of adults with ADHD and 10 (46%) of adults without ADHD presenting with at least one comorbid diagnosis. The most commonly diagnosed comorbidities in the ADHD group were anxiety (33%, n = 14), depression (23%, n = 10), and a combination of anxiety and depressive disorders (21%, n = 9). Individuals with ADHD did not differ from those with primary internalizing/adjustment disorders in terms of age or sex, but rated themselves significantly higher in terms of ADHD symptom severity. Independent sample t-tests did not indicate any group differences in SCT, SCT factors, or ME. Table 1 provides information about participant demographics.
Demographics of the Study Sample.
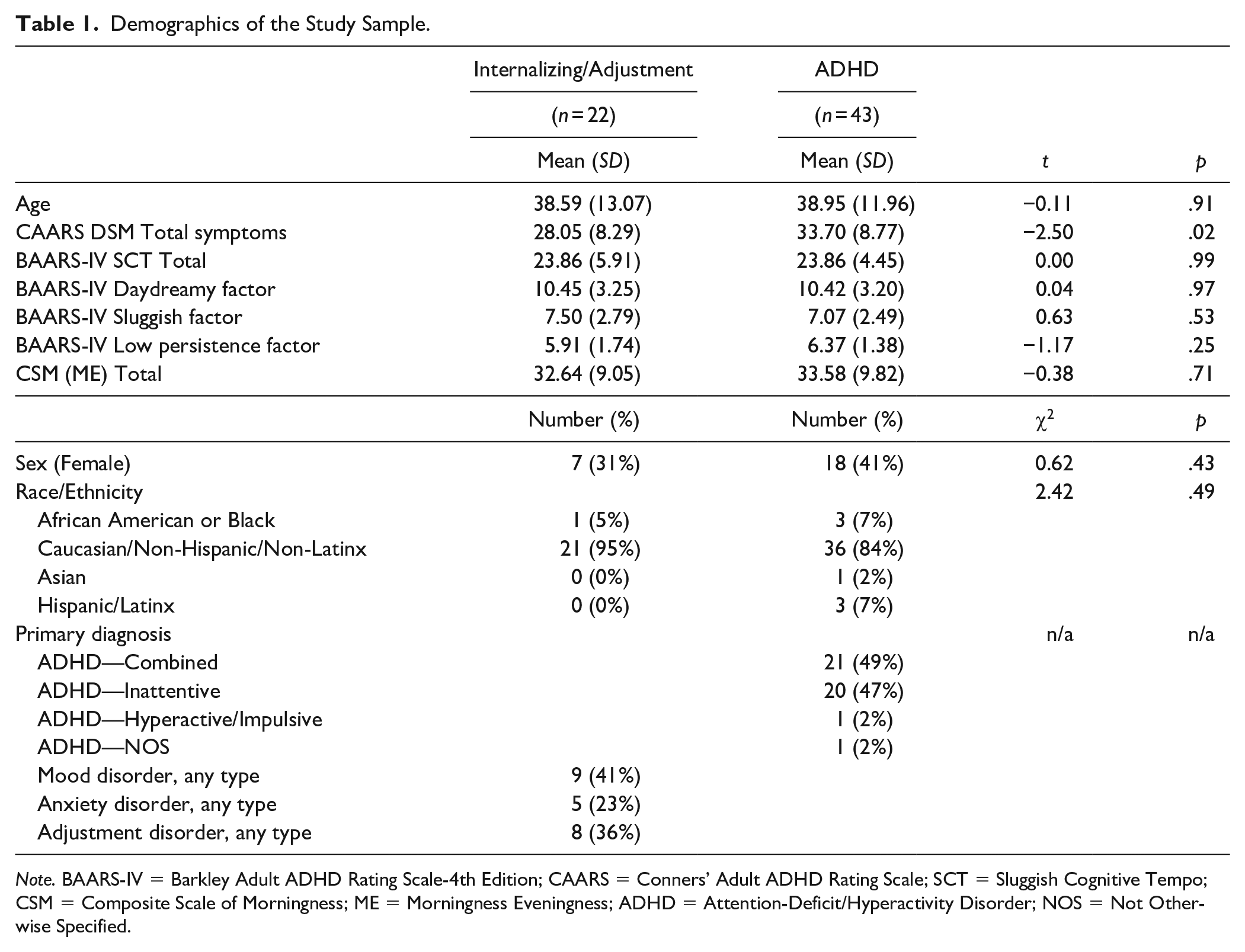
Note. BAARS-IV = Barkley Adult ADHD Rating Scale-4th Edition; CAARS = Conners’ Adult ADHD Rating Scale; SCT = Sluggish Cognitive Tempo; CSM = Composite Scale of Morningness; ME = Morningness Eveningness; ADHD = Attention-Deficit/Hyperactivity Disorder; NOS = Not Otherwise Specified.
Relationship between ME and SCT in the Full Sample
Controlling for age, sex, comorbidity, and ADHD severity, greater tendency toward eveningness was correlated with worsened severity of total SCT symptoms (r = –.26, p = .04), as well as greater severity of sleepy/sluggish symptoms (r = –.41, p = .001). Eveningness was not associated with either the slow/daydreamy (r = .07, p = .61) or low initiation/persistence SCT factors (r = –.19, p = .13).
Relationships of ME to SCT across Groups
In the group analyses, there was a trend for a main effect of ME (β = –.225, t (59) = –1.90, p = .06), but no group effect (ADHD versus internalizing/adjustment disorders; β = –.06, t (59) = .18, p = .63), on total SCT severity was significant after covarying for age, sex, and comorbidity. In addition, the ME-group interaction was significant (β = 1.26, t (59) = 2.69, p = .009). Specifically, although SCT severity did not differ between ADHD and internalizing/adjustment disorder groups in a model that also included ME, the relationship between greater eveningness and worsened SCT symptoms was stronger for the individuals with internalizing/adjustment disorders than for those with ADHD. See Figure 1.
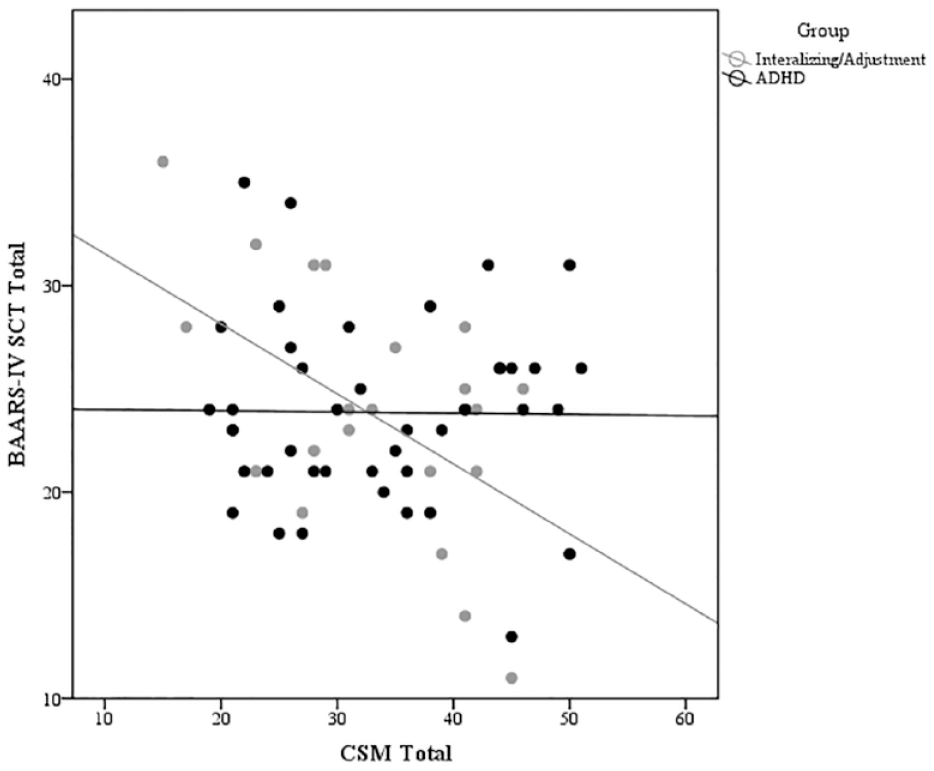
Relationship of ME to BAARS-IV SCT total score by group.
Regarding SCT factors, neither group status (β = -.14, t (59) = 1.09, p = .28) nor ME (β = .06, t (59) = .46, p = .65) was significantly related to the slow/daydreamy factor after controlling for age, gender, and comorbidity. However, the ME-group interaction was significant (β = 1.05, t (59) = 2.19, p = .03), suggesting the association between greater eveningness and worsened slow/daydreamy symptoms was more robust for the individuals with internalizing/adjustment disorders than individuals with ADHD. See Figure 2.
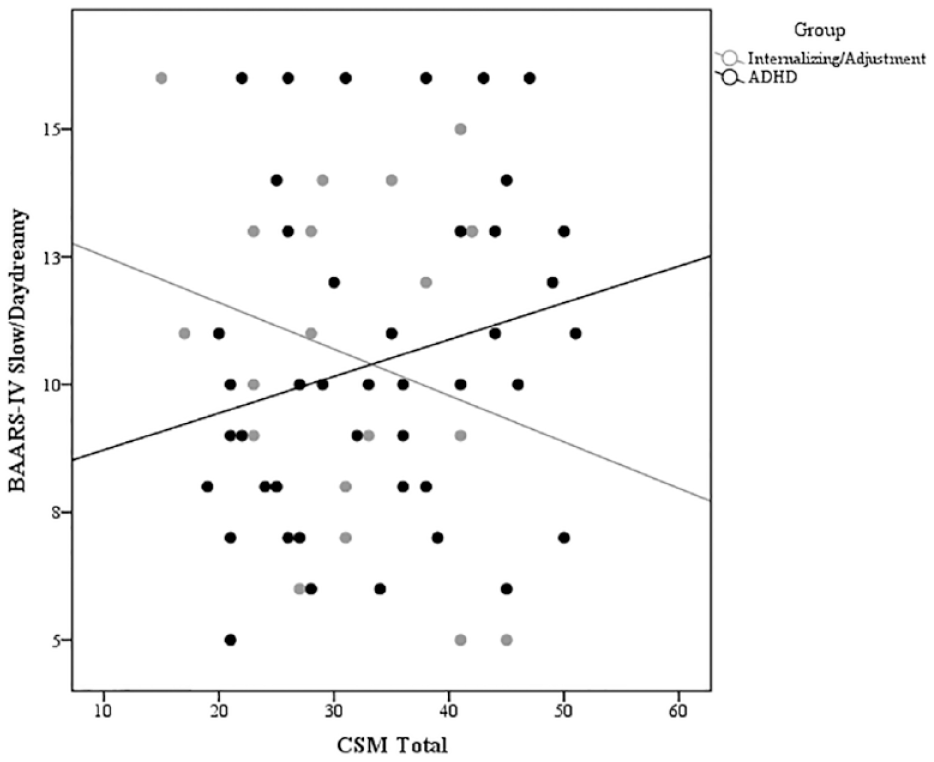
Relationship of ME to slow/daydreamy SCT factor by group.
Concerning the sleepy/sluggish factor, the main effect for ME was significant (β = –.40, t (59) = -3.46, p = .001) after covarying for age, sex, and comorbidity, but not the group main effect (β = -.05, t (59) = –.43, p = .67) or the group-ME interaction (β = .75, t (59) = 1.60, p = .12), suggesting that greater eveningness contributes to greater sleepy/sluggish symptoms in a similar pattern across groups. See Figure 3. Finally, neither main effect nor the interaction was associated the low initiation/persistence factor after controlling for age, sex, and comorbidity (p’s > .10).
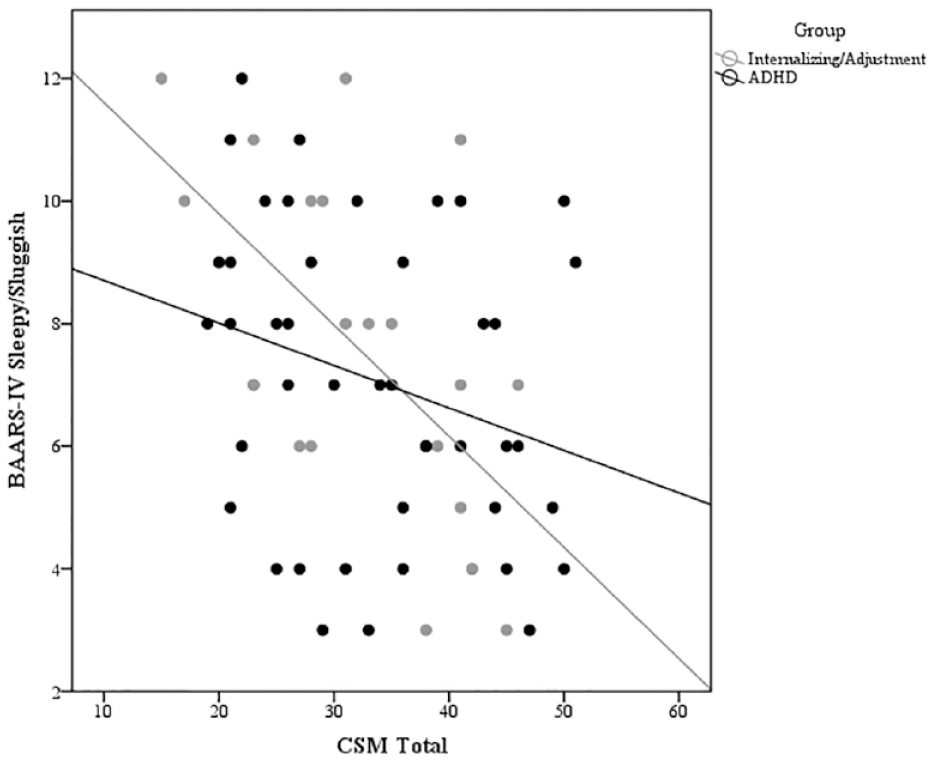
Relationship of ME to sleepy/sluggish SCT factor by group.
Discussion
To our knowledge, this is the first study to examine relationships between diurnal preference and SCT in an adult clinical sample. Results indicated that greater eveningness preference was associated with greater overall self-reported SCT among adult outpatients presenting for an ADHD evaluation, and this association appears to be driven primarily by a relationship between eveningness and the sleepy/sluggish SCT factor. These associations are robust after controlling for potentially important covariates, including ADHD severity, comorbidity, age, and sex, and are consistent with a prior finding linking eveningness and SCT in a population sample (Voinescu et al., 2012). The specific relationship between the sleepy/sluggish factor and eveningness provides additional evidence for the validity of this specific factor as separate from other SCT factors (Lunsford-Avery et al., 2018) and is consistent with prior work suggesting an association between SCT, particularly items related to lethargy and difficulty remaining alert, and daytime sleepiness (Langberg et al., 2014).
In addition, current findings indicated that relationships between eveningness and SCT differed among individuals who received an ADHD diagnosis and those who received internalizing and/or adjustment diagnoses following evaluation. Specifically, associations between eveningness and overall SCT severity and specifically, the slow/daydreamy factor, were stronger for individuals with internalizing/adjustment disorders than those with ADHD, whereas the relationship between eveningness and the sleepy/sluggish factor was uniform across groups. This pattern may suggest that contributors to SCT symptoms may differ across individuals with ADHD versus those who present with attentional concerns, but do not meet criteria for the disorder, and has important research and clinical implications. Notably—given the high rates of internalizing disorder comorbidity within the ADHD group—it is largely the presence of ADHD, rather than the absence of internalizing symptoms, that differentiated the groups in this study. This may suggest the presence of other factors that contribute to SCT in ADHD adults, while suggesting a greater role of eveningness in SCT presentation among individuals with attentional complaints who do not meet ADHD criteria.
Although a body of research exists to support the prevalence and burden of SCT, as well as its distinction from ADHD, the etiology of SCT symptoms remains largely unknown (Becker & Barkley, 2018). The link between eveningness and SCT, particularly with sleepy/sluggish symptoms, highlights a potential role of eveningness diurnal preference in the presentation of SCT among adult outpatients. However, whether eveningness represents a cause, consequence, or correlate of SCT is unclear and beyond the scope of the current study. It is possible that for some individuals, greater eveningness preference results in a mismatch between their preference for activity in the evening/night and their daytime requirements for task completion at work and home, and subsequently contributes to sleepy, sluggish daytime symptoms (i.e., eveningness a cause of SCT). Alternatively, increased SCT symptoms and difficulty completing tasks during the day could interfere with adhering to earlier bedtimes (i.e., eveningness a consequence of SCT), or SCT and eveningness could co-occur, perhaps due to a shared underlying genetic or neurobiological etiology (i.e., eveningness a correlate of SCT).
Future research is vital to tease out the direction of these effects and to clarify how the SCT construct intersects with other constructs resulting in sluggishness, including sleep/circadian factors. Recently, Becker and colleagues outlined a research agenda for advancing the understanding of SCT using a Research Domain Criteria (RDoC) framework and highlighted examination of the arousal/circadian construct as a potential biomarker underlying SCT and linking it with internalizing disorders and ADHD (Becker & Willcutt, 2019). They argued that examination of the arousal/circadian construct in relationship to multiple disorders/dimensions (i.e., SCT, ADHD, and depression) was critical for clarifying relationships among these disorders with respect to overlapping and unique symptoms. Our findings suggest that eveningness—a close correlate of a delayed circadian rhythm—may be a biomarker of interest for future investigation of SCT. In addition, eveningness may underlie overlapping sleepy/sluggish symptoms across disorders while uniquely contributing to slow/daydreamy symptoms in internalizing/adjustment disorders in the absence of ADHD. However, these findings require replication and further study.
Clinically, results have implications for both assessment and treatment of adult outpatients. Regarding assessment, all of the adults included in this study were seeking an evaluation for ADHD, and as such, endorsed presenting concerns such as inattention, difficulty completing tasks, and/or restlessness. However, following a thorough ADHD assessment, a third of the sample did not meet criteria for ADHD. The current study suggests the importance of assessing both diurnal preference and SCT in clinical evaluations for ADHD, as eveningness, SCT, and their interplay may underlie the daytime dysfunction experienced by these individuals. Indeed, systematic evaluation of sleep disorders, including circadian rhythm disorders, as well as SCT are frequently absent from psychiatric evaluations and would inform both clinical assessment and research in this area. Relatedly, identification of eveningness diurnal preference may suggest the possibility of circadian treatments, such as melatonin and bright light therapy, in the amelioration of SCT symptoms among adult outpatients, a possibility that should also be the focus of future investigation.
This study is subject to several limitations. First, as mentioned above, this cross-sectional, observational study cannot shed light on the direction of effects between eveningness and SCT. Second, this study relied on subjective reports of eveningness and SCT, which may be vulnerable to reporter biases. Third, this sample was relatively small and largely homogeneous in terms of race/ethnicity, and thus, generalization of results to diverse populations should be made with caution. Fourth, this study did not include a non-clinical control group, so it was not possible to evaluate whether SCT-eveningness relationships differ between clinical and healthy populations. Given the outpatient nature of our clinic, our sample also did not include adults with significant externalizing behaviors other than ADHD (e.g., severe substance use, antisocial behaviors). Finally, although the BAARS-IV SCT subscale has been validated in several adult samples (Barkley, 2012; Becker, Langberg, et al., 2014; Lunsford-Avery et al., 2018), there has been a recent effort to develop a specific SCT scale for use with adults (Becker et al., 2017), which may be useful for future studies assessing relationships between SCT and eveningness. Future studies using longitudinal and/or experimental designs, objective measures of circadian function such as dim light melatonin onset, and diverse samples including non-clinical controls and adults with externalizing behaviors other than those consistent with ADHD may further elucidate associations between circadian functioning and SCT among adult outpatients.
In conclusion, greater eveningness appears to be associated with SCT among adult outpatients, particularly sleepy/sluggish symptoms. In addition, relationships between eveningness and SCT may differ across individuals presenting with externalizing disorders, such as ADHD, versus those with primary internalizing and/or adjustment disorders. Future research is necessary to clarify a potential role of circadian processes in the etiology and treatment of SCT.
Footnotes
Acknowledgements
Thank you to Michelle Lepsch-Halligan, Savannah Wellington, Caroline Barry, and Sierra Tolbert for their assistance with data management and to Julia Schechter, Ph.D., Jessica Solis Sloan, Ph.D., Cara Lusby, Ph.D., and Naomi Ornstein Davis, Ph.D. for serving as assessment clinicians. We also express our gratitude to the participants and their families for their valuable contribution to research.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Lunsford-Avery and Dr. Sweitzer have no conflicts of interest to report. Dr. Mitchell has consulting fees from Avanir Pharmaceuticals. Dr. Kollins has received research support and/or consulting fees from the following commercial sources: Akili Interactive, Bose, Jazz, KemPharm, Neos, OnDosis, Otsuka, Rhodes, Sana Health, and Tris.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Mental Health grant K23 MH108704 to Dr. Lunsford-Avery and the National Institute of Drug Abuse grants K23 DA032577 to Dr. Mitchell, K24 DA023464 to Dr. Kollins, and K23 DA039294 to Dr. Sweitzer.