
Abstract
Objective
The aim of this study was to characterize the course of ADHD during pregnancy.
Method
Women ages 18 to 45 were followed prospectively at <20 weeks, 24 weeks, and 36 weeks pregnant. Three groups emerged: women who discontinued, maintained, or adjusted their ADHD medications. ADHD symptoms were recorded using the AISRS. Anxiety, depression, stress, and functional impairment were monitored.
Results
A total of 25 women with ADHD were eligible for analysis. No significant difference observed between three groups in AISRS scores. Significant differences found between medication discontinuers vs adjusters for both mood and family functioning (EPDS, 5.3, p < .0001; WFIRS, 3.3, p = .0309). Significant differences also found between discontinuers vs maintainers for mood and family functioning (EPDS, 4.98, p = .0009; WFIRS, 3.09, p = .0197).
Conclusion
This preliminary study provides novel insight into the course of ADHD during pregnancy, underscoring mood and family functioning as critical domains that may contribute to growing use of psychostimulants during pregnancy.
Introduction
ADHD is a prevalent neurobehavioral disorder of relevance to women’s health. It affects approximately one in 30 women, and ADHD that persists into adulthood is associated with depression, anxiety, substance misuse, and impairment across domains of functioning (Biederman et al., 2010; Faraone, 2018). Adult women with ADHD can experience difficulties at work and in their personal and family lives related to their ADHD symptoms (Owens et al., 2017). Given that treatment of adult ADHD improves functioning and quality of life, some women may elect to continue their medications during pregnancy (Agarwal et al., 2012).
To date, there are no systematic data available about the course of ADHD during pregnancy. Prospective data about the course of ADHD in the general population highlights the disorder as being heterogenous, a chronic condition best managed multimodally (psychosocial and pharmacotherapy interventions), and most often associated with comorbid mood and anxiety disorders (Wilens & Spencer, 2010). Data available about reproductive safety of stimulant medication are growing. A recent scoping review of methylphenidate exposure during pregnancy demonstrates a small but statistically significant risk of cardiac malformations with a number needed to harm of about one in 159 (Koren et al., 2020). There are fewer available data about the reproductive safety of stimulant medications in terms of obstetrical, perinatal, and neurobehavioral outcomes. Despite this, recent epidemiological studies suggest stimulants are among the most commonly prescribed medications during pregnancy, with an estimated 1% exposure prevalence (Louik et al., 2015). This observational cohort study was designed to characterize the course of ADHD during pregnancy, including the treatment decisions and associated maternal outcomes.
Methods
This observational cohort study investigated the severity of ADHD symptoms, psychiatric comorbidities, and functional outcomes among pregnant women ≥18 years old. Participants were eligible if they (1) met Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for ADHD via a structured diagnostic clinical interview with a research-trained board-certified psychiatrist, (2) had current or past history of psychostimulant use for ADHD, (3) were English-speaking, and (4) were planning pregnancy or ≤20 weeks pregnant. All medical treatment decisions were made between the participant and her treating provider, independent of study participation.
Assessments
From August 2017 to May 2019, psychiatric assessments were administered longitudinally to participants who were either pregnant or planning pregnancy as outlined in Figure 1. At each interview, study staff administered the Montgomery–Asberg Depression Rating Scale (MADRS) and the Adult ADHD Investigator Symptom Rating Scale (AISRS), an 18-item questionnaire that evaluates the severity of both hyperactivity and inattentive ADHD in symptoms over the past 2 weeks. Study staff were trained in the AISRS by a board-certified child psychiatrist. Subjects also completed the Edinburgh Postnatal Depression Scale (EPDS), the Generalized Anxiety Disorder 7-item (GAD-7) scale, the Perceived Stress Scale (PSS), and the Weiss Functional Impairment Rating Scale Self-Report (WFIRS-S).
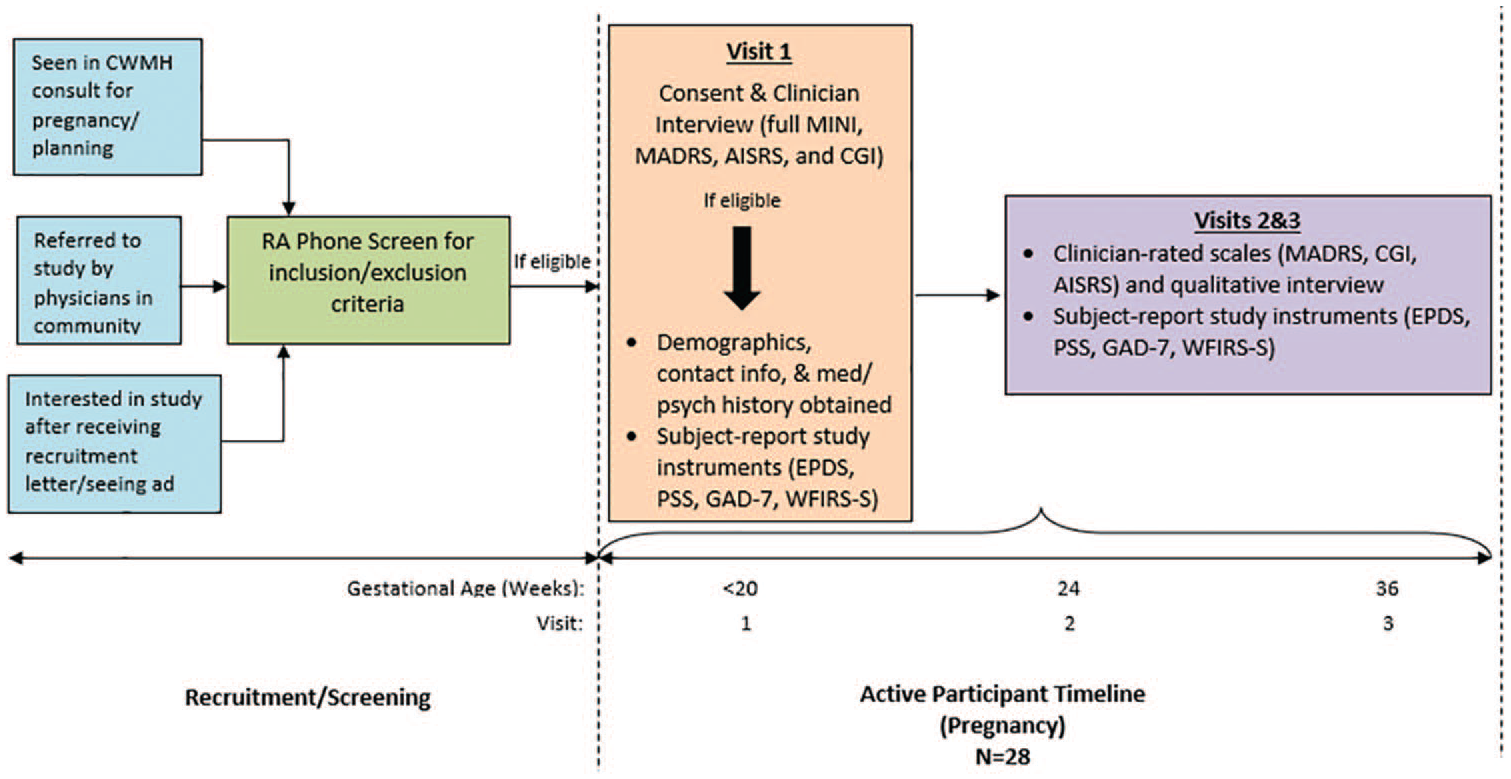
Detailed overview of study design and assessments.
Analysis and Results
N = 28 women with ADHD were followed through pregnancy. A total of 25 were eligible for analysis comprising three groups: five women who discontinued ADHD medications (Group A), eight women who changed their ADHD medication regimen with the effort to decrease use in pregnancy but maintain therapeutic benefits “as needed” (Group B), and 12 women who continued their ADHD medication with no changes through pregnancy (Group C).
To determine differences among the groups over time for each of the various scales, a linear model using generalized estimating equations was used. The dependent variable was the change in the scale measure from baseline (visit 1) to visits 2 and 3. The independent variables were the baseline measure (continuous), visit (categorical; 2 or 3), and group membership (categorical: discontinued, PRN, or maintained). Least squares mean values for the differences among the groups over time are reported for results (p-values are not adjusted for multiple testing).
Results for three measures indicated statistically significant differences among the groups over time. Baseline values of these measures were:
For the Hyperactive AISRS, the group that discontinued ADHD medication had an average score of 13.2 (SD 5.72), the group that changed meds as needed had an average score of 10.5 (SD 5.68), and the group that continued meds had an average score of 9.5 (SD 5.37).
For the EPDS Total measure, women who discontinued ADHD medications had a score of 5.4 (SD 4.98), those changing meds as needed had a score of 5.6 (SD 2.200), and those discontinuing meds had an average score of 5.3 (SD 4.67).
For the WFIRS-Family measure, the discontinuing group’s score was 4.2 (SD 3.42), the group that changed meds as needed had an average score of 4.5 (SD 4.00), and the group that continued meds had an average score of 2.7 (SD 2.42).
Results from the GEE modeling showed:
For the Hyperactive AISRS sub-score, adjusted mean changes of: discontinuers, −0.39, the PRN group, −1.92, and Maintainers, −2.78, showing a significant difference between those who discontinued medication versus those who maintained their meds of 2.39 (p = .0128).
For the total EPDS score, adjusted mean changes of: discontinuers, 4.32, meds as needed, −1.01, and maintainers, −0.65, showing significant differences between those who discontinued meds and those changing meds as needed (5.3, p < .0001) and discontinuers vs maintainers (4.98, p = .0009).
For the sum of the WFIRS Family Domain, the adjusted mean changes of: discontinuers, 1.55, meds as needed, −1.70, maintainers, −1.54, showing significant differences between those who discontinued meds and those changing meds as needed (3.3, p = .0309) and discontinuers versus maintainers (3.09, p = .0197).
Discussion
Women who discontinued psychostimulant treatment during pregnancy had a clinically significant increase in EPDS scores despite not changing their antidepressant medication (Figure 2a). Further, women who discontinued psychostimulant treatment during pregnancy had significant impairment in family functioning (Figure 2b). Specifically, this means they are more likely to experience conflict within the family, have a harder time having fun as a family, rate parenting as more difficult, and describe being more isolated from their family (Weiss et al., 2018). While there was not a clinically meaningful significant difference found between groups in terms of overall ADHD symptoms (Figure 2c), the combined increase in depressed mood symptoms and functional disability in the family domain suggest that symptoms alone may not be a reliable proxy for overall functioning when it comes to understanding the course and impact of ADHD in pregnancy.
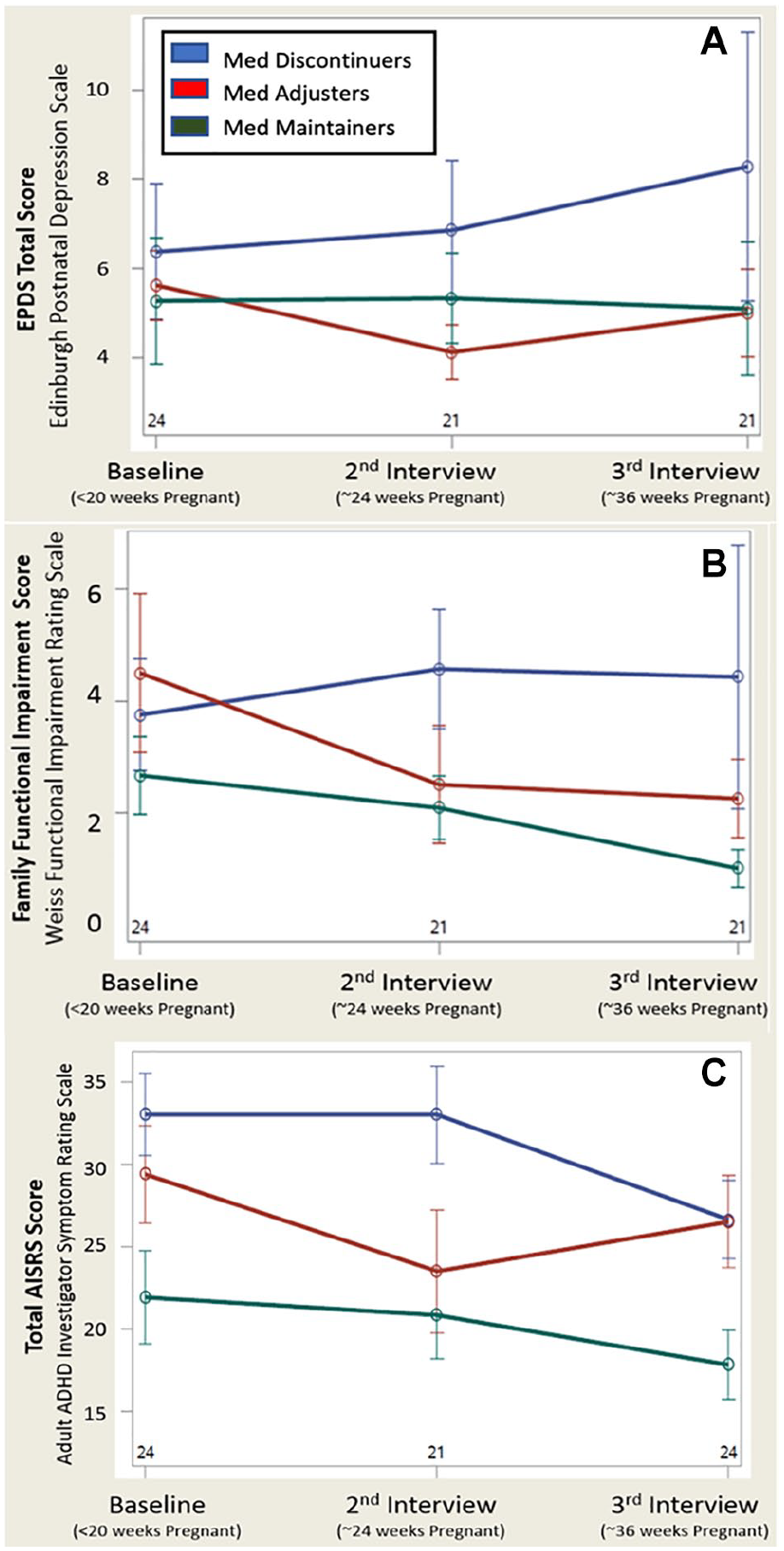
(a) Edinburgh Postnatal Depression Scale (EPDS), self-reported depression and anxiety symptoms across timepoints and treatment groups. Adjusted mean changes of: discontinuers, 4.32, meds as needed, –1.01, and maintainers, –0.65, showing significant differences between those who discontinued meds and those changing meds as needed (5.3, p < .0001) and discontinuers vs maintainers (4.98, p = .0009), (b) self-reported impairment in family functioning measured across three pregnancy timepoints and between medication groups. The adjusted mean changes of: discontinuers, 1.55, meds as needed, –1.70, maintainers, –1.54, showing significant differences between those who discontinued meds and those changing meds as needed (3,3, p = .0309) and discontinuers vs maintainers (3.09, p = .0197), and (c) adult ADHD Investigator Symptom Rating Scale (AISRS), investigator rated ADHD symptoms across timepoints and treatment groups. Adjusted mean changes of: discontinuers, meds as needed, and maintainers, showing no significant differences between groups.
Clinical Implications
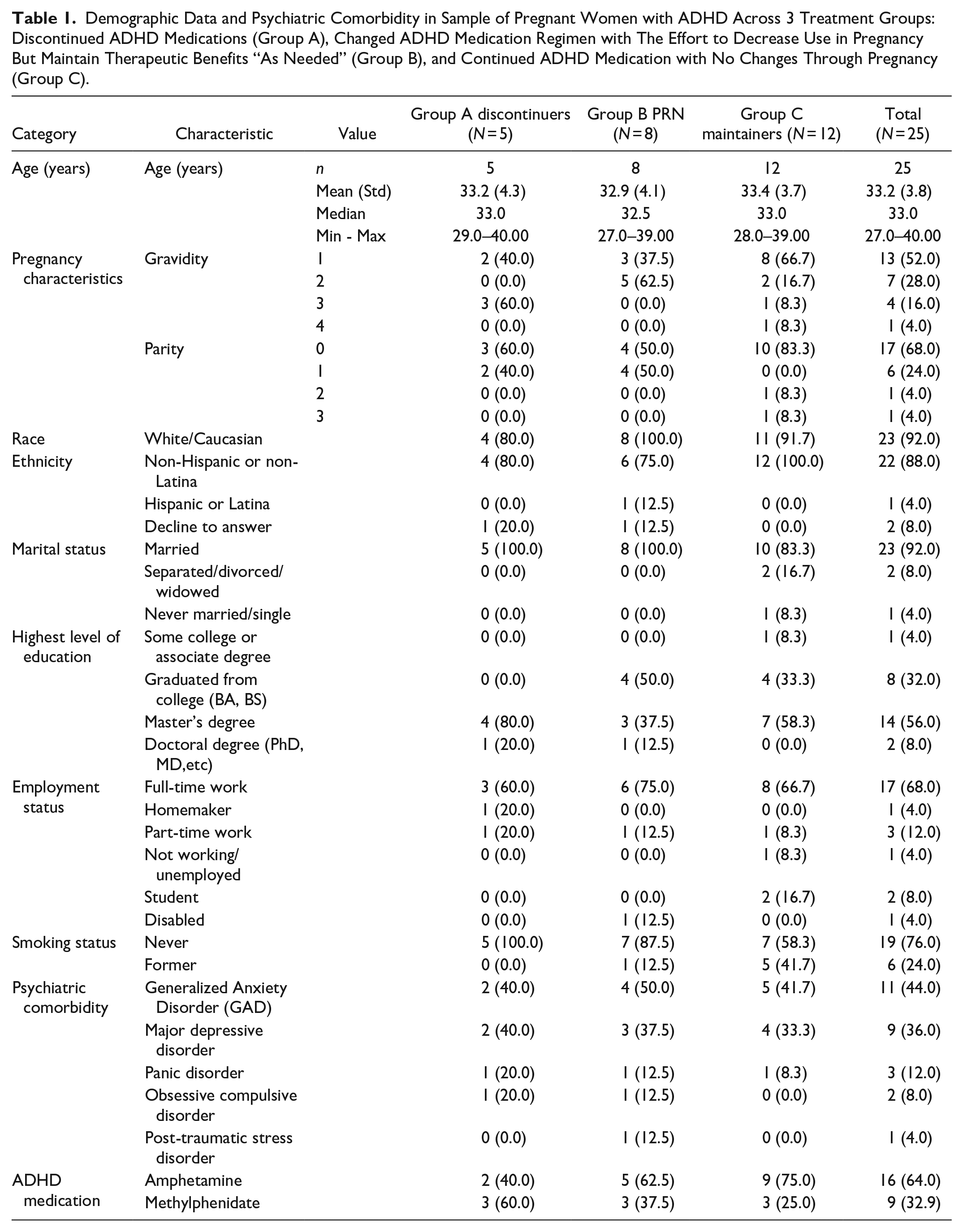
These data mirror the clinical phenomenon of an expectant woman with ADHD who describes feeling more “together,” centered, and generally competent when she has the ability to take her stimulant medication as she deems appropriate. 50% of participants had Generalized Anxiety Disorder, and 32% had Major Depressive Disorder (Table 1). Given this reality of psychiatric comorbidity, clinicians must consider the whole clinical picture in concert to collaborate effectively with their patients. Historically, physicians have advised patients to reconsider stimulant medication use during pregnancy based on paucity of data, but this study highlights the importance and nuance of the risk-risk assessment when prescribing during pregnancy: weighing the risks of medication exposure during pregnancy with the risks of exposure to untreated psychiatric disorders (Ornoy, 2018). In particular, these data suggest that the benefit of taking stimulants during pregnancy on an as-needed basis extend beyond management of ADHD symptoms like hyperactivity and inattention. This approach gives women the option to decrease medication exposure while optimizing their ability to function in their family setting and lowering their risk for comorbidity.
Demographic Data and Psychiatric Comorbidity in Sample of Pregnant Women with ADHD Across 3 Treatment Groups: Discontinued ADHD Medications (Group A), Changed ADHD Medication Regimen with The Effort to Decrease Use in Pregnancy But Maintain Therapeutic Benefits “As Needed” (Group B), and Continued ADHD Medication with No Changes Through Pregnancy (Group C).
Strengths of this study include its prospective design and the diagnostic heterogeneity of the sample, representative of the highly comorbid nature of ADHD. Limitations of this study include small sample size and lack of placebo or case control. It is also possible that interaction with study staff throughout pregnancy offered ancillary support to women in the enrolled sample, thereby minimizing the impact of psychostimulant discontinuation on ADHD symptoms.
ADHD is a neurobiological disorder that affects women across the lifespan. This preliminary study provides novel insight into the course of the disorder during pregnancy, underscoring depression risk and family functioning as critical domains that may contribute to decision making about psychostimulant use during pregnancy.
Footnotes
Acknowledgements
The authors would like to thank Dr. Joseph Biederman for graciously facilitating their use of the AISRS, and Dr. Craig Surman for generously training Dr. Baker on the AISRS.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LSC and MF receive research funding for the National Pregnancy Registry for Atypical Antipsychotics from: Alkermes Biopharmaceuticals; Forest/Actavis Pharmaceuticals; Otsuka Pharmaceuticals; Sunovion Pharmaceuticals, Inc.; Teva Pharmaceuticals; Sage Therapeutics, Inc. LSC also receives research support from: Brain & Behavior Research Foundation; JayMac Pharmaceuticals; National Institute on Aging; National Institutes of Health; SAGE Therapeutics. MF also receives research support from: JayMac Pharmaceuticals, SAGE Therapeutics; As an employee of MGH, Dr. Freeman works with the MGH CTNI, which has had research funding from multiple pharmaceutical companies and NIMH. AB, RW, PG and ON have no disclosures to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Gerstner Family Foundation through the 2017 Louis V. Gerstner III Research Scholar Award. The Foundation had no role in study design, writing of the report, or data collection, analysis, or interpretation.